
In Vitro Major Arterial Cardiovascular Simulator to Generate Benchmark Data Sets for In Silico Model Validation

Abstract
:1. Introduction
2. Materials and Methods
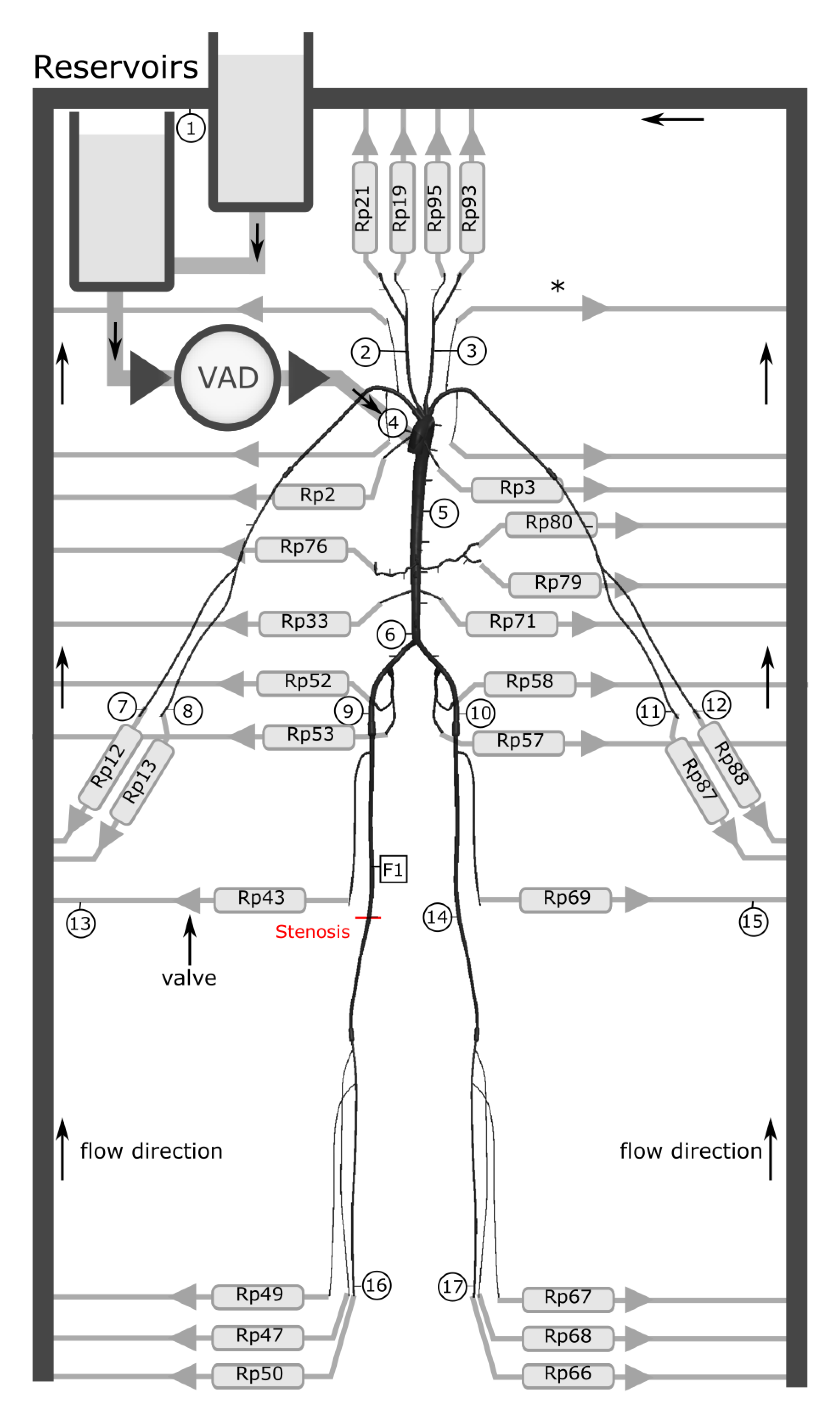
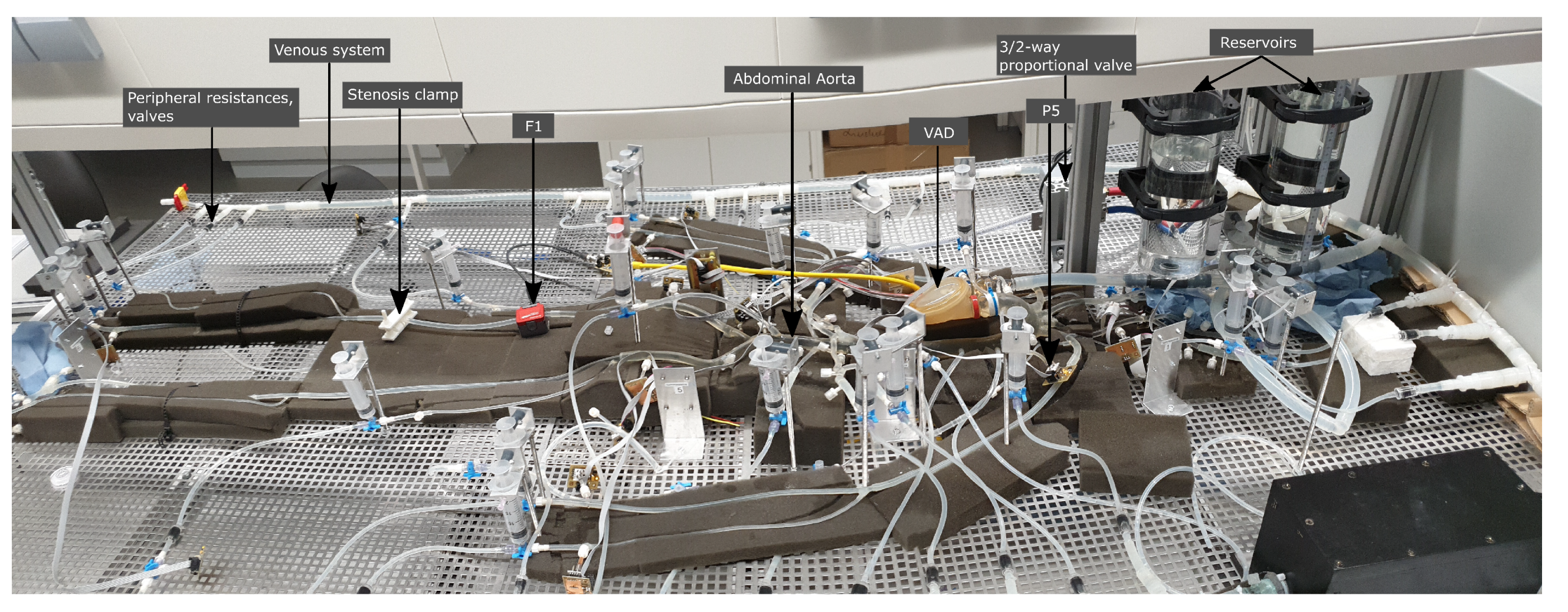
2.1. Cardiovascular Simulator
- 1.
- Minimisation of the pulse wave reflection with the condition of obtaining realistic wave reflections from peripheral bifurcations and pathologies.
- 2
- Adjustable flow conditions to a wide range of physiological conditions, such as heart rate, systolic pressure, compliance, and peripheral resistances.
- 3
- Measurement of pressure and flow at several locations within the cardiovascular simulator.
- 4
- Improved laboratory conditions for a highly reproducible pressure and flow measurement on a sample.
- 5
- Parametric scripting of ventricular boundary conditions.
- 6
- Persistent data management in a relational database for post-processing.
2.1.1. Arterial and Venous System
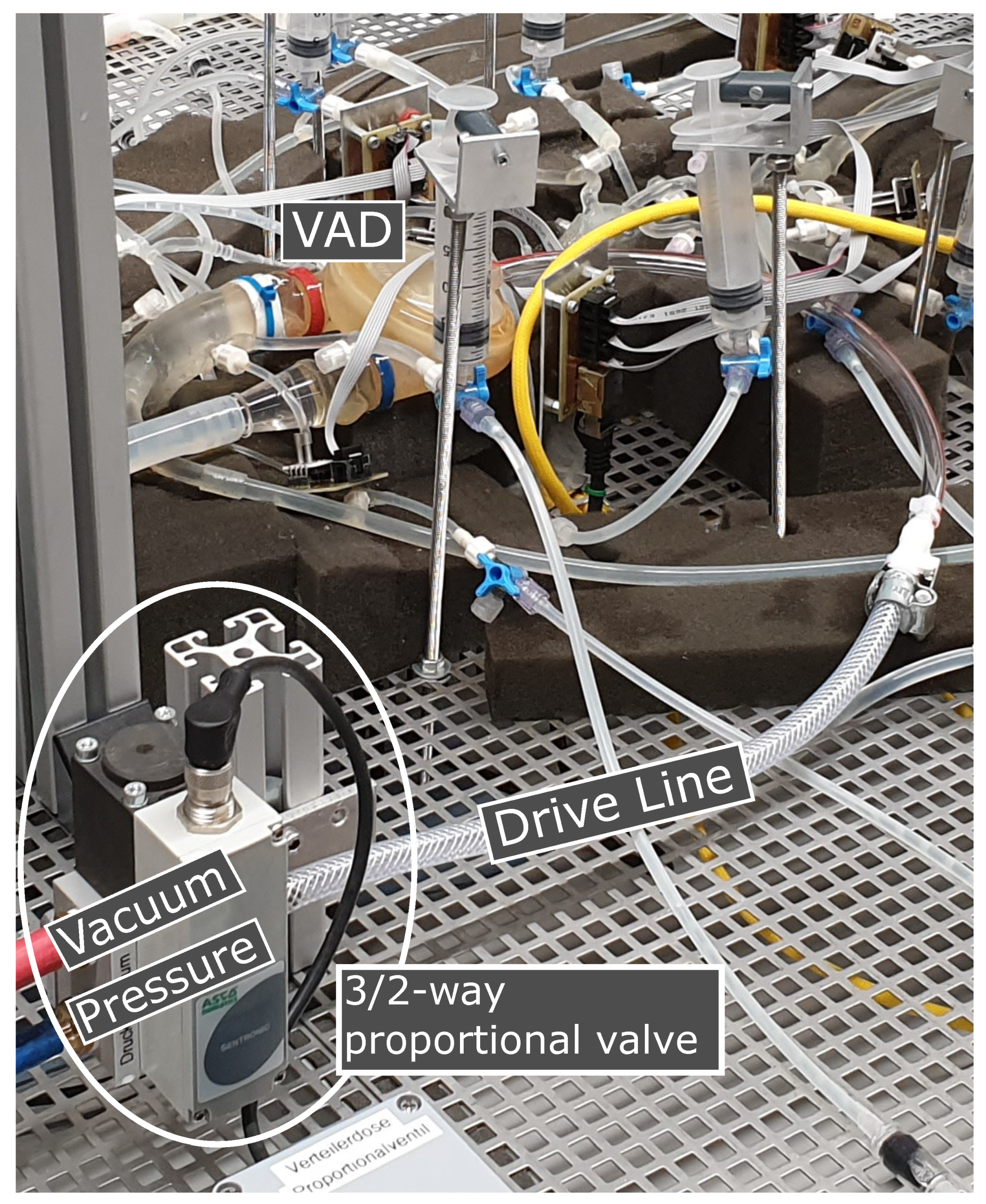
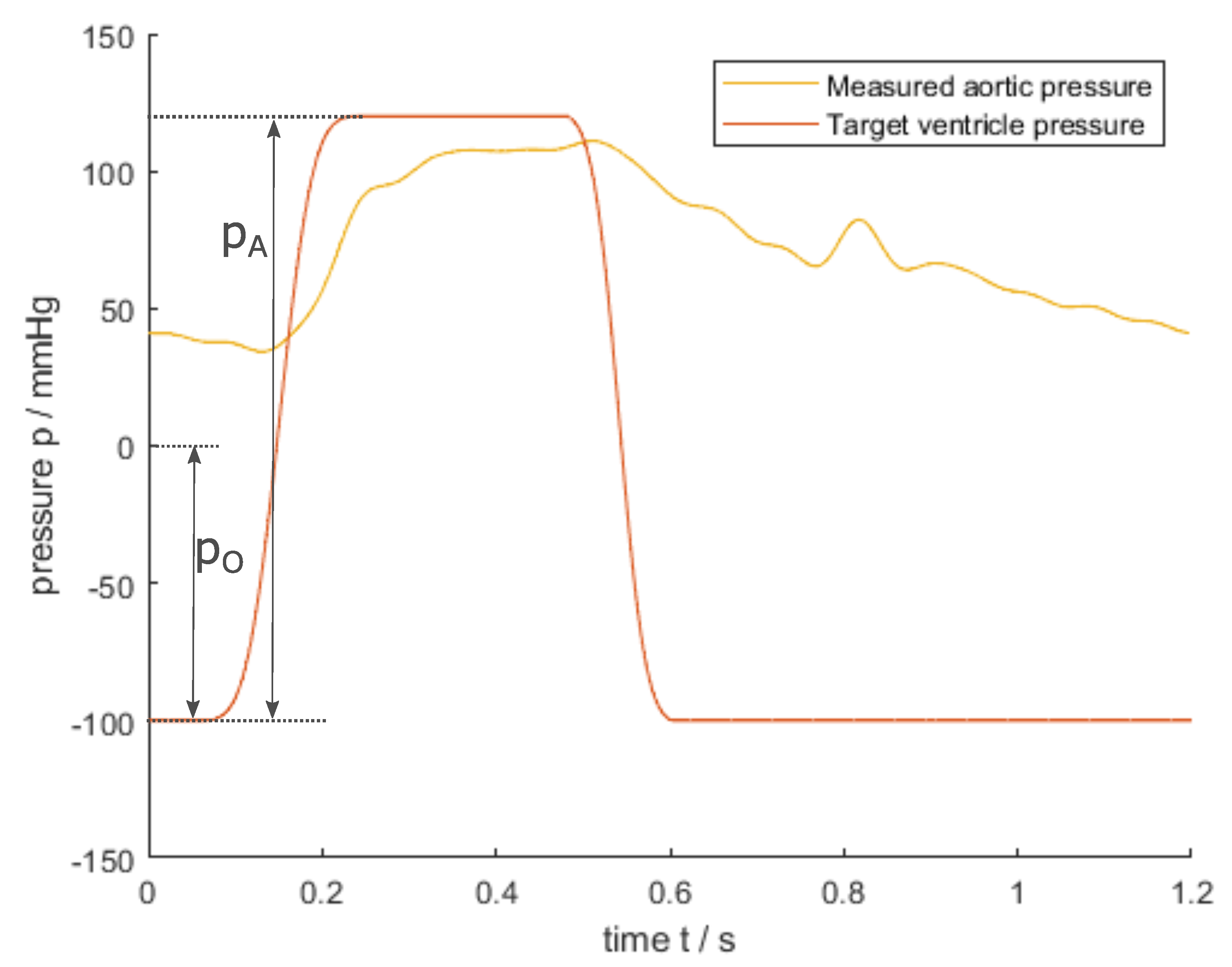
2.1.2. Heart Pump
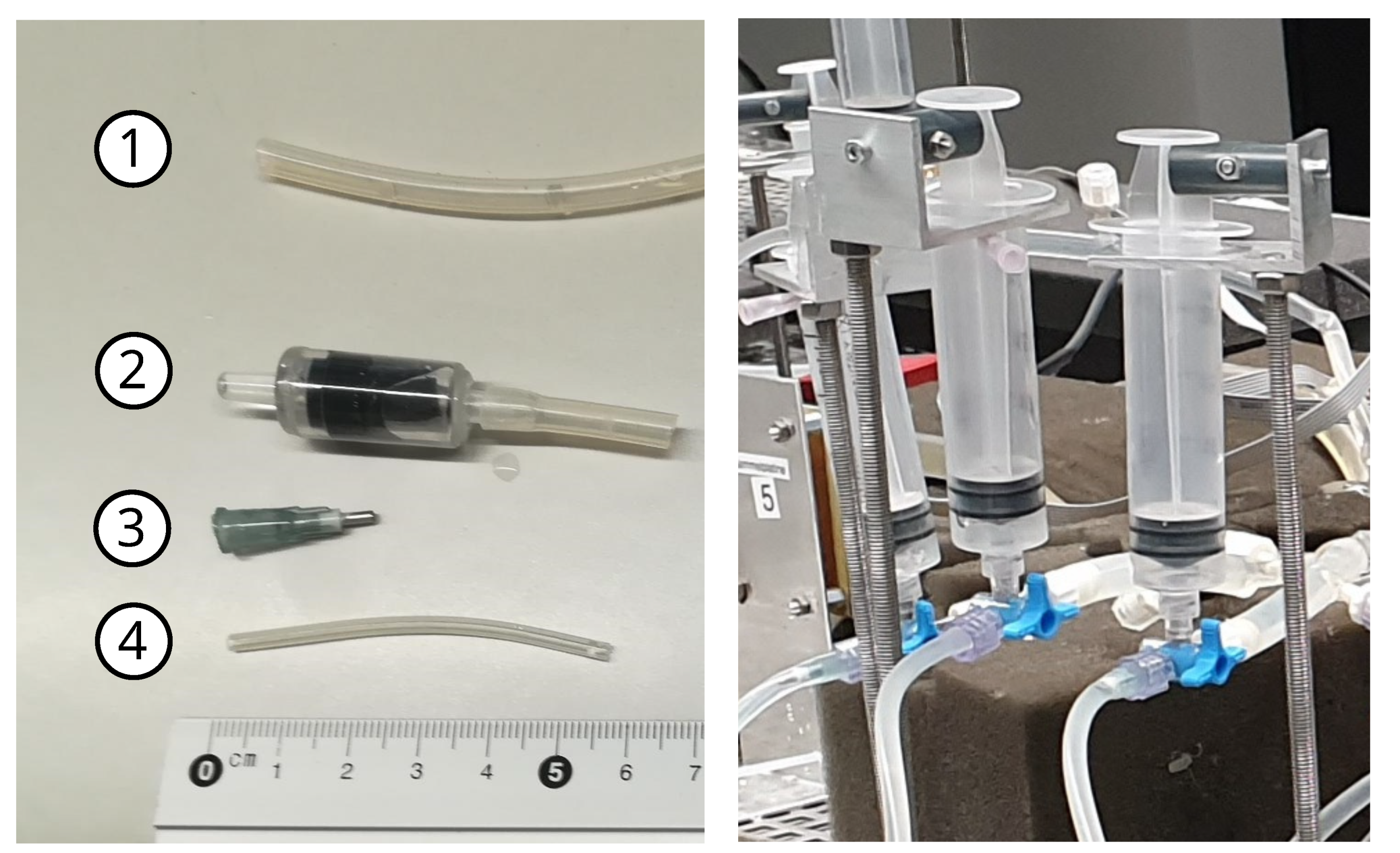
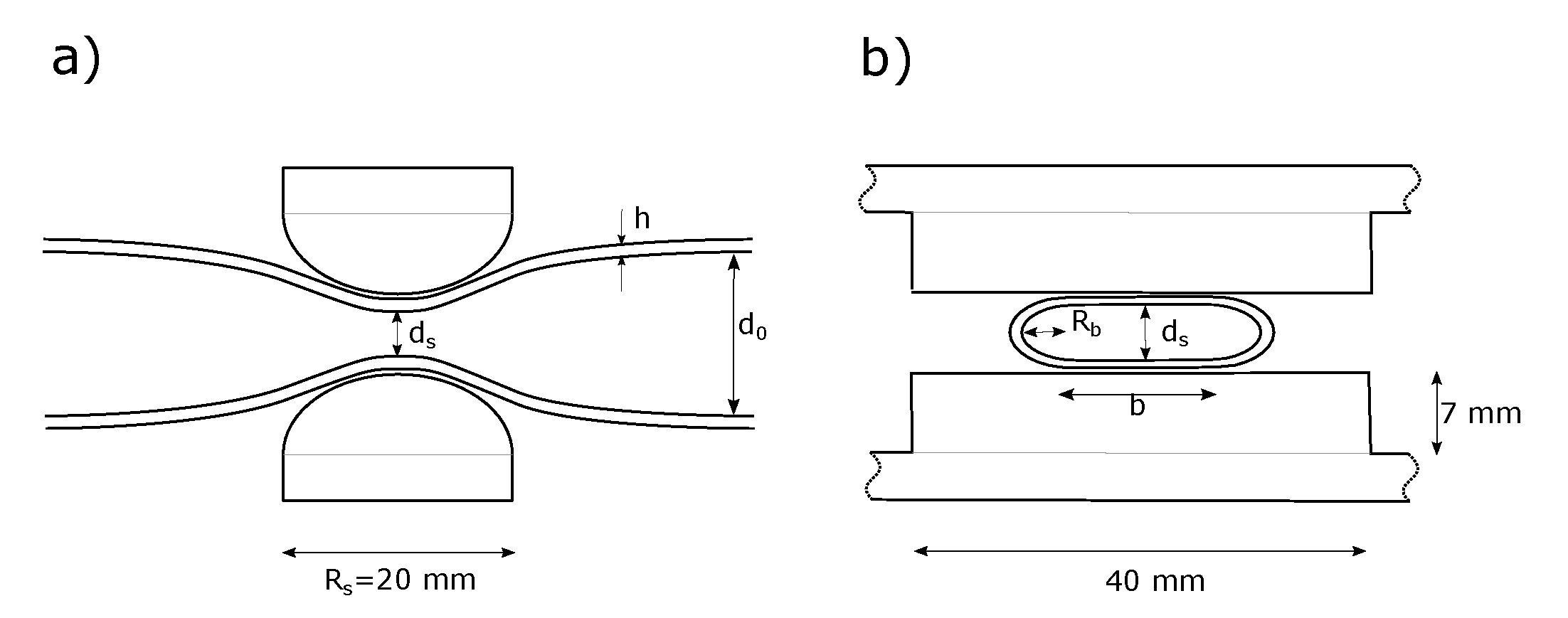
2.1.3. Peripheral Resistance and Compliance
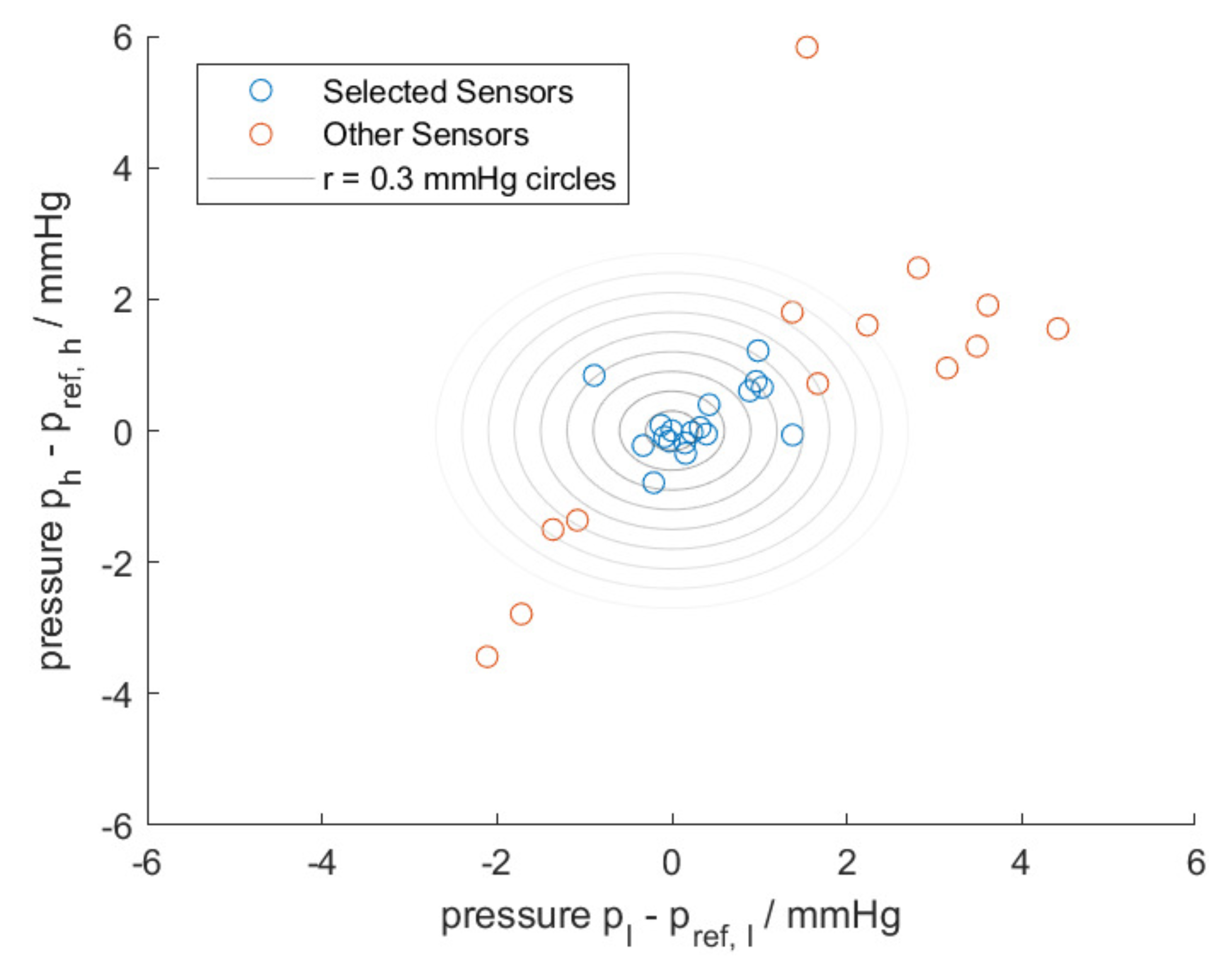
2.1.4. Pressure and Flow Sensors
2.2. Measurement Setup and Procedure
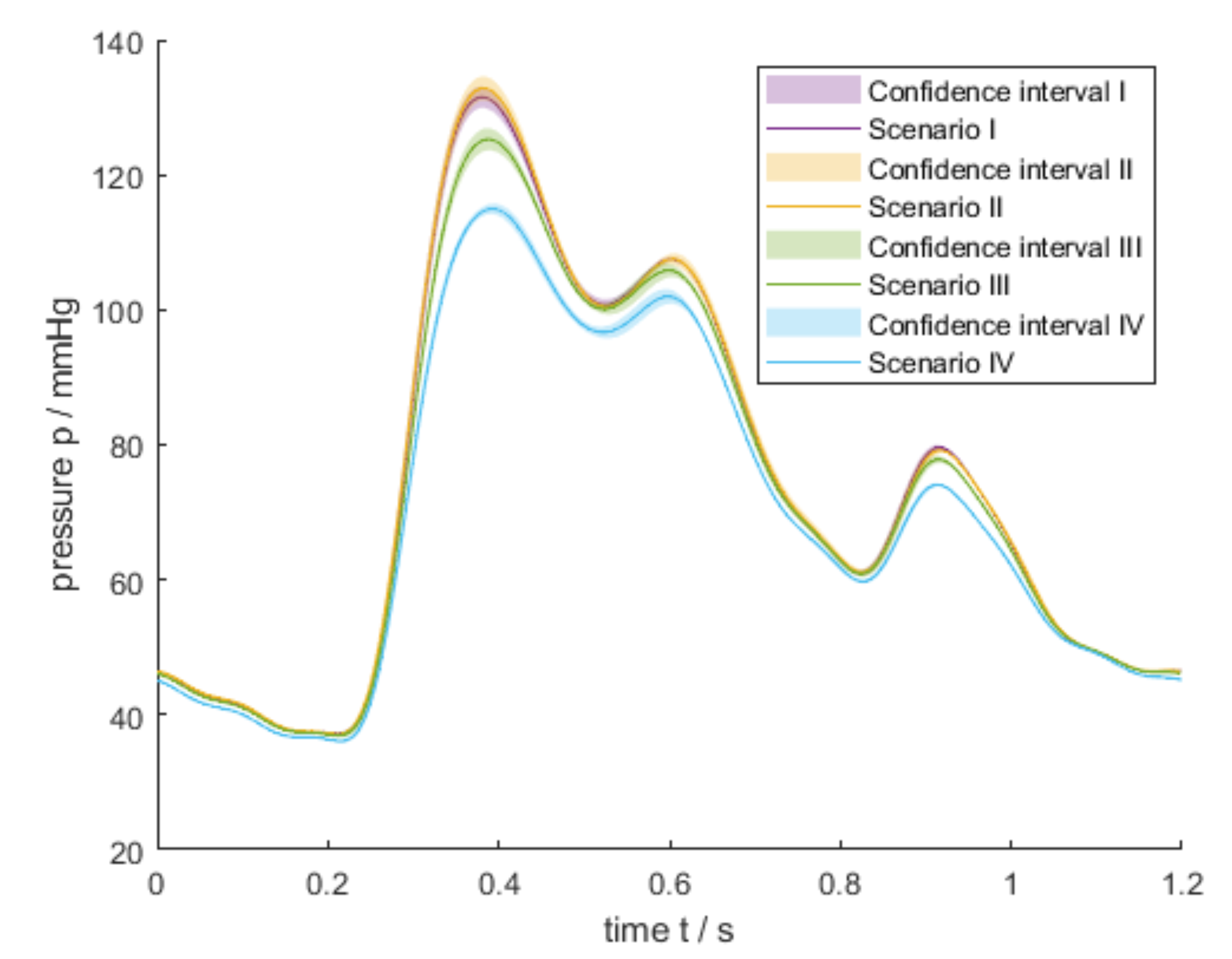
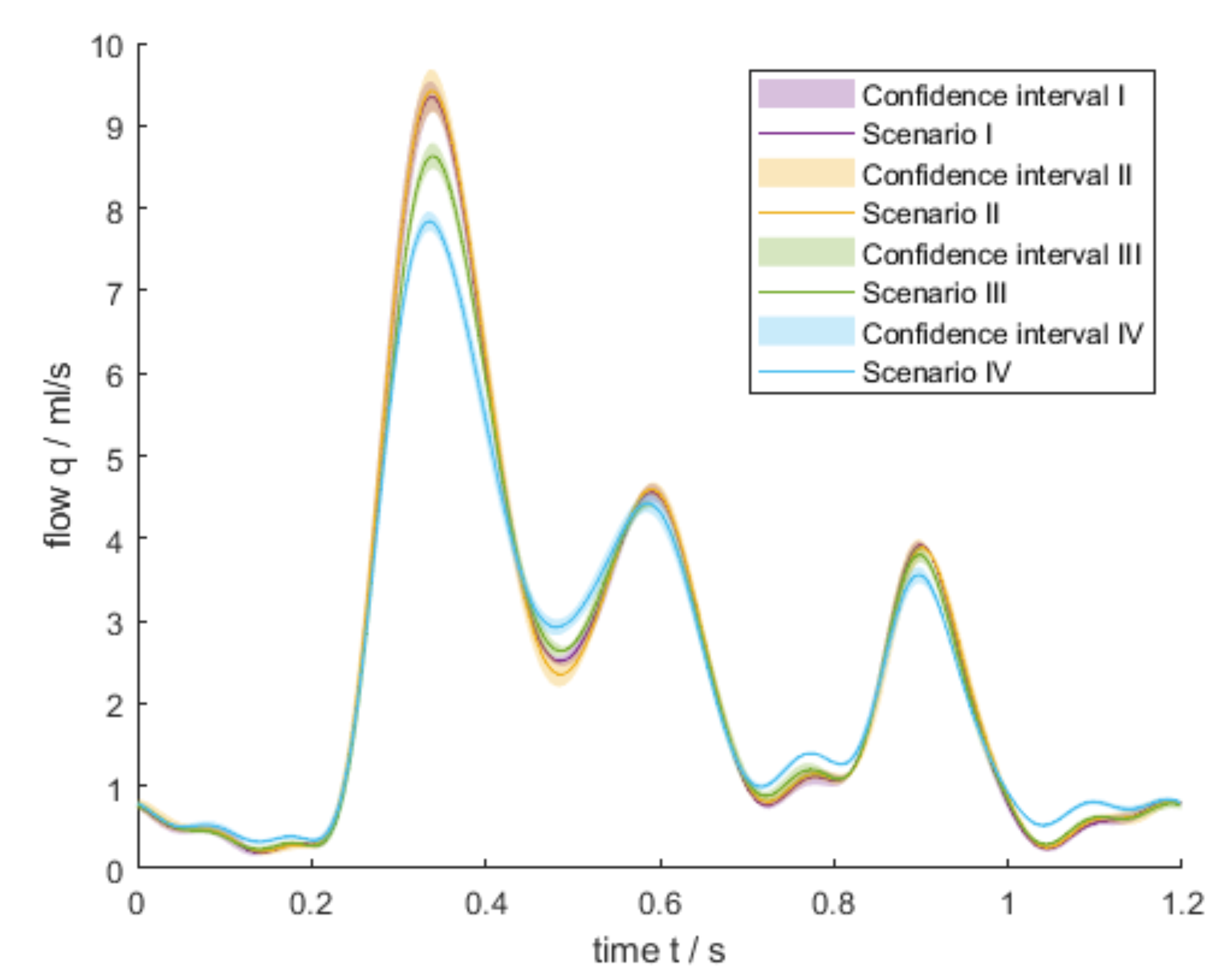
2.3. Measurement Scenarios
3. Results
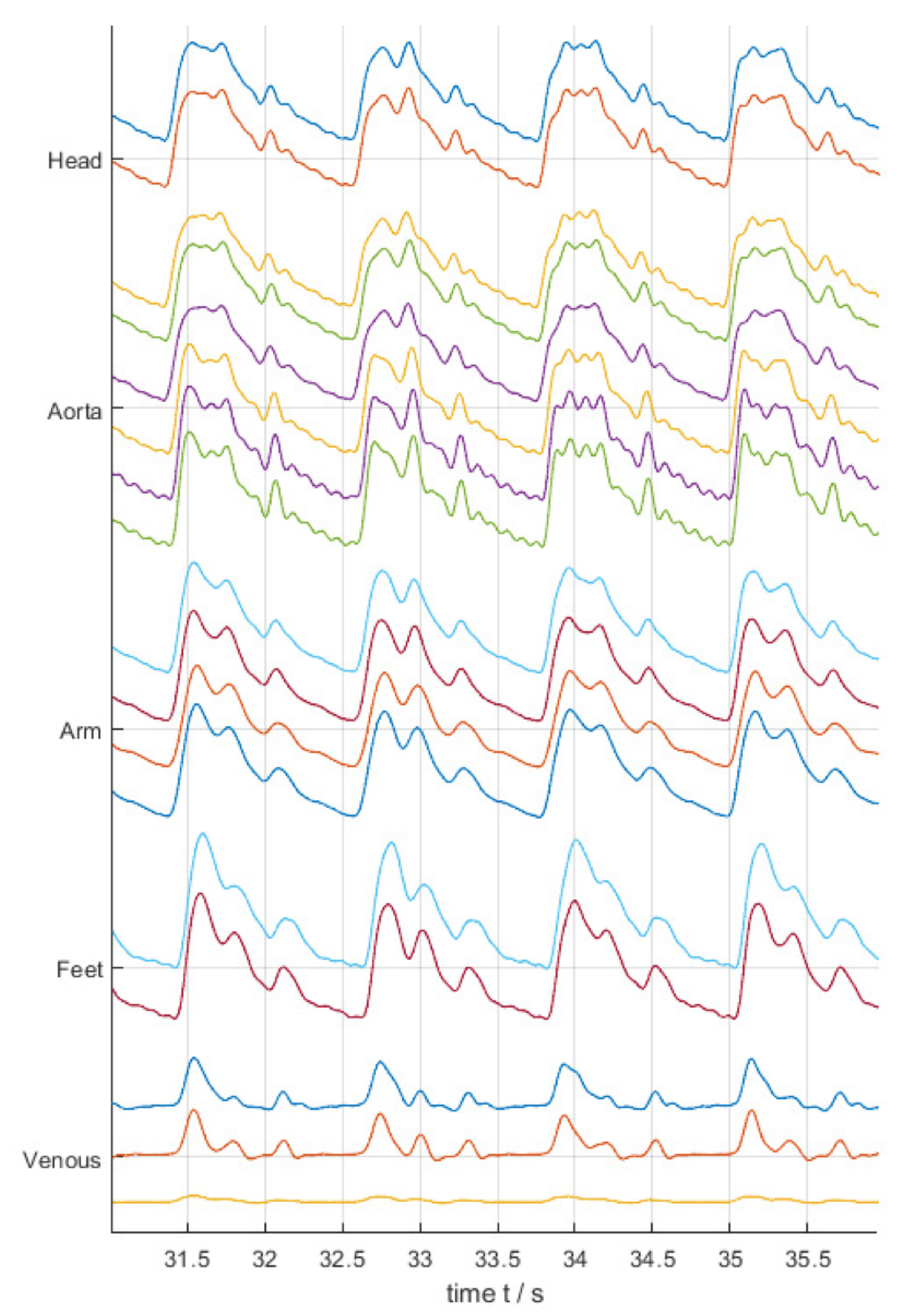
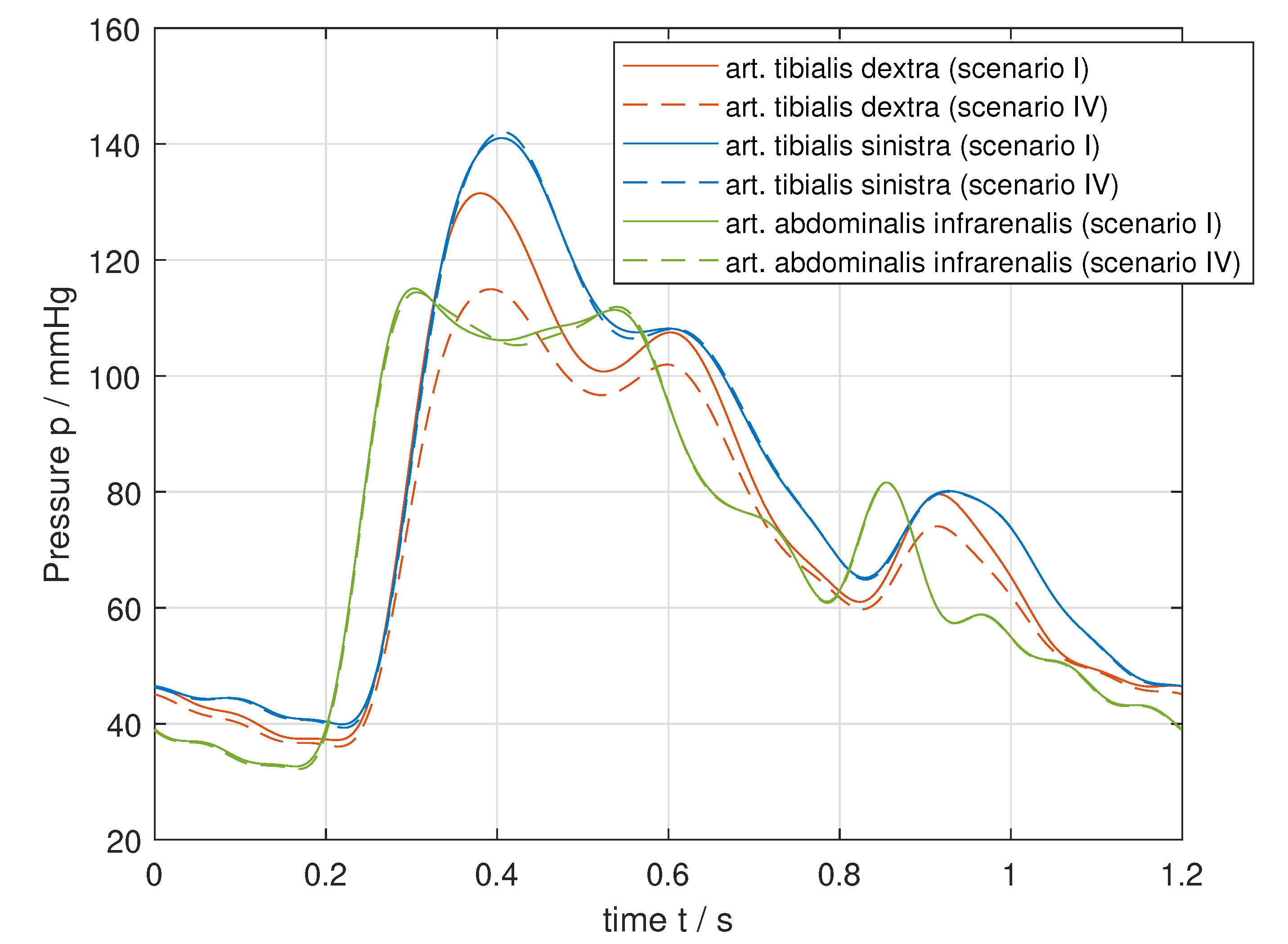
3.1. Pressure Waves along the Arterial Network
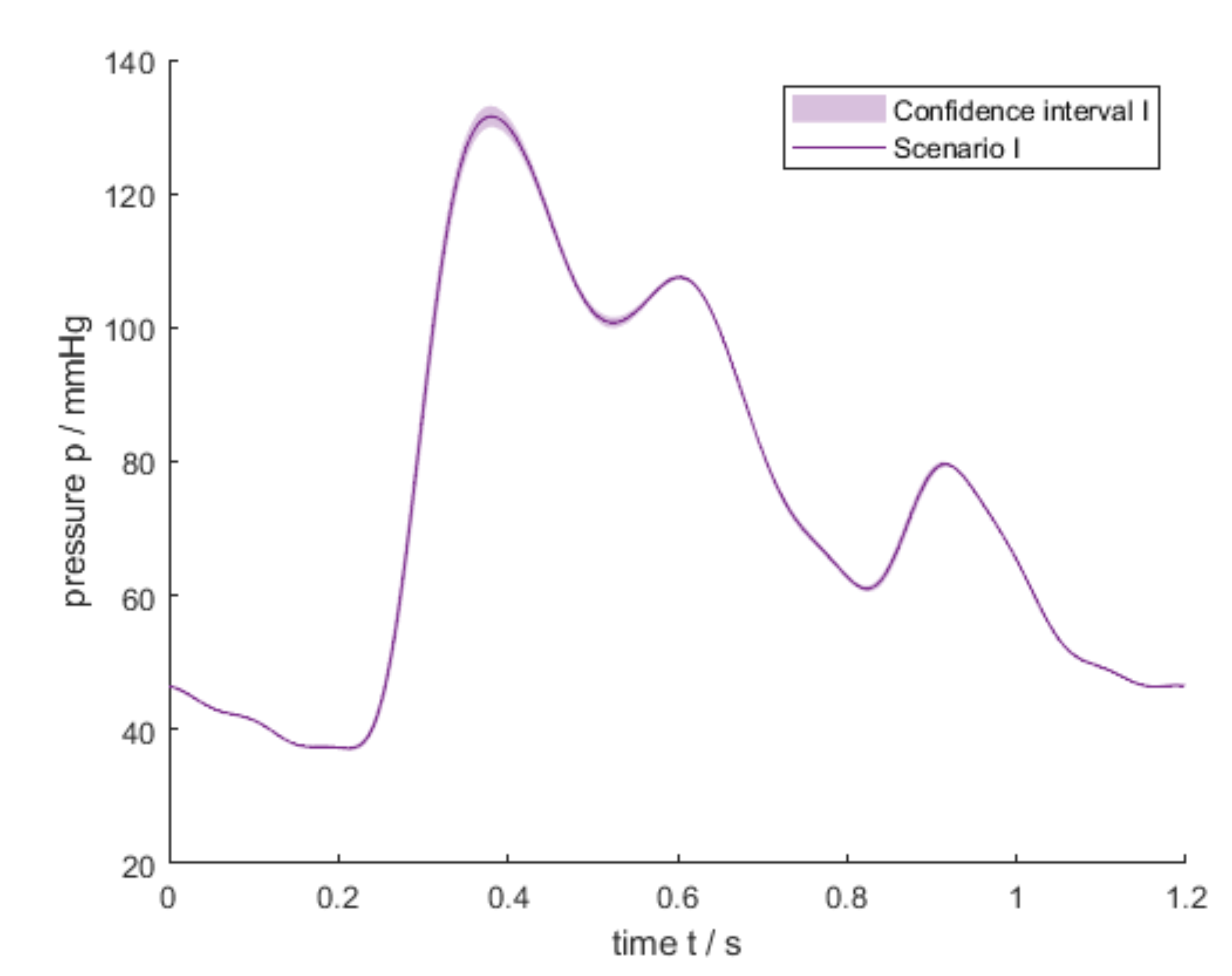
3.2. Scenario I—Healthy Conditions
3.3. Scenarios II–VI—Pathological Conditions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
Appendix A.1. Calibration Measurements
Appendix A.2. Calibration of Pressure Sensors
Appendix A.3. Calibration Flow Sensor
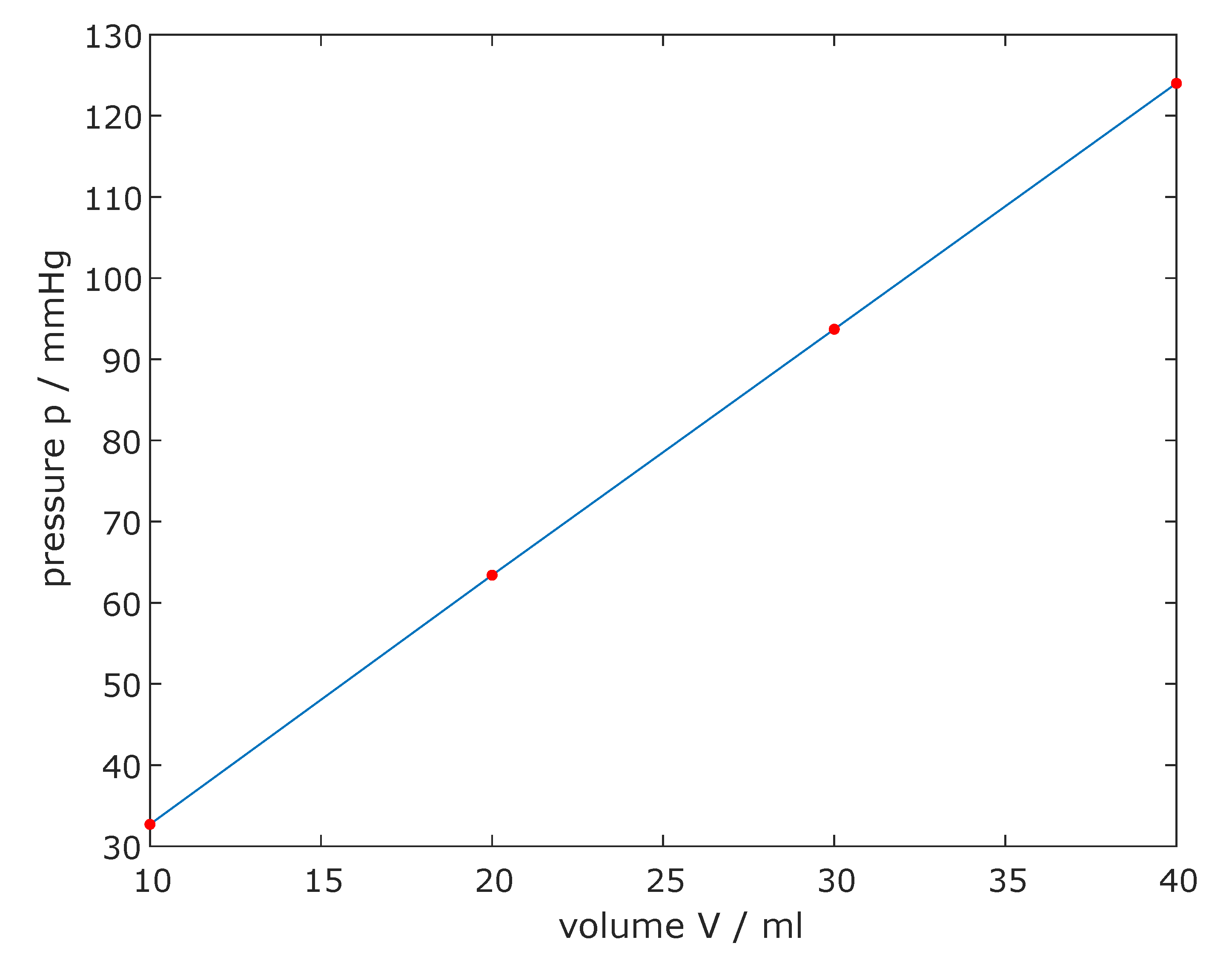
Appendix A.4. Compliance


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | (mmHg) | (mL) | C (mL/mmHg) |
|---|---|---|---|
| 1 | 32.7 | 10 | 0.3058 |
| 2 | 30.7 | 10 | 0.3257 |
| 3 | 30.3 | 10 | 0.3300 |
| 4 | 30.3 | 10 | 0.3300 |
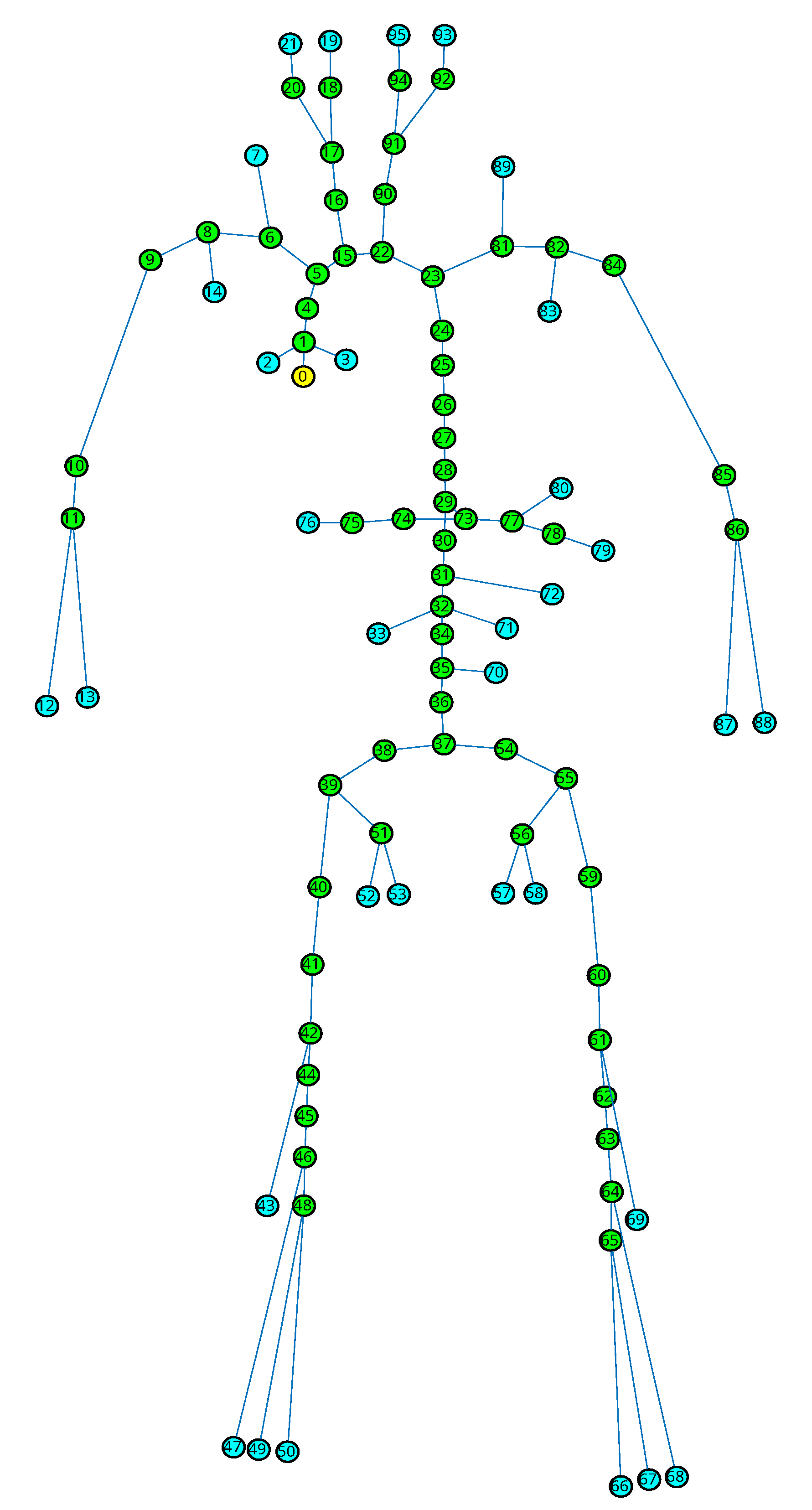
Appendix A.5. SISCA Model
Appendix A.6. Overview of the Structural Properties of the MACSim

| Node ID | L (m) | h (m) | d (m) | E (Pa) |
|---|---|---|---|---|
| 1 | 0.02 | 0.0015 | 0.025 | 6,700,000 |
| 2 | 0.067 | 0.0005 | 0.004 | 1,650,000 |
| 3 | 0.08 | 0.0005 | 0.004 | 1,650,000 |
| 4 | 0.01 | 0.0015 | 0.025 | 6,700,000 |
| 5 | 0.052 | 0.0015 | 0.025 | 6,700,000 |
| 6 | 0.049 | 0.001 | 0.01 | 6,700,000 |
| 7 | 0.14 | 0.0005 | 0.0015 | 1,650,000 |
| 8 | 0.016 | 0.001 | 0.01 | 6,700,000 |
| 9 | 0.053 | 0.001 | 0.01 | 6,700,000 |
| 10 | 0.35 | 0.001 | 0.006 | 1,650,000 |
| 11 | 0.021 | 0.001 | 0.004 | 1,650,000 |
| 12 | 0.325 | 0.001 | 0.004 | 1,650,000 |
| 13 | 0.345 | 0.0005 | 0.003 | 1,650,000 |
| 14 | 0.095 | 0.0004 | 0.0015 | 1,650,000 |
| 15 | 0.013 | 0.0015 | 0.025 | 6,700,000 |
| 16 | 0.11 | 0.0005 | 0.0065 | 6,700,000 |
| 17 | 0.045 | 0.0005 | 0.0065 | 6,700,000 |
| 18 | 0.054 | 0.0005 | 0.004 | 6,700,000 |
| 19 | 0.036 | 0.0005 | 0.004 | 6,700,000 |
| 20 | 0.06 | 0.0005 | 0.006 | 6,700,000 |
| 21 | 0.029 | 0.0005 | 0.006 | 6,700,000 |
| 22 | 0.012 | 0.0015 | 0.028 | 6,700,000 |
| 23 | 0.01 | 0.0015 | 0.028 | 6,700,000 |
| 24 | 0.002 | 0.0015 | 0.028 | 6,700,000 |
| 25 | 0.05 | 0.0015 | 0.025 | 6,700,000 |
| 26 | 0.05 | 0.0015 | 0.021 | 6,700,000 |
| 27 | 0.05 | 0.0015 | 0.02 | 6,700,000 |
| 28 | 0.049 | 0.0015 | 0.019 | 6,700,000 |
| 29 | 0.027 | 0.0015 | 0.019 | 6,700,000 |
| 30 | 0.02 | 0.0015 | 0.018 | 6,700,000 |
| 31 | 0.006 | 0.0015 | 0.017 | 6,700,000 |
| 32 | 0.028 | 0.0015 | 0.016 | 6,700,000 |
| 33 | 0.08 | 0.0005 | 0.004 | 1,650,000 |
| 34 | 0.021 | 0.0015 | 0.016 | 6,700,000 |
| 35 | 0.031 | 0.0015 | 0.015 | 6,700,000 |
| 36 | 0.018 | 0.0015 | 0.015 | 6,700,000 |
| 37 | 0.015 | 0.0015 | 0.014 | 6,700,000 |
| 38 | 0.041 | 0.0001 | 0.01 | 6,700,000 |
| 39 | 0.02 | 0.0001 | 0.01 | 6,700,000 |
| 40 | 0.094 | 0.0001 | 0.01 | 6,700,000 |
| 41 | 0.015 | 0.0001 | 0.01 | 6,700,000 |
| 42 | 0.039 | 0.0001 | 0.008 | 1,650,000 |
| 43 | 0.28 | 0.0005 | 0.003 | 1,650,000 |
| 44 | 0.13 | 0.0005 | 0.008 | 1,650,000 |
| 45 | 0.34 | 0.0005 | 0.006 | 1,650,000 |
| 46 | 0.035 | 0.001 | 0.004 | 1,650,000 |
| 47 | 0.425 | 0.0005 | 0.002 | 1,650,000 |
| 48 | 0.049 | 0.001 | 0.004 | 1,650,000 |
| 49 | 0.375 | 0.0005 | 0.002 | 1,650,000 |
| 50 | 0.36 | 0.001 | 0.004 | 1,650,000 |
| 51 | 0.073 | 0.0005 | 0.006 | 6,700,000 |
| 52 | 0.055 | 0.0005 | 0.006 | 6,700,000 |
| 53 | 0.063 | 0.0005 | 0.006 | 6,700,000 |
| 54 | 0.041 | 0.0001 | 0.01 | 6,700,000 |
| 55 | 0.02 | 0.0001 | 0.01 | 6,700,000 |
| 56 | 0.073 | 0.0005 | 0.006 | 6,700,000 |
| 57 | 0.063 | 0.0005 | 0.006 | 6,700,000 |
| 58 | 0.055 | 0.0005 | 0.006 | 6,700,000 |
| 59 | 0.094 | 0.0001 | 0.01 | 6,700,000 |
| 60 | 0.015 | 0.0001 | 0.01 | 6,700,000 |
| 61 | 0.039 | 0.0001 | 0.008 | 1,650,000 |
| 62 | 0.13 | 0.0005 | 0.008 | 1,650,000 |
| 63 | 0.34 | 0.0005 | 0.006 | 4,000,000 |
| 64 | 0.035 | 0.001 | 0.004 | 1,650,000 |
| 65 | 0.049 | 0.001 | 0.004 | 1,650,000 |
| 66 | 0.36 | 0.001 | 0.004 | 1,650,000 |
| 67 | 0.375 | 0.0005 | 0.002 | 1,650,000 |
| 68 | 0.425 | 0.0005 | 0.002 | 1,650,000 |
| 69 | 0.28 | 0.0005 | 0.003 | 1,650,000 |
| 70 | 0.0167 | 0.0005 | 0.005 | 1,650,000 |
| 71 | 0.008 | 0.0005 | 0.004 | 1,650,000 |
| 72 | 0.0175 | 0.0005 | 0.005 | 1,650,000 |
| 73 | 0.025 | 0.001 | 0.005 | 6,700,000 |
| 74 | 0.027 | 0.001 | 0.005 | 6,700,000 |
| 75 | 0.025 | 0.001 | 0.005 | 6,700,000 |
| 76 | 0.047 | 0.001 | 0.005 | 6,700,000 |
| 77 | 0.054 | 0.001 | 0.005 | 6,700,000 |
| 78 | 0.01 | 0.001 | 0.005 | 6,700,000 |
| 79 | 0.034 | 0.001 | 0.005 | 6,700,000 |
| 80 | 0.038 | 0.001 | 0.005 | 6,700,000 |
| 81 | 0.049 | 0.001 | 0.01 | 6,700,000 |
| 82 | 0.016 | 0.001 | 0.01 | 6,700,000 |
| 83 | 0.095 | 0.0004 | 0.0015 | 1,650,000 |
| 84 | 0.053 | 0.001 | 0.01 | 6,700,000 |
| 85 | 0.35 | 0.001 | 0.006 | 1,650,000 |
| 86 | 0.021 | 0.001 | 0.004 | 1,650,000 |
| 87 | 0.345 | 0.0005 | 0.003 | 1,650,000 |
| 88 | 0.325 | 0.001 | 0.004 | 1,650,000 |
| 89 | 0.14 | 0.0005 | 0.0015 | 1,650,000 |
| 90 | 0.11 | 0.0005 | 0.0065 | 6,700,000 |
| 91 | 0.045 | 0.0005 | 0.0065 | 6,700,000 |
| 92 | 0.06 | 0.0005 | 0.006 | 6,700,000 |
| 93 | 0.029 | 0.0005 | 0.006 | 6,700,000 |
| 94 | 0.054 | 0.0005 | 0.004 | 6,700,000 |
| 95 | 0.036 | 0.0005 | 0.004 | 6,700,000 |

Appendix A.7. Peripheral Resistance Measurement
| Node ID | (mm) |
|---|---|
| 2 | 19.8 |
| 3 | 19.4 |
| 12 | 7 |
| 13 | 8.3 |
| 19 | 2.4 |
| 21 | 2.7 |
| 33 | 19.5 |
| 43 | 13 |
| 47 | 8.3 |
| 49 | 17.6 |
| 50 | 17.2 |
| 52 | 19.4 |
| 53 | 19.4 |
| 57 | 19.4 |
| 58 | 19.5 |
| 66 | 17.6 |
| 67 | 17.2 |
| 68 | 4.7 |
| 69 | 13.3 |
| 70 | 8.3 |
| 71 | 19.4 |
| 72 | 8.2 |
| 76 | 8.4 |
| 79 | 5.4 |
| 80 | 8.4 |
| 87 | 8.9 |
| 88 | 7 |
| 93 | 2.3 |
| 95 | 2.1 |
| 7 | / |
| 89 | / |
| 14 | / |
| 83 | / |
References
- Fowkes, F.G.R.; Rudan, D.; Rudan, I.; Aboyans, V.; Denenberg, J.O.; McDermott, M.M.; Norman, P.E.; Sampson, U.K.A.; Williams, L.J.; Mensah, G.A.; et al. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: A systematic review and analysis. Lancet 2013, 382, 1329–1340. [Google Scholar] [CrossRef]
- Mathiesen, E.B.; Joakimsen, O.; Bønaa, K.H. Prevalence of and risk factors associated with carotid artery stenosis: The Tromsø Study. Cerebrovasc. Dis. 2001, 12, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Quick, C.M.; Young, W.L.; Noordergraaf, A. Infinite number of solutions to the hemodynamic inverse problem. Am. J. Physiol.-Heart Circ. Physiol. 2001, 280, H1472–H1479. [Google Scholar] [CrossRef]
- Huttary, R.; Goubergrits, L.; Schütte, C.; Bernhard, S. Simulation, identification and statistical variation in cardiovascular analysis (SISCA)—A software framework for multi-compartment lumped modeling. Comput. Biol. Med. 2017, 87, 104–123. [Google Scholar] [CrossRef] [PubMed]
- Gul, R.; Bernhard, S. Parametric uncertainty and global sensitivity analysis in a model of the carotid bifurcation: Identification and ranking of most sensitive model parameters. Math. Biosci. 2015, 269, 104–116. [Google Scholar] [CrossRef] [PubMed]
- Quarteroni, A.; Veneziani, A.; Vergara, C. Geometric multiscale modeling of the cardiovascular system, between theory and practice. Comput. Methods Appl. Mech. Eng. 2016, 302, 193–252. [Google Scholar] [CrossRef] [Green Version]
- Quarteroni, A.; Ragni, S.; Veneziani, A. Coupling between lumped and distributed models for blood flow problems. Comput. Vis. Sci. 2001, 4, 111–124. [Google Scholar] [CrossRef]
- Zenker, S.; Rubin, J.; Clermont, G. From inverse problems in mathematical physiology to quantitative differential diagnoses. PLoS Comput. Biol. 2007, 3, e204. [Google Scholar] [CrossRef] [Green Version]
- Garber, L.; Khodaei, S.; Keshavarz-Motamed, Z. The Critical Role of Lumped Parameter Models in Patient-Specific Cardiovascular Simulations. Arch. Comput. Methods Eng. 2021, 29, 2977–3000. [Google Scholar] [CrossRef]
- Ježek, F.; Kulhánek, T.; Kalecký, K.; Kofránek, J. Lumped models of the cardiovascular system of various complexity. Biocybern. Biomed. Eng. 2017, 37, 666–678. [Google Scholar] [CrossRef]
- Jones, G.; Parr, J.; Nithiarasu, P.; Pant, S. A physiologically realistic virtual patient database for the study of arterial haemodynamics. Int. J. Numer. Methods Biomed. Eng. 2021, e3497. [Google Scholar] [CrossRef] [PubMed]
- Boileau, E.; Nithiarasu, P.; Blanco, P.J.; Müller, L.O.; Fossan, F.E.; Hellevik, L.R.; Donders, W.P.; Huberts, W.; Willemet, M.; Alastruey, J. A benchmark study of numerical schemes for one-dimensional arterial blood flow modelling. Int. J. Numer. Methods Biomed. Eng. 2015, 31, e02732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vignon-Clementel, I.E.; Chapelle, D.; Barakat, A.I.; Bel-Brunon, A.; Moireau, P.; Vibert, E. Special Issue of the VPH2020 Conference:Virtual Physiological Human: When Models, Methods and Experiments Meet the Clinic. Ann. Biomed. Eng. 2022, 50, 483–484. [Google Scholar] [CrossRef]
- Jin, W.; Alastruey, J. Arterial pulse wave propagation across stenoses and aneurysms: Assessment of one-dimensional simulations against three-dimensional simulations and in vitro measurements. J. R. Soc. Interface 2021, 18, 20200881. [Google Scholar] [CrossRef] [PubMed]
- Korzeniowski, P.; White, R.J.; Bello, F. VCSim3: A VR simulator for cardiovascular interventions. Int. J. Comput. Assist. Radiol. Surg. 2018, 13, 135–149. [Google Scholar] [CrossRef] [Green Version]
- Gehron, J.; Zirbes, J.; Bongert, M.; Schäfer, S.; Fiebich, M.; Krombach, G.; Böning, A.; Grieshaber, P. Development and Validation of a Life-Sized Mock Circulatory Loop of the Human Circulation for Fluid-Mechanical Studies. ASAIO J. 2019, 65, 788–797. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, G.; de Lazzari, C.; Kozarski, M.; Clemente, F.; Górczynska, K.; Mimmo, R.; Monnanni, E.; Tosti, G.; Guaragno, M. A Hybrid Mock Circulatory System: Testing a Prototype Under Physiologic and Pathological Conditions. ASAIO J. 2002, 48, 487. [Google Scholar] [CrossRef] [PubMed]
- Pugovkin, A.A.; Selishchev, S.V.; Telyshev, D.V. Simulator for Modeling the Cardiovascular System for Testing Circulatory Assist Devices. Biomed. Eng. 2015, 49, 213–216. [Google Scholar] [CrossRef]
- Pugovkin, A.A.; Telyshev, D.V. Automated pediatric cardiovascular simulator for left ventricular assist device evaluation. In Proceedings of the 2017 International Siberian Conference on Control and Communications (SIBCON), Astana, Kazakhstan, 29–30 June 2017; pp. 1–4. [Google Scholar] [CrossRef]
- Bernhard, S.; Wisotzki, M.; Schlett, P.; Lindner, B.; Mair, A.; Oberhardt, M. In-vitro Major Arterial Cardiovascular Simulator: Benchmark Data Set for in-silico Model Validation. arXiv 2022, arXiv:2204.10005. [Google Scholar]
- Thuaudet, S. The Medos ventricular assist device system. Perfusion 2000, 15, 337–343. [Google Scholar] [CrossRef]
- Bernhard, S.; Möhlenkamp, S.; Tilgner, A. Transient integral boundary layer method to calculate the translesional pressure drop and the fractional flow reserve in myocardial bridges. Biomed. Eng. Online 2006, 5, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Rourke, M.F.; Yaginuma, T. Wave Reflections and the Arterial Pulse. Arch. Intern. Med. 1984, 144, 366–371. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, P.E.; Barras, J.P.; Holstein, P. Systolic Pressure Amplification in the Arteries of Normal Subjects. Scand. J. Clin. Lab. Investig. 1974, 33, 371–377. [Google Scholar] [CrossRef]
- Murgo, J.P.; Westerhof, N.G.J.; Sa, A. A. Aortic input impedance in normal man: Relationship to pressure wave forms. Circulation 1980, 62, 105–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matthys, K.S.; Alastruey, J.; Peiró, J.; Khir, A.W.; Segers, P.; Verdonck, P.R.; Parker, K.H.; Sherwin, S.J. Pulse wave propagation in a model human arterial network: Assessment of 1-D numerical simulations against in vitro measurements. J. Biomech. 2007, 40, 3476–3486. [Google Scholar] [CrossRef] [PubMed]
- Hacham, W.S.; Khir, A.W. The speed, reflection and intensity of waves propagating in flexible tubes with aneurysm and stenosis: Experimental investigation. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2019, 233, 979–988. [Google Scholar] [CrossRef] [PubMed]
- Huttary, R.; Maier, A.; Bernhard, S. agbernhard.lse.thm.de/SISCA, GitLab. 2021. Available online: https://gitlab.com/agbernhard.lse.thm/sisca/ (accessed on 6 April 2022).











| Group | Corresponding Elements | (%) |
|---|---|---|
| Head | 17.52 | |
| Coronar Art. | 5.57 | |
| Arm dextra | 14.94 | |
| Arm sinistra | 10.27 | |
| Organs | 23.12 | |
| Femoralis | 9.51 | |
| Leg dextra | 10.44 | |
| Leg sinistra | 8.63 |
| No. | / | |
|---|---|---|
| I | 100% | 100% |
| II | 25% | 37.5% |
| III | 12.5% | 23.4% |
| IV | 3.3% | 6.56% |
| No. | (mmHg) | (mmHg) | (mmHg) | (mmHg) | (mL/s) | (mL/s) | (mL/s) |
|---|---|---|---|---|---|---|---|
| I | 132.0 | 37.2 | 73.7 | 0.7 | 9.4 | 2.4 | 0.1 |
| II | 133.0 | 37.4 | 73.9 | 0.8 | 9.3 | 2.4 | 0.1 |
| III | 126.0 | 37.0 | 72.4 | 0.7 | 8.6 | 2.3 | 0.1 |
| IV | 115.8 | 36.2 | 69.4 | 0.6 | 7.8 | 2.3 | 0.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wisotzki, M.; Mair, A.; Schlett, P.; Lindner, B.; Oberhardt, M.; Bernhard, S. In Vitro Major Arterial Cardiovascular Simulator to Generate Benchmark Data Sets for In Silico Model Validation. Data 2022, 7, 145. https://doi.org/10.3390/data7110145
Wisotzki M, Mair A, Schlett P, Lindner B, Oberhardt M, Bernhard S. In Vitro Major Arterial Cardiovascular Simulator to Generate Benchmark Data Sets for In Silico Model Validation. Data. 2022; 7(11):145. https://doi.org/10.3390/data7110145
Chicago/Turabian StyleWisotzki, Michelle, Alexander Mair, Paul Schlett, Bernhard Lindner, Max Oberhardt, and Stefan Bernhard. 2022. "In Vitro Major Arterial Cardiovascular Simulator to Generate Benchmark Data Sets for In Silico Model Validation" Data 7, no. 11: 145. https://doi.org/10.3390/data7110145