
A Biopsychosocial Model of Mealtime Management in Persons with Dementia, an Asset-Based Approach to Patient-Centered Care


{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Current Models That Can Inform Mealtime Management
2.1. World Health Organization’s International Classification of Function, Disability, and Health
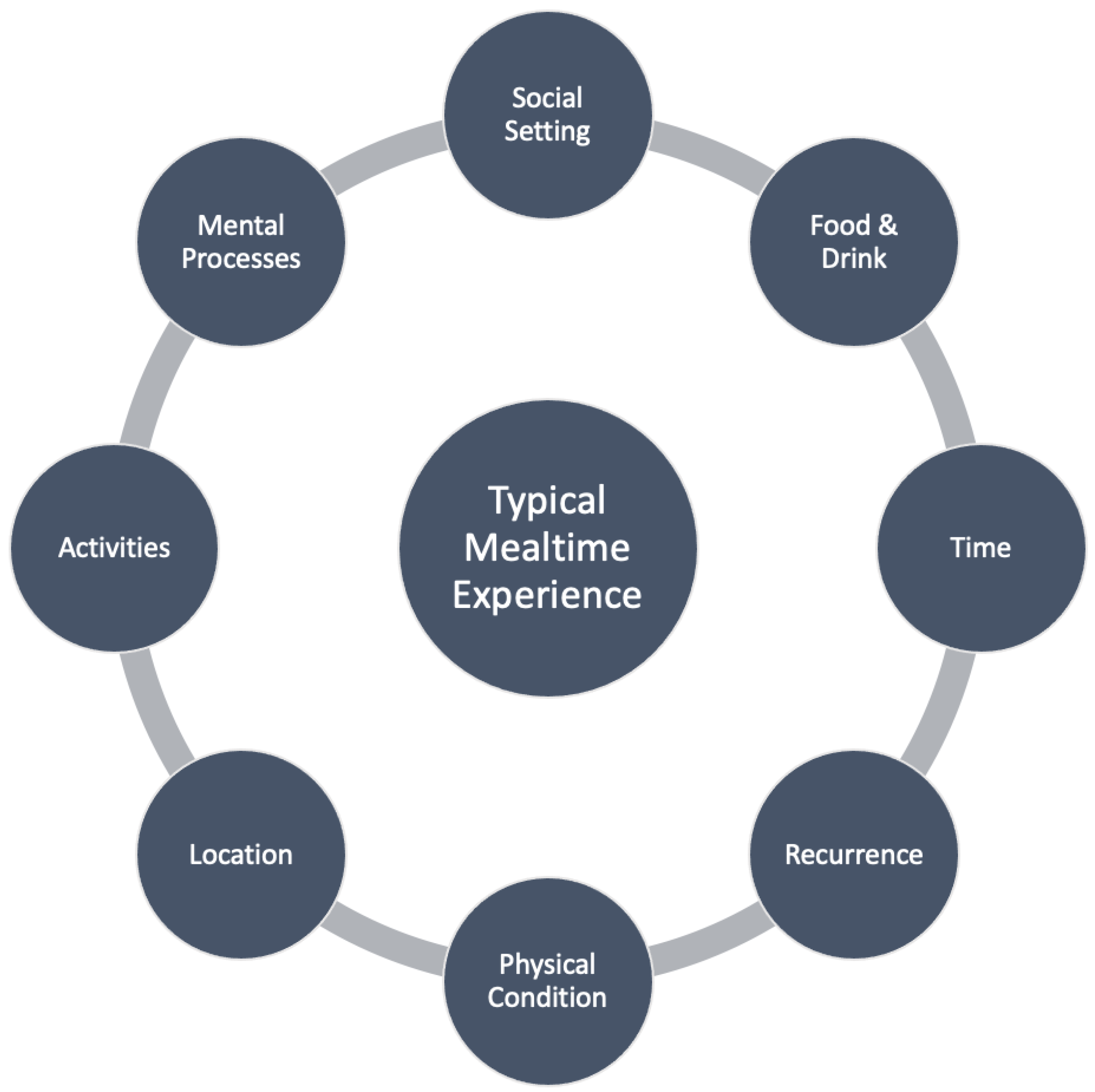
2.2. Bisogni et al.’s Framework of Typical Mealtime Processes
2.3. Historical Perspectives of the Biopsychosocial Model of Patient Care
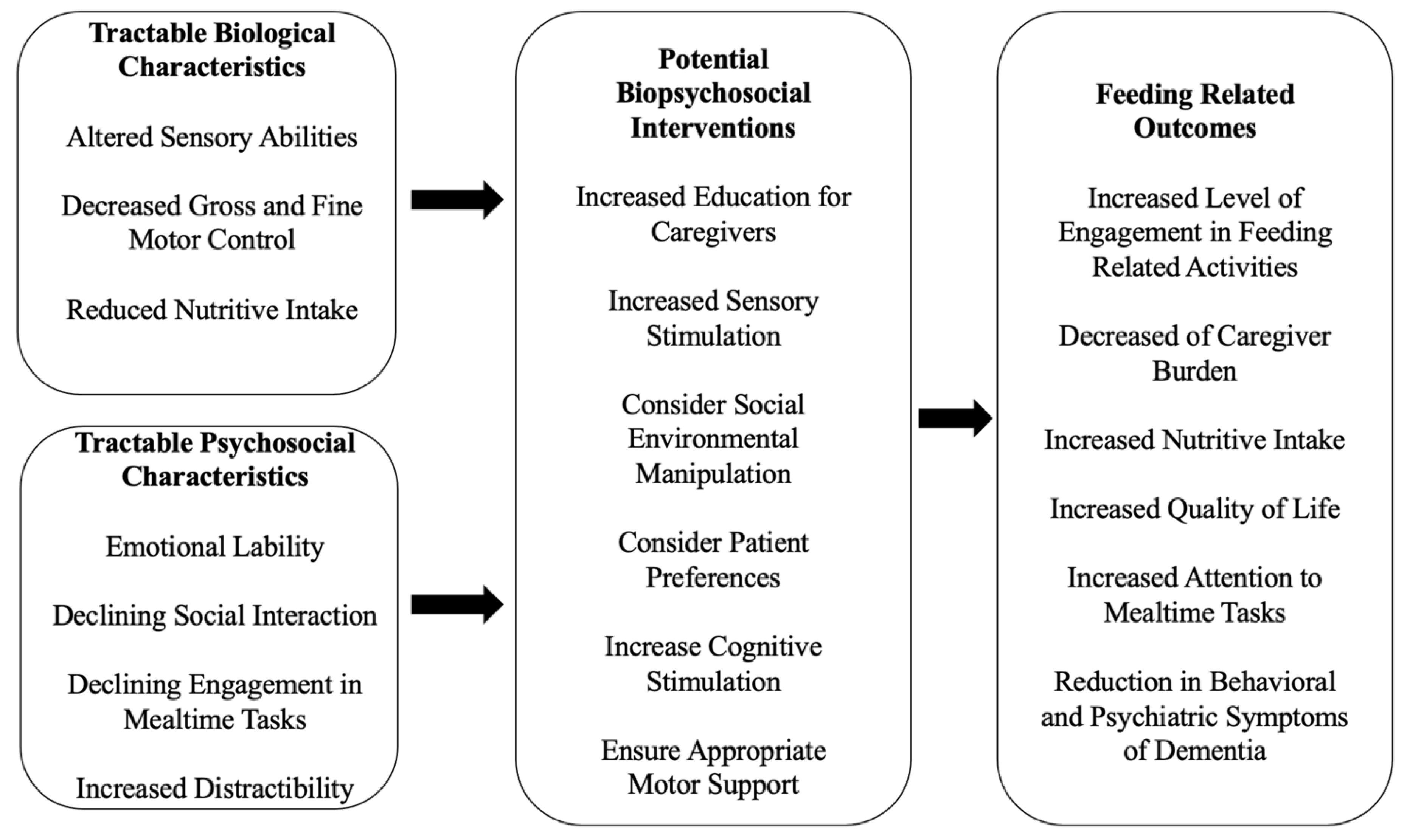
3. A Biopsychosocial Model of Mealtime Management in PWD
3.1. Tractable Characteristics
3.1.1. Tractable Biological Characteristics
3.1.2. Tractable Psychosocial Characteristics
3.2. Biopsychosocial Interventions and Outcomes
3.2.1. Caregiver Education
3.2.2. Sensory Stimulation
3.2.3. Social Environment Manipulation
3.2.4. Patient Preferences
3.2.5. Cognitive Stimulation
3.2.6. Adaptive Motor Support
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Administration of Community Living. 2019 Profile of Older Americans; Administration of Community Living: Washington, DC, USA, 2020. [Google Scholar]
- U. C. Bureau. “2012 National Population Projections Table: Table 2. Projections of the Population by Selected Age Groups and Sex for the United States: 2015 to 2060,” Washington D.C.; 2012. Available online: https://www.census.gov/data/tables/2012/demo/popproj/2012-summary-tables.html (accessed on 13 August 2020).
- Jin, K.; Simpkins, J.W.; Ji, X.; Leis, M.; Stambler, I. The Critical Need to Promote Research of Aging and Aging-related Diseases to Improve Health and Longevity of the Elderly Population. Aging Dis. 2015, 6, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alzheimer’s Association. 2014 Alzheimer’s disease facts and figures. Alzheimer’s Dement. 2014, 10, e47–e92. [Google Scholar] [CrossRef] [Green Version]
- Prince, M.; Comas-Herrera, A.; Knapp, M.; Guerchet, M.; Karagiannidou, M. World Alzheimer Report 2016: Improving Healthcare for People Living with Dementia: Coverage, Quality and Costs Now and in the Future. 2016. Available online: http://www.alz.co.uk/ (accessed on 2 September 2020).
- Ismail, Z.; Smith, E.E.; Geda, Y.; Sultzer, D.; Brodaty, H.; Smith, G.; Agüera-Ortiz, L.; Sweet, R.; Miller, D.; Lyketsos, C.G.; et al. Neuropsychiatric symptoms as early manifestations of emergent dementia: Provisional diagnostic criteria for mild behavioral impairment. Alzheimer’s Dement. 2015, 12, 195–202. [Google Scholar] [CrossRef]
- Leder, S.B.; Suiter, D.M. An Epidemiologic Study on Aging and Dysphagia in the Acute Care Hospitalized Population: 2000–2007. Gerontology 2009, 55, 714–718. [Google Scholar] [CrossRef] [PubMed]
- Alagiakrishnan, K.; Bhanji, R.A.; Kurian, M. Evaluation and management of oropharyngeal dysphagia in different types of dementia: A systematic review. Arch. Gerontol. Geriatr. 2013, 56, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Espinosa-Val, M.C.; Martín-Martínez, A.; Graupera, M.; Arias, O.; Elvira, A.; Cabré, M.; Palomera, E.; Bolívar-Prados, M.; Clavé, P.; Ortega, O. Prevalence, Risk Factors, and Complications of Oropharyngeal Dysphagia in Older Patients with Dementia. Nutrients 2020, 12, 863. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- White, G.N.; O’Rourke, F.; Ong, B.S.; Cordato, D.J.; Chan, D.K.Y. Dysphagia: Causes, assessment, treatment, and management. Geriatrics 2008, 63, 15–20. [Google Scholar] [PubMed]
- Easterling, C.S.; Robbins, E. Dementia and Dysphagia. Geriatr. Nurs. 2008, 29, 275–285. [Google Scholar] [CrossRef] [PubMed]
- Namasivayam, A.M.; Steele, C.M. Malnutrition and Dysphagia in Long-Term Care: A Systematic Review. J. Nutr. Gerontol. Geriatr. 2015, 34, 1–21. [Google Scholar] [CrossRef]
- Ebihara, S.; Sekiya, H.; Miyagi, M.; Ebihara, T.; Okazaki, T. Dysphagia, dystussia, and aspiration pneumonia in elderly people. J. Thorac. Dis. 2016, 8, 632–639. [Google Scholar] [CrossRef]
- Chen, P.-H.; Golub, J.S.; Hapner, E.; Johns, M.M. Prevalence of Perceived Dysphagia and Quality-of-Life Impairment in a Geriatric Population. Dysphagia 2009, 24, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Jones, E.; Speyer, R.; Kertscher, B.; Denman, D.; Swan, K.; Cordier, R. Health-Related Quality of Life and Oropharyngeal Dysphagia: A Systematic Review. Dysphagia 2018, 33, 141–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plowman-Prine, E.K.; Sapienza, C.M.; Okun, M.; Bs, S.L.P.; Jacobson, C.; Wu, S.S.; Rosenbek, J.C. The relationship between quality of life and swallowing in Parkinson’s disease. Mov. Disord. 2009, 24, 1352–1358. [Google Scholar] [CrossRef] [Green Version]
- Kostanjsek, N. Use of The International Classification of Functioning, Disability and Health (ICF) as a conceptual framework and common language for disability statistics and health information systems. BMC Public Health 2011, 11, S3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. How to use the ICF A Practical Manual for Using the International Classification of Functioning, Disability and Health (ICF) Exposure Draft for Comment; World Health Organization: Geneva, Switzerlanad, 2013. [Google Scholar]
- Hopkins, T.; Rippon, S.; Tait, M. Head, Hands and Heart: Asset-Based Approaches in Health Care A Review of the Conceptual Evidence and Case Studies of Asset-Based Approaches in Health, Care and Wellbeing, London. 2015. Available online: www.alignedconsultancy.co.uk (accessed on 11 November 2021).
- Bisogni, C.A.; Falk, L.W.; Madore, E.; Blake, C.E.; Jastran, M.; Sobal, J.; Devine, C.M. Dimensions of everyday eating and drinking episodes. Appetite 2007, 48, 218–231. [Google Scholar] [CrossRef]
- Engel, G. The Need for a New Medical Model: A Challenge for Biomedicine. Science 1977, 196, 129–136. [Google Scholar] [CrossRef]
- Cohen-Mansfield, J. Heterogeneity in Dementia: Challenges and Opportunities: Alzheimer Disease & Associated Disorders. Alzheimer Dis. Assoc. Disord. 2000, 14, 60–63. [Google Scholar] [PubMed]
- Spector, A.; Orrell, M. Using a biopsychosocial model of dementia as a tool to guide clinical practice. Int. Psychogeriatrics 2010, 22, 957–965. [Google Scholar] [CrossRef] [PubMed]
- Gitlin, L.N.; Piersol, C.; Hodgson, N.; Marx, K.; Roth, D.L.; Johnston, D.; Samus, Q.; Pizzi, L.; Jutkowitz, E.; Lyketsos, C.G. Reducing neuropsychiatric symptoms in persons with dementia and associated burden in family caregivers using tailored activities: Design and methods of a randomized clinical trial. Contemp. Clin. Trials 2016, 49, 92–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duxbury, J.; Pulsford, D.; Hadi, M.; Sykes, S. Staff and relatives’ perspectives on the aggressive behaviour of older people with dementia in residential care: A qualitative study. J. Psychiatr. Ment. Health Nurs. 2012, 20, 792–800. [Google Scholar] [CrossRef]
- Kitwood, T. Dementia Reconsidered: The Person Comes First; Open University Press: Berkshire, UK, 1997. [Google Scholar]
- Aliev, G.; Ashraf, G.; Kaminsky, Y.G.; Sheikh, I.A.; Sudakov, S.; Yakhno, N.; Benberin, V.V.; Bachurin, S.O. Implication of the Nutritional and Nonnutritional Factors in the Context of Preservation of Cognitive Performance in Patients with Dementia/Depression and Alzheimer Disease. Am. J. Alzheimer’s Dis. Other Dement. 2013, 28, 660–670. [Google Scholar] [CrossRef] [PubMed]
- de Paula, J.J.; Albuquerque, M.R.; Lage, G.M.; Bicalho, M.A.; Romano-Silva, M.A.; Malloy-Diniz, L.F. Impairment of fine motor dexterity in mild cognitive impairment and Alzheimer’s disease dementia: Association with activities of daily living. Rev. Bras. Psiquiatr. 2016, 38, 235–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drenth, H.; Zuidema, S.; Bautmans, I.; Marinelli, L.; Kleiner, G.; Hobbelen, H. Paratonia in Dementia: A Systematic Review. J. Alzheimer’s Dis. 2020, 78, 1615–1637. [Google Scholar] [CrossRef]
- Bautmans, I.; Demarteau, J.; Cruts, B.; Lemper, J.-C.; Mets, T. Dysphagia in elderly nursing home residents with severe cognitive impairment: Feasibility and effects of cervical spine mobilization. J. Rehabil. Med. 2008, 40, 755–760. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taragano, F.E.; Allegri, R.F.; Krupitzki, H.; Sarasola, D.R.; Serrano, C.M.; Loñ, L.; Lyketsos, C.G. Mild Behavioral Impairment and Risk of Dementia: A Prospective Cohort Study of 358 Patients. J. Clin. Psychiatry 2009, 70, 584–592. [Google Scholar] [CrossRef] [Green Version]
- Resnick, H.E.; Fries, B.E.; Verbrugge, L.M. Windows to Their World: The Effect of Sensory Impairments on Social Engagement and Activity Time in Nursing Home Residents. J. Gerontol. Soc. Sci. 1997, 52, 35–144. [Google Scholar] [CrossRef] [Green Version]
- Kolanowski, A.; Litaker, M. Social Interaction, Premorbid Personality, and Agitation in Nursing Home Residents with Dementia. Arch. Psychiatr. Nurs. 2006, 20, 12–20. [Google Scholar] [CrossRef]
- Lee, K.H.; Boltz, M.; Lee, H.; Algase, D.L. Does Social Interaction Matter Psychological Well-Being in Persons with Dementia? Am. J. Alzheimer’s Dis. Other Dement. 2017, 32, 207–212. [Google Scholar] [CrossRef] [Green Version]
- Cohen-Mansfield, J.; Dakheel-Ali, M.; Marx, M.S. Engagement in Persons with Dementia: The Concept and Its Measurement. Am. J. Geriatr. Psychiatry 2009, 17, 299–307. [Google Scholar] [CrossRef] [Green Version]
- Keller, H.H.; Martin, L.S.; Dupuis, S.; Reimer, H.; Genoe, R. Strategies to support engagement and continuity of activity during mealtimes for families living with dementia; a qualitative study. BMC Geriatr. 2015, 15, 119. [Google Scholar] [CrossRef]
- Liu, W.; Perkhounkova, E.; Williams, K.; Batchelor, M.; Hein, M. Food intake is associated with verbal interactions between nursing home staff and residents with dementia: A secondary analysis of videotaped observations. Int. J. Nurs. Stud. 2020, 109, 103654. [Google Scholar] [CrossRef] [PubMed]
- Smits, L.L.; van Harten, A.C.; Pijnenburg, Y.A.L.; Koedam, E.L.G.E.; Bouwman, F.H.; Sistermans, N.; Reuling, I.E.W.; Prins, N.D.; Lemstra, A.W.; Scheltens, P.; et al. Trajectories of cognitive decline in different types of dementia. Psychol. Med. 2014, 45, 1051–1059. [Google Scholar] [CrossRef] [Green Version]
- Nell, D.; Neville, S.; Bellew, R.; O’Leary, C.; Beck, K.L. Factors affecting optimal nutrition and hydration for people living in specialised dementia care units: A qualitative study of staff caregivers’ perceptions. Australas. J. Ageing 2016, 35, E1–E6. [Google Scholar] [CrossRef] [Green Version]
- Anderson, J.G.; Rose, K.M.; Taylor, A.G. A descriptive study of the nutrition-related concerns of caregivers of persons with Dementia. J. Aging Res. Lifestyle 2016, 5, 1–6. [Google Scholar] [CrossRef]
- Salva, A.; Andrieu, S.; Fernandez, E.; Schiffrin, E.J.; Moulin, J.; Decarli, B.; Rojano-i-Luque, X.; Guigoz, Y.; Vellas, B.; The Nutrialz Group. Health and nutrition promotion program for patients with dementia (NutriAlz): Cluster randomized trial. J. Nutr. Health Aging 2011, 15, 822–830. [Google Scholar] [CrossRef] [PubMed]
- Staedtler, A.V.; Nunez, D. Nonpharmacological Therapy for the Management of Neuropsychiatric Symptoms of Alzheimer’s Disease: Linking Evidence to Practice. Worldviews Evid. Based Nurs. 2015, 12, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Fischer, C.E.; Ismail, Z.; A Schweizer, T. Impact of neuropsychiatric symptoms on caregiver burden in patients with Alzheimer’s disease. Neurodegener. Dis. Manag. 2012, 2, 269–277. [Google Scholar] [CrossRef]
- Paller, K.A.; Creery, J.; Florczak, S.M.; Weintraub, S.; Mesulam, M.-M.; Reber, P.J.; Kiragu, J.; Rooks, J.; Safron, A.; Morhardt, D.; et al. Benefits of Mindfulness Training for Patients with Progressive Cognitive Decline and Their Caregivers. Am. J. Alzheimer’s Dis. Other Dement. 2015, 30, 257–267. [Google Scholar] [CrossRef] [Green Version]
- Wright, L.; Hickson, M.; Frost, G. Eating together is important: Using a dining room in an acute elderly medical ward increases energy intake. J. Hum. Nutr. Diet. 2006, 19, 23–26. [Google Scholar] [CrossRef] [PubMed]
- Batchelor-Murphy, M.A.P.F. Supportive handfeeding in dementia: Establishing evidence for three handfeeding techniques. In Proceedings of the Sigma Theta Tau International Honor Society of Nursing 27th International Research Congress, Cape Town, South Africa, 24 July 2016. [Google Scholar]
- Batchelor-Murphy, M.K.; McConnell, E.S.; Amella, E.J.; Anderson, R.A.; Bales, C.W.; Silva, S.; Barnes, A.; Beck, C.; Colon-Emeric, C.S. Experimental Comparison of Efficacy for Three Handfeeding Techniques in Dementia. J. Am. Geriatr. Soc. 2017, 65, e89–e94. [Google Scholar] [CrossRef]
- Wegner, D.M.; Sparrow, B.; Winerman, L. Vicarious Agency: Experiencing Control Over the Movements of Others. J. Pers. Soc. Psychol. 2004, 86, 838–848. [Google Scholar] [CrossRef]
- Hicks-Moore, S.L. Relaxing Music at Mealtime in Nursing Homes. J. Gerontol. Nurs. 2005, 31, 26–32. [Google Scholar] [CrossRef]
- Thomas, D.W.; Smith, M. The Effect of Music on Caloric Consumption Among Nursing Home Residents with Dementia of the Alzheimer’s Type. Act. Adapt. Aging 2009, 33, 1–16. [Google Scholar] [CrossRef]
- Edwards, N.; Beck, A.M. The Influence of Aquariums on Weight in Individuals with Dementia. Alzheimer Dis. Assoc. Disord. 2013, 27, 379–383. [Google Scholar] [CrossRef]
- Dunne, T.E.; Neargarder, S.A.; Cipolloni, P.; Cronin-Golomb, A. Visual contrast enhances food and liquid intake in advanced Alzheimer’s disease. Clin. Nutr. 2004, 23, 533–538. [Google Scholar] [CrossRef] [PubMed]
- Sulmont-Rossé, C.; Gaillet, M.; Raclot, C.; Duclos, M.; Servelle, M.; Chambaron, S. Impact of Olfactory Priming on Food Intake in an Alzheimer’s Disease Unit. J. Alzheimer’s Dis. 2018, 66, 1497–1506. [Google Scholar] [CrossRef]
- Liu, W.; Jao, Y.; Williams, K. Factors influencing the pace of food intake for nursing home residents with dementia: Resident characteristics, staff mealtime assistance and environmental stimulation. Nurs. Open 2019, 6, 772–782. [Google Scholar] [CrossRef] [Green Version]
- Curle, L.; Keller, H. Resident interactions at mealtime: An exploratory study. Eur. J. Ageing 2010, 7, 189–200. [Google Scholar] [CrossRef] [Green Version]
- Burdick, R.; Lin, T.-F.; Shune, S.E. Visual Modeling: A Socialization-Based Intervention to Improve Nutritional Intake Among Nursing Home Residents. Am. J. Speech-Lang. Pathol. 2021, 30, 2202–2213. [Google Scholar] [CrossRef]
- Nijs, K.A.N.D.; De Graaf, C.; Kok, F.J.; Van Staveren, W.A. Effect of family style mealtimes on quality of life, physical performance, and body weight of nursing home residents: Cluster randomised controlled trial. BMJ 2006, 332, 1180–1184. [Google Scholar] [CrossRef]
- HReimer, H.D.; Keller, H.H. Mealtimes in Nursing Homes: Striving for Person-Centered Care. J. Nutr. Elder. 2009, 28, 327–347. [Google Scholar] [CrossRef]
- Shune, S.E.; Linville, D. Understanding the dining experience of individuals with dysphagia living in care facilities: A grounded theory analysis. Int. J. Nurs. Stud. 2019, 92, 144–153. [Google Scholar] [CrossRef]
- Mol, A. The Logic of Care: Health and the Problem of Patient Choice, 1st ed.; Routledge Taylor & Francis Group: London, UK, 2008. [Google Scholar]
- Shune, S.; Barewal, R. Redefining the value of snacks for nursing home residents: Bridging psychosocial and nutritional needs. Geriatr. Nurs. 2022, 44, 39–47. [Google Scholar] [CrossRef]
- Brush, J.A.; Camp, C.J. Using Spaced Retrieval as an Intervention During Speech-Language Therapy. Clin. Gerontol. 1998, 19, 51–64. [Google Scholar] [CrossRef]
- Lin, L.-C.; Huang, Y.-J.; Su, S.-G.; Watson, R.; Tsai, B.W.J.; Wu, S.-C. Using spaced retrieval and Montessori-based activities in improving eating ability for residents with dementia. Int. J. Geriatr. Psychiatry 2010, 25, 953–959. [Google Scholar] [CrossRef] [PubMed]
- Bourgeois, M.S.; Camp, C.; Rose, M.; White, B.; Malone, M.; Carr, J.; Rovine, M. A comparison of training strategies to enhance use of external aids by persons with dementia. J. Commun. Disord. 2003, 36, 361–378. [Google Scholar] [CrossRef]
- Booth, S.; Zizzo, G.; Robertson, J.; Goodwin-Smith, I. Positive Interactive Engagement (PIE): A pilot qualitative case study evaluation of a person-centred dementia care programme based on Montessori principles. Dementia 2018, 19, 975–991. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.-C.; Huang, Y.-J.; Watson, R.; Wu, S.-C.; Lee, Y.-C. Using a Montessori method to increase eating ability for institutionalised residents with dementia: A crossover design. J. Clin. Nurs. 2011, 20, 3092–3101. [Google Scholar] [CrossRef] [PubMed]
- Cartwright, J.; Roberts, K.; Oliver, E.; Bennett, M.; Whitworth, A. Montessori mealtimes for dementia: A pathway to person-centred care. Dementia 2022, 21, 1098–1119. [Google Scholar] [CrossRef]
- Aguirre, E.; Stott, J.; Charlesworth, G.; Noone, D.; Payne, J.; Patel, M.; Spector, A. Mindfulness-Based Cognitive Therapy (MBCT) programme for depression in people with early stages of dementia: Study protocol for a randomised controlled feasibility study. Pilot Feasibility Stud. 2017, 3, 28. [Google Scholar] [CrossRef] [PubMed]
- Rogus-Pulia, N.; Malandraki, G.A.; Johnson, S.; Robbins, J. Understanding Dysphagia in Dementia: The Present and the Future. Curr. Phys. Med. Rehabilitation Rep. 2015, 3, 86–97. [Google Scholar] [CrossRef]
- Scherder, E.; Dekker, W.; Eggermont, L. Higher-Level Hand Motor Function in Aging and (Preclinical) Dementia: Its Relationship with (Instrumental) Activities of Daily Life —A Mini-Review. Gerontology 2008, 54, 333–341. [Google Scholar] [CrossRef]
- Mse, V.K.R.; Siemionow, V.; Sahgal, V.; Yue, G.H. Effects of Aging on Hand Function. J. Am. Geriatr. Soc. 2001, 49, 1478–1484. [Google Scholar] [CrossRef]
- Carmeli, E.; Patish, H.; Coleman, R. The Aging Hand. J. Gerontol. Ser. A 2003, 58, M146–M152. [Google Scholar] [CrossRef] [Green Version]
- Chang, C.-C.; Roberts, B.L. Feeding difficulty in older adults with dementia. J. Clin. Nurs. 2008, 17, 2266–2274. [Google Scholar] [CrossRef]
- Dick, M.B.; Nielson, K.A.; Beth, R.E.; Shankle, W.; Cotman, C. Acquisition and Long-Term Retention of a Fine Motor Skill in Alzheimers-Disease. Brain Cogn. 1995, 29, 294–306. [Google Scholar] [CrossRef] [Green Version]
- Dick, M.B.; Hsieh, S.; Bricker, J.; Dick-Muehlke, C. Facilitating acquisition and transfer of a continuous motor task in healthy older adults and patients with Alzheimer’s disease. Neuropsychology 2003, 17, 202–212. [Google Scholar] [CrossRef]
- Carnaby, G.D.; Harenberg, L. What is ‘usual care’ in dysphagia rehabilitation: A survey of usa dysphagia practice patterns. Dysphagia 2013, 28, 567–574. [Google Scholar] [CrossRef]
- Sura, L.; Madhavan, A.; Carnaby, G.; Crary, M.A. Dysphagia in the elderly: Management and nutritional considerations. Clin. Interv. Aging 2012, 7, 287–298. [Google Scholar] [CrossRef] [Green Version]
- Beck, A.M.; Kjaersgaard, A.; Hansen, T.; Poulsen, I. Systematic review and evidence based recommendations on texture modified foods and thickened liquids for adults (above 17 years) with oropharyngeal dysphagia—An updated clinical guideline. Clin. Nutr. 2018, 37, 1980–1991. [Google Scholar] [CrossRef]
- Bayne, D.; Barewal, R.; Shune, S.E. Sensory-Enhanced, Fortified Snacks for Improved Nutritional Intake Among Nursing Home Residents. J. Nutr. Gerontol. Geriatr. 2022, 41, 92–101. [Google Scholar] [CrossRef]
- Hanson, L.C.; Ersek, M.; Gilliam, R.; Carey, T.S. Oral Feeding Options for People with Dementia: A Systematic Review. J. Am. Geriatr. Soc. 2011, 59, 463–472. [Google Scholar] [CrossRef]
- Papachristou, I.; Giatras, N.; Ussher, M. Impact of Dementia Progression on Food-Related Processes. Am. J. Alzheimer’s Dis. Other Dement. 2013, 28, 568–574. [Google Scholar] [CrossRef]
- Visscher, A.; Battjes-Fries, M.C.E.; van de Rest, O.; Patijn, O.N.; van der Lee, M.; Wijma-Idsinga, N.; Pot, G.K.; Voshol, P. Fingerfoods: A feasibility study to enhance fruit and vegetable consumption in Dutch patients with dementia in a nursing home. BMC Geriatr. 2020, 20, 1–8. [Google Scholar] [CrossRef]
- Pouyet, V.; Giboreau, A.; Benattar, L.; Cuvelier, G. Attractiveness and consumption of finger foods in elderly Alzheimer’s disease patients. Food Qual. Preference 2014, 34, 62–69. [Google Scholar] [CrossRef]
- Mitchell, S.L.; Teno, J.M.; Kiely, D.K.; Shaffer, M.L.; Jones, R.; Prigerson, H.G.; Volicer, L.; Givens, J.L.; Hamel, M.B. The Clinical Course of Advanced Dementia. N. Engl. J. Med. 2009, 361, 1529–1538. [Google Scholar] [CrossRef]
- Milte, R.; Shulver, W.; Killington, M.; Bradley, C.; Miller, M.; Crotty, M. Struggling to maintain individuality—Describing the experience of food in nursing homes for people with dementia. Arch. Gerontol. Geriatr. 2017, 72, 52–58. [Google Scholar] [CrossRef]
- Davis, S.; Byers, S.; Nay, R.; Koch, S. Guiding design of dementia friendly environments in residential care settings: Considering the living experiences. Dementia 2009, 8, 185–203. [Google Scholar] [CrossRef]
- Alsawy, S.; Mansell, W.; McEvoy, P.; Tai, S. What is good communication for people living with dementia? A mixed-methods systematic review. Int. Psychogeriatrics 2017, 29, 1785–1800. [Google Scholar] [CrossRef]
- McKeown, J.; Ryan, T.; Ingleton, C.; Clarke, A. ‘You have to be mindful of whose story it is’: The challenges of undertaking life story work with people with dementia and their family carers. Dementia 2013, 14, 238–256. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bayne, D.F.; Shune, S.E. A Biopsychosocial Model of Mealtime Management in Persons with Dementia, an Asset-Based Approach to Patient-Centered Care. Geriatrics 2022, 7, 112. https://doi.org/10.3390/geriatrics7050112
Bayne DF, Shune SE. A Biopsychosocial Model of Mealtime Management in Persons with Dementia, an Asset-Based Approach to Patient-Centered Care. Geriatrics. 2022; 7(5):112. https://doi.org/10.3390/geriatrics7050112
Chicago/Turabian StyleBayne, David F., and Samantha E. Shune. 2022. "A Biopsychosocial Model of Mealtime Management in Persons with Dementia, an Asset-Based Approach to Patient-Centered Care" Geriatrics 7, no. 5: 112. https://doi.org/10.3390/geriatrics7050112