
The Use of Patient Reported Outcome Measures (PROMs) 6 Months Post-Stroke and Their Association with the National Institute of Health Stroke Scale (NIHSS) on Admission to Hospital

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Trial Design
2.2. Scoring of PROMs
2.3. Missing Data
2.4. Statistical Analysis
3. Results
Statistical Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
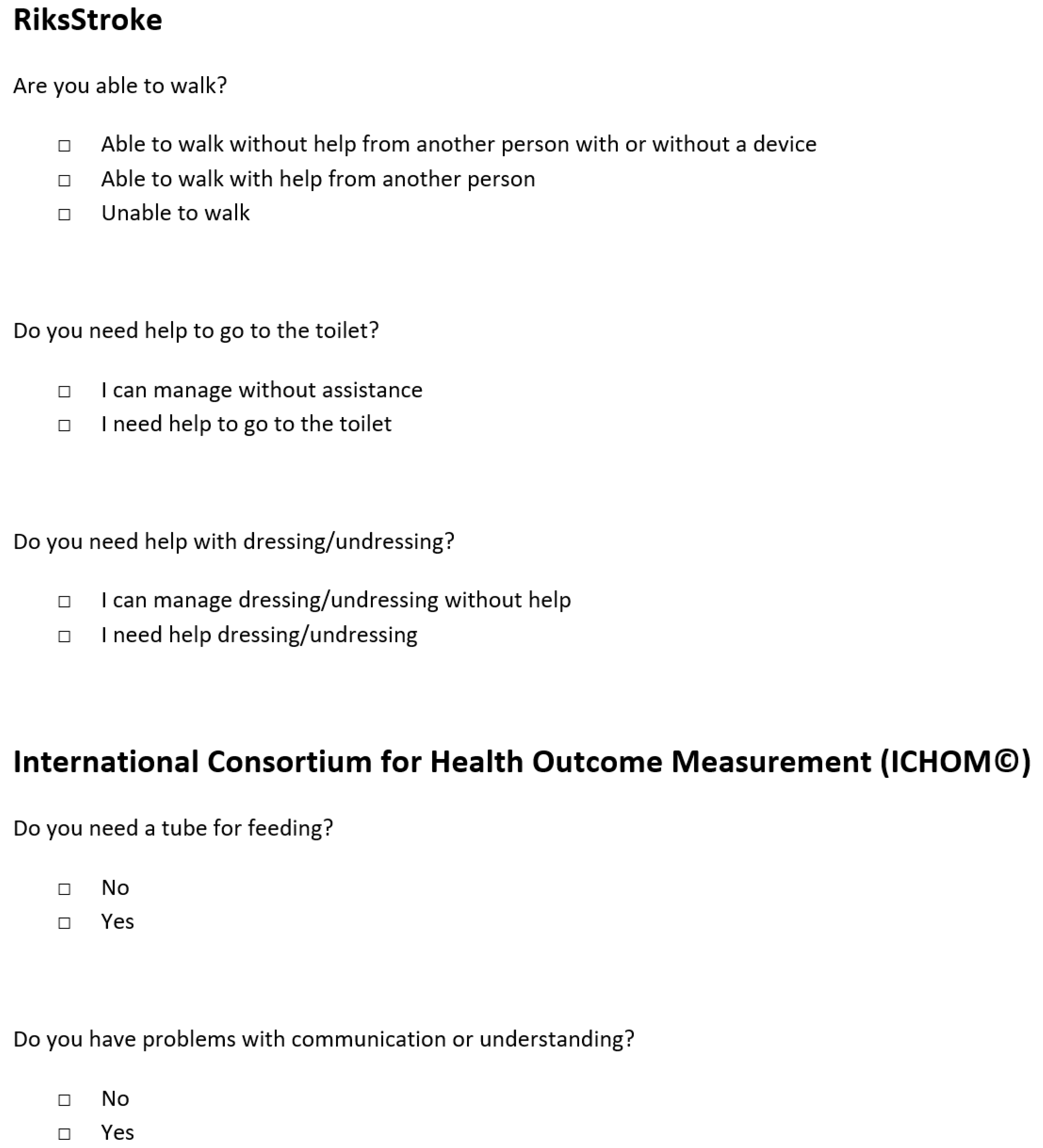
Appendix A



{kind=link}
{kind=link}
| Completed Follow-Up | Did Not Complete Follow-Up | Total | ||
|---|---|---|---|---|
| Number of Participants | 348 (16.3%) | 1726 (6.4%) | 2074 | |
| Grouped Age | <60 60–69 70–79 80–89 ≥90 | 47 (13.5%) 93 (26.7%) 122 (35.1%) 77 (22.1%) 9 (2.6%) | 317 (18.4%) 302 (17.5%) 492 (28.5%) 475 (27.5%) 140 (8.1%) | 364 (47.6%) 395 (16.4%) 614 (21.1%) 552 (13.0%) 149 (2.0%) |
| Sex | Female | 135 (38.8%) | 797 (46.1%) | 932 (44.9%) |
| NIHSS Grouped Frequencies | No Symptoms Mild Moderate Moderate-Severe Severe Missing | 135 (38.8%) 23 (14.0%) 167 (19.2%) 133 (17.2%) 14 (15.2%) 4 (4.9%) 7 | 797 (46.1%) 141 (86.0%) 701 (80.8%) 639 (82.8%) 78 (84.8%) 77 (95.1%) 90 | 932 (44.9%) 164 (7.9%) 868 (41.9%) 772 (37.2%) 92 (4.4%) 81 (3.9%) 97 |
| Thrombolysis Status | Received | 69 (20.2%) | 237 (14.2%) | 306 (15.3%) |
| Modified Rankin Classification | 0 1 2 3 4 5 Missing | 92 (23.7%) 81 (22.3%) 40 (17.0%) 43 (13.8%) 20 (9.9%) 3 (2.8%) 69 | 296 (76.3%) 282 (77.7%) 195 (83.0%) 269 (86.2%) 182 (90.1%) 106 (97.2%) 396 | 388 (24.1) 363 (22.6%) 235 (14.6%) 312 (19.4%) 202 (12.6%) 109 (6.8%) 465 |
| Stroke Classification | Ischaemic Haemorrhagic Not Specified | 308 (16.7%) 35 (17.2%) 5 (17.2%) | 1533 (83.6%) 169 (82.8%) 24 (82.8%) | 1841 (88.8%) 204 (9.8%) 29 (1.4%) |
References
- EuroQol—A new facility for the measurement of health-related quality of life. Health Policy 1990, 16, 199–208. [CrossRef]
- Brazier, J.E.; Harper, N.M.; Jones, A.; O’Cathain, K.J.; Thomas, T.; Usherwood, T.; Westlake, L. Validating the SF-36 health questionnaire: A new outcome measure for primary care. Br. Med. J. 1992, 305, 160–164. [Google Scholar] [CrossRef] [Green Version]
- Cameron, L.J.; Wales, K.; Casey, A.; Pike, S.; Jolliffe, L.; Schneider, E.J.; Christie, L.J.; Ratcliffe, J.; Lannin, N.A. Self-reported quality of life following stroke: A systematic review of instruments with a focus on their psychometric properties. Qual. Life Res. 2021, 1–14. [Google Scholar] [CrossRef]
- Salinas, J.; Sprinkhuizen, S.M.; Ackerson, T.; Bernhardt, J.; Davie, C.; George, M.G.; Gething, S.; Kelly, A.G.; Lindsay, P.; Liu, L.; et al. An International Standard Set of Patient-Centered Outcome Measures After Stroke. Stroke 2016, 47, 180–186. [Google Scholar] [CrossRef] [Green Version]
- Kelley, T.A. International Consortium for Health Outcomes Measurement (ICHOM). Trials 2015, 16, 04. [Google Scholar] [CrossRef] [Green Version]
- Hewitt, J.; Pennington, A.; Smith, A.; Gething, S.; Price, M.; White, J.; Dewar, R.; Carter, B. A multi-centre, UK-based, non-inferiority randomised controlled trial of 4 follow-up assessment methods in stroke survivors. BMC Med. 2019, 17, 111. [Google Scholar] [CrossRef] [Green Version]
- Smith, A.; Pennington, A.; Carter, B.; Gething, S.; Price, M.; White, J.; Dewar, R.; Hewitt, J. Acceptability of the method of administration of a patient-reported outcome measure (PROM) with stroke survivors, a randomised controlled trial protocol. Trials 2018, 19, 349. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. The ICD-10 Classification of Mental and Behavioural Disorders: Clinical Descriptions and Diagnostic Guidelines; World Health Organization: Geneva, Switzerland, 1992. [Google Scholar]
- Kwah, L.K.; Diong, J. National Institutes of Health Stroke Scale (NIHSS). J. Physiother. 2014, 60, 61. [Google Scholar] [CrossRef] [Green Version]
- Odderson, I.R. The National Institutes of Health Stroke Scale and Its Importance in Acute Stroke Management. Phys. Med. Rehabil. Clin. N. Am. 1999, 10, 787–800. [Google Scholar] [CrossRef]
- Saver, J.L.; Filip, B.; Hamilton, S.; Yanes, A.; Craig, S.; Cho, M.; Conwit, R.; Starkman, S.; for the FAST-MAG Investigators and Coordinators. Improving the reliability of stroke disability grading in clinical trials and clinical practice: The Rankin Focused Assessment (RFA). Stroke 2010, 41, 992–995. [Google Scholar] [CrossRef] [Green Version]
- Alonso, J.; Bartlett, S.J.; Rose, M.; Aaronson, N.K.; Chaplin, J.E.; Efficace, F.; Leplège, A.; Lu, A.; Tulsky, D.S.; Raat, H.; et al. The case for an international patient-reported outcomes measurement information system (PROMIS®) initiative. Health Qual. Life Outcomes 2013, 11, 210. [Google Scholar] [CrossRef] [Green Version]
- Hays, R.D.; Schalet, B.D.; Spritzer, K.L.; Cella, D. Two-item PROMIS® global physical and mental health scales. J. Patient Rep. Outcomes 2017, 1, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asplund, K.; Hulter Åsberg, K.; Appelros, P.; Bjarne, D.; Eriksson, M.; Johansson, A.; Jonsson, F.; Norrving, B.; Stegmayr, B.; Terént, A.; et al. The Riks-Stroke story: Building a sustainable national register for quality assessment of stroke care. Int. J. Stroke 2011, 6, 99–108. [Google Scholar] [CrossRef]
- Palmcrantz, S.; Sommerfeld, D.K. Development and validation of the Swedish national stroke register Riksstroke’s questionnaires in patients at 3 and 12 months after stroke: A qualitative study. BMJ Open 2018, 8, e018702. [Google Scholar] [CrossRef] [Green Version]
- Hays, R.D.; Bjorner, J.B.; Revicki, D.A.; Spritzer, K.L.; Cella, D. Development of physical and mental health summary scores from the patient-reported outcomes measurement information system (PROMIS) global items. Qual. Life Res. Int. J. Qual. Life Asp. Treat. Care Rehabil. 2009, 18, 873–880. [Google Scholar] [CrossRef] [Green Version]
- Duncan, P.W.; Wallace, D.; Lai, S.M.; Johnson, D.; Embretson, S.; Laster, L.J. The stroke impact scale version 2.0. Evaluation of reliability, validity, and sensitivity to change. Stroke 1999, 30, 2131–2140. [Google Scholar] [CrossRef] [Green Version]
- Van Straten, A.; De Haan, R.J.; Limburg, M.; Schuling, J.; Bossuyt, P.M.; Van den Bos, G.A. A stroke-adapted 30-item version of the Sickness Impact Profile to assess quality of life (SA-SIP30). Stroke 1997, 28, 2155–2161. [Google Scholar] [CrossRef]
- Soto-Cámara, R.; González-Santos, J.; González-Berna, J.; Trejo-Gabriel-Galán, J.M. Factors associated with a rapid call for assistance for patients with ischemic stroke. Emerg. Rev. Soc. Esp. Med. Emerg. 2020, 32, 33–39. [Google Scholar]
- Rossnagel, K.; Jungehülsing, G.J.; Nolte, C.H.; Müller-Nordhorn, J.; Roll, S.; Wegscheider, K.; Villringer, A.; Willich, S.N. Out-of-hospital delays in patients with acute stroke. Ann. Emerg. Med. 2004, 44, 476–483. [Google Scholar] [CrossRef]
- Gall, S.; Phan, H.; Madsen, T.E.; Reeves, M.; Rist, P.; Jimenez, M.; Lichtman, J.; Dong, L.; Lisabeth, L.D. Focused Update of Sex Differences in Patient Reported Outcome Measures After Stroke. Stroke 2018, 49, 531–535. [Google Scholar] [CrossRef]
- Farace, E.; Alves, W. Do women fare worse: A metaanalysis of gender differences in traumatic brain injury outcome. Neurosurg. Focus 2000, 8, e6. [Google Scholar] [CrossRef]
- Holbrook, T.L.; Hoyt, D.B. The impact of major trauma: Quality-of-life outcomes are worse in women than in men, independent of mechanism and injury severity. J. Trauma 2004, 56, 284–290. [Google Scholar] [CrossRef] [PubMed]
- Norris, C.M.; Ghali, W.A.; Galbraith, P.D.; Graham, M.M.; Jensen, L.A.; Knudtson, M.L.; the APPROACH Investigators. Women with coronary artery disease report worse health-related quality of life outcomes compared to men. Health Qual. Life Outcomes 2004, 2, 21. [Google Scholar] [CrossRef] [Green Version]
- Roquer, J.; Campello Ana, R.; Gomis, M. Sex Differences in First-Ever Acute Stroke. Stroke 2003, 34, 1581–1585. [Google Scholar] [CrossRef] [Green Version]
- Kapral Moira, K.; Fang, J.; Hill Michael, D.; Silver, F.; Richards, J.; Jaigobin, C.; Cheung Angela, M. Sex Differences in Stroke Care and Outcomes. Stroke 2005, 36, 809–814. [Google Scholar] [CrossRef] [PubMed]
- Andersen Klaus, K.; Olsen Tom, S.; Dehlendorff, C.; Kammersgaard Lars, P. Hemorrhagic and Ischemic Strokes Compared. Stroke 2009, 40, 2068–2072. [Google Scholar] [CrossRef] [Green Version]
- Jørgensen, H.S.; Nakayama, H.; Raaschou, H.O.; Olsen, T.S. Intracerebral hemorrhage versus infarction: Stroke severity, risk factors, and prognosis. Ann. Neurol. 1995, 38, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Saposnik, G.; Cote, R.; Phillips, S.; Gubitz, G.; Bayer, N.; Minuk, J.; Black, S. Stroke Outcome in Those Over 80. Stroke 2008, 39, 2310–2317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katzan, I.L.; Thompson, N.R.; Lapin, B.; Uchino, K. Added Value of Patient-Reported Outcome Measures in Stroke Clinical Practice. J. Am. Heart Assoc. 2017, 6, e005356. [Google Scholar] [CrossRef]
| Number of Participants | Total 343 | |
|---|---|---|
| Grouped Age | <60 60–69 70–79 80> | 47 (13.7%) 91 (26.5%) 121 (35.3%) 83 (24.2%) |
| Sex | Female Male | 133 (38.8%) 210 (61.2%) |
| Carer Assisted | Yes | 44 (12.8%) |
| NIHSS Grouped Frequencies | No Symptoms Mild Moderate Moderate-Severe Severe Missing | 23 (6.9%) 164 (47.8%) 132 (38.5%) 14 (4.1%) 3 (0.9%) 7 (2.0%) |
| Thrombolysis Status | Received | 69 (20.5%) |
| Rankin Classification | 0 1 2 3 4 5 Missing | 92 (33.3%) 80 (29.0%) 39 (14.1%) 43 (15.6%) 20 (7.2%) 2 (0.7%) 67 (24.3%) |
| Stroke Classification | Ischaemic Haemorrhagic Not Specific | 304 (88.6%) 34 (9.9%) 5 (1.5%) |
| PROMIS Mental Health | PROMIS Physical Health | Stroke Specific Domain | PROM Total | ||
|---|---|---|---|---|---|
| Grouped Age | <60 60–69 70–79 80–89 ≥90 | 41.10 (8.93) 45.30 (9.95) 46.82 (9.93) 45.27 (9.84) 41.26 (12.04) | 40.97 (9.79) 42.59 (9.33) 43.75 (8.95) 41.063 (9.33) 39.46 (10.00) | 63.52 (7.27) 63.48 (6.31) 64.37 (6.76) 61.90 (8.90) 51.15 (14.80) | 71.78 (10.83) 74.62 (10.76) 76.48 (10.42) 73.23 (11.60) 67.02 (15.88) |
| Sex | Female Male | 43.74 (9.90) 45.77 (9.95) | 40.62 (8.77) 43.68 (9.44) | 62.03 (8.92) 63.82 (6.90) | 72.30 (11.45) 75.73 (10.68) |
| Carer Assisted | No Yes | 46.25 (9.56) 36.35 (8.44) | 43.58 (9.02) 35.20 (7.75) | 64.55 (6.10) 53.56 (10.69) | 76.21 (10.02) 62.10 (10.24) |
| NIHSS Grouped Frequencies | No Symptoms Mild Moderate Moderate-Severe Severe Missing | 45.13 (10.52) 45.95 (9.63) 44.16 (10.00) 42.44 (13.66) 36.96 (8.27) 47.25 (6.03) | 42.75 (7.75) 43.46 (8.92) 42.27 (9.94) 38.36 (9.71) 32.23 (3.87) 37.64 (5.45) | 62.11 (9.28) 64.78 (5.96) 62.51 (7.90) 57.54 (10.54) 42.31 (8.52) 61.90 (9.91) | 73.89 (11.36) 76.23 (9.88) 73.35 (11.64) 68.10 (15.54) 57.23 (5.98) 73.09 (5.79) |
| Thrombolysis Status | Not Received Received | 44.82 (9.96) 45.47 (10.33) | 42.47 (9.00) 43.15 (10.50) | 63.23 (7.89) 63.19 (6.93) | 74.42 (10.95) 74.78 (11.94) |
| Rankin Classification | 0 1 2 3 4 5 Missing | 46.20 (11.30) 45.68 (8.95) 44.35 (8.49) 42.16 (9.50) 42.60 (11.30) 33.3 (9.36) 45.89 (9.49) | 44.26 (10.18) 42.44 (8.95) 40.57 (8.32) 39.87 (8.13) 41.42 (8.16) 37.15 (19.30) 43.49 (9.46) | 64.68 (5.44) 64.11 (7.35) 62.62 (7.80) 61.72 (8.51) 59.91 (7.70) 51.90 (14.09) 62.50 (9.44) | 76.42 (11.12) 75.10 (10.48) 72.62 (10.59) 70.88 (10.91) 71.28 (11.32) 65.07 (20.83) 75.31 (11.37) |
| Stroke Classification | Ischaemic Haemorrhagic Not Specified | 45.18 (10.03) 43.35 (9.72) 43.94 (7.57) | 42.64 (9.40) 41.47 (8.90) 40.32 (4.43) | 63.43 (7.06) 60.54 (11.95) 62.28 (12.11) | 74.68 (11.02) 72.26 (12.28) 72.19 (5.59) |
| Crude Mean Difference (95% CI) | p-Value | Adjusted Mean Difference (95% CI) | p-Value | ||
|---|---|---|---|---|---|
| Grouped Age | <60 60–69 70–79 ≥80 | Ref 2.84 (−1.04, 6.72) 4.70 (0.98, 8.42) 0.85 (−3.08, 4.79) | Ref 0.151 0.013 0.670 | Ref 2.13 (−1.82, 6.09) 4.47 (0.69, 8.25) 0.39 (−3.62, 4.40) | Ref 0.290 0.020 0.849 |
| Sex | Male Female | Ref −3.42 (−5.82, −1.03) | Ref 0.005 | Ref −3.85 (−6.30, −1.41) | Ref 0.002 |
| Stroke Classification | Ischaemic Haemorrhagic Other | Ref −2.42 (−6.37, 1.53) −2.49 (−12.33, 7.35) | Ref 0.228 0.619 | Ref −3.38 (−7.37, 0.61) −4.05 (−14.15, 6.06) | Ref 0.097 0.431 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hewitt, J.; Bains, N.; Wallis, K.; Gething, S.; Pennington, A.; Carter, B. The Use of Patient Reported Outcome Measures (PROMs) 6 Months Post-Stroke and Their Association with the National Institute of Health Stroke Scale (NIHSS) on Admission to Hospital. Geriatrics 2021, 6, 88. https://doi.org/10.3390/geriatrics6030088
Hewitt J, Bains N, Wallis K, Gething S, Pennington A, Carter B. The Use of Patient Reported Outcome Measures (PROMs) 6 Months Post-Stroke and Their Association with the National Institute of Health Stroke Scale (NIHSS) on Admission to Hospital. Geriatrics. 2021; 6(3):88. https://doi.org/10.3390/geriatrics6030088
Chicago/Turabian StyleHewitt, Jonathan, Natalie Bains, Katherine Wallis, Stephanie Gething, Anna Pennington, and Ben Carter. 2021. "The Use of Patient Reported Outcome Measures (PROMs) 6 Months Post-Stroke and Their Association with the National Institute of Health Stroke Scale (NIHSS) on Admission to Hospital" Geriatrics 6, no. 3: 88. https://doi.org/10.3390/geriatrics6030088