
Acceptance of a Novel, Highly Palatable, Calorically Dense, and Nutritionally Complete Diet in Dogs with Benign and Malignant Tumors
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics
2.2. Study Design
2.3. Study Animals
2.4. Study Food
2.5. Statistical Analysis and Methods
3. Results
3.1. Population
3.2. Food Effects
3.3. Quality of Life
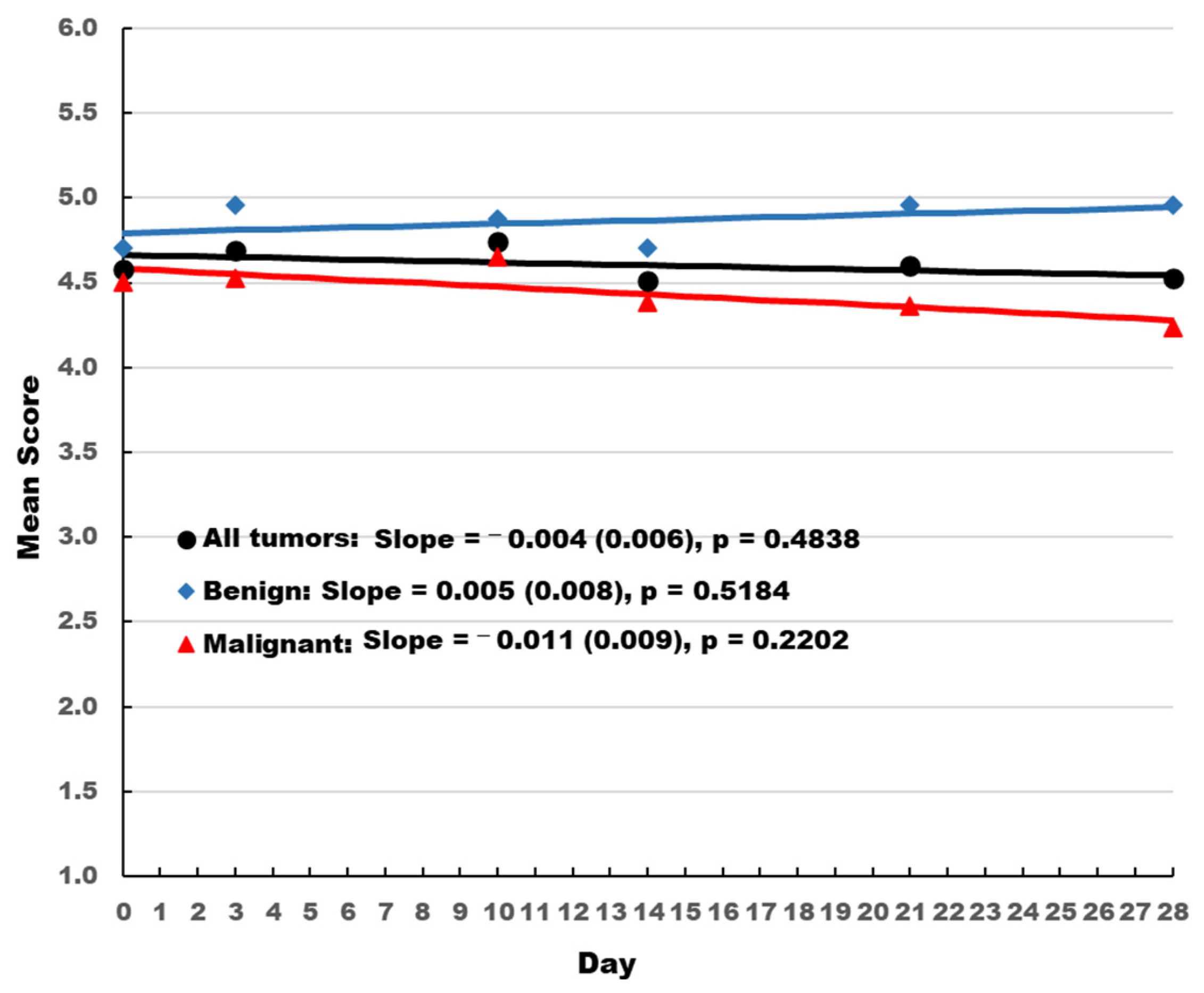
3.4. Stool Quality
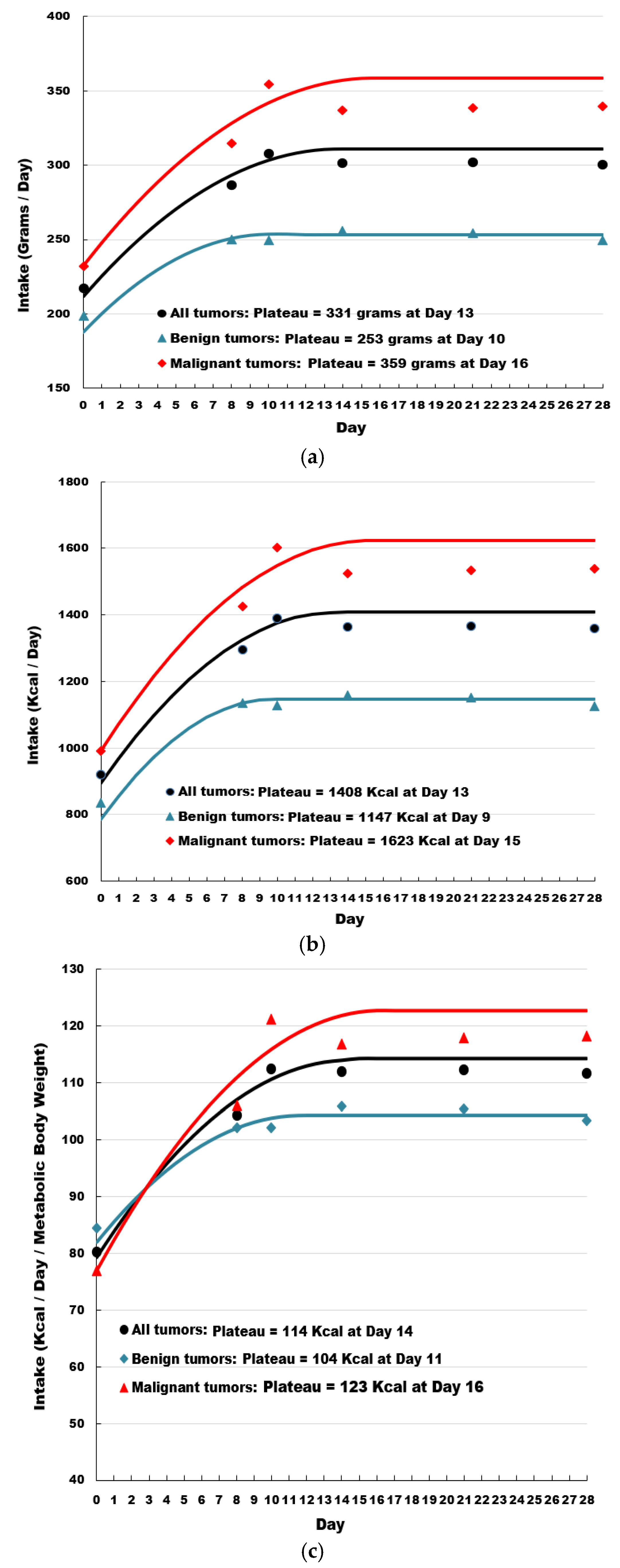
3.5. Food Intake
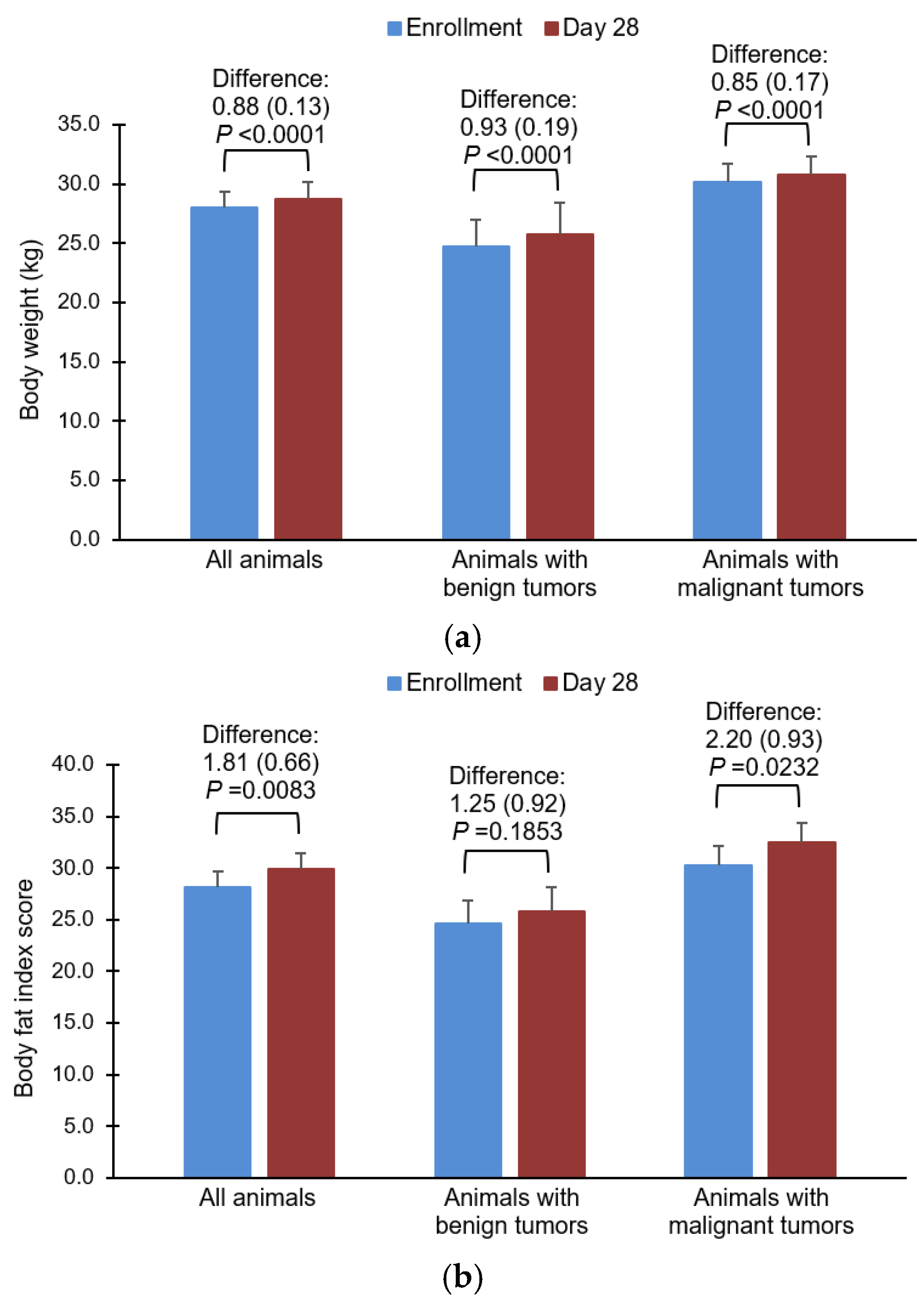
3.6. Body Weight
3.7. Adverse Events and Laboratory Measures
3.8. Exit Interviews
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Veterinary Medical Association. 2022 AVMA Pet Ownership and Demographics Sourcebook; American Veterinary Medical Association: Schaumburg, IL, USA, 2022. [Google Scholar]
- Tanaka, M.; Yamaguchi, S.; Iwasa, Y. Enhanced risk of cancer in companion animals as a response to the longevity. Sci. Rep. 2020, 10, 19508. [Google Scholar] [CrossRef]
- Schiffman, J.D.; Breen, M. Comparative oncology: What dogs and other species can teach us about humans with cancer. Philos. Trans. R. Soc. Lond. Ser. B Biol. Sci. 2015, 370, 20140231. [Google Scholar] [CrossRef]
- Johannes, C.M.; Musser, M.L. Anorexia and the Cancer Patient. Vet. Clin. N. Am. Small Anim. Pract. 2019, 49, 837–854. [Google Scholar] [CrossRef]
- Michel, K.E.; Sorenmo, K.; Shofer, F.S. Evaluation of body condition and weight loss in dogs presented to a veterinary oncology service. J. Vet. Intern. Med. 2004, 18, 692–695. [Google Scholar] [CrossRef] [PubMed]
- Mauldin, G.E. Supportive Care for the Cancer Patient. In Withrow and MacEwen’s Small Animal Clinical Oncology, 4th ed.; Withrow, S.J., Vail, D.M., Eds.; Saunders Elsevier: St. Louis, MO, USA, 2006; pp. 307–323. [Google Scholar]
- Harris, J.; Sengar, D.; Stewart, T.; Hyslop, D. The effect of immunosuppressive chemotherapy on immune function in patients with malignant disease. Cancer 1976, 37, 1058–1069. [Google Scholar] [CrossRef]
- Heidecke, C.D.; Weighardt, H.; Feith, M.; Fink, U.; Zimmermann, F.; Stein, H.J.; Siewert, J.R.; Holzmann, B. Neoadjuvant treatment of esophageal cancer: Immunosuppression following combined radiochemotherapy. Surgery 2002, 132, 495–501. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.; Phillips, C.; Byrd, H.M. Factors Which Influence Owners When Deciding to Use Chemotherapy in Terminally Ill Pets. Animals 2017, 7, 18. [Google Scholar] [CrossRef] [PubMed]
- Baez, J.L.; Michel, K.E.; Sorenmo, K.; Shofer, F.S. A prospective investigation of the prevalence and prognostic significance of weight loss and changes in body condition in feline cancer patients. J. Feline Med. Surg. 2007, 9, 411–417. [Google Scholar] [CrossRef]
- Marchitelli, B.; Shearer, T.; Cook, N. Factors Contributing to the Decision to Euthanize: Diagnosis, Clinical Signs, and Triggers. Vet. Clin. N. Am. Small Anim. Pract. 2020, 50, 573–589. [Google Scholar] [CrossRef]
- Nakano, Y.; Matsushima, M.; Nakamori, A.; Hiroma, J.; Matsuo, E.; Wakabayashi, H.; Yoshida, S.; Ichikawa, H.; Kaneko, M.; Mutai, R.; et al. Depression and anxiety in pet owners after a diagnosis of cancer in their pets: A cross-sectional study in Japan. BMJ Open 2019, 9, e024512. [Google Scholar] [CrossRef] [Green Version]
- Stoewen, D.L.; Coe, J.B.; MacMartin, C.; Stone, E.A.; Dewey, C.E. Identification of Illness Uncertainty in Veterinary Oncology: Implications for Service. Front. Vet. Sci. 2019, 6, 147. [Google Scholar] [CrossRef] [PubMed]
- Tran, L.; Crane, M.F.; Phillips, J.K. The distinct role of performing euthanasia on depression and suicide in veterinarians. J. Occup. Health Psychol. 2014, 19, 123–132. [Google Scholar] [CrossRef]
- Laflamme, D.P.; Abood, S.K.; Fascetti, A.J.; Fleeman, L.M.; Freeman, L.M.; Michel, K.E.; Bauer, C.; Kemp, B.L.; Doren, J.R.; Willoughby, K.N. Pet feeding practices of dog and cat owners in the United States and Australia. J. Am. Vet. Med. Assoc. 2008, 232, 687–694. [Google Scholar] [CrossRef]
- Michel, K.E.; Willoughby, K.N.; Abood, S.K.; Fascetti, A.J.; Fleeman, L.M.; Freeman, L.M.; Laflamme, D.P.; Bauer, C.; Kemp, B.L.; Doren, J.R. Attitudes of pet owners toward pet foods and feeding management of cats and dogs. J. Am. Vet. Med. Assoc. 2008, 233, 1699–1703. [Google Scholar] [CrossRef] [PubMed]
- Wakshlag, J.; Kallfelz, F. Nutritional status of dogs with cancer: Dietetic evaluation and recommendations. In Encyclopedia of Canine Clinical Nutrition; Pascale, P., Biourge, V., Elliott, D., Eds.; Royal Canin: Aimargues, France, 2006; pp. 408–412. [Google Scholar]
- Rajagopaul, S.; Parr, J.M.; Woods, J.P.; Pearl, D.L.; Coe, J.B.; Verbrugghe, A. Owners’ attitudes and practices regarding nutrition of dogs diagnosed with cancer presenting at a referral oncology service in Ontario, Canada. J. Small Anim. Pract. 2016, 57, 484–490. [Google Scholar] [CrossRef]
- Lana, S.E.; Kogan, L.R.; Crump, K.A.; Graham, J.T.; Robinson, N.G. The use of complementary and alternative therapies in dogs and cats with cancer. J. Am. Anim. Hosp. Assoc. 2006, 42, 361–365. [Google Scholar] [CrossRef] [PubMed]
- Freeman, L.M.; Abood, S.K.; Fascetti, A.J.; Fleeman, L.M.; Michel, K.E.; Laflamme, D.P.; Bauer, C.; Kemp, B.L.; Van Doren, J.R.; Willoughby, K.N. Disease prevalence among dogs and cats in the United States and Australia and proportions of dogs and cats that receive therapeutic diets or dietary supplements. J. Am. Vet. Med. Assoc. 2006, 229, 531–534. [Google Scholar] [CrossRef]
- Remillard, R.L. Homemade diets: Attributes, pitfalls, and a call for action. Top Companion Anim. Med. 2008, 23, 137–142. [Google Scholar] [CrossRef]
- Schlesinger, D.P.; Joffe, D.J. Raw food diets in companion animals: A critical review. Can. Vet. J. 2011, 52, 50–54. [Google Scholar]
- Freeman, L.M.; Chandler, M.L.; Hamper, B.A.; Weeth, L.P. Current knowledge about the risks and benefits of raw meat-based diets for dogs and cats. J. Am. Vet. Med. Assoc. 2013, 243, 1549–1558. [Google Scholar] [CrossRef]
- Heinze, C.R.; Gomez, F.C.; Freeman, L.M. Assessment of commercial diets and recipes for home-prepared diets recommended for dogs with cancer. J. Am. Vet. Med. Assoc. 2012, 241, 1453–1460. [Google Scholar] [CrossRef]
- Tobie, C.; Péron, F.; Larose, C. Assessing Food Preferences in Dogs and Cats: A Review of the Current Methods. Animals 2015, 5, 126–137. [Google Scholar] [CrossRef]
- Bourgeois, H.; Elliott, D.; Marniquet, P.; Soulard, Y. Dietary behavior of dogs and cats. Bull. Acad. Vet. Fr. 2006, 159, 301–308. [Google Scholar] [CrossRef]
- Bradshaw, J.W. The evolutionary basis for the feeding behavior of domestic dogs (Canis familiaris) and cats (Felis catus). J. Nutr. 2006, 136, 1927S–1931S. [Google Scholar] [CrossRef]
- Samant, S.S.; Crandall, P.G.; Jarma Arroyo, S.E.; Seo, H.S. Dry Pet Food Flavor Enhancers and Their Impact on Palatability: A Review. Foods 2021, 10, 2599. [Google Scholar] [CrossRef] [PubMed]
- National Research Council. Nutrient Requirements of Dogs and Cats; National Academies Press: Washington, DC, USA, 2006. [Google Scholar]
- Brown, H.; Prescott, R. Applied Mixed Models in Medicine, 2nd ed.; John Wiley & Sons, Ltd.: West Sussex, UK, 2006. [Google Scholar]
- Littell, R.C.; Milliken, G.A.; Stroup, W.W.; Wolfinger, R.D.; Schabenberger, O. SAS® for Mixed Models, 2nd ed.; SAS Institute, Inc.: Cary, NC, USA, 2006. [Google Scholar]
- Kenward, M.G.; Roger, J.H. Small sample inference for fixed effects from restricted maximum likelihood. Biometrics 1997, 53, 983–997. [Google Scholar] [CrossRef]
- Rogers, W.A.; Donovan, E.F.; Kociba, G.J. Lipids and lipoproteins in normal dogs and dogs with secondary hyperlipoproteinemia. J. Am. Vet. Med. Assoc. 1975, 166, 1092–1100. [Google Scholar]
- Gaafer, O.U.; Zimmers, T.A. Nutrition challenges of cancer cachexia. J. Parenter. Enter. Nutr. 2021, 45, 16–25. [Google Scholar] [CrossRef]
- Ogilvie, G.K.; Vail, D.M. Nutrition and cancer: Recent developments. Vet. Clin. N. Am. Small Anim. Pract. 1990, 20, 969–985. [Google Scholar] [CrossRef] [PubMed]
- Ogilvie, G.K. Interventional nutrition for the cancer patient. Clin. Tech. Small Anim. Pract. 1998, 13, 224–231. [Google Scholar] [CrossRef] [PubMed]
- Bozzetti, F.; Pagnoni, A.M.; Del Vecchio, M. Excessive caloric expenditure as a cause of malnutrition in patients with cancer. Surg. Gynecol. Obstet. 1980, 150, 229–234. [Google Scholar] [PubMed]
- Holroyde, C.P.; Skutches, C.L.; Boden, G.; Reichard, G.A. Glucose metabolism in cachectic patients with colorectal cancer. Cancer Res. 1984, 44, 5910–5913. [Google Scholar] [PubMed]
- DeWys, W.D. Pathophysiology of cancer cachexia: Current understanding and areas for future research. Cancer Res. 1982, 42, 721s–726s. [Google Scholar] [PubMed]
- Vail, D.M.; Ogilvie, G.K.; Wheeler, S.L.; Fettman, M.J.; Johnston, S.D.; Hegstad, R.L. Alterations in carbohydrate metabolism in canine lymphoma. J. Vet. Intern. Med. 1990, 4, 8–11. [Google Scholar] [CrossRef]
- Mazzaferro, E.M.; Hackett, T.B.; Stein, T.P.; Ogilvie, G.K.; Wingfield, W.E.; Walton, J.; Turner, A.S.; Fettman, M.J. Metabolic alterations in dogs with osteosarcoma. Am. J. Vet. Res. 2001, 62, 1234–1239. [Google Scholar] [CrossRef] [PubMed]
- Bullock, A.F.; Greenley, S.L.; McKenzie, G.A.G.; Paton, L.W.; Johnson, M.J. Relationship between markers of malnutrition and clinical outcomes in older adults with cancer: Systematic review, narrative synthesis and meta-analysis. Eur. J. Clin. Nutr. 2020, 74, 1519–1535. [Google Scholar] [CrossRef]
- Romano, F.R.; Heinze, C.R.; Barber, L.G.; Mason, J.B.; Freeman, L.M. Association between Body Condition Score and Cancer Prognosis in Dogs with Lymphoma and Osteosarcoma. J. Vet. Intern. Med. 2016, 30, 1179–1186. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.S.; Lee, J.J.; Liao, A.T.; Kao, C.L.; Wang, S.L. Association between weight change during initial chemotherapy and clinical outcome in dogs with multicentric lymphoma. Vet. Comp. Oncol. 2021, 19, 53–60. [Google Scholar] [CrossRef]
- Giuffrida, M.A.; Kerrigan, S.M. Quality of life measurement in prospective studies of cancer treatments in dogs and cats. J. Vet. Intern. Med. 2014, 28, 1824–1829. [Google Scholar] [CrossRef]
- Persson, C.; Glimelius, B. The relevance of weight loss for survival and quality of life in patients with advanced gastrointestinal cancer treated with palliative chemotherapy. Anticancer Res. 2002, 22, 3661–3668. [Google Scholar]
- Kasvis, P.; Vigano, M.; Vigano, A. Health-related quality of life across cancer cachexia stages. Ann. Palliat. Med. 2019, 8, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Vøls, K.K.; Heden, M.A.; Kristensen, A.T.; Sandøe, P. Quality of life assessment in dogs and cats receiving chemotherapy—A review of current methods. Vet. Comp. Oncol. 2017, 15, 684–691. [Google Scholar] [CrossRef]
- Saker, K.E. Nutritional Concerns for Cancer, Cachexia, Frailty, and Sarcopenia in Canine and Feline Pets. Vet. Clin. N. Am. Small Anim. Pract. 2021, 51, 729–744. [Google Scholar] [CrossRef] [PubMed]
- Freedman, B. Equipoise and the ethics of clinical research. N. Engl. J. Med. 1987, 317, 141–145. [Google Scholar] [CrossRef] [PubMed]
- Michels, K.B.; Rothman, K.J. Update on unethical use of placebos in randomised trials. Bioethics 2003, 17, 188–204. [Google Scholar] [CrossRef]
- Castro, M. Placebo versus best-available-therapy control group in clinical trials for pharmacologic therapies: Which is better? Proc. Am. Thorac. Soc. 2007, 4, 570–573. [Google Scholar] [CrossRef]
- Punt, N.P.; Johannes, C.M.; Hackbarth, L.R.; Fox, L.E. Clinical survey of veterinary specialists evaluating management of chemotherapy induced vomiting and inappetence in dogs. J. Vet. Intern. Med. 2017, 31, O13. [Google Scholar]
- Zollers, B.; Wofford, J.A.; Heinen, E.; Huebner, M.; Rhodes, L. A Prospective, Randomized, Masked, Placebo-Controlled Clinical Study of Capromorelin in Dogs with Reduced Appetite. J. Vet. Intern. Med. 2016, 30, 1851–1857. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Nutrient | Dry Matter |
|---|---|
| Protein | 29.31% |
| Fat | 24.45% |
| Carbohydrate | 39.29% |
| Total dietary fiber | 8.40% |
| Arginine | 1.50% |
| Carnitine | 375.10 mg/kg |
| Total omega-3 fatty acids | 1.18% |
| EPA | 0.40% |
| DHA | 0.26% |
| Total omega-6 fatty acids | 3.73% |
| Ash | 4.95% |
| Calcium | 0.76% |
| Phosphorus | 0.55% |
| Sodium | 0.33% |
| Potassium | 0.89% |
| Magnesium | 0.09% |
| Vitamin E | 937.00 IU/kg |
| Vitamin C | 280.00 ppm |
| Vitamin A | 43,200.00 IU/kg |
| Vitamin D | 3080.00 IU/kg |
| Ingredients: Chicken, Whole Grain Wheat, Corn Gluten Meal, Chicken Fat, Hydrolyzed Chicken Liver, Soybean Meal, Brown Rice, Cracked Pearled Barley, Egg Product, Chicken Liver Flavor, Coconut Oil, Fish Oil, Ground Pecan Shells, Pork Liver Flavor, Lactic Acid, Calcium Carbonate, Potassium Citrate, Flaxseed, Dried Beet Pulp, Dried Citrus Pulp, Carrots, Iodized Salt, DL-Methionine, Pressed Cranberries, vitamins (Vitamin E Supplement, L-Ascorbyl-2-Polyphosphate (source of Vitamin C), Niacin Supplement, Thiamine Mononitrate, Calcium Pantothenate, Vitamin A Supplement, Riboflavin Supplement, Biotin, Pyridoxine Hydrochloride, Vitamin B12 Supplement, Folic Acid, Vitamin D3 Supplement), Choline Chloride, L-Tryptophan, Natural Flavors, minerals (Ferrous Sulfate, Zinc Oxide, Copper Sulfate, Manganous Oxide, Calcium Iodate, Sodium Selenite), Taurine, Mixed Tocopherols for freshness, L-Carnitine, Beta-Carotene. | |
| AAFCO statement: Animal feeding tests using AAFCO procedures substantiate that Hill’s Prescription Diet ONC Care with Chicken Dog Food provides complete and balanced nutrition for maintenance of adult dogs. | |
| Tumor Type | n |
|---|---|
| Lipoma Adnexal Adenoma/cystadenoma Histiocytoma Keratinizing Lung neoplasia Extramedullary plasma cell tumor | 18 2 1 1 1 1 1 |
| Total benign | 25 |
| Mast cell tumor Malignant melanoma/melanosarcoma Perivascular wall tumor Osteosarcoma/multilobular osteochondrosarcoma Hemangiosarcoma Lymphoma Squamous cell carcinoma Mammary epithelial tumor Bronchoalveolar carcinoma Soft tissue sarcoma Splenic sarcoma Sarcoma Anal sac gland adenocarcinoma Spindle cell sarcoma Gastrointestinal stromal tumor Nasal sarcoma Prostatic | 17 3 2 2 2 2 2 1 1 1 1 1 1 1 1 1 1 |
| Total malignant | 40 |
| All Dogs | With Benign Tumor | With Malignant Tumor | |
|---|---|---|---|
| N (%) | 65 (100) | 25 (38.5) | 40 (61.5) |
| Age (y) | 9.34 ± 2.64 | 8.82 ± 2.85 | 9.67 ± 2.48 |
| Weight (kg) | 28.0 ± 10.6 † | 24.7 ± 11.3 | 30.1 ± 9.7 1 |
| Gender (n, %) | |||
| Female | 34 (52.3) | 12 (48.0) | 22 (55.0) |
| Male | 31 (47.7) | 13 (52.0) | 18 (45.0) |
| Breed (n, %) | |||
| Purebreed | 26 (40.0) | 11 (44.0) | 15 (37.5) |
| Mixed | 39 (60.0) | 14 (56.0) | 25 (62.5) |
| Assessment | Tumor Type | Slope (SE) | 95% CI Lower, Upper | p Value |
|---|---|---|---|---|
| Stool scores | All | −0.004 (0.006) | −0.017, 0.008 | 0.4838 |
| Benign | 0.005 (0.008) | −0.012, 0.022 | 0.5184 | |
| Malignant | −0.011 (0.009) | −0.028, 0.007 | 0.2202 | |
| Enthusiasm for eating food | All | −0.027 (0.008) | −0.042, −0.012 | 0.0008 |
| Benign | −0.010 (0.006) | −0.022, 0.003 | 0.1165 | |
| Malignant | −0.038 (0.012) | −0.062, −0.014 | 0.0028 | |
| Dog’s strength | All | −0.044 (0.066) | −0.178, 0.090 | 0.5134 |
| Benign | 0.032 (0.019) | −0.008, 0.072 | 0.1126 | |
| Malignant | −0.098 (0.113) | −0.331, 0.135 | 0.3925 | |
| Dog’s energy level | All | 0.050 (0.096) | −0.143, 0.244 | 0.6036 |
| Benign | 0.105 (0.075) | −0.050, 0.259 | 0.1753 | |
| Malignant | 0.002 (0.161) | −0.329, 0.332 | 0.9916 | |
| Dog’s vitality | All | −0.034 (0.087) | −0.211, 0.144 | 0.7030 |
| Benign | 0.063 (0.051) | −0.043, 0.168 | 0.2335 | |
| Malignant | −0.107 (0.148) | −0.413, 0.199 | 0.4781 | |
| Vomited in last 48 h | All | 0.018 (0.067) | −0.117, 0.153 | 0.7901 |
| Benign | −0.063 (0.106) | −0.282, 0.156 | 0.5555 | |
| Malignant | 0.079 (0.087) | −0.101, 0.259 | 0.3742 | |
| Dog is playful today | All | 0.008 (0.099) | −0.192, 0.208 | 0.9351 |
| Benign | 0.162 (0.168) | −0.185, 0.509 | 0.3456 | |
| Malignant | −0.103 (0.118) | −0.349, 0.142 | 0.3922 | |
| Capable of doing favorite activity | All | −0.131 (0.066) | −0.265, 0.002 | 0.0540 |
| Benign | −0.009 (0.040) | −0.091, 0.073 | 0.8261 | |
| Malignant | −0.225 (0.111) | −0.452, 0.003 | 0.0524 | |
| Acted like normal today | All | −0.200 (0.087) | −0.376, −0.024 | 0.0267 |
| Benign | −0.017 (0.061) | −0.142, 0.109 | 0.7864 | |
| Malignant | −0.349 (0.148) | −0.659, −0.039 | 0.0293 | |
| Dog is joyful today | All | −0.131 (0.082) | −0.297, 0.036 | 0.1205 |
| Benign | 0.075 (0.070) | −0.069, 0.219 | 0.2929 | |
| Malignant | −0.299 (0.135) | −0.589, −0.010 | 0.0436 | |
| Enjoyed being near me today | All | −0.100 (0.064) | −0.249, 0.049 | 0.1579 |
| Benign | −0.022 (0.017) | −0.056, 0.012 | 0.1950 | |
| Malignant | −0.181 (0.132) | −0.685, 0.322 | 0.2886 | |
| Dog showed normal affection | All | −0.070 (0.063) | −0.206, 0.066 | 0.2868 |
| Benign | 0.018 (0.048) | −0.082, 0.117 | 0.7161 | |
| Malignant | -0.122 (0.098) | −0.358, 0.115 | 0.2595 | |
| Enjoyed being petted or touched | All | −0.182 (0.128) | −0.446, 0.082 | 0.1675 |
| Benign | −0.004 (0.017) | −0.038, 0.031 | 0.8348 | |
| Malignant | −0.309 (0.220) | −0.774, 0.156 | 0.1779 | |
| Dog sleeps well | All | −0.059 (0.044) | −0.148, 0.030 | 0.1855 |
| Benign | −0.015 (0.033) | −0.082, 0.052 | 0.6500 | |
| Malignant | −0.107 (0.080) | −0.280, 0.066 | 0.2046 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Anthony, R.M.; Amundson, M.D.; Brejda, J.; Becvarova, I. Acceptance of a Novel, Highly Palatable, Calorically Dense, and Nutritionally Complete Diet in Dogs with Benign and Malignant Tumors. Vet. Sci. 2023, 10, 148. https://doi.org/10.3390/vetsci10020148
Anthony RM, Amundson MD, Brejda J, Becvarova I. Acceptance of a Novel, Highly Palatable, Calorically Dense, and Nutritionally Complete Diet in Dogs with Benign and Malignant Tumors. Veterinary Sciences. 2023; 10(2):148. https://doi.org/10.3390/vetsci10020148
Chicago/Turabian StyleAnthony, Reshma M., Madison D. Amundson, John Brejda, and Iveta Becvarova. 2023. "Acceptance of a Novel, Highly Palatable, Calorically Dense, and Nutritionally Complete Diet in Dogs with Benign and Malignant Tumors" Veterinary Sciences 10, no. 2: 148. https://doi.org/10.3390/vetsci10020148