
Physiotherapeutic Strategies and Their Current Evidence for Canine Osteoarthritis


Abstract
:Simple Summary
Abstract
1. Introduction
2. Role of Physiotherapy in Management of Osteoarthritis
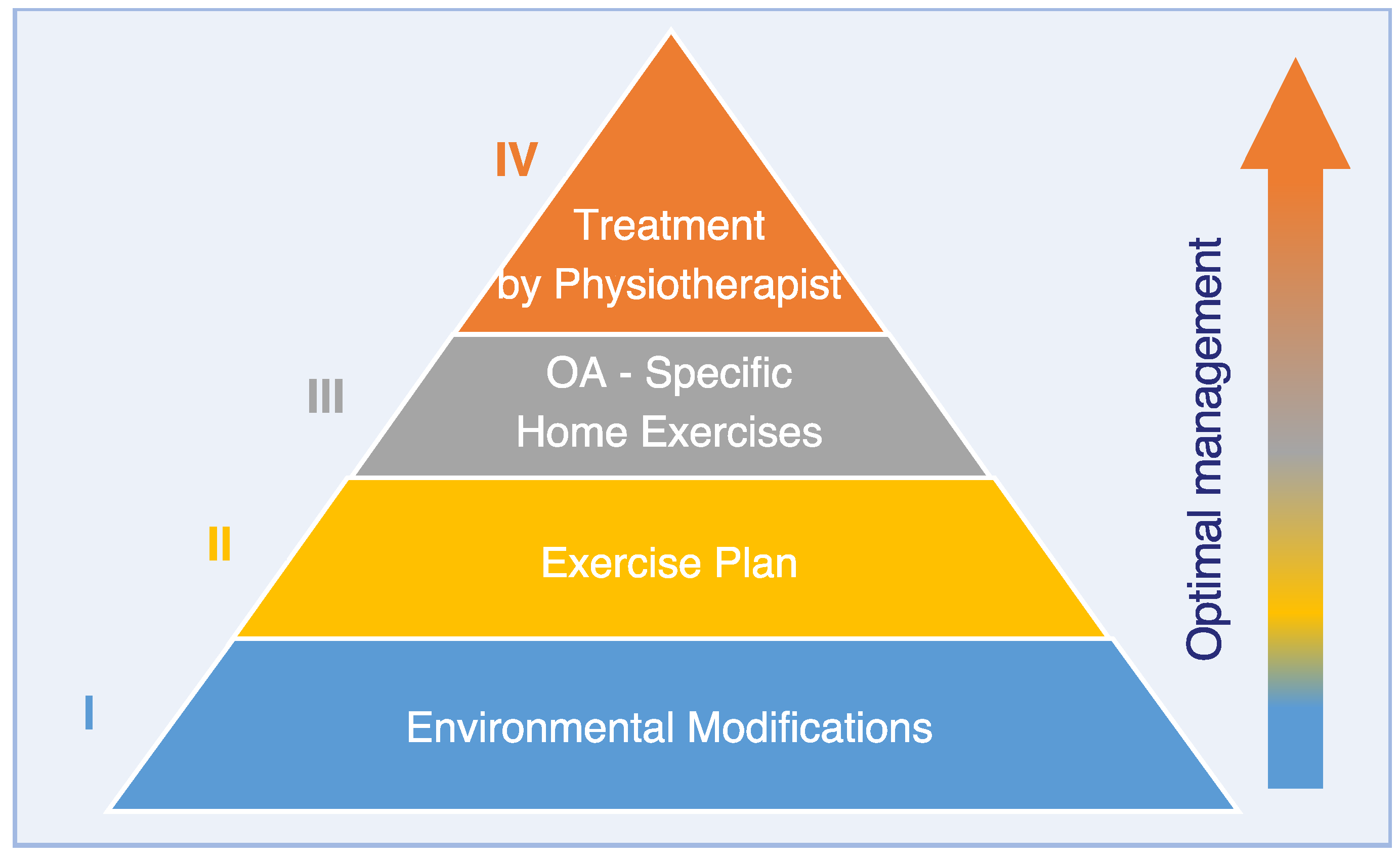
3. Physical Therapy Pyramid
3.1. Pyramid Level I: Environmental Modification
3.2. Pyramid Level II: Exercise Regimen/Activity
3.3. Pyramid Level III: OA Specific Home Exercises
3.3.1. Introduction
3.3.2. Strengthening Exercises
3.3.3. Passive Range of Motion (ROM) Techniques
3.3.4. Proprioceptive and Balance Exercises
3.3.5. Massage
3.3.6. Aquatic Exercise
3.4. Pyramid Level IV: Treatment by Physiotherapist
3.4.1. Role of a Physiotherapist in Treatment of Osteoarthritis
3.4.2. Physiotherapeutic Assessment in Canine OA
4. Efficacy of Modalities Applicable by Physiotherapists
4.1. Low Level Laser Therapy (LLLT) in Osteoarthritis
4.2. Therapeutic Ultrasound
4.3. Extracorporeal Shock Wave Therapy
4.4. Electrotherapy
4.4.1. Electrotherapy in Canine Osteoarthritis
4.4.2. Interferential Current
4.4.3. Neuromuscular Electrical Stimulation
4.4.4. Transcutaneous Electrical Nerve Stimulation
4.4.5. Capacitive-Resistive Electric Transfer (CRET)
5. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Anderson, K.; O’Neill, D.G.; Brodbelt, D.C.; Church, D.B.; Meeson, R.L.; Sargan, D.R.; Summers, J.F.; Zulch, H.; Collins, L.M. Prevalence, duration and risk factors for appendicular osteoarthritis in a UK dog population under primary veterinary care. Sci. Rep. 2018, 8, 5641. [Google Scholar] [CrossRef] [PubMed]
- O′neill, D.G.; Church, D.B.; McGreevy, P.D.; Thomson, P.C.; Brodbelt, D.C. Prevalence of Disorders Recorded in Dogs Attending Primary-Care Veterinary Practices in England. PLoS ONE 2014, 9, e90501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belshaw, Z.; Dean, R.; Asher, L. “You can be blind because of loving them so much”: The impact on owners in the United Kingdom of living with a dog with osteoarthritis. BMC Vet. Res. 2020, 16, 190. [Google Scholar] [CrossRef] [PubMed]
- Belshaw, Z.; Dean, R.; Asher, L. Slower, shorter, sadder: A qualitative study exploring how dog walks change when the canine participant develops osteoarthritis. BMC Vet. Res. 2020, 16, 85. [Google Scholar] [CrossRef]
- Gore, M.; Lana, S.E.; Bishop, G.A. Colorado State University, Pet Hospice Program. Vet. Clin. N. Am. Small Anim. Pract. 2019, 49, 339–349. [Google Scholar] [CrossRef]
- Catarino, J.; Carvalho, P.; Santos, S.; Martins, Â.; Requicha, J. Treatment of canine osteoarthritis with allogeneic platelet-rich plasma: Review of five cases. Open Vet. J. 2020, 10, 226–231. [Google Scholar] [CrossRef]
- Johnston, S.A.; McLaughlin, R.M.; Budsberg, S.C. Nonsurgical Management of Osteoarthritis in Dogs. Vet. Clin. N. Am. Small Anim. Pract. 2008, 38, 1449–1470. [Google Scholar] [CrossRef]
- Lauer, S. Preword. In Essential Facts of Physical Medicine, Rehabilitation and Sports Medicine in Companion Animals; Bockstahler, B., Ed.; VBS GmbH: Babenhausen, Germany, 2019; pp. 3–4. [Google Scholar]
- Caring for a dog with osteoarthritis. Vet. Rec. 2018, 182, 440. [CrossRef] [Green Version]
- Robinson, N.J.; Dean, R.S.; Cobb, M.; Brennan, M.L. Consultation length in first opinion small animal practice. Vet. Rec. 2014, 175, 486. [Google Scholar] [CrossRef] [Green Version]
- Marcellin-Little, D.J.; Levine, D.; Millis, D.L. Physical rehabilitation for geriatric and arthritic patients. In Canine Rehabilitation and Physical Therapy; Millis, D.L., Levine, D., Eds.; Elsevier: Amsterdam, The Netherlands, 2014; pp. 628–641. [Google Scholar]
- McLean, H.; Millis, D. Treatment plans (osteoarthritis). In Essential Facts of Physical Medicine, Rehabilitation and Sports Medicine in Companion Animals; Bockstahler, B., Wittek, K., Levine, D., Maierl, J., Millis, D., Eds.; VBS GmbH: Babenhausen, Germany, 2019; pp. 581–585. [Google Scholar]
- Langley-Hobbs, S. Patients with orthopedic disease. In BSAVA Manual of Canine and Feline Rehabilitation, Supportive and Palliative Care: Case Studies in Patient Management; Lindley, S., Watson, P., Eds.; British Small Animal Veterinary Association: Quedgeley, UK, 2010; pp. 224–231. [Google Scholar]
- Martel-Pelletier, J.; Boileau, C.; Pelletier, J.-P.; Roughley, P.J. Cartilage in normal and osteoarthritis conditions. Best Pract. Res. Clin. Rheumatol. 2008, 22, 351–384. [Google Scholar] [CrossRef]
- de Sire, A.; Marotta, N.; Marinaro, C.; Curci, C.; Invernizzi, M.; Ammendolia, A. Role of Physical Exercise and Nutraceuticals in Modulating Molecular Pathways of Osteoarthritis. Int. J. Mol. Sci. 2021, 22, 5722. [Google Scholar] [CrossRef] [PubMed]
- Knapik, D.M.; Harris, J.D.; Pangrazzi, G.; Griesser, M.J.; Siston, R.A.; Agarwal, S.; Flanigan, D.C. The Basic Science of Continuous Passive Motion in Promoting Knee Health: A Systematic Review of Studies in a Rabbit Model. Arthroscopy 2013, 29, 1722–1731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, H.-X.; Zhan, Y.-X.; Ou, H.-N.; You, Y.-Y.; Li, W.-Y.; Jiang, S.-S.; Zheng, M.-F.; Zhang, L.-Z.; Chen, K.; Chen, Q.-X. Effects of lower body positive pressure treadmill on functional improvement in knee osteoarthritis: A randomized clinical trial study. World J. Clin. Cases 2021, 9, 10604–10615. [Google Scholar] [CrossRef] [PubMed]
- Page, C.J.; Hinman, R.S.; Bennell, K.L. Physiotherapy management of knee osteoarthritis. Int. J. Rheum. Dis. 2011, 14, 145–151. [Google Scholar] [CrossRef] [PubMed]
- McAlindon, T.E.; Bannuru, R.R.; Sullivan, M.C.; Arden, N.K.; Berenbaum, F.; Bierma-Zeinstra, S.M.; Hawker, G.A.; Henrotin, Y.; Hunter, D.J.; Kawaguchi, H.; et al. OARSI guidelines for the non-surgical management of knee osteoarthritis. Osteoarthr. Cartil. 2014, 22, 363–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, C.; Lefevre-Colau, M.-M.; Poiraudeau, S.; Rannou, F. Rehabilitation (exercise and strength training) and osteoarthritis: A critical narrative review. Ann. Phys. Rehabil. Med. 2016, 59, 190–195. [Google Scholar] [CrossRef]
- Deyle, G.D.; Allison, S.C.; Matekel, R.L.; Ryder, M.G.; Stang, J.M.; Gohdes, D.D.; Hutton, J.P.; Henderson, N.E.; Garber, M.B. Physical Therapy Treatment Effectiveness for Osteoarthritis of the Knee: A Randomized Comparison of Supervised Clinical Exercise and Manual Therapy Procedures Versus a Home Exercise Program. Phys. Ther. 2005, 85, 1301–1317. [Google Scholar] [CrossRef] [Green Version]
- Bannuru, R.R.; Osani, M.C.; Vaysbrot, E.E.; Arden, N.K.; Bennell, K.; Bierma-Zeinstra, S.M.A.; Kraus, V.B.; Lohmander, L.S.; Abbott, J.H.; Bhandari, M.; et al. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthr. Cartil. 2019, 27, 1578–1589. [Google Scholar] [CrossRef] [Green Version]
- Roddy, E.; Zhang, W.; Doherty, M.; Arden, N.K.; Barlow, J.; Birrell, F.; Carr, A.; Chakravarty, K.; Dickson, J.; Hay, E.; et al. Evidence-based recommendations for the role of exercise in the management of osteoarthritis of the hip or knee--the MOVE consensus. Rheumatology 2005, 44, 67–73. [Google Scholar] [CrossRef] [Green Version]
- Bennell, K.; Buchbinder, R.; Hinman, R. Physical therapies in the management of osteoarthritis: Current state of the evidence. Curr. Opin. Rheumatol. 2015, 27, 304–311. [Google Scholar] [CrossRef]
- Coudeyre, E.; Kraus, V.B.; Rannou, F. Osteoarthritis in physical medicine and rehabilitation. Ann. Phys. Rehabil. Med. 2016, 59, 133. [Google Scholar] [CrossRef] [PubMed]
- Mazzei, D.R.; Ademola, A.; Abbott, J.H.; Sajobi, T.; Hildebrand, K.; Marshall, D.A. Are education, exercise and diet interventions a cost-effective treatment to manage hip and knee osteoarthritis? A systematic review. Osteoarthr. Cartil. 2020, 29, 456–470. [Google Scholar] [CrossRef] [PubMed]
- Conaghan, P.G.; Dickson, J.; Grant, R.L. Care and management of osteoarthritis in adults: Summary of NICE guidance. BMJ 2008, 336, 502–503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Douglas, W.W.; Malcolm, J.L. The effect of localized cooling on conduction in cat nerves. J. Physiol. 1955, 130, 53–71. [Google Scholar] [CrossRef]
- Ely, T.S.; Goldman, D.E.; Hearon, J.Z. Heating Characteristics of Laboratory Animals Exposed to Ten-Centimeter Microwaves. IEEE Trans. Biomed. Eng. 1964, 11, 123–137. [Google Scholar] [CrossRef]
- Waller, B.; Ogonowska-Slodownik, A.; Vitor, M.; Lambeck, J.; Daly, D.; Kujala, U.; Heinonen, A. Effect of Therapeutic Aquatic Exercise on Symptoms and Function Associated With Lower Limb Osteoarthritis: Systematic Review With Meta-Analysis. Phys. Ther. 2014, 94, 1383–1395. [Google Scholar] [CrossRef]
- Tomazoni, S.S.; Leal-Junior, E.C.P.; Pallotta, R.C.; Teixeira, S.; de Almeida, P.; Lopes-Martins, R.B. Effects of photobiomodulation therapy, pharmacological therapy, and physical exercise as single and/or combined treatment on the inflammatory response induced by experimental osteoarthritis. Lasers Med. Sci. 2016, 32, 101–108. [Google Scholar] [CrossRef]
- Zhao, Z.; Ji, H.; Jing, R.; Liu, C.; Wang, M.; Zhai, L.; Bai, X.; Xing, G. Extracorporeal shock-wave therapy reduces progression of knee osteoarthritis in rabbits by reducing nitric oxide level and chondrocyte apoptosis. Arch. Orthop. Trauma Surg. 2012, 132, 1547–1553. [Google Scholar] [CrossRef]
- Johnson, J.M.; Johnson, A.L.; Pijanowski, G.J.; Kneller, S.K.; Schaeffer, D.; Eurell, J.A.; Smith, C.W.; Swan, K.S. Rehabilitation of dogs with surgically treated cranial cruciate ligament-deficient stifles by use of electrical stimulation of muscles. Am. J. Vet. Res. 1997, 58, 1473–1478. [Google Scholar]
- Barnes, K.; Faludi, A.; Takawira, C.; Aulakh, K.; Rademacher, N.; Liu, C.; Lopez, M.J. Extracorporeal shock wave therapy improves short-term limb use after canine tibial plateau leveling osteotomy. Vet. Surg. 2019, 48, 1382–1390. [Google Scholar] [CrossRef]
- Marsolais, G.S.; Dvorak, G.; Conzemius, M.G. Effects of postoperative rehabilitation on limb function after cranial cruciate ligament repair in dogs. J. Am. Vet. Med. Assoc. 2002, 220, 1325–1330. [Google Scholar] [CrossRef] [PubMed]
- Upariputti, R.; Vijarnsorn, M.; Niyom, S.; Boonyong, S. Effect of interferential current therapy on ground reaction force in dogs with hip osteoarthritis: A randomized placebo controlled cross-over clinical trial. Thai J. Vet. Med. 2018, 48, 111–116. [Google Scholar]
- Fitch, G.; Evans, R.B.; McClure, S.R.; Conzemius, M.; Dahlberg, J. The evaluation of extracorporeal shockwave therapy in naturally occurring osteoarthritis of the stifle joint in dogs. Vet. Comp. Orthop. Traumatol. 2005, 18, 147–152. [Google Scholar] [CrossRef]
- Millis, D.; Drum, M.; Whitlock, D. Complementary Use of Extracorporeal Shock Wave Therapy on Elbow Osteoarthritis in Dogs. Vet. Comp. Orthop. Traumatol. 2011, 24, A1. [Google Scholar]
- Mueller, M.; Bockstahler, B.; Skalicky, M.; Mlacnik, E.; Lorinson, D. Effects of radial shockwave therapy on the limb function of dogs with hip osteoarthritis. Vet. Rec. 2007, 160, 762–765. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, M.P.; Hagen, S.C.F.; Patricio, G.C.F.; Matera, J.M.; Souza, A.N.A. Radial shock wave therapy in dogs with hip osteoarthritis. Vet. Comp. Orthop. Traumatol. 2016, 29, 108–114. [Google Scholar] [CrossRef] [Green Version]
- Barale, L.; Monticelli, P.; Raviola, M.; Adami, C. Preliminary clinical experience of low-level laser therapy for the treatment of canine osteoarthritis-associated pain: A retrospective investigation on 17 dogs. Open Vet. J. 2020, 10, 116–119. [Google Scholar] [CrossRef]
- Looney, A.L.; Huntingford, J.L.; Blaeser, L.L.; Mann, S. A randomized blind placebo-controlled trial investigating the effects of photobiomodulation therapy (PBMT) on canine elbow osteoarthritis. Can. Vet. J. 2018, 59, 959–966. [Google Scholar]
- Crook, T.; McGowan, C.; Pead, M. Effect of passive stretching on the range of motion of osteoarthritic joints in 10 labrador retrievers. Vet. Rec. 2007, 160, 545–547. [Google Scholar] [CrossRef]
- Fox, S.M. Multimodal Management of Canine Osteoarthritis, 2nd ed.; Group T and F, Ed.; CRC Press: Boca Raton, FL, USA, 2016. [Google Scholar]
- Millis, D.L. Getting the Dog Moving After Surgery. J. Am. Anim. Hosp. Assoc. 2004, 40, 429–436. [Google Scholar] [CrossRef]
- Swaim, S.F.; Votau, K. Prevention and treatment of decubital ulcers in the dog. Vet. Med. small Anim. Clin. 1975, 70, 1069–1074. [Google Scholar] [PubMed]
- Adamson, C.; Kaufmann, M.; Levine, D.; Millis, D.L.; Marcellin-Little, D.J. Assistive Devices, Orthotics, and Prosthetics. Vet. Clin. N. Am. Small Anim. Pract. 2005, 35, 1441–1451. [Google Scholar] [CrossRef] [PubMed]
- Esser, S.; Bailey, A. Effects of Exercise and Physical Activity on Knee Osteoarthritis. Curr. Pain Headache Rep. 2011, 15, 423–430. [Google Scholar] [CrossRef] [PubMed]
- Martel-Pelletier, J.; Lajeunesse, D.; Fahmi, H.; Tardif, G.; Pelletier, J.-P. New thoughts on the pathophysiology of osteoarthritis: One more step toward new therapeutic targets. Curr. Rheumatol. Rep. 2006, 8, 30–36. [Google Scholar] [CrossRef]
- Kiviranta, I.; Tammi, M.; Jurvelin, J.; Säämänen, A.-M.; Helminen, H.J. Moderate running exercise augments glycosaminoglycans and thickness of articular cartilage in the knee joint of young beagle dogs. J. Orthop. Res. 1988, 6, 188–195. [Google Scholar] [CrossRef] [PubMed]
- Chakravarty, E.F.; Hubert, H.B.; Lingala, V.B.; Zatarain, E.; Fries, J.F. Long Distance Running and Knee Osteoarthritis: A Prospective Study. Am. J. Prev. Med. 2008, 35, 133–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kraus, V.B.; Sprow, K.; Powell, K.E.; Buchner, D.; Bloodgood, B.; Piercy, K.; George, S.M.; Kraus, W.E. Effects of Physical Activity in Knee and Hip Osteoarthritis: A Systematic Umbrella Review. Med. Sci. Sports Exerc. 2019, 51, 1324–1339. [Google Scholar] [CrossRef]
- Warburton, D.E.R.; Bredin, S.S.D. Health benefits of physical activity: A systematic review of current systematic reviews. Curr. Opin. Cardiol. 2017, 32, 541–556. [Google Scholar] [CrossRef]
- Lee, A.H.; Detweiler, K.B.; Harper, T.A.; Knap, K.E.; de Godoy, M.R.C.; Swanson, K.S. Physical activity patterns of free living dogs diagnosed with osteoarthritis. J. Anim. Sci. 2021, 99, skab204. [Google Scholar] [CrossRef]
- Preet, G.S.; Turkar, S.; Gupta, S.; Kumar, S. Dog obesity: Epidemiology, risk factors, diagnosis and management: A review pa-per. Pharma. Innov. J. 2021, 10, 698–705. [Google Scholar]
- Bockstahler, B.A.; Hulse, D.A.; Carmichael, S.; Marshall, W.G. A review of osteoarthritis and obesity: Current understanding of the relationship and benefit of obesity treatment and prevention in the dog. Vet. Comp. Orthop. Traumatol. 2009, 22, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Piantedosi, D.; Di Loria, A.; Guccione, J.; De Rosa, A.; Fabbri, S.; Cortese, L.; Carta, S.; Ciaramella, P. Serum biochemistry profile, inflammatory cytokines, adipokines and cardiovascular findings in obese dogs. Vet. J. 2016, 216, 72–78. [Google Scholar] [CrossRef] [PubMed]
- Ostlund, R.E., Jr.; Yang, J.W.; Klein, S.; Gingerich, R. Relation between plasma leptin concentration and body fat, gender, diet, age, and metabolic covariates. J. Clin. Endocrinol. Metab. 1996, 81, 3909–3913. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Millis, D.L.; Levine, D. The Role of Exercise and Physical Modalities in The Treatment of Osteoarthritis. Vet. Clin. N. Am. Small Anim. Pract. 1997, 27, 913–930. [Google Scholar] [CrossRef] [PubMed]
- Abbott, J.H.; Robertson, M.C.; Chapple, C.; Pinto, D.; Wright, A.A.; De La Barra, S.L.; Baxter, G.D.; Theis, J.-C.; Campbell, A.J.; MOA Trial Team. Manual therapy, exercise therapy, or both, in addition to usual care, for osteoarthritis of the hip or knee: A randomized controlled trial. 1: Clinical effectiveness. Osteoarthr. Cartil. 2013, 21, 525–534. [Google Scholar] [CrossRef]
- French, H.P.; Cusack, T.; Brennan, A.; Caffrey, A.; Conroy, R.; Cuddy, V.; Fitzgerald, O.M.; Gilsenan, C.; Kane, D.; O’Connell, P.G.; et al. Exercise and manual physiotherapy arthritis research trial (EMPART) for osteoarthritis of the hip: A multicenter randomized controlled trial. Arch. Phys. Med. Rehabil. 2013, 94, 302–314. [Google Scholar] [CrossRef]
- Millis, D.L.; Drum, M.; Levine, D. Therapeutic exercises: Early limb use exercises. In Canine Rehabilitation and Physical Therapy; Millis, D.L., Levine, D., Eds.; Elsevier: Amsterdam, The Netherlands, 2014; pp. 495–505. [Google Scholar]
- Fransen, M.; McConnell, S.; Bell, M. Therapeutic exercise for people with osteoarthritis of the hip or knee. A systematic review. J. Rheumatol. 2002, 29, 1737–1745. [Google Scholar]
- Roos, E.M.; Herzog, W.; Block, J.A.; Bennell, K.L. Muscle weakness, afferent sensory dysfunction and exercise in knee osteoarthritis. Nat. Rev. Rheumatol. 2010, 7, 57–63. [Google Scholar] [CrossRef]
- O’Reilly, S.; Jones, A.; Doherty, M. Muscle weakness in osteoarthritis. Curr. Opin. Rheumatol. 1997, 9, 259–262. [Google Scholar] [CrossRef]
- De Zwart, A.H.; Van Der Esch, M.; Pijnappels, M.; Hoozemans, M.; Van Der Leeden, M.; Roorda, L.D.; Dekker, J.; Lems, W.F.; van Dieen, J. Falls Associated with Muscle Strength in Patients with Knee Osteoarthritis and Self-reported Knee Instability. J. Rheumatol. 2015, 42, 1218–1223. [Google Scholar] [CrossRef] [Green Version]
- Runhaar, J.; Luijsterburg, P.; Dekker, J.; Bierma-Zeinstra, S.M. Identifying potential working mechanisms behind the positive effects of exercise therapy on pain and function in osteoarthritis; a systematic review. Osteoarthr. Cartil. 2015, 23, 1071–1082. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jansen, M.J.; Viechtbauer, W.; Lenssen, A.F.; Hendriks, E.J.; de Bie, R.A. Strength training alone, exercise therapy alone, and exercise therapy with passive manual mobilisation each reduce pain and disability in people with knee osteoarthritis: A systematic review. J. Physiother. 2011, 57, 11–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pelland, L.; Brosseau, L.; Wells, G.; MacLeay, L.; Lambert, J.; Lamothe, C.; Robinson, V.; Tugwell, P. Efficacy of strengthening exercises for osteoarthritis (Part I): A meta-analysis. Phys. Ther. Rev. 2004, 9, 77–108. [Google Scholar] [CrossRef]
- Latham, N.; Liu, C.-J. Strength Training in Older Adults: The Benefits for Osteoarthritis. Clin. Geriatr. Med. 2010, 26, 445–459. [Google Scholar] [CrossRef] [Green Version]
- Millis, D.L.; Levine, D. Exercises for proprioception and balance. In Canine Rehabilitation and Physical Therapy, 2nd ed.; Millis, D.L., Levine, D., Eds.; Elsevier: Amsterdam, The Netherlands, 2014; pp. 484–493. [Google Scholar]
- Drum, M.; McKay, E.; Levine, D.; Marcellin-Little, D.J. The Role of Strengthening in the Management of Canine Osteoarthritis. Adv. Small Anim. Care 2021, 2, 31–38. [Google Scholar] [CrossRef]
- Zink, C.; Van Dyke, J. Canine Sports Medicine and Rehabilitation, 2nd ed.; Wiley Blackwell: Hoboken, NJ, USA, 2018. [Google Scholar]
- Uthman, O.A.; van der Windt, D.A.; Jordan, J.; Dziedzic, K.S.; Healey, E.L.; Peat, G.M.; Foster, N.E. Exercise for lower limb osteoarthritis: Systematic review incorporating trial sequential analysis and network meta-analysis. Br. J. Sports Med. 2014, 48, 1579. [Google Scholar] [CrossRef] [PubMed]
- Marks, R.; Allegrante, J.P. Chronic Osteoarthritis and Adherence to Exercise: A Review of the Literature. J. Aging Phys. Act. 2005, 13, 434–460. [Google Scholar] [CrossRef] [PubMed]
- Carrier, D.R.; Deban, S.M.; Fischbein, T. Locomotor function of forelimb protractor and retractor muscles of dogs:evidence of strut-like behavior at the shoulder. J. Exp. Biol. 2008, 211 Pt 1, 150–162. [Google Scholar] [CrossRef] [Green Version]
- Deban, S.M.; Schilling, N.; Carrier, D.R. Activity of extrinsic limb muscles in dogs at walk, trot and gallop. J. Exp. Biol. 2012, 215, 287–300. [Google Scholar] [CrossRef] [Green Version]
- Holler, P.J.; Brazda, V.; Dal-Bianco, B.; Lewy, E.; Mueller, M.C.; Peham, C.; Bockstahler, B.A. Kinematic motion analysis of the joints of the forelimbs and hind limbs of dogs during walking exercise regimens. Am. J. Vet. Res. 2010, 71, 734–740. [Google Scholar] [CrossRef]
- Salter, R.B.; Simmonds, D.F.; Malcolm, B.W.; Rumble, E.J.; MacMichael, D.; Clements, N.D. The biological effect of continuous passive motion on the healing of full-thickness defects in articular cartilage. An experimental investigation in the rabbit. J. Bone Jt. Surg. Am. 1980, 62, 1232–1251. [Google Scholar] [CrossRef]
- D’Amore, T.; Rao, S.; Corvi, J.; Jack, I.R.A.; Tjoumakaris, F.P.; Ciccotti, M.G.; Freedman, K.B. The Utility of Continuous Passive Motion After Anterior Cruciate Ligament Reconstruction: A Systematic Review of Comparative Studies. Orthop. J. Sports Med. 2021, 9, 23259671211013840. [Google Scholar] [CrossRef] [PubMed]
- Richter, M.; Trzeciak, T.; Kaczmarek, M. Effect of continuous passive motion on the early recovery outcomes after total knee arthroplasty. Int. Orthop. 2021, 46, 549–553. [Google Scholar] [CrossRef] [PubMed]
- Nugent-Derfus, G.E.; Takara, T.; O’Neill, J.; Cahill, S.; Görtz, S.; Pong, T.; Inoue, H.; Aneloski, N.; Wang, W.; Vega, K.; et al. Continuous passive motion applied to whole joints stimulates chondrocyte biosynthesis of PRG4. Osteoarthr. Cartil. 2007, 15, 566–574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kitay, G.S.; Koren, M.J.; Helfet, D.L.; Parides, M.K.; Markenson, J.A. Efficacy of combined local mechanical vibrations, continuous passive motion and thermotherapy in the management of osteoarthritis of the knee. Osteoarthr. Cartil. 2009, 17, 1269–1274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henderson, A.; Levine, D.; Millis, D.; Drum, M. Protocol Development and Protocol. In Canine Rehabilitation and Physical Therapy, 2nd ed.; Millis, D.L., Levine, D., Eds.; Elsevier: Amsterdam, The Netherlands, 2014; p. 711. [Google Scholar]
- Millis, D.L.; Levine, D. Range of motion and stretching exercises. In Canine Rehabilitation and Physical Therapy, 2nd ed.; Millis, D.L., Levine, D., Eds.; Elsevier: Amsterdam, The Netherlands, 2014; pp. 431–446. [Google Scholar]
- Saunders, D.G.; Walker, J.R.; Levine, D. Joint Mobilization. Vet. Clin. N. Am. Small Anim. Pract. 2005, 35, 1287–1316. [Google Scholar] [CrossRef]
- Fitzpatrick, R.; McCloskey, D.I. Proprioceptive, visual and vestibular thresholds for the perception of sway during standing in humans. J. Physiol. 1994, 478 Pt 1, 173–186. [Google Scholar] [CrossRef]
- Hurley, M.V.; Scott, D.L.; Rees, J.; Newham, D.J. Sensorimotor changes and functional performance in patients with knee osteoarthritis. Ann. Rheum. Dis. 1997, 56, 641–648. [Google Scholar] [CrossRef]
- Smith, T.O.; King, J.J.; Hing, C.B. The effectiveness of proprioceptive-based exercise for osteoarthritis of the knee: A systematic review and meta-analysis. Rheumatol. Int. 2012, 32, 3339–3351. [Google Scholar] [CrossRef]
- Lee, P.-A.; Wu, K.-H.; Lu, H.-Y.; Su, K.-W.; Wang, T.-M.; Liu, H.-C.; Lu, T.-W. Compromised balance control in older people with bilateral medial knee osteoarthritis during level walking. Sci. Rep. 2021, 11, 3742. [Google Scholar] [CrossRef]
- López, S.; Vilar, J.M.; Rubio, M.; Sopena, J.J.; Damiá, E.; Chicharro, D.; Santana, A.; Carrillo, J.M. Center of pressure limb path differences for the detection of lameness in dogs: A preliminary study. BMC Vet. Res. 2019, 15, 138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levinger, P.; Dunn, J.; Bifera, N.; Butson, M.; Elias, G.; Hill, K.D. High-speed resistance training and balance training for people with knee osteoarthritis to reduce falls risk: Study protocol for a pilot randomized controlled trial. Trials 2017, 18, 384. [Google Scholar] [CrossRef] [Green Version]
- Saussac, A.; Sawaya, S.G. Impact of a training program with the motorized platform Imoove-Vet in agility dogs. In Proceedings of the 6th VEPRA-1st ECVSMR Conference 2019, Ghent, Belgium, 19–21 September 2019; p. 140. [Google Scholar]
- Qin, S.; Chi, Z.; Xiao, Y.; Zhu, D.; Zhong, G.; Xu, W.; Ouyang, X.; Li, J.; Cheng, P.; Yu, T.; et al. Effectiveness and safety of massage for knee osteoarthritis: A protocol for systematic review and meta-analysis. Medicine 2020, 99, e22853. [Google Scholar] [CrossRef] [PubMed]
- Moraska, A.; Pollini, R.A.; Boulanger, K.; Brooks, M.Z.; Teitlebaum, L. Physiological Adjustments to Stress Measures Following Massage Therapy: A Review of the Literature. Evid.-Based Complement. Altern. Med. 2010, 7, 409–418. [Google Scholar] [CrossRef] [Green Version]
- Billhult, A.; Määttä, S. Light pressure massage for patients with severe anxiety. Complement. Ther. Clin. Pract. 2009, 15, 96–101. [Google Scholar] [CrossRef] [PubMed]
- Formenton, M.R.; Pereira, M.A.A.; Fantoni, D.T. Small Animal Massage Therapy: A Brief Review and Relevant Observations. Top. Companion Anim. Med. 2017, 32, 139–145. [Google Scholar] [CrossRef]
- Perlman, A.; Fogerite, S.G.; Glass, O.; Bechard, E.; Ali, A.; Njike, V.Y.; Pieper, C.; Dmitrieva, N.O.; Luciano, A.; Rosenberger, L.; et al. Efficacy and Safety of Massage for Osteoarthritis of the Knee: A Randomized Clinical Trial. J. Gen. Intern. Med. 2018, 34, 379–386. [Google Scholar] [CrossRef] [Green Version]
- Davies, L. Rehabilitation medicine: Provision of canine hydrotherapy in the UK. Vet. Rec. 2011, 168, 465–466. [Google Scholar] [CrossRef] [PubMed]
- Waining, M.; Young, I.; Williams, S.B. Evaluation of the status of canine hydrotherapy in the UK. Vet. Rec. 2011, 168, 407. [Google Scholar] [CrossRef]
- Millis, D.L.; Levine, D. Therapeutic exercise and manual therapy. In Canine Rehabilitation and Physical Therapy, 2nd ed.; Millis, D.L., Levine, D., Eds.; Saunders: Philadelphia, PA, USA, 2014; pp. 431–446. [Google Scholar]
- Bertocci, G.; Smalley, C.; Brown, N.; Bialczak, K.; Carroll, D. Aquatic treadmill water level influence on pelvic limb kinematics in cranial cruciate ligament-deficient dogs with surgically stabilised stifles. J. Small Anim. Pract. 2018, 59, 121–127. [Google Scholar] [CrossRef]
- Marsolais, G.S.; McLean, S.; Derrick, T.; Conzemius, M.G. Kinematic analysis of the hind limb during swimming and walking in healthy dogs and dogs with surgically corrected cranial cruciate ligament rupture. J. Am. Vet. Med. Assoc. 2003, 222, 739–743. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnicoat, F.; Wills, A. Effect of water depth on limb kinematics of the domestic dog (Canis lupus familiaris) during underwater treadmill exercise. Comp. Exerc. Physiol. 2016, 12, 199–207. [Google Scholar] [CrossRef]
- Vitger, A.D.; Bruhn-Rasmussen, T.; Pedersen, E.O.; Fuglsang-Damgaard, L.H.; Harrison, A.P. The impact of water depth and speed on muscle fiber activation of healthy dogs walking in a water treadmill. Acta Vet. Scand. 2021, 63, 46. [Google Scholar] [CrossRef] [PubMed]
- Parkinson, S.; Wills, A.; Tabor, G.; Williams, J. Effect of water depth on muscle activity of dogs when walking on a water tread-mill. Comp Exerc Physiol. 2018, 14, 79–89. [Google Scholar] [CrossRef] [Green Version]
- Preston, T.; Wills, A. A single hydrotherapy session increases range of motion and stride length in Labrador retrievers diagnosed with elbow dysplasia. Vet. J. Lond. Engl. 2018, 234, 105–110. [Google Scholar] [CrossRef]
- Ebelt-Paprotny, R.P.; Taxhet, G.; Wappelhorst, U. Leitfaden Physiotherapie; Elsevier Urban & Fischer: Munich, Germany, 2008. [Google Scholar]
- Belshaw, Z.; Asher, L.; Dean, R.S. Systematic Review of Outcome Measures Reported in Clinical Canine Osteoarthritis Research. Vet. Surg. VS 2016, 45, 480–487. [Google Scholar] [CrossRef]
- Allet, L.; Bürge, E.; Monnin, D. ICF: Clinical relevance for physiotherapy? A critical review. Adv. Physiother. 2008, 10, 127–137. [Google Scholar] [CrossRef]
- Skou, S.T.; Roos, E.M. Physical therapy for patients with knee and hip osteoarthritis: Supervised, active treatment is current best practice. Clin. Exp. Rheumatol. 2019, 37, 112–117. [Google Scholar] [PubMed]
- Juhl, C.; Christensen, R.; Roos, E.M.; Zhang, W.; Lund, H. Impact of Exercise Type and Dose on Pain and Disability in Knee Osteoarthritis: A Systematic Review and Meta-Regression Analysis of Randomized Controlled Trials. Arthritis Rheumatol. 2014, 66, 622–636. [Google Scholar] [CrossRef]
- Sobeck, C.; Lenk, L.; Knipper, S.; Rhoda, A.; Stickler, L.; Stephenson, P. The effectiveness of functional massage on pain and range of motion measurements in patients with orthopedic impairments of the extremities. Int. Musculoskelet. Med. 2016, 38, 21–25. [Google Scholar] [CrossRef]
- Sharman, M.J.; Cresswell, A.G.; Riek, S. Proprioceptive Neuromuscular Facilitation Stretching: Mechanisms and clinical implica-tions. Sports Med. 2006, 36, 929–939. [Google Scholar] [CrossRef] [PubMed]
- Brantingham, J.W.; Bonnefin, D.; Perle, S.M.; Cassa, T.K.; Globe, G.; Pribicevic, M.; Hicks, M.; Korporaal, C. Manipulative Therapy for Lower Extremity Conditions: Update of a Literature Review. J. Manip. Physiol. Ther. 2012, 35, 127–166. [Google Scholar] [CrossRef] [PubMed]
- Wellsandt, E.; Golightly, Y. Exercise in the management of knee and hip osteoarthritis. Curr. Opin. Rheumatol. 2018, 30, 151–159. [Google Scholar] [CrossRef]
- Kolasinski, S.L.; Kolasinski, S.L.; Neogi, T.; Neogi, T.; Hochberg, M.C.; Hochberg, M.C.; Oatis, C.; Oatis, C.; Guyatt, G.; Guyatt, G.; et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis Care Res. Hoboken 2020, 72, 149–162. [Google Scholar] [CrossRef] [PubMed]
- Bellew, J.W. Therapeutic Modalities Past, Present, and Future: Their Role in the Patient Care Management Model. In Modalities for Therapeutic Intervention, 6th ed.; Bellew, J.W., Michlovitz, S.L., Nolan, T.P., Jr., Eds.; F. A. Davis Company: Philadelphia, PA, USA, 2016. [Google Scholar]
- LoGiudice, R.J.; Starr, L. Rehabilitation for Geriatric Patients. In Canine Sports Medicine and Rehabilitation; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2018; pp. 454–478. [Google Scholar] [CrossRef]
- Niebaum, K.; McCauley, L.; Medina, C. Rehabilitation Physical Modalities. In Canine Sports Medicine and Rehabilitation; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2018; pp. 136–176. [Google Scholar] [CrossRef]
- Barger, B.K.; Bisges, A.M.; Fox, D.B.; Torres, B. Low-Level Laser Therapy for Osteoarthritis Treatment in Dogs at Missouri Veterinary Practice. J. Am. Anim. Hosp. Assoc. 2020, 56, 139–145. [Google Scholar] [CrossRef]
- Gendron, D.J.; Hamblin, M.R. Applications of Photobiomodulation Therapy to Musculoskeletal Disorders and Osteoarthritis with Particular Relevance to Canada. Photobiomodulation Photomed. Laser Surg. 2019, 37, 408–420. [Google Scholar] [CrossRef] [PubMed]
- Hagiwara, S.; Iwasaka, H.; Okuda, K.; Noguchi, T. GaAlAs (830 nm) low-level laser enhances peripheral endogenous opioid analgesia in rats. Lasers Surg. Med. 2007, 39, 797–802. [Google Scholar] [CrossRef]
- Chow, R.T.; Armati, P.J.; Laakso, E.-L.; Bjordal, J.M.; Baxter, G.D. Inhibitory Effects of Laser Irradiation on Peripheral Mammalian Nerves and Relevance to Analgesic Effects: A Systematic Review. Photomed. Laser Surg. 2011, 29, 365–381. [Google Scholar] [CrossRef]
- Rubio, C.R.; Cremonezzi, D.; Moya, M.; Soriano, F.; Palma, J.; Campana, V. Helium-Neon Laser Reduces the Inflammatory Process of Arthritis. Photomed. Laser Surg. 2010, 28, 125–129. [Google Scholar] [CrossRef] [PubMed]
- Hegedüs, B.; Viharos, L.; Gervain, M.; Gálfi, M. The Effect of Low-Level Laser in Knee Osteoarthritis: A Double-Blind, Randomized, Placebo-Controlled Trial. Photomed. Laser Surg. 2009, 27, 577–584. [Google Scholar] [CrossRef] [Green Version]
- Mantineo, M.; Pinheiro, J.P.; Morgado, A.M. Low-level laser therapy on skeletal muscle inflammation: Evaluation of irradiation parameters. J. Biomed. Opt. 2014, 19, 098002. [Google Scholar] [CrossRef]
- Welch, V.; Wells, G.; Debie, R.; Gam, A.; Harman, K.; Morin, M.; Shea, B.; Tugwell, P.; Robinson, V. Low level laser therapy (Classes I, II and III) for treating osteoarthritis. Cochrane Database Syst. Rev. 2004, 3, CD002046. [Google Scholar] [CrossRef]
- Monici, M.; Millis, D.L.; Ciuperca, I.; McCarthy, D. Laser therapy. In Essential Facts of Physical Medicine, Rehabilitation and Sports Medicine in Companion Animals; Bockstahler, B., Ed.; VBS GmbH: Babenhausen, Germany, 2019. [Google Scholar]
- Mason, T.J. Therapeutic ultrasound an overview. Ultrason. Sonochemistry 2011, 18, 847–852. [Google Scholar] [CrossRef] [PubMed]
- Yildirim, M.A.; Yıldırım, M.A.; Öneş, K.; Gökşenoğlu, G. Effectiveness of Ultrasound Therapy on Myofascial Pain Syndrome of the Upper Trapezius: Randomized, Single-Blind, Placebo-Controlled Study. Arch. Rheumatol. 2018, 33, 418–423. [Google Scholar] [CrossRef] [PubMed]
- Baker, K.G.; Robertson, V.J.; Duck, F.A. A Review of Therapeutic Ultrasound: Biophysical Effects. Phys. Ther. 2001, 81, 1351–1358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bockstahler, B.; Levine, D. Therapeutic ultrasound. In Essential Facts of Physical Medicine, Rehabilitation and Sports Medicine in Companion Animals; Bockstahler, B., Wittek, K., Levine, D., Maierl, J., Millis, D.L., Eds.; VBS GmbH: Babenhausen, Germany, 2019. [Google Scholar]
- Acevedo, B.; Millis, D.L.; Levine, D.; Guevara, J.L. Effect of Therapeutic Ultrasound on Calcaneal Tendon Heating and Extensibility in Dogs. Front. Vet. Sci. 2019, 6, 185. [Google Scholar] [CrossRef]
- Yang, Q.; Nanayakkara, G.K.; Drummer, C.; Sun, Y.; Johnson, C.; Cueto, R.; Fu, H.; Shao, Y.; Wang, L.; Yang, W.Y.; et al. Low-Intensity Ultrasound-Induced Anti-inflammatory Effects Are Mediated by Several New Mechanisms Including Gene Induction, Immunosuppressor Cell Promotion, and Enhancement of Exosome Biogenesis and Docking. Front. Physiol. 2017, 8, 818. [Google Scholar] [CrossRef] [Green Version]
- Wu, Y.; Zhu, S.; Lv, Z.; Kan, S.; Wu, Q.; Song, W.; Ning, G.; Feng, S. Effects of therapeutic ultrasound for knee osteoarthritis: A systematic review and meta-analysis. Clin. Rehabil. 2019, 33, 1863–1875. [Google Scholar] [CrossRef]
- Rothenberg, J.B.; Jayaram, P.; Naqvi, U.; Gober, J.; Malanga, G.A. The Role of Low-Intensity Pulsed Ultrasound on Cartilage Healing in Knee Osteoarthritis: A Review. PM&R 2017, 9, 1268–1277. [Google Scholar] [CrossRef]
- Goranov, N.; Stara, Z. Effect of therapeutic pulsed ultrasound in dogs with experimental stifle joint osteoarthritis. Bulg J. Vet. Med. 2010, 13, 162–168. [Google Scholar]
- Zeng, C.; Li, H.; Yang, T.; Deng, Z.-H.; Yang, Y.; Zhang, Y.; Ding, X.; Lei, G.-H. Effectiveness of continuous and pulsed ultrasound for the management of knee osteoarthritis: A systematic review and network meta-analysis. Osteoarthr. Cartil. 2014, 22, 1090–1099. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, J.H.; Wang, C.-J. Biological mechanism of shockwave in bone. Int. J. Surg. 2015, 24 Pt B, 143–146. [Google Scholar] [CrossRef]
- Cleveland, R.O.; Chitnis, P.V.; McClure, S.R. Acoustic Field of a Ballistic Shock Wave Therapy Device. Ultrasound Med. Biol. 2007, 33, 1327–1335. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.-J. Extracorporeal shockwave therapy in musculoskeletal disorders. J. Orthop. Surg. Res. 2012, 7, 11. [Google Scholar] [CrossRef] [Green Version]
- Zimmermann, R.; Cumpanas, A.; Miclea, F.; Janetschek, G. Extracorporeal Shock Wave Therapy for the Treatment of Chronic Pelvic Pain Syndrome in Males: A Randomised, Double-Blind, Placebo-Controlled Study. Eur. Urol. 2009, 56, 418–424. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.-J.; Cheng, J.-H.; Chou, W.-Y.; Hsu, S.-L.; Chen, J.-H.; Huang, C.-Y. Changes of articular cartilage and subchondral bone after extracorporeal shockwave therapy in osteoarthritis of the knee. Int. J. Med. Sci. 2017, 14, 213–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.-J.; Hsu, S.-L.; Weng, L.-H.; Sun, Y.-C.; Wang, F.-S. Extracorporeal shockwave therapy shows a number of treatment related chondroprotective effect in osteoarthritis of the knee in rats. BMC Musculoskelet. Disord. 2013, 14, 44. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.-J.; Wang, F.-S.; Yang, K.D.; Weng, L.-H.; Hsu, C.-C.; Huang, C.-S.; Yang, L.-C. Shock wave therapy induces neovascularization at the tendon–bone junction. A study in rabbits. J. Orthop. Res. 2003, 21, 984–989. [Google Scholar] [CrossRef]
- Wang, C.-J.; Wang, F.-S.; Yang, K.D. Biological effects of extracorporeal shockwave in bone healing: A study in rabbits. Arch. Orthop. Trauma. Surg. 2008, 128, 879–884. [Google Scholar] [CrossRef]
- Ohtori, S.; Inoue, G.; Mannoji, C.; Saisu, T.; Takahashi, K.; Mitsuhashi, S.; Wada, Y.; Takahashi, K.; Yamagata, M.; Moriya, H. Shock wave application to rat skin induces degeneration and reinnervation of sensory nerve fibres. Neurosci. Lett. 2001, 315, 57–60. [Google Scholar] [CrossRef]
- An, S.; Li, J.; Xie, W.; Yin, N.; Li, Y.; Hu, Y. Extracorporeal shockwave treatment in knee osteoarthritis: Therapeutic effects and possible mechanism. Biosci. Rep. 2020, 40, BSR20200926. [Google Scholar] [CrossRef] [PubMed]
- Bolt, D.M.; Burba, D.J.; Hubert, J.D.; Strain, G.M.; Hosgood, G.L.; Henk, W.G.; Cho, D.-Y. Determination of functional and morphologic changes in palmar digital nerves after nonfocused extracorporeal shock wave treatment in horses. Am. J. Vet. Res. 2004, 65, 1714–1718. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, N.; Wada, Y.; Ohtori, S.; Saisu, T.; Moriya, H. Application of shock waves to rat skin decreases calcitonin gene-related peptide immunoreactivity in dorsal root ganglion neurons. Auton. Neurosci. 2003, 107, 81–84. [Google Scholar] [CrossRef] [PubMed]
- Fricová, J.; Rokyta, R. The effects of extracorporeal shock wave therapy on pain patients. Neuro Endocrinol. Lett. 2015, 36, 161–164. [Google Scholar] [PubMed]
- Kirkby, K.A.; Lewis, D.D. Canine Hip Dysplasia: Reviewing the Evidence for Nonsurgical Management. Vet. Surg. 2011, 41, 2–9. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Ye, L.; Liu, H.; Yang, P.; Yang, B. Extracorporeal Shock Wave Therapy for the Treatment of Osteoarthritis: A Systematic Review and Meta-Analysis. BioMed Res. Int. 2020, 2020, 1907821. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhong, Z.; Liu, B.; Liu, G.; Chen, J.; Li, Y.; Chen, J.; Liu, X.; Hu, Y. A Randomized Controlled Trial on the Effects of Low-Dose Extracorporeal Shockwave Therapy in Patients With Knee Osteoarthritis. Arch. Phys. Med. Rehabil. 2019, 100, 1695–1702. [Google Scholar] [CrossRef] [Green Version]
- Levine, D.; Bockstahler, B. Electrical stimulation. In Canine Rehabiliation and Physical Therapy; Millis, D.L., Levine, D., Eds.; Elsevier: Amsterdam, The Netherlands, 2014; pp. 342–358. [Google Scholar]
- Bockstahler, B.; Levine, D.; Ciuperca, I. Electrotherapy. In Essential Facts of Physical Medicine, Rehabilitation and Sports Medicine in Companion Animals; Bockstahler, B., Wittek, K., Levine, D., Maierl, J., Millis, D.L., Eds.; VBS GmbH: Babenhausen, Germany, 2019. [Google Scholar]
- Zeng, C.; Li, H.; Yang, T.; Deng, Z.-H.; Yang, Y.; Zhang, Y.; Lei, G.-H. Electrical stimulation for pain relief in knee osteoarthritis: Systematic review and network meta-analysis. Osteoarthr. Cartil. 2014, 23, 189–202. [Google Scholar] [CrossRef] [Green Version]
- Livitchi, L.; Muste, A.; Beteg, F.; Scurtu, I.; Bota, A.; Briciu, R.; Donisa, A. Research and Observations on the Interferential Currents Stimulation for the Treatment of Musculoskeletal Pain in Dog. Bull. Univ. Agric. Sci. Vet. Med. Cluj-Napoca Vet. Med. 2010, 66, 218–223. [Google Scholar] [CrossRef]
- Hainaut, K.; Duchateau, J.; Hainaut, K.; Hainaut, K. Neuromuscular Electrical Stimulation and Voluntary Exercise. Sports Med. 1992, 14, 100–113. [Google Scholar] [CrossRef]
- Vaz, M.A.; Baroni, B.M.; Geremia, J.M.; Lanferdini, F.J.; Mayer, A.; Arampatzis, A.; Herzog, W. Neuromuscular electrical stimulation (NMES) reduces structural and functional losses of quadriceps muscle and improves health status in patients with knee osteoarthritis. J. Orthop. Res. 2012, 31, 511–516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruce-Brand, R.A.; Walls, R.J.; Ong, J.C.; Emerson, B.S.; O’Byrne, J.M.; Moyna, N.M. Effects of home-based resistance training and neuromuscular electrical stimulation in knee osteoarthritis: A randomized controlled trial. BMC Musculoskelet. Disord. 2012, 13, 118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burgess, L.C.; Taylor, P.; Wainwright, T.W.; Bahadori, S.; Swain, I.D. Adherence to Neuromuscular Electrical Stimulation Interventions for Muscle Impairment in Hip and Knee Osteoarthritis: A Systematic Review. Clin. Med. Insights Arthritis Musculoskelet. Disord. 2021, 14, 11795441211028746. [Google Scholar] [CrossRef] [PubMed]
- DeSantana, J.M.; da Silva, L.F.S.; Sluka, K.A. Cholecystokinin receptors mediate tolerance to the analgesic effect of TENS in arthritic rats. Pain 2010, 148, 84–93. [Google Scholar] [CrossRef] [Green Version]
- Radhakrishnan, R.; Sluka, K.A. Deep Tissue Afferents, but not Cutaneous Afferents, Mediate Transcutaneous Electrical Nerve Stimulation–Induced Antihyperalgesia. J. Pain 2005, 6, 673–680. [Google Scholar] [CrossRef]
- Sluka, K.A.; Bailey, K.; Bogush, J.; Olson, R.; Ricketts, A. Treatment with either high or low frequency TENS reduces the secondary hyperalgesia observed after injection of kaolin and carrageenan into the knee joint. Pain 1998, 77, 97–102. [Google Scholar] [CrossRef]
- Sluka, K.A.; Deacon, M.; Stibal, A.; Strissel, S.; Terpstra, A. Spinal blockade of opioid receptors prevents the analgesia produced by TENS in arthritic rats. J. Pharmacol. Exp. Ther. 1999, 289, 840–846. [Google Scholar]
- Vance, C.G.T.; Rakel, B.A.; Blodgett, N.P.; DeSantana, J.M.; Amendola, A.; Zimmerman, M.B.; Walsh, D.M.; Sluka, K.A. Effects of Transcutaneous Electrical Nerve Stimulation on Pain, Pain Sensitivity, and Function in People With Knee Osteoarthritis: A Randomized Controlled Trial. Phys. Ther. 2012, 92, 898–910. [Google Scholar] [CrossRef] [Green Version]
- Levine, D. The effect of TENS on osteoarthritic pain in the stifle of dogs. In Proceedings of the 2nd International Symposium on Rehabilitation and Physical Therapy in Veterinary Medicine, Knoxville, Tennessee, 10–14 August 2002. [Google Scholar]
- Mlacnik, E.; Bockstahler, B.A.; Müller, M.; Tetrick, M.A.; Nap, R.C.; Zentek, J. Effects of caloric restriction and a moderate or intense physiotherapy program for treatment of lameness in overweight dogs with osteoarthritis. J. Am. Vet. Med. Assoc. 2006, 229, 1756–1760. [Google Scholar] [CrossRef] [Green Version]
- Rutjes, A.W.; Nüesch, E.; Sterchi, R.; Kalichman, L.; Hendriks, E.; Osiri, M.; Brosseau, L.; Reichenbach, S.; Jüni, P. Transcutaneous electrostimulation for osteoarthritis of the knee. Cochrane Database Syst. Rev. 2009, 2009, CD002823. [Google Scholar] [CrossRef] [Green Version]
- Osiri, M.; Welch, V.; Brosseau, L.; Shea, B.; McGowan, J.L.; Tugwell, P.; Wells, G.A. Transcutaneous electrical nerve stimulation for knee osteoarthritis. Cochrane Database Syst Rev. 2000, 4, CD002823. [Google Scholar] [CrossRef]
- Jones, I.; Johnson, M.I. Transcutaneous electrical nerve stimulation. Contin. Educ. Anaesth. Crit. Care Pain 2009, 9, 130–135. [Google Scholar] [CrossRef] [Green Version]
- Hernández-Bule, M.L.; Paino, C.; Trillo, M.; Úbeda, A. Electric Stimulation at 448 kHz Promotes Proliferation of Human Mesenchymal Stem Cells. Cell. Physiol. Biochem. 2014, 34, 1741–1755. [Google Scholar] [CrossRef] [PubMed]
- Coccetta, C.A.; Sale, P.; Ferrara, P.E.; Specchia, A.; Maccauro, G.; Ferriero, G.; Ronconi, G. Effects of capacitive and resistive electric transfer therapy in patients with knee osteoarthritis: A randomized controlled trial. Int. J. Rehabil. Res. 2019, 42, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Costantino, C.; Pogliacomi, F.; Vaienti, E. Cryoultrasound therapy and tendonitis in athletes: A comparative evaluation versus laser CO2 and t.e.ca.r. therapy. Acta Biomed. 2005, 76, 37–41. [Google Scholar]
- Paolucci, T.; Pezzi, L.; Centra, M.; Porreca, A.; Barbato, C.; Bellomo, R.; Saggini, R. Effects of capacitive and resistive electric transfer therapy in patients with painful shoulder impingement syndrome: A comparative study. J. Int. Med. Res. 2020, 48, 300060519883090. [Google Scholar] [CrossRef] [Green Version]
- López-De-Celis, C.; Hidalgo-García, C.; Pérez-Bellmunt, A.; Fanlo-Mazas, P.; González-Rueda, V.; Tricás-Moreno, J.M.; Ortiz, S.; Rodríguez-Sanz, J. Thermal and non-thermal effects off capacitive-resistive electric transfer application on the Achilles tendon and musculotendinous junction of the gastrocnemius muscle: A cadaveric study. BMC Musculoskelet. Disord. 2020, 21, 46. [Google Scholar] [CrossRef]
- Tashiro, Y.; Hasegawa, S.; Yokota, Y.; Nishiguchi, S.; Fukutani, N.; Shirooka, H.; Tasaka, S.; Matsushita, T.; Matsubara, K.; Nakayama, Y.; et al. Effect of Capacitive and Resistive electric transfer on haemoglobin saturation and tissue temperature. Int. J. Hyperth. 2017, 33, 696–702. [Google Scholar] [CrossRef] [Green Version]
- Yokota, Y.; Sonoda, T.; Tashiro, Y.; Suzuki, Y.; Kajiwara, Y.; Zeidan, H.; Nakayama, Y.; Kawagoe, M.; Shimoura, K.; Tatsumi, M.; et al. Effect of Capacitive and Resistive electric transfer on changes in muscle flexibility and lumbopelvic alignment after fatiguing exercise. J. Phys. Ther. Sci. 2018, 30, 719–725. [Google Scholar] [CrossRef] [Green Version]
- Kumaran, B.; Watson, T. Treatment using 448 kHz capacitive resistive monopolar radiofrequency improves pain and function in patients with osteoarthritis of the knee joint: A randomised controlled trial. Physiotherapy 2018, 105, 98–107. [Google Scholar] [CrossRef] [Green Version]
- Rosemann, T.; Wensing, M.; Joest, K.; Backenstrass, M.; Mahler, C.; Szecsenyi, J. Problems and needs for improving primary care of osteoarthritis patients: The views of patients, general practitioners and practice nurses. BMC Musculoskelet. Disord. 2006, 7, 48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kloek, C.J.J.; Van Dongen, J.M.; De Bakker, D.H.; Bossen, D.; Dekker, J.; Veenhof, C. Cost-effectiveness of a blended physiotherapy intervention compared to usual physiotherapy in patients with hip and/or knee osteoarthritis: A cluster randomized controlled trial. BMC Public Health 2018, 18, 1082. [Google Scholar] [CrossRef] [PubMed]
- Oke, S.L.; McIlwraith, C.W.; Moyer, W. Review of the economic impact of osteoarthritis and oral joint-health supplements in horses. In Proceedings of the 56th Annual Convention of the American Association of Equine Practitioners, Baltimore, MD, USA, 4–8 December 2010. [Google Scholar]



{kind=link}
{kind=link}
| Study | Mode | Wavelength | Intensity | Frequency | Treatment Duration |
|---|---|---|---|---|---|
| Looney et al. [42] | continuous | 650 nm and 980 nm | 10–20 J/cm2 | 2/week | 6 weeks |
| Barale et al. [41] | continuous and pulsed | 808 nm | 5 J/cm2 (affected joint) 4.2 J/cm2 (associated skeletal muscle) | 1/week | 6 weeks |
| Authors | Dogs Number | OA | ESWT Therapy Technical Details | Clinical Follow-Up | Effect |
|---|---|---|---|---|---|
| Dahlberg et al. (2005) [2,37] | ESWT = 7 Control = 5 | Stifle | 800 pulses, focal pressure depth: 20 mm; 700 pulses: focal depth: 5 mm 4 Hz, energy flux density: 0.14 mJ/mm2, 3 times every 3 weeks | 98 days | No significant improvement for PVF, VI and owner questionnaires |
| Mueller et al. (2007) [39] | ESWT = 18 Control = 6 | Hip | Radial, 2000 pulses, 15 Hz, 2 bars, 3 times every 7 days | 6 months | Improved PVF, VI |
| Millis et al. (2011) [38] | ESWT = 8 Control = 7 | Elbow | Focused, 500 pulses, 5 mm probe, energy flux density: 0.13 mJ/mm2, twice every 2 weeks | 28 days | Improved PVF, lameness scores |
| Souza et al. [40] | ESWT = 30 Control = 30 | Hip | Radial, 2000 pulses, 10 Hz, 2–3.4 bars, 3 times every 7 days | 3 months | Improved PVF and VI, VAS and activity |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mille, M.A.; McClement, J.; Lauer, S. Physiotherapeutic Strategies and Their Current Evidence for Canine Osteoarthritis. Vet. Sci. 2023, 10, 2. https://doi.org/10.3390/vetsci10010002
Mille MA, McClement J, Lauer S. Physiotherapeutic Strategies and Their Current Evidence for Canine Osteoarthritis. Veterinary Sciences. 2023; 10(1):2. https://doi.org/10.3390/vetsci10010002
Chicago/Turabian StyleMille, Monika Anna, Jamie McClement, and Susanne Lauer. 2023. "Physiotherapeutic Strategies and Their Current Evidence for Canine Osteoarthritis" Veterinary Sciences 10, no. 1: 2. https://doi.org/10.3390/vetsci10010002