

Use of Laryngeal Mask and Anesthetic Management in Hamadryas Baboons (Papio hamadryas) Undergoing Laparoscopic Salpingectomy—A Case Series
 , , , , and
, , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- AZA Baboon Species Survival Plan®. Hamadryas Baboon Care Manual; Association of Zoos and Aquariums: Silver Spring, MD, USA, 2020. [Google Scholar]
- Yu, P.-H.; Weng, C.-C.; Kuo, H.-C.; Chi, C.-H. Evaluation of endoscopic salpingectomy for sterilization of female Formosan macaques (Macaca cyclopis). Am. J. Primatol. 2015, 77, 359–367. [Google Scholar] [CrossRef] [PubMed]
- Lacitignola, L.; Laricchiuta, P.; Dvm, A.I.; Dvm, C.A.; Stabile, M.; Dvm, F.S.; Dvm, L.L.; Dvm, E.P.L.; Dvm, M.S. Laparoscopic salpingectomy in Papio hamadryas for birth control in captivity. Vet. Surg. 2022, 51, O98–O106. [Google Scholar] [CrossRef] [PubMed]
- Krikri, A.; Alexopoulos, V.; Zoumakis, E.; Katsaronis, P.; Balafas, E.; Kouraklis, G.; Karayannacos, P.; Chrousos, G.; Skalkeas, G. Laparoscopic vs. open abdominal surgery in male pigs: Marked. differences in cortisol and catecholamine response depending on the size of surgical incision. Hormones 2013, 12, 283–291. [Google Scholar] [CrossRef] [Green Version]
- Devitt, C.M.; Cox, R.E.; Hailey, J.J. Duration, complications, stress, and pain of open ovariohysterectomy versus a simple method of laparoscopic-assisted. ovariohysterectomy in dogs. J. Am. Vet. Med. Assoc. 2005, 227, 921–927. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haleem, S.; Ansari, M.M.; Mussarat, J.; Ahmed, A.; Islam, N.; Bano, S.; Singh, B.R. Cortisol and Glycemic Response to Open and Laparoscopic Cholecystectomy—A Comparative Evaluation. J. Anaesthesiol. Clin. Pharmacol. 2008, 24, 437–440. [Google Scholar]
- Garcia-Pereira, F. Physiology, Pathophysiology, and Anesthetic Management of Patients with Hepatic Disease. In Veterinary Anesthesia and Analgesia: The Fifth Edition of Lumb and Jones, 5th ed.; Grimm, K.A., Lamont, L.A., Tranquilli, W.J., Greene, S.A., Robertson, S.A., Eds.; John Wiley & Sons, Inc.: Ames, IA, USA, 2015; pp. 627–640. [Google Scholar]
- Joris, J.L. Anesthesia for laparoscopic surgery. In Miller’s Anesthesia, 8th ed.; Miller, R.D., Cohen, N.H., Fleischer, L.A., Wiener-Kronish, J.P., Young, W.L., Eds.; Saunders: Philadelphia, PA, USA, 2014; Volume 2, pp. 2185–2197. [Google Scholar]
- Ølberg, R.-A.; Sinclair, M. Monkeys and Gibbons. In Zoo Animal and Wildlife Immobilization and Anesthesia, 2nd ed.; West, G., Heard, D., Caulkett, N., Eds.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2014; pp. 561–571. [Google Scholar]
- Langoi, D.; Mwethera, P.; Abelson, K.; Farah, I.; Carlsson, H. Reversal of Ketamine/Xylazine combination anesthesia by Atipamezole in olive baboons (Papio anubis). J. Med. Primatol. 2009, 38, 404–410. [Google Scholar] [CrossRef]
- Yeung, K.R.; Lind, J.M.; Heffernan, S.J.; Sunderland, N.; Hennessy, A.; Makris, A. Comparison of indirect and direct blood pressure measurements in baboons during ketamine anaesthesia. J. Med. Primatol. 2014, 43, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Saba, W.; Goutal, S.; Kuhnast, B.; Dollé, F.; Auvity, S.; Fontyn, Y.; Cayla, J.; Peyronneau, M.-A.; Valette, H.; Tournier, N. Differential influence of propofol and isoflurane anesthesia in a non-human primate on the brain kinetics and binding of [18F]DPA-714, a positron emission tomography imaging marker of glial activation. Eur. J. Neurosci. 2015, 42, 1738–1745. [Google Scholar] [CrossRef]
- Santerre, D.; Chen, R.; Kadner, A.; Lee-Parritz, D.; Adams, D. Anaesthetic management of baboons undergoing heterotopic porcine cardiac xenotransplantation. Vet. Res. Commun. 2001, 25, 251–259. [Google Scholar] [CrossRef]
- Giffard, C.; Young, A.R.; Mézenge, F.; Derlon, J.-M.; Baron, J.-C. Histopathological effects of delayed. reperfusion after middle cerebral artery occlusion in the anesthetized baboon. Brain Res. Bull. 2005, 67, 335–340. [Google Scholar] [CrossRef] [PubMed]
- Schumann-Bard, P.; Touzani, O.; Young, A.R.; Toutain, J.; Baron, J.-C.; MacKenzie, E.T.; Schmidt, E.A. Cerebrovascular Effects of Sodium Nitroprusside in the Anaesthetized. Baboon: A Positron Emission Tomographic Study. J. Cereb. Blood Flow Metab. 2005, 25, 535–544. [Google Scholar] [CrossRef] [PubMed]
- Reedy, M.B.; Galan, H.L.; Bean-Lijewski, J.D.; Carnes, A.; Knight, A.B.; Kuehl, T.J. Maternal and fetal effects of laparoscopic insufflation in the gravid baboon. J. Am. Assoc. Gynecol. Laparoscopists 1995, 2, 399–406. [Google Scholar] [CrossRef]
- D’Hooghe, T.M.; Bambra, C.S.; Farah, I.O.; Raeymaekers, B.M.; Koninckx, P. High intraabdominal pressure: Effects on clinical parameters and lung pathology in baboons (Papio cynocephalus and Papio anubis). Am. J. Obstet. Gynecol. 1993, 169, 1352–1356. [Google Scholar] [CrossRef]
- Flecknell, P.A.; Thomas, A.A. Comparative Anesthesia and Analgesia of Laboratory Animals. In Veterinary Anesthesia and Analgesia: The Fifth Edition of Lumb and Jones, 5th ed.; Grimm, K.A., Lamont, L.A., Tranquilli, W.J., Greene, S.A., Robertson, S.A., Eds.; John Wiley & Sons, Inc.: Ames, OA, USA, 2015; pp. 754–763. [Google Scholar]
- Miller, R.D.; Cohen, N.H.; Fleischer, L.A.; Wiener-Kronish, J.P.; Young, W.L. (Eds.) Airway Management in the Adult. In Miller’s Anesthesia, 8th ed.; Saunders: Philadelphia, PA, USA, 2014; Volume 2. [Google Scholar]
- Johnson, J.A.; Atkins, A.L.; Heard, D.J. Application of the Laryngeal Mask Airway for Anesthesia in Three Chimpanzees and One Gibbon. J. Zoo Wildl. Med. 2010, 41, 535–537. [Google Scholar] [CrossRef]
- Cerveny, S.N.; D’Agostino, J.J.; Davis, M.R.; Payton, M.E. Comparison of Laryngeal Mask Airway Use with Endotracheal Intubation during Anesthesia of Western Lowland Gorillas (Gorilla gorilla gorilla). J. Zoo Wildl. Med. 2012, 43, 759–767. [Google Scholar] [CrossRef]
- Stabile, M.; Lacitignola, L.; Piemontese, M.R.; Di Bella, C.; Acquafredda, C.; Grasso, S.; Crovace, A.M.; de Segura, I.A.G.; Staffieri, F. Comparison of CPAP and oxygen therapy for treatment of postoperative hypoxaemia in dogs. J. Small Anim. Pract. 2021, 62, 351–358. [Google Scholar] [CrossRef]
- International Species Information System. 2002. Available online: www.isis.org (accessed on 19 November 2020).
- Deleuze, S.; Brotcorne, F.; Polet, R.; Soma, G.; Rigaux, G.; Giraud, G.; Cloutier, F.; Poncin, P.; Wandia, N.; Huynen, M.-C. Tubectomy of Pregnant and Non-pregnant Female Balinese Macaques (Macaca fascicularis) With Post-operative Monitoring. Front. Vet. Sci. 2021, 8, 688656. [Google Scholar] [CrossRef]
- Fahlman, A.; Bosi, E.J.; Nyman, G. Reversible Anesthesia of Southeast Asian Primates with Medetomidine, Zolazepam, and Tiletamine. J. Zoo Wildl. Med. 2006, 37, 558–561. [Google Scholar] [CrossRef]
- Brain, A.I.J. The Laryngeal Mask—A New Concept in Airway Management. Br. J. Anaesth. 1983, 55, 801–805. [Google Scholar] [CrossRef]
- Wiederstein, I.; Moens, Y.P. Guidelines and criteria for the placement of laryngeal mask airways in dogs. Vet. Anaesth. Analg. 2008, 35, 374–382. [Google Scholar] [CrossRef] [PubMed]
- Cassu, R.; Luna, S.P.; Neto, F.T.; Braz, J.R.; Gasparini, S.S.; Crocci, A.J. Evaluation of laryngeal mask as an alternative to endotracheal intubation in cats anesthetized under spontaneous or controlled ventilation. Vet. Anaesth. Analg. 2004, 31, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Bateman, L.; Ludders, J.W.; Gleed, R.D.; Erb, H.N. Comparison between facemask and laryngeal mask airway in rabbits during isoflurane anesthesia. Vet. Anaesth. Analg. 2005, 32, 280–288. [Google Scholar] [CrossRef]
- Fulkerson, P.J.; Gustafson, S.B. Use of laryngeal mask airway compared. to endotracheal tube with positive-pressure ventilation in anesthetized swine. Vet. Anaesth. Analg. 2007, 34, 284–288. [Google Scholar] [CrossRef] [PubMed]
- Girotto, C.H.; Teixeira-Neto, F.J.; Justo, A.A.; Carvalho, E.R.; Fonseca, M.W.; Garofalo, N.A. Evaluation of a laryngeal mask airway as an alternative to orotracheal intubation for maintaining airway patency during inhalant anesthesia under spontaneous ventilation in capybaras (Hydrochoerus hydrochaeris). J. Zoo Wildl. Med. 2021, 52, 276–286. [Google Scholar] [CrossRef] [PubMed]
- Beleña, J.M.; Ochoa, E.J.; Núñez, M.; Gilsanz, C.; Vidal, A. Role of laryngeal mask airway in laparoscopic cholecystectomy. World J. Gastrointest. Surg. 2015, 7, 319–325. [Google Scholar] [CrossRef]
- Aydogmus, M.T.; Turk, H.S.Y.; Oba, S.; Unsal, O.; Sınıkoglu, S.N. Can supreme™ laryngeal mask airway be an alternative to endotracheal intubation in laparoscopic surgery? Braz. J. Anesthesiol. 2014, 64, 66–70. [Google Scholar] [CrossRef] [Green Version]
- Ozden, E.S.; Meco, B.C.; Alanoglu, Z.; Alkıs, N. Comparison of ProSeal laryngeal mask airway (PLMA) with cuffed. and uncuffed. endotracheal tubes in infants. Bosn. J. Basic Med. Sci. 2016, 16, 286–291. [Google Scholar] [CrossRef] [Green Version]
- Asida, S.; Ahmed, S. Ease of insertion of the laryngeal mask airway in pediatric surgical patients: Predictors of failure and outcome. Saudi J. Anaesth. 2016, 10, 295–300. [Google Scholar] [CrossRef]
- Wong, D.T.; Yang, J.J.; Jagannathan, N. Brief review: The LMA SupremeTM supraglottic airway Article de synthèse court: Le dispositif supraglottique LMA SupremeTM. Can. J. Anesth. 2012, 59, 483–493. [Google Scholar] [CrossRef] [Green Version]
- Gordon, J.; Cooper, R.M.; Parotto, M. Supraglottic airway devices: Indications, contraindications and management. Minerva Anestesiol. 2018, 84, 389–397. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Mean (95% CI) | Reference Range a |
|---|---|---|
| RBC (M/µL) | 4.7 (4.3–5.1) | 3.9–6.9 |
| Hb (g/dL) | 11.7 (10.7–12.7) | 9.1–17.5 |
| Hct (%) | 36.3 (33.9–38.8) | 30.3–61.1 |
| MCV (fL) | 77.2 (75.8–78.6) | 64.3–97.4 |
| MCHC (g/dL) | 32.4 (31.1–33.8) | 24.6–40.2 |
| WBC (K/µL) | 9.2 (6.6–11.7) | 3.2–28.6 |
| NEU (/µL) | 7200 (4700–9800) | 1090–24,300 |
| LYM (/µL) | 1300 (900–1800) | 1290–8760 |
| MONO (/µL) | 500 (300–600) | 0–2106 |
| EOS (/µL) | 20 (7–40) | 0–923 |
| BASO (/µL) | 30 (20–40) | 0–172 |
| Plt (K/µL) | 448.9 (401.8–495.9) | 157–875 |
| Variable | Mean (95% CI) | Reference Range a |
|---|---|---|
| CPK (IU/L) | 626.7 (38.6–1214.7) | 38–2262 |
| AST (IU/L) | 45.2 (34.4–56.1) | 11–141 |
| ALT (IU/L) | 29.5 (16.8–42.2) | 11–107 |
| ALP (IU/L) | 437.7 (204.4–670.9) | 55–1213 |
| GGT (IU/L) | 35.3 (26.9–43.7) | 13–123 |
| TB (mg/dL) | 0.17 (0.14–0.2) | 0–1.0 |
| TP (g/dL) | 6.3 (5.8–6.8) | 5–8.9 |
| Alb (g/dL) | 3.4 (2.9–3.9) | 2.8–5.2 |
| Glob (g/dL) | 2.9 (2.6–3.2) | 1.6–5.1 |
| Chol (mg/dL) | 97.5 (80.1–115.1) | 55–189 |
| Trig (mg/dL) | 49.9 (37.6–62.1) | 14–149 |
| BUN (mg/dL) | 31.1 (21.6–40.5) | 6–29 |
| Crea (mg/dL) | 1.1 (0.8–1.2) | 0.6–1.9 |
| Gluc (mg/dL) | 134.1 (104.5–163.6) | 37–391 |
| Ca (mg/dL) | 8.9 (8.3–9.4) | 7.8–11.4 |
| P (mg/dL) | 3.6 (2.4–4.7) | 0.8–9.5 |
| Mg (mg/dL) | 1.7 (1.5–1.9) | 1.1–2.2 |
| Na (mEq/L) | 145.3 (142.6–147.9) | 141–162 |
| K (mEq/L) | 4.1 (3.5–4.5) | 2.8–5.1 |
| Cl (mEq/L) | 106.1 (103.1–109.2) | 96–126 |
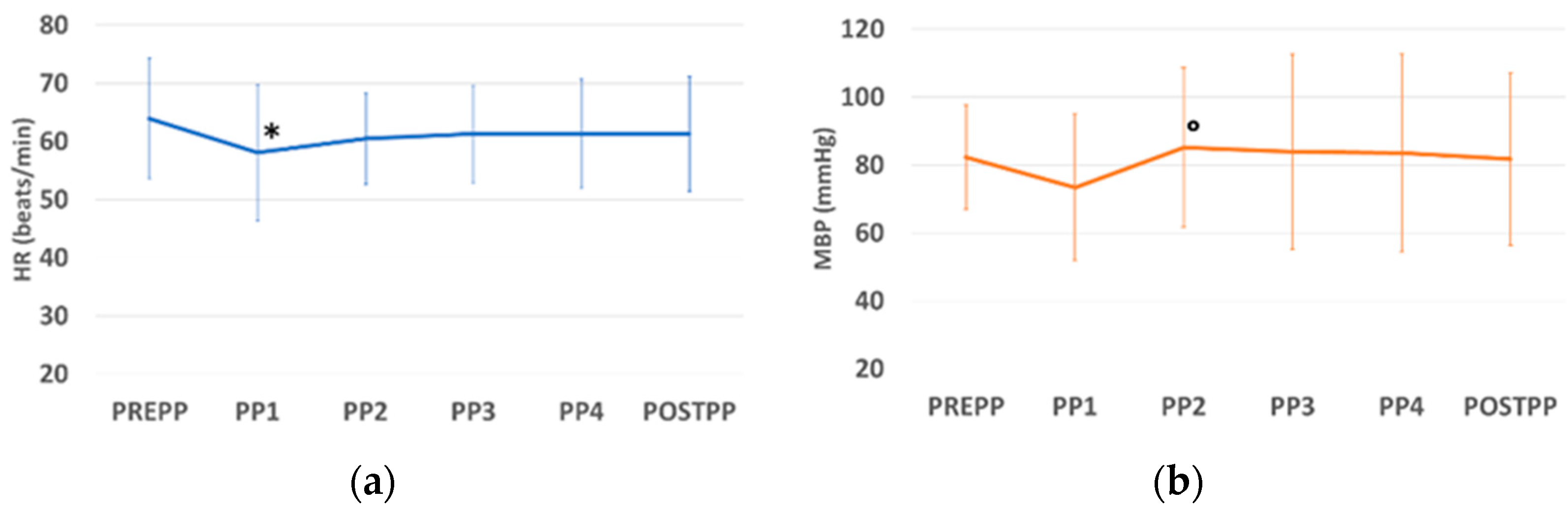
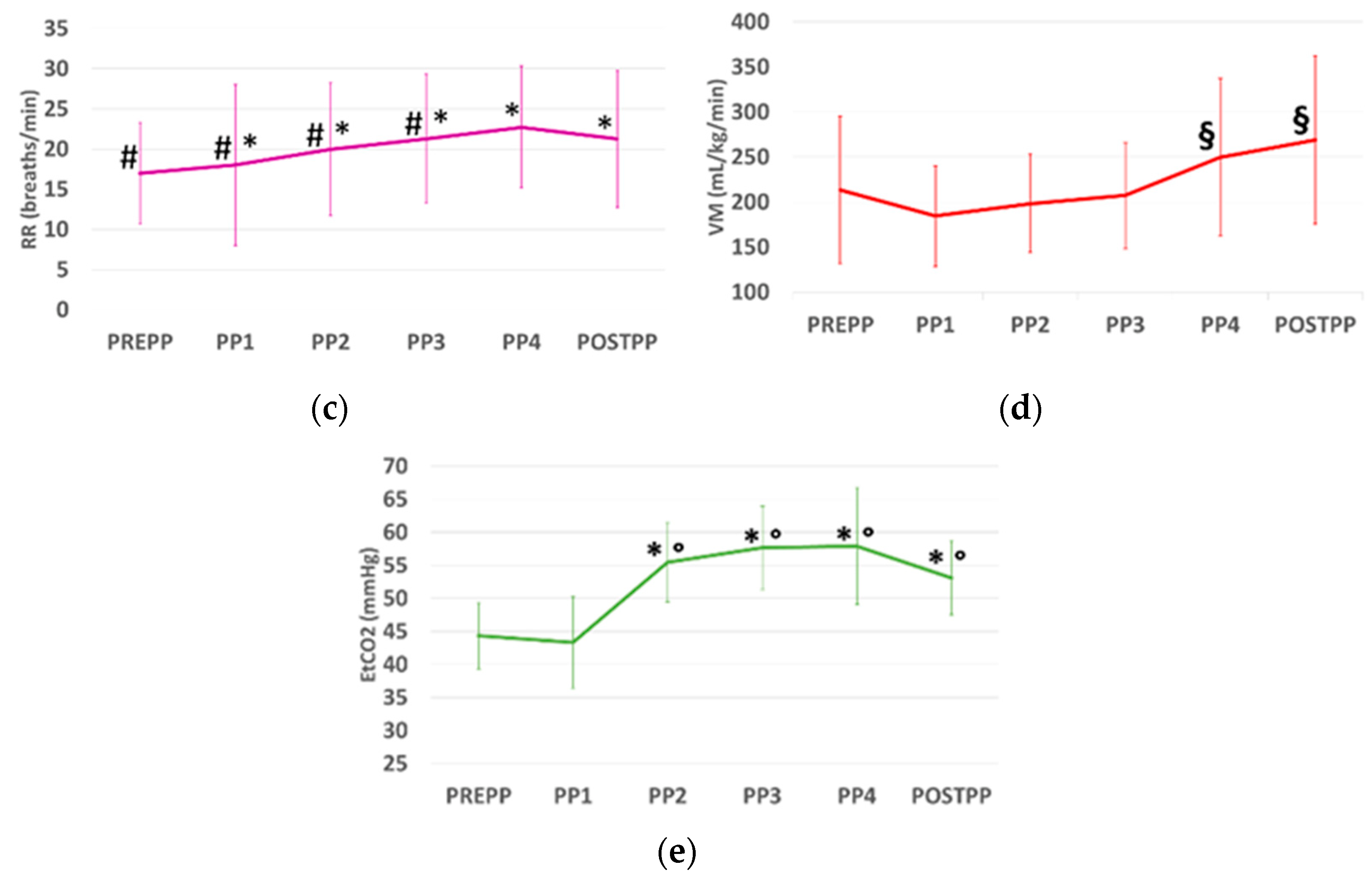
| Parameters | PREPP | PP1 | PP2 | PP3 | PP4 | POSTPP |
|---|---|---|---|---|---|---|
| HR (beats/min) | 64 (57–71) | 58 (50–66) * | 60 (55–66) | 61 (56–67) | 61 (55–68) | 61 (55–68) |
| MAP (mmHg) | 82 (72–93) | 73(59–88) | 85(69–101) ° | 84 (65–103) | 84 (64–103) | 82 (65–99) |
| RR (breaths/min) | 17 (13–21) # | 18 (11–25) *# | 20 (14–26) *# | 21 (16–27) *# | 23 (18–28) * | 21 (16–27) * |
| EtCO2 (mmHg) | 44 (41–48) | 43 (39–48) | 55 (51–60) *° | 58 (53–62) *° | 58 (52–64) *° | 53 (50–57) *° |
| TV (mL/kg) | 11.7 (7.2–16.1) | 10.4 (6.8–13.9) | 11.3 (7.8–14.7) | 11.1 (8.1–14.0) | 11.4 (8.3–14.4) | 12.6 (10.2–14.9) |
| MV (mL/min/kg) | 213.5 (158.7–268.3) | 184.4 (146.1–221.9) | 198.3 (161.9–234.8) | 207.3 (168.1–246.7) | 249.4 (190.7–308.1) § | 269.1 (206.1–331.8) § |
| SpO2 (%) | 97 (96- 98) | 97 (96–99) | 98 (97–99) | 98 (96–99) | 98 (98–99) | 98 (98–99) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scardia, A.; Laricchiuta, P.; Stabile, M.; Acquafredda, C.; Lacitignola, L.; Uva, A.; Crovace, A.; Staffieri, F. Use of Laryngeal Mask and Anesthetic Management in Hamadryas Baboons (Papio hamadryas) Undergoing Laparoscopic Salpingectomy—A Case Series. Vet. Sci. 2023, 10, 158. https://doi.org/10.3390/vetsci10020158
Scardia A, Laricchiuta P, Stabile M, Acquafredda C, Lacitignola L, Uva A, Crovace A, Staffieri F. Use of Laryngeal Mask and Anesthetic Management in Hamadryas Baboons (Papio hamadryas) Undergoing Laparoscopic Salpingectomy—A Case Series. Veterinary Sciences. 2023; 10(2):158. https://doi.org/10.3390/vetsci10020158
Chicago/Turabian StyleScardia, Annalaura, Pietro Laricchiuta, Marzia Stabile, Claudia Acquafredda, Luca Lacitignola, Annamaria Uva, Antonio Crovace, and Francesco Staffieri. 2023. "Use of Laryngeal Mask and Anesthetic Management in Hamadryas Baboons (Papio hamadryas) Undergoing Laparoscopic Salpingectomy—A Case Series" Veterinary Sciences 10, no. 2: 158. https://doi.org/10.3390/vetsci10020158