

Full-Body Mobility Data to Validate Inertial Measurement Unit Algorithms in Healthy and Neurological Cohorts
 , , , ,
, , , ,
Abstract
:1. Summary
2. Data Description
2.1. Subjects
2.2. Demographic Data and Clinical Scores
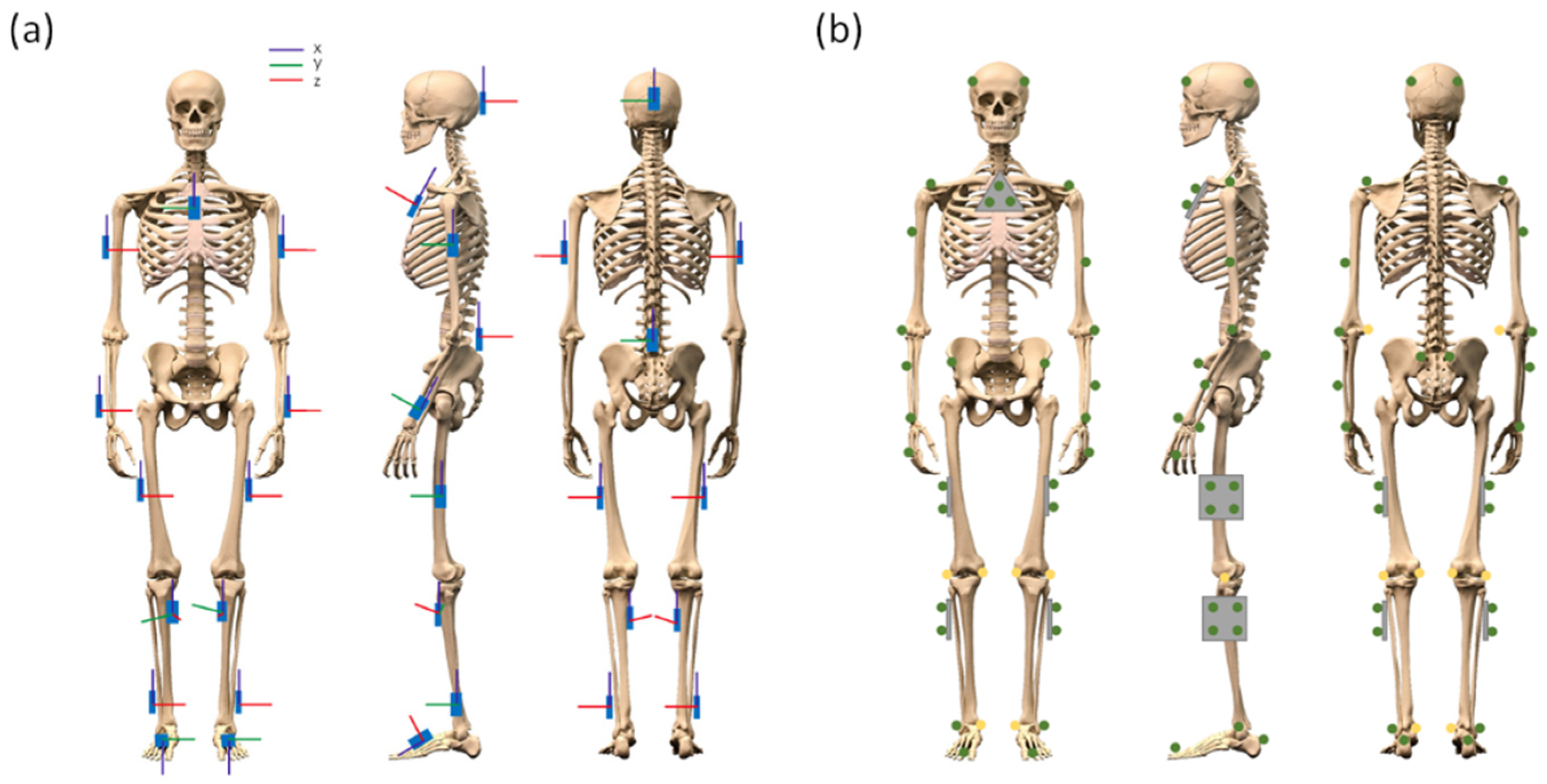
2.3. Equipment
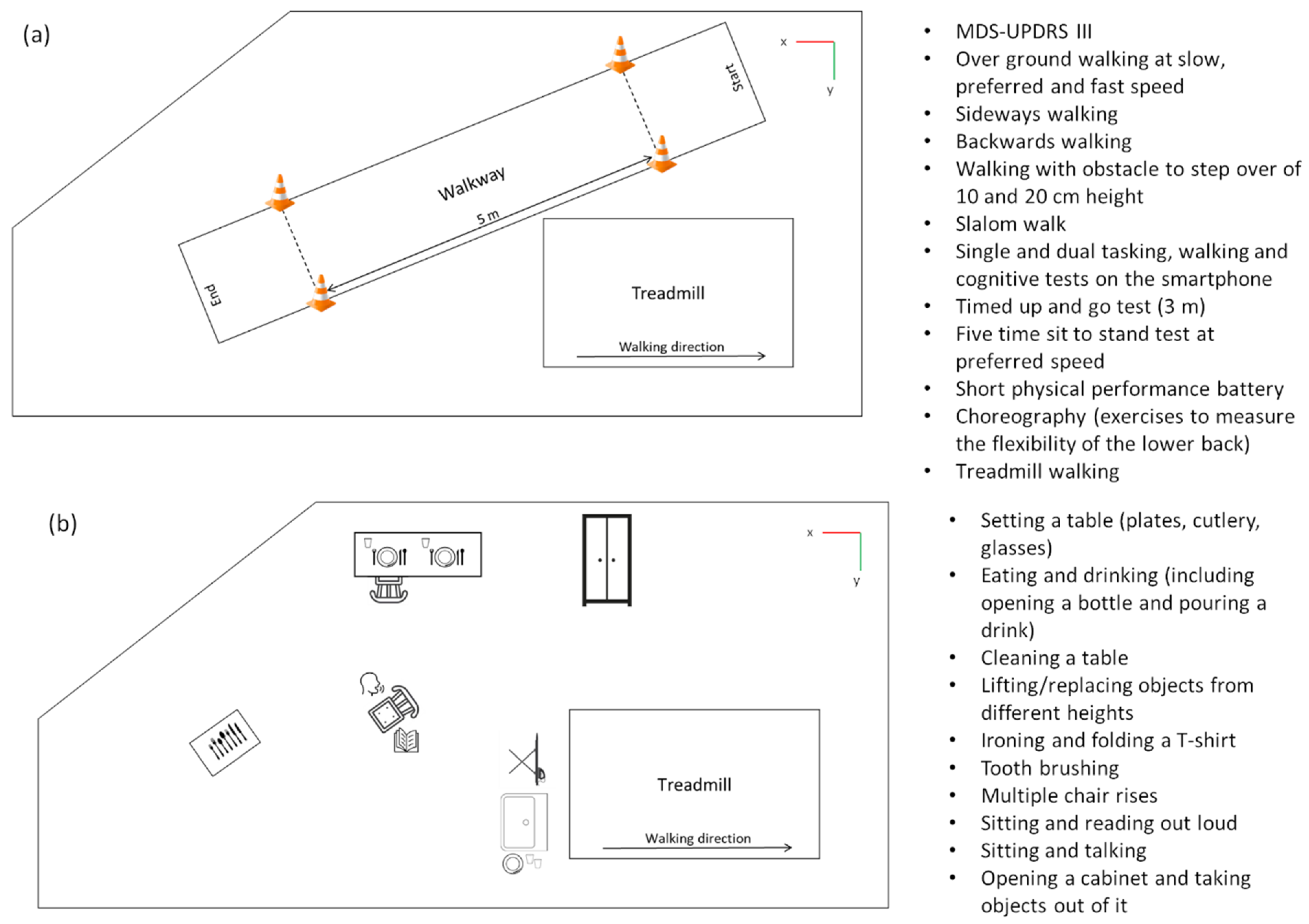
3. Methods
4. Data Records
- The column name (“name”);
- The type of data (e.g., “ACC” for acceleration and “ANGVEL” for angular velocity, “POS” for position);
- Which component, (e.g., “x”, “y”, “z”, or “err” for the residual);
- Which tracked point, (e.g., “head” and “sternum”);
- Which units, e.g., “mm” or “g”;
- Which sampling frequency was used (in Hz);
- The tracking system, that is “omc” for the optical motion capture system and “imu” for the inertial measurement units.
5. User Notes
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. International Classification of Functioning, Disability and Health. 2021. Available online: https://www.who.int/standards/classifications/international-classification-of-functioning-disability-and-health (accessed on 20 September 2022).
- Shafrin, J.; Sullivan, J.; Goldman, D.P.; Gill, T.M. The association between observed mobility and quality of life in the near elderly. PLoS ONE 2017, 12, e0182920. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.C.; Bryan, S.; Li, L.C.; Best, J.R.; Hsu, C.L.; Gomez, C.; Vertes, K.A.; Liu-Ambrose, T. Mobility and cognition are associated with wellbeing and health related quality of life among older adults: A cross-sectional analysis of the Vancouver Falls Prevention Cohort. BMC Geriatr. 2015, 15, 75. [Google Scholar] [CrossRef] [PubMed]
- Mirelman, A.; Bonato, P.; Camicioli, R.; Ellis, T.D.; Giladi, N.; Hamilton, J.L.; Hass, C.J.; Hausdorff, J.M.; Pelosin, E.; Almeida, Q.J. Gait impairments in Parkinson’s disease. Lancet Neurol. 2019, 18, 697–708. [Google Scholar] [CrossRef]
- Creaby, M.W.; Cole, M.H. Gait characteristics and falls in Parkinson’s disease: A systematic review and meta-analysis. Park. Relat. Disord. 2018, 57, 1–8. [Google Scholar] [CrossRef]
- Comber, L.; Galvin, R.; Coote, S. Gait deficits in people with multiple sclerosis: A systematic review and meta-analysis. Gait Posture 2017, 51, 25–35. [Google Scholar] [CrossRef]
- E Hicks, G.; Sions, J.M.; Coyle, P.C.; Pohlig, R.T. Altered spatiotemporal characteristics of gait in older adults with chronic low back pain. Gait Posture 2017, 55, 172–176. [Google Scholar] [CrossRef]
- Warmerdam, E.; Romijnders, R.; Hansen, C.; Elshehabi, M.; Zimmermann, M.; Metzger, F.G.; von Thaler, A.K.; Berg, D.; Schmidt, G.; Maetzler, W. Arm swing responsiveness to dopaminergic medication in Parkinson’ s disease depends on task complexity. npj Parkinson’s Dis. 2021, 7, 89. [Google Scholar] [CrossRef]
- Wonsetler, E.C.; Bowden, M.G. A systematic review of mechanisms of gait speed change post-stroke. Part 1: Spatiotemporal parameters and asymmetry ratios. Top. Stroke Rehabil. 2017, 24, 435–446. [Google Scholar] [CrossRef]
- Dowd, H.; Zdrodowska, M.A.; Radler, K.H.; Cersonsky, T.E.K.; Rao, A.K.; Huey, E.D.; Cosentino, S.; Louis, E.D. Prospective Longitudinal Study of Gait and Balance in a Cohort of Elderly Essential Tremor Patients. Front. Neurol. 2020, 11, 1–14. [Google Scholar] [CrossRef]
- Schlachetzki, J.C.M.; Barth, J.; Marxreiter, F.; Gossler, J.; Kohl, Z.; Reinfelder, S.; Gassner, H.; Aminian, K.; Eskofier, B.M.; Winkler, J.; et al. Wearable sensors objectively measure gait parameters in Parkinson’s disease. PLoS ONE 2017, 12, e0183989. [Google Scholar] [CrossRef]
- Schloemer, S.A.; Thompson, J.A.; Silder, A.; Thelen, D.G.; Siston, R.A. Age-Related Differences in Gait Kinematics, Kinetics, and Muscle Function: A Principal Component Analysis. Ann. Biomed. Eng. 2017, 45, 695–710. [Google Scholar] [CrossRef] [PubMed]
- Baker, J.M. Gait Disorders. Am. J. Med. 2018, 131, 602–607. [Google Scholar] [CrossRef] [PubMed]
- Topley, M.; Richards, J.G. A comparison of currently available optoelectronic motion capture systems. J. Biomech. 2020, 106, 109820. [Google Scholar] [CrossRef] [PubMed]
- Buckley, A.C.; Galna, B.; Rochester, L.; Mazz, C. Upper body accelerations as a biomarker of gait impairment in the early stages of Parkinson’s disease. Gait Posture 2019, 71, 289–295. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool For Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Deyo, R.A.; Cherkin, D.C.; Ciol, M.A. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J. Clin. Epidemiol. 1992, 45, 613–619. [Google Scholar] [CrossRef]
- Feng, Y.-S.; Kohlmann, T.; Janssen, M.F.; Buchholz, I. Psychometric properties of the EQ-5D-5L: A systematic review of the literature. Qual. Life Res. 2020, 30, 647–673. [Google Scholar] [CrossRef]
- Graf, C. The Lawton Instrumental Activities of Daily Living Scale. AJN Am. J. Nurs. 2008, 108, 52–62. [Google Scholar] [CrossRef]
- Malmstrom, T.K.; Miller, D.K.; Simonsick, E.M.; Ferrucci, L.; Morley, J.E. SARC-F: A symptom score to predict persons with sarcopenia at risk for poor functional outcomes. J. Cachexia Sarcopenia Muscle 2016, 7, 28–36. [Google Scholar] [CrossRef]
- Haase, I.; Schwarz, A.; Burger, A.; Kladny, B. Der funktionsfragebogen hannover (FFbH) und die subskala “körperliche funktionsfähigkeit” aus dem SF-36 im vergleich. Rehabilitation 2001, 40, 40–42. [Google Scholar] [CrossRef]
- Luszczynska, A.; Scholz, U.; Schwarzer, R. The General Self-Efficacy Scale: Multicultural Validation Studies. J. Psychol. 2005, 139, 439–457. [Google Scholar] [CrossRef] [PubMed]
- Herlofson, K.; Larsen, J.P. Measuring fatigue in patients with Parkinson’s disease—the Fatigue Severity Scale. Eur. J. Neurol. 2002, 9, 595–600. [Google Scholar] [CrossRef] [PubMed]
- Williamson, A.; Hoggart, B. Pain: A review of three commonly used pain rating scales. J. Clin. Nurs. 2005, 14, 798–804. [Google Scholar] [CrossRef] [PubMed]
- Goetz, C.G.; Tilley, B.C.; Shaftman, S.R.; Stebbins, G.T.; Fahn, S.; Martinez-Martin, P.; Poewe, W.; Sampaio, C.; Stern, M.B.; Dodel, R.; et al. Movement Disorder Society-sponsored revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS): Scale presentation and clinimetric testing results. Mov. Disord. 2008, 23, 2129–2170. [Google Scholar] [CrossRef]
- Pestronk, A.; Florence, J.; Levine, T.; Al-Lozi, M.T.; Lopate, G.; Miller, T.; Ramneantu, I.; Waheed, W.; Stambuk, M. Sensory exam with a quantitative tuning fork: Rapid, sensitive and predictive of SNAP amplitude. Neurology 2004, 62, 461–464. [Google Scholar] [CrossRef] [PubMed]
- Hoehn, M.M.; Yahr, M.D. Parkinsonism: Onset, progression, and mortality. Neurology 1967, 17, 427–442. [Google Scholar] [CrossRef]
- Kurtzke, J.F. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology 1983, 33, 1444–1452. [Google Scholar] [CrossRef]
- Brott, T.; Adams, H.P.; Olinger, C.P.; Marler, J.R.; Barsan, W.G.; Biller, J.; Spilker, J.; Holleran, R.; Eberle, R.; Hertzberg, V. Measurements of acute cerebral infarction: A clinical examination scale. Stroke 1989, 20, 864–870. [Google Scholar] [CrossRef]
- Warmerdam, E.; Romijnders, R.; Geritz, J.; Elshehabi, M.; Maetzler, C.; Otto, J.C.; Reimer, M.; Stuerner, K.; Baron, R.; Paschen, S.; et al. Proposed Mobility Assessments with Simultaneous Full-Body Inertial Measurement Units and Optical Motion Capture in Healthy Adults and Neurological Patients for Future Validation Studies: Study Protocol. Sensors 2021, 21, 5833. [Google Scholar] [CrossRef]
- Welzel, J.; Jueng, S. Brain Imaging Data Structure. BEP029. Available online: https://bids.neuroimaging.io/get_involved.html#extending-the-bids-specification (accessed on 20 September 2022).
- Gorgolewski, K.J.; Auer, T.; Calhoun, V.D.; Craddock, R.C.; Das, S.; Duff, E.P.; Flandin, G.; Ghosh, S.S.; Glatard, T.; Halchenko, Y.O.; et al. The brain imaging data structure, a format for organizing and describing outputs of neuroimaging experiments. Sci. Data 2016, 3, 160044. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Healthy Adults (18–60 Years) | Healthy Elderly (>60 Years) | Patients with PD | Patients with Stroke | Patients with Multiple Sclerosis | Patients with Chronic Low Back Pain | Patients with Other Diagnosis | Total | |
|---|---|---|---|---|---|---|---|---|
| n [% male] | 43 (51%) | 24 (50%) | 34 (62%) | 23 (74%) | 21 (38%) | 10 (70%) | 12 (75%) | 167 (58%) |
| Age [years] | 29 ± 8 | 72 ± 6 | 65 ± 11 | 68 ± 16 | 39 ± 13 | 64 ± 15 | 66 ± 17 | 54 ± 21 |
| Height [m] | 1.79 ± 0.09 | 1.74 ± 0.10 | 1.74 ± 0.09 | 1.73 ± 0.10 | 1.80 ± 0.12 | 1.75 ± 0.09 | 1.77 ± 0.09 | 1.76 ± 0.10 |
| Weight [kg] | 74 ± 13 | 79 ± 17 | 81 ± 18 | 79 ± 17 | 84 ± 24 | 83 ± 19 | 85 ± 15 | 79 ± 17 |
| MoCA (0–30) | 29 ± 2 | 25 ± 4 | 23 ± 3 | 22 ± 4 | 27 ± 3 | 25 ± 2 | 24 ± 4 | 26 ± 4 |
| MDS-UPDRS III (0–132) | 1 ± 2 | 5 ± 4 | 27 ± 20 | 6 ± 6 | 9 ± 8 | 6 ± 5 | 11 ± 9 | 9 ± 14 |
| SARC-F (0–10) | 0.14 ± 0.35 | 0.71 ± 1.02 | 2.38 ± 2.00 | 1.33 ± 1.86 | 1.33 ± 1.32 | 0.75 ± 1.23 | 2.83 ± 1.95 | 1.29 ± 1.73 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Warmerdam, E.; Hansen, C.; Romijnders, R.; Hobert, M.A.; Welzel, J.; Maetzler, W. Full-Body Mobility Data to Validate Inertial Measurement Unit Algorithms in Healthy and Neurological Cohorts. Data 2022, 7, 136. https://doi.org/10.3390/data7100136
Warmerdam E, Hansen C, Romijnders R, Hobert MA, Welzel J, Maetzler W. Full-Body Mobility Data to Validate Inertial Measurement Unit Algorithms in Healthy and Neurological Cohorts. Data. 2022; 7(10):136. https://doi.org/10.3390/data7100136
Chicago/Turabian StyleWarmerdam, Elke, Clint Hansen, Robbin Romijnders, Markus A. Hobert, Julius Welzel, and Walter Maetzler. 2022. "Full-Body Mobility Data to Validate Inertial Measurement Unit Algorithms in Healthy and Neurological Cohorts" Data 7, no. 10: 136. https://doi.org/10.3390/data7100136