
Informal Caregivers’ Health Literacy in Lisbon, Portugal: A Profile for Health Promotion Prioritization
 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
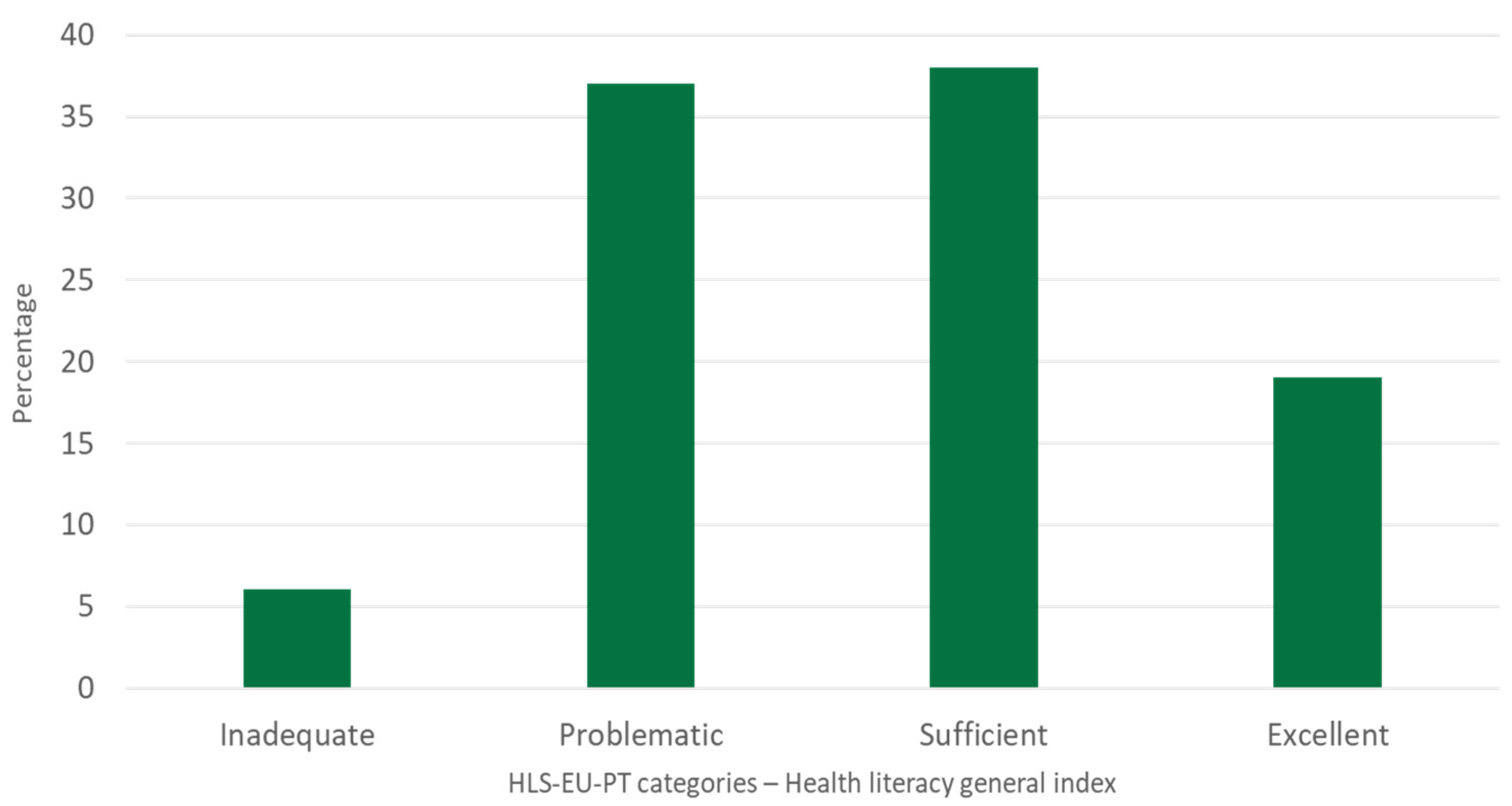
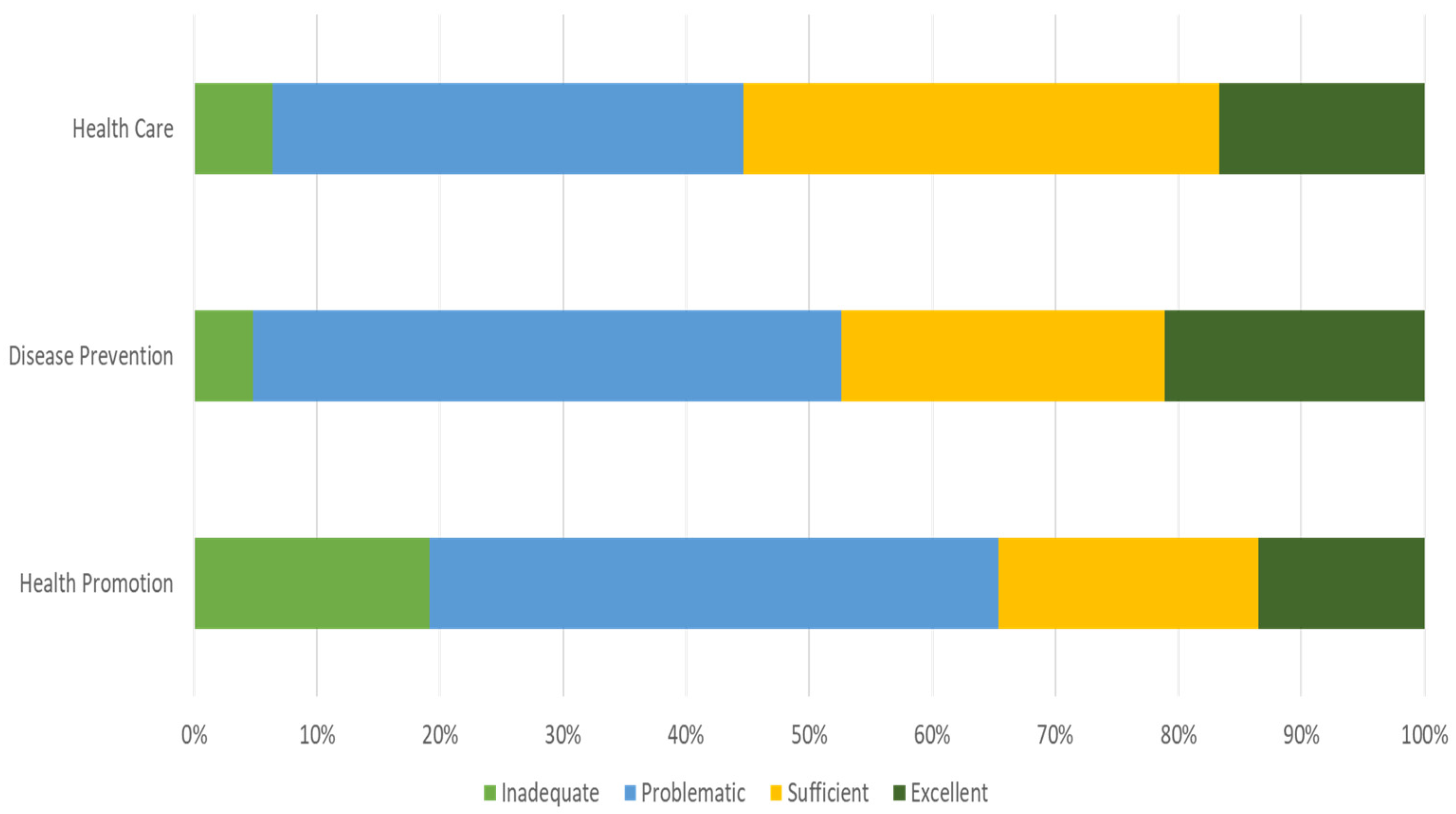
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Sociodemographic Data of the Informal Caregiver

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Dimension | N | % |
|---|---|---|---|
| Gender | Female | 231 | 73% |
| Male | 84 | 27% | |
| Marital status | Married | 167 | 57% |
| Single | 61 | 21% | |
| Divorced/Separated | 51 | 17% | |
| Widowed | 16 | 5% | |
| Education | Does not know how to read and write | 4 | 1% |
| Knows how to read and write | 3 | 1% | |
| 4 years (primary school) | 37 | 13% | |
| 6 years (junior school) | 15 | 5% | |
| 9 years (basic school) | 37 | 13% | |
| 12 years (high school) | 67 | 23% | |
| Higher education degree | 131 | 44% | |
| Other | 1 | 0% | |
| Profession | Armed forces | 1 | 0% |
| Representatives of the legislative offices and executive institutions, directors and executive managers | 26 | 9% | |
| Scientific and intellectual activities specialists | 85 | 29% | |
| Technicians and associate professions | 31 | 11% | |
| Administrative personnel | 71 | 24% | |
| Personal and security services and sellers | 45 | 15% | |
| Farmers and skilled agricultural, fishing and forestry workers | 2 | 1% | |
| Skilled workers in industry, construction and craftsmen | 13 | 4% | |
| Facility workers and machine operators | 12 | 1% | |
| Non-skilled workers | 16 | 6% | |
| Financial status (average monthly income) | <EUR 665 | 81 | 28% |
| EUR 665—1270 | 113 | 38% | |
| EUR 1270—1905 | 52 | 18% | |
| EUR 1905—2540 | 26 | 9% | |
| EUR 2540—3175 | 12 | 4% | |
| >EUR 3175 | 10 | 3% |
Appendix B. Bivariate Statistics—Health Literacy and Sociodemographic Factors
| Covariate/Factor | Dependent Variable | Test | Significance |
|---|---|---|---|
| Gender | Health literacy—HLS-EU-PT categories | Pearson’s Chi-Square | p = 0.487 |
| Health literacy—HLS-EU-PT score | Student’s t Mann–Whitney | p = 0.618 p = 0.470 | |
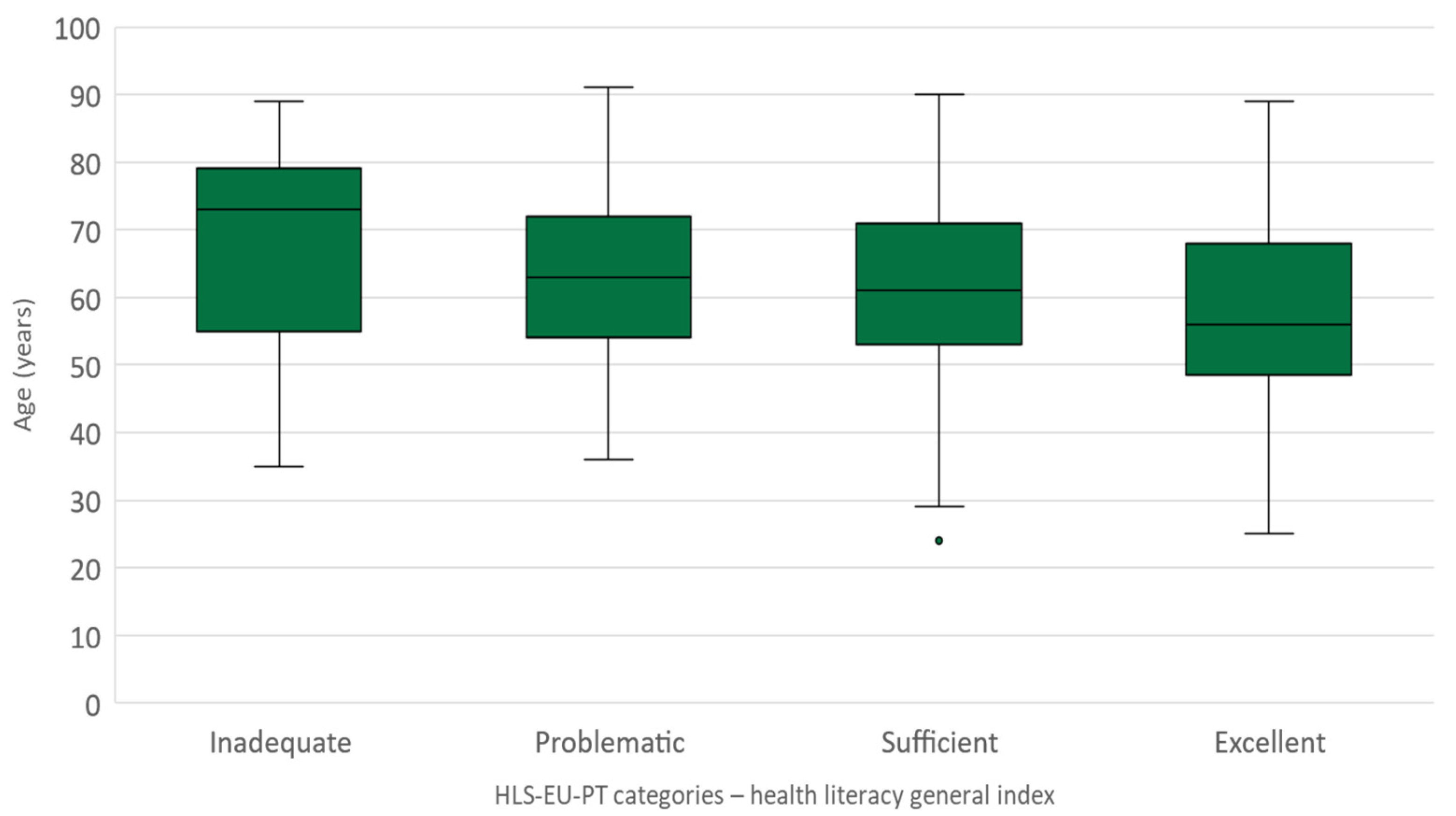
| Age | Health literacy—HLS-EU-PT categories | ANOVA Kruskal–Wallis | p = 0.046 p = 0.049 |
| Health literacy—HLS-EU-PT score | Pearson’s correlation coefficient | p = 0.069 | |
| Education | Health literacy—HLS-EU-PT categories | Fisher’s Exact Test (Monte Carlo approach, IC 95%) | p = 0.001 |
| Health literacy—HLS-EU-PT score | Kruskal–Wallis | p = 0.274 | |
| Barthel Index for Activities of Daily Living (score) | Health literacy—HLS-EU-PT categories | ANOVA Kruskal–Wallis | p = 0.531 p = 0.560 |
| Health literacy—HLS-EU-PT score | Pearson’s correlation coefficient | p = 0.515 | |
| Lawton & Brody Instrumental Activities of Daily Living (score) | Health literacy—HLS-EU-PT categories | ANOVA Kruskal–Wallis | p = 0.380 p = 0.222 |
| Health literacy—HLS-EU-PT score | Pearson’s correlation coefficient | p = 0.227 | |
| Financial status | Health literacy—HLS-EU-PT categories | Fisher’s Exact Test (Monte Carlo approach, IC 95%) | p = 0.409 |
| Health literacy—HLS-EU-PT score | ANOVA Kruskal–Wallis | p = 0.228 p = 0.287 | |
| Caregiver transition | Health literacy—HLS-EU-PT categories | Fisher’s Exact Test (Monte Carlo approach, IC 95%) | p = 0.375 |
| Health literacy—HLS-EU-PT score | ANOVA Kruskal–Wallis | p = 0.476 p = 0.291 | |
| Family / friends support | Health literacy—HLS-EU-PT categories | Pearson’s Chi-Square | p = 0.557 |
| Health literacy—HLS-EU-PT score | Student’s t Kruskal–Wallis | p = 0.173 p = 0.091 | |
| Professional support | Health literacy—HLS-EU-PT categories | Pearson’s Chi-Square | p = 0.967 |
| Health literacy—HLS-EU-PT score | Student’s t Mann–Whitney | p = 0.764 p = 0.856 | |
| Private support | Health literacy—HLS-EU-PT categories | Pearson’s Chi-Square | p = 0.305 |
| Health literacy—HLS-EU-PT score | Student’s t Mann–Whitney | p = 0.113 p = 0.284 | |
| Knowledge about community resources | Health literacy—HLS-EU-PT categories | Pearson’s Chi-Square | p = 0.177 |
| Health literacy—HLS-EU-PT score | Student’s t Mann–Whitney | p = 0.006 p = 0.007 | |
| Demand for health services | Health literacy—HLS-EU-PT categories | Pearson’s Chi-Square | p = 0.793 |
| Health literacy—HLS-EU-PT score | Student’s t Mann–Whitney | p = 0.910 p = 0.856 | |
| Demand for social services | Health literacy—HLS-EU-PT categories | Pearson’s Chi-Square | p = 0.779 |
| Health literacy—HLS-EU-PT score | Student’s t Mann–Whitney | p = 0.691 p = 0.899 | |
| Inclusion in caregiver’s support program | Health literacy—HLS-EU-PT categories | Fisher’s Exact Test (Monte Carlo approach, IC 95%) | p = 0.103 |
| Health literacy—HLS-EU-PT score | ANOVA Kruskal–Wallis | p = 0.755 p = 0.679 | |
| Knowledge about the statute of the informal caregiver | Health literacy—HLS-EU-PT categories | Pearson’s Chi-Square | p = 0.103 |
| Health literacy—HLS-EU-PT score | Student’s t Mann–Whitney | p = 0.672 p = 0.793 | |
| WHO Well-Being Index (score) | Health literacy—HLS-EU-PT categories | ANOVA Kruskal–Wallis | p = 0.001 p = 0.001 |
| Health literacy—HLS-EU-PT score | Pearson’s correlation coefficient | p = 0.001 |
References
- Portuguese Directorate-General of Health (DGS); Institute for Health Metrics and Evaluation. Portugal: The Nation’s Health 1990-2016, An Overview of the Global Burden of Disease Study 2016 Results; IHME: Lisbon, Portugal, 2018; Available online: http://hdl.handle.net/10400.26/22502 (accessed on 12 July 2022).
- pordata.org. Data on Portuguese Birth Rate. Available online: https://www.pordata.pt/Portugal/Taxa+bruta+de+natalidade-527 (accessed on 12 July 2022).
- Boskovic, S.; Ghio, D.; Goujon, A.; Kalantaryan, S.; Belmonte, M.; Scipioni, M.; Conte, A.; Gómez-González, E.; Gómez, E.; Tolan, S.; et al. Health and Long-Term Workforce: Demographic Challenges and the Potential Contribution of Migration and Digital Technology; Publications Office of the European Union: Luxembourg, 2021. [Google Scholar] [CrossRef]
- Directorate-General for Employment, Social Affairs and Inclusion; ECORYS. Study on Exploring the Incidence and Costs of Informal Long-Term Care in the EU; Publications Office of the European Union: Luxembourg, 2021. [Google Scholar] [CrossRef]
- Spasova, S.; Baeten, R.; Coster, S.; Ghailani, D.; Peña-Casa, R.; Vanhercke, B. Challenges in Long-Term Care in Europe: A Study of National Policies; European Commission: Brussels, Belgium, 2018. [Google Scholar] [CrossRef]
- eurocarers.org. Data about Informal Caregivers in Europe. Available online: https://eurocarers.org/about-carers/ (accessed on 12 July 2022).
- OECD. Health at a Glance 2019: OECD Indicators; OECD Publishing: Paris, France, 2020. [Google Scholar] [CrossRef]
- Nolan, M.; Davies, S.; Brown, J.; Keady, J.; Nolan, J. Beyond ‘person-centred’ care: A new vision for gerontological nursing. J. Clin. Nurs. 2004, 13, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, M.; Queirós, C.; Guerra, M. The caregivers concept analysed in an autopoietic perspective: From the chaos to the autopoiesis. Psicol. Saúde Doenças 2007, 8, 181–196. [Google Scholar]
- André, S.; Nunes, M.; Martins, M.; Rodrigues, V. Mental health of informal caregivers of dependent elderly patients after cerebrovascular accident. Rev. De Enferm. Ref. 2013, 3, 85–94. [Google Scholar] [CrossRef]
- World Health Organization. Promoting Health: Guide to National Implementation of the Shanghai Declaration; World Health Organization: Geneva, Switzerland, 2018; Available online: https://www.who.int/publications/i/item/WHO-NMH-PND-18.2 (accessed on 12 July 2022).
- World Health Organization. Health Literacy: The Solid Facts; World Health Organization: Geneva, Switzerland, 2013; Available online: https://apps.who.int/iris/bitstream/handle/10665/128703/e96854.pdf (accessed on 12 July 2022).
- Portuguese Directorate-General of Health (DGS). Manual de Boas Práticas Literacia em Saúde-Capacitação dos Profissionais de Saúde; DGS: Lisbon, Portugal, 2019; Available online: https://www.dgs.pt/documentos-e-publicacoes/manual-de-boas-praticas-literacia-em-saude-capacitacao-dos-profissionais-de-saude.aspx (accessed on 12 July 2022).
- Costa, A.; Arriaga, M.; Veloso Mendes, R.; Miranda, D.; Barbosa, P.; Sakellarides, C.; Peralta, A.; Ambrósio Lopes, N.; Roque, C.; Ribeiro, S. A Strategy for the Promotion of Health Literacy in Portugal, Centered around the Life-Course Approach: The Importance of Digital Tools. Port. J. Public Health 2019, 37, 50–54. [Google Scholar] [CrossRef]
- Portuguese Directorate-General of Health (DGS). Levels of Health Literacy; DGS: Lisbon, Portugal, 2021; Available online: https://www.dgs.pt/documentos-e-publicacoes/estudo-apresenta-nivel-de-literacia-em-saude-dos-portugueses-pdf.aspx (accessed on 12 July 2022).
- Yuen, E.; Knight, T.; Ricciardelli, L.; Burney, S. Health literacy of caregivers of adult care recipients: A systematic scoping review. Health Soc. Care Community 2018, 26, e191–e206. [Google Scholar] [CrossRef] [PubMed]
- Fields, B.; Rodakowski, J.; James, A.; Beach, S. Caregiver health literacy predicting healthcare communication and system navigation difficulty. Fam. Syst. Health 2018, 36, 482–492. [Google Scholar] [CrossRef]
- Häikio, K.; Cloutier, D.; Rugkåsa, J. Is health literacy of family carers associated with carer burden, quality of life, and time spent on informal care for older persons living with dementia? PLoS ONE 2020, 15, e0241982. [Google Scholar] [CrossRef] [PubMed]
- Creswell, J. Research Design: Qualitative, Quantitative, and Mixed Methods Approaches, 4th ed.; Sage: Thousand Oaks, CA, USA, 2014. [Google Scholar]
- Fortin, M.; Cotê, J.; Filion, F. Fundamentos e Etapas do Processo de Investigação; Lusociência: Loures, Lisbon, 2009. [Google Scholar]
- Nunes, L.; Sorensen, K. The European health literacy survey (HLS-EU) and its Portuguese cultural adaptation and validation (HLS-PT). Aten. Primaria 2013, 45, 47. Available online: https://novaresearch.unl.pt/en/publications/the-european-health-literacy-survey-hls-eu-and-its-portuguese-cul (accessed on 12 July 2022).
- Espanha, R.; Ávila, P.; Mendes, R. Literacia em Saúde em Portugal-Relatório Síntese; Calouste Gulbenkian Foundation: Lisbon, Portugal, 2016; Available online: https://gulbenkian.pt/publications/literacia-em-saude-em-portugal-relatorio-sintese/ (accessed on 12 July 2022).
- Topp, C.; Østergaard, S.; Søndergaard, S.; Bech, P. The WHO-5 well-being index: A systematic review of the literature. Psychother. Psychosom. 2015, 84, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Marques, J. Literacia em Saúde: Avaliação Através do European Health Literacy Survey em Português Num Serviço de Internamento hospitalar. Master’s Thesis, ISCTE, Lisbon, Portugal, 2015. Available online: https://repositorio.iscte-iul.pt/bitstream/10071/11458/1/Tese%20-%20Literacia%20em%20Sau%CC%81de.pdf (accessed on 12 July 2022).
- HLS-EU Consortium. Comparative Report of Health Literacy in Eight eu Member States: The European Health Literacy Survey HLS-EU, 2nd ed.; HLS-EU Consortium: Vienna, Austria, 2012; Available online: http://www.health-literacy.eu (accessed on 12 July 2022).
- Pedro, A.; Amaral, O.; Escoval, A. Health Literacy, from Data to Action: Translation, Validation and Application of the European Health Literacy Survey in Portugal. Rev. Port. De Saúde Pública 2016, 34, 259–275. [Google Scholar] [CrossRef]
- Mahoney, F.; Barthel, D. Functional evaluation: The Barthel Index. Md. State Med J. 1965, 14, 61–65. [Google Scholar] [PubMed]
- Araújo, F.; Ribeiro, J.; Oliveira, A.; Pinto, C. Validation of the Barthel Index in a sample of non-institutionalized elderly. Rev. Port. De Saúde Pública 2007, 25, 59–66. [Google Scholar]
- Lawton, M.; Brody, M. Assessment of older people: Self maintaining and instrumental activities of daily living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Araújo, F.; Pais-Ribeiro, J.; Oliveira, A.; Pinto, C.; Martins, T. Validação da escala de Lawton & Brody numa amostra de idosos não institucionalizados. In Actas do 7° Congresso Nacional de Psicologia da Saúde; Leal, I., Pais-Ribeiro, J., Silva, I., Marques, S., Eds.; ISPA: Porto, Lisboa, 2008; pp. 217–220. Available online: https://sigarra.up.pt/fpceup/pt/pub_geral.pub_view?pi_pub_base_id=83826 (accessed on 12 July 2022).
- Arriaga, M.; Freitas, G.; Costa, A.; Ribeiro da Silva, C.; Mata, F.; dos Santos, B.; Chaves da Silva, N. Health Literacy Action Plan: The Portuguese Implementation. Eur. J. Public Health 2020, 30, 512. [Google Scholar] [CrossRef]
- Ribeiro, O.; Pires, C.; Brandão, D.; Teixeira, L. Cuidar de Quem Cuida: Sumário Executivo de Avaliação Final; UNIFAI/ICBAS-UP: Porto, Portugal, 2013; Available online: https://cuidardequemcuida.com/wp-content/uploads/2019/05/relat%C3%B3rio-s%C3%ADntese_fase-1.pdf.scml.pt (accessed on 12 July 2022).
- Data on a Study about the Profile of Informal Caregivers Using the Centre for Education, Training and Certification. Available online: http://www.scml.pt/media/noticias/vivo-para-cuidar-de-ti (accessed on 12 July 2022).
- Eurocarers; IRCCS-INRCA. Impact of the COVID-19 Outbreak on Informal Carers Across Europe; Eurocarers: Brussels, Belgium, 2021; Available online: https://eurocarers.org/publications/impact-of-the-covid-19-outbreak-on-informal-carers-across-europe/ (accessed on 12 July 2022).
- Teixeira, A.; Alves, B.; Augusto, B.; Fonseca, C.; Nogueira, J.; Almeida, M.; Matias, M.; Ferreira, M.; Narigão, M.; Lourenço, R.; et al. Medidas de Intervenção Junto dos Cuidadores Informais; Gabinete de Estratégia e Planeamento do Ministério do Trabalho, Solidariedade e Segurança Social: Lisbon, Portugal, 2017; Available online: https://app.parlamento.pt/webutils/docs/doc.pdf?path=6148523063446f764c324679626d56304c334e706447567a4c31684a53556c4d5a5763765130394e4c7a4577513152545579394562324e31625756756447397a51574e3061585a705a47466b5a554e7662576c7a633246764c7a597a4f54646c5a6a63784c5449304d7a63744e445a6b5a4330344e444e6a4c57526a4e7a5a695a5749334e5451354e6935775a47593d&fich=697ef71-2437-46dd-843c-dc76beb75496.pdf&Inline=true (accessed on 12 July 2022).
- Embracing Carers. Embracing the Critical Role of Carers around the World: White Paper and Action Plan; Embracing Carers, Merck KGaA: Darmstadt, Germany, 2017; Available online: https://www.embracingcarers.com/content/dam/web/healthcare/corporate/embracing-carers/media/infographics/us/Merck%20KGaA%20Embracing%20Carers_White%20Paper%20Flattened.pdf (accessed on 12 July 2022).
- OECD. Health Literacy for People-Centred Care: Where Do OECD Countries Stand? OECD: Paris, France, 2018. [Google Scholar] [CrossRef]
- Wittenberg, E.; Goldsmith, J.; Ferrell, B.; Ragan, B. Promoting improved family caregiver health literacy: Evaluation of caregiver communication resources. Psycho-Oncol. 2017, 26, 935–942. [Google Scholar] [CrossRef] [PubMed]
- Verma, M.; Saldanha, C.; Ellis, U.; Sattar, S.; Haase, K. eHealth literacy among older adults living with cancer and their caregivers: A scoping review. J. Geriatr. Oncol. 2022, 13, 555–562. [Google Scholar] [CrossRef] [PubMed]
- Cianfrocca, C.; Camponnetto, V.; Donati, D.; Lancia, L.; Tartaglini, D.; Stasio, E. The effects of a multidisciplinary education course on the burden, health literacy and needs of family caregivers. Appl. Nurs. Res. 2018, 44, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Kampouroglou, G.; Velonaki, V.-S.; Pavlopoulou, I.; Kosmopoulos, M.; Kouvas, N.; Drakou, E.; Skoutelis, N.; Spinos, D.; Tsagkaris, S.; Tsoumakas, K. Health Literacy of Parents/Caregivers of Paediatric Surgical Patients: A Study on 1000 Individuals. Afr. J. Paediatr. Surg. 2021, 18, 85–89. [Google Scholar] [CrossRef] [PubMed]
- ine.pt. Platform for Census Results Dissemination. Available online: https://www.ine.pt/scripts/db_censos_2021.html (accessed on 12 July 2022).
- Zhou, Z.; Wang, Y.; Feng, P.; Li, T.; Tebes, J.K.; Luan, R.; Yu, Y. Associations of Caregiving Knowledge and Skills with Caregiver Burden, Psychological Well-Being, and Coping Styles Among Primary Family Caregivers of People Living with Schizophrenia in China. Front. Psychiatry 2021, 12, 631420. [Google Scholar] [CrossRef] [PubMed]
- Hu, C.; Kung, S.; Rummans, T.; Clark, M.; Lapid, M. Reducing caregiver stress with internet-based interventions: A systematic review of open-label and randomized controlled trials. J. Am. Med. Inform. Assoc. 2015, 22, e194–e209. [Google Scholar] [CrossRef] [PubMed] [Green Version]




| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Informal caregiver aged 18 years old or above; Informal caregiver assuming care to a care receiver living in Lisbon county, Portugal; Informal caregiver assuming care to a person with care recipient in a home setting; Informal caregiver assuming care of a person with limitation in at least one dimension of self-care. | Informal caregiver aged 17 years old or below; Informal caregiver living outside the Lisbon county or in other country; Informal caregiver assuming care to a person with dependence in community settings or residential facilities; Formal caregiver assuming care to a person in need; Informal caregiver assuming care to a child without a chronic or disability condition. Person assuming care to another person without limitations of self-care or daily living activities. |
| According to This Study, the Informal Caregiver is Most Frequently |
|---|
| a woman aged, in average, 62 years old, married, with a university-level degree, who is retired and earns a monthly financial income between 665 and 1270 euros. |
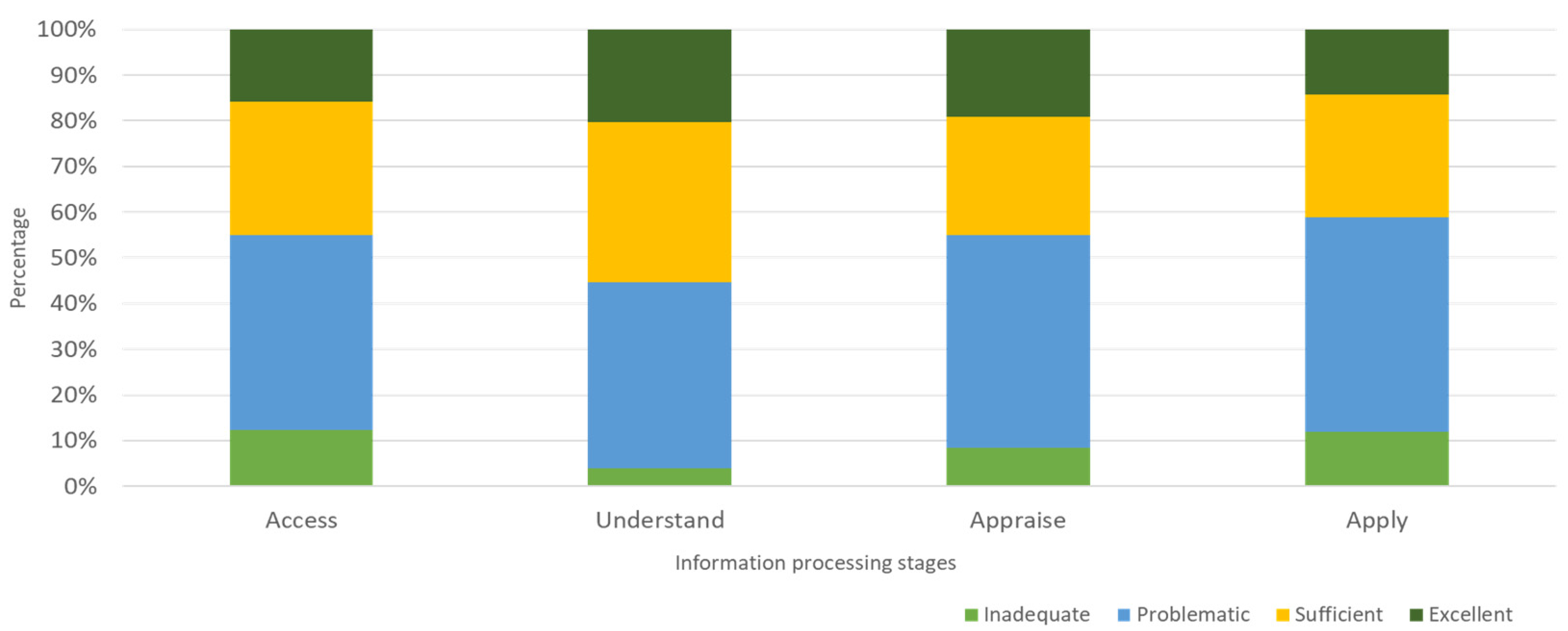
| Health Literacy (HLS-EU-PT) Scores by Information Processing Stages | Statistics | ||
|---|---|---|---|
| Mean | Standard Deviation | Median | |
| Access | 33.7 | 8.4 | 33.3 |
| Understanding | 36.6 | 7.3 | 34.9 |
| Appraisal | 34.7 | 8.0 | 33.3 |
| Use | 33.3 | 8.1 | 33.3 |
| Covariate/Factor | Statistic Test | p Value |
|---|---|---|
| Gender | Pearson’s Chi-Square | 0.470 |
| Age | ANOVA | 0.046 |
| Education | Fisher’s Exact Test (Monte Carlo approach, IC 95%) | 0.001 |
| Barthel Index for Activities of Daily Living (score) | Pearson’s correlation coefficient | 0.515 |
| Lawton & Brody Instrumental Activities of Daily Living (score) | Kruskal–Wallis | 0.222 |
| Financial status | ANOVA | 0.228 |
| Caregiver transition | Kruskal–Wallis | 0.291 |
| Family/friends support | Mann–Whitney | 0.091 |
| Professional support | Student’s t | 0.764 |
| Private support | Student’s t | 0.113 |
| Knowledge about community resources | Student’s t | 0.006 |
| Demand for health services | Pearson’s Chi-Square | 0.793 |
| Demand for social services | Student’s t | 0.691 |
| Inclusion in caregiver’s support program | Fisher’s Exact Test (Monte Carlo approach, IC 95%) | 0.103 |
| Knowledge about the statute of the informal caregiver | Pearson’s Chi-Square | 0.103 |
| WHO Well-Being Index (score) | ANOVA/Pearson’s correlation coefficient | 0.001 |
| Health Literacy Categories (HLS-EU-PT) | Education Level | |||||||
|---|---|---|---|---|---|---|---|---|
| Does not know how to read and write | Knows how to read and write | 4 years (primary school) | 6 years (junior school) | 9 years (basic school) | 12 years (high school) | Higher education degree | Other | |
| Inadequate | 2 | 0 | 7 | 0 | 1 | 2 | 3 | 0 |
| Problematic | 0 | 2 | 9 | 5 | 13 | 23 | 42 | 1 |
| Sufficient | 1 | 0 | 15 | 4 | 14 | 26 | 39 | 0 |
| Excellent | 0 | 1 | 2 | 1 | 4 | 7 | 34 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costa, A.; Loura, D.d.S.; Nogueira, P.; Melo, G.; Gomes, I.; Ferraz, I.; Viegas, L.; Henriques, M.A. Informal Caregivers’ Health Literacy in Lisbon, Portugal: A Profile for Health Promotion Prioritization. Geriatrics 2022, 7, 92. https://doi.org/10.3390/geriatrics7050092
Costa A, Loura DdS, Nogueira P, Melo G, Gomes I, Ferraz I, Viegas L, Henriques MA. Informal Caregivers’ Health Literacy in Lisbon, Portugal: A Profile for Health Promotion Prioritization. Geriatrics. 2022; 7(5):92. https://doi.org/10.3390/geriatrics7050092
Chicago/Turabian StyleCosta, Andreia, David de Sousa Loura, Paulo Nogueira, Graça Melo, Idalina Gomes, Isabel Ferraz, Laura Viegas, and Maria Adriana Henriques. 2022. "Informal Caregivers’ Health Literacy in Lisbon, Portugal: A Profile for Health Promotion Prioritization" Geriatrics 7, no. 5: 92. https://doi.org/10.3390/geriatrics7050092