
Complicated Crown Fracture of Permanent Incisors: A Conservative Treatment Case Report and a Narrative Review
 ,
,  , and
, and 
Abstract
:1. Introduction
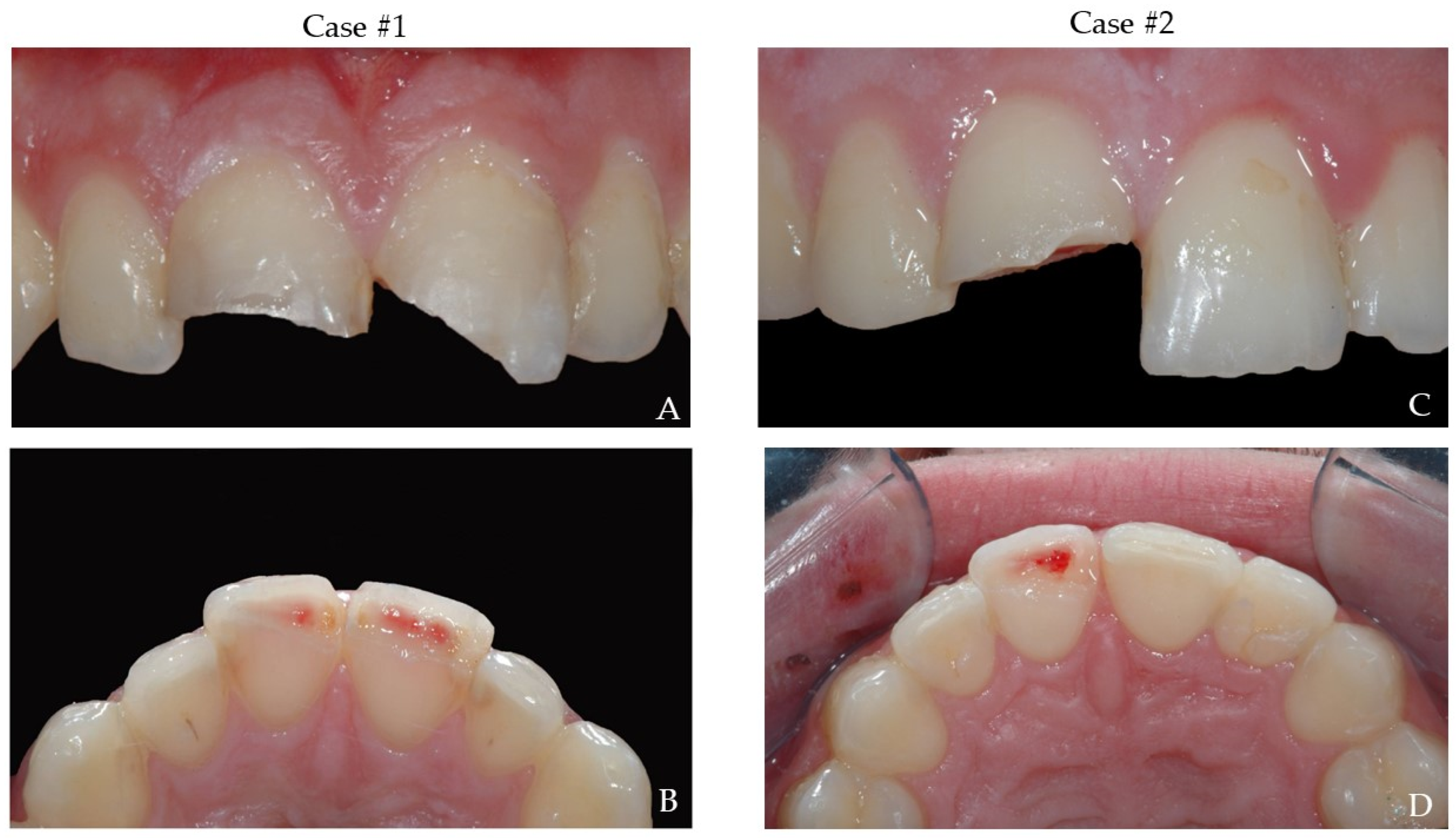
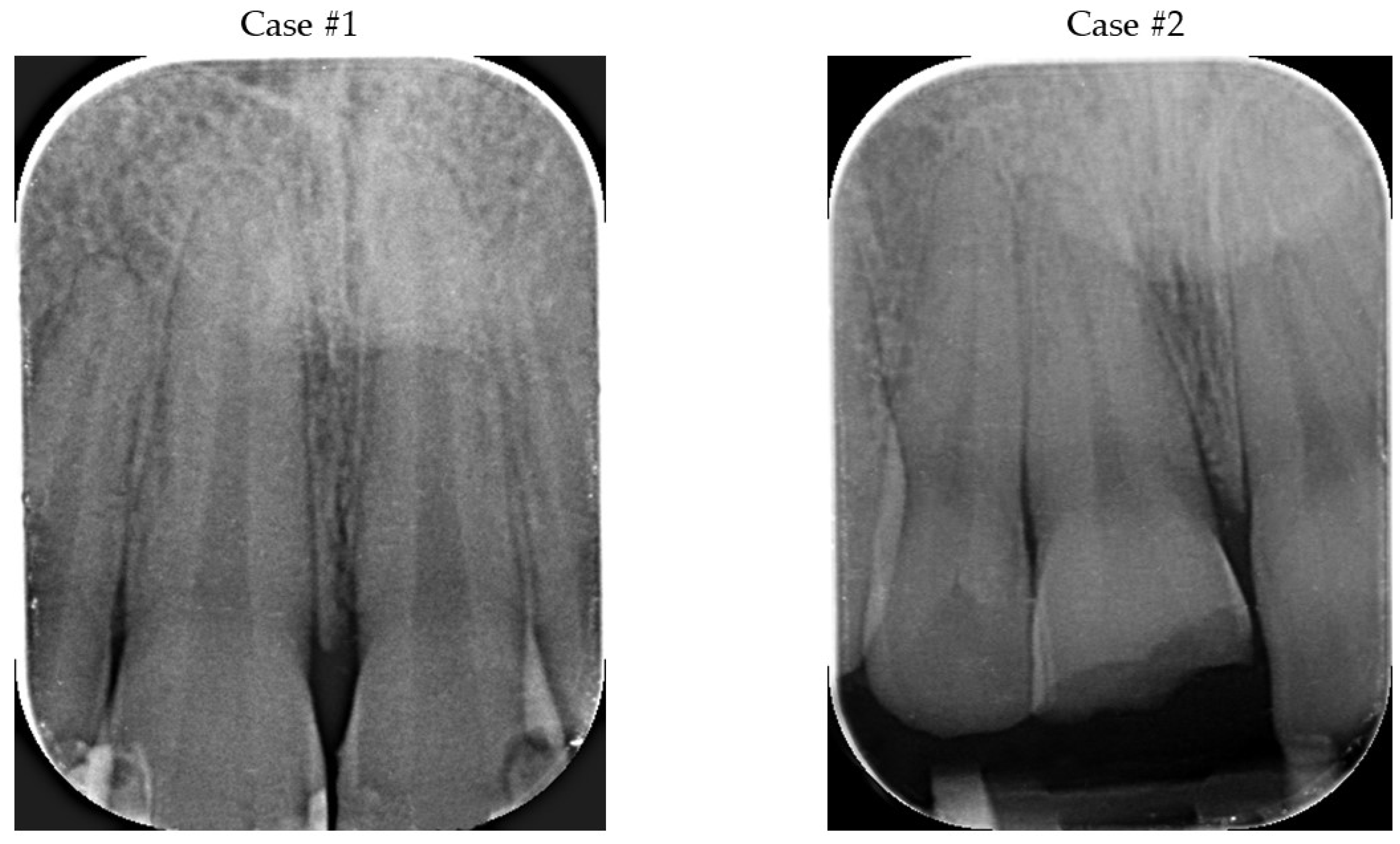
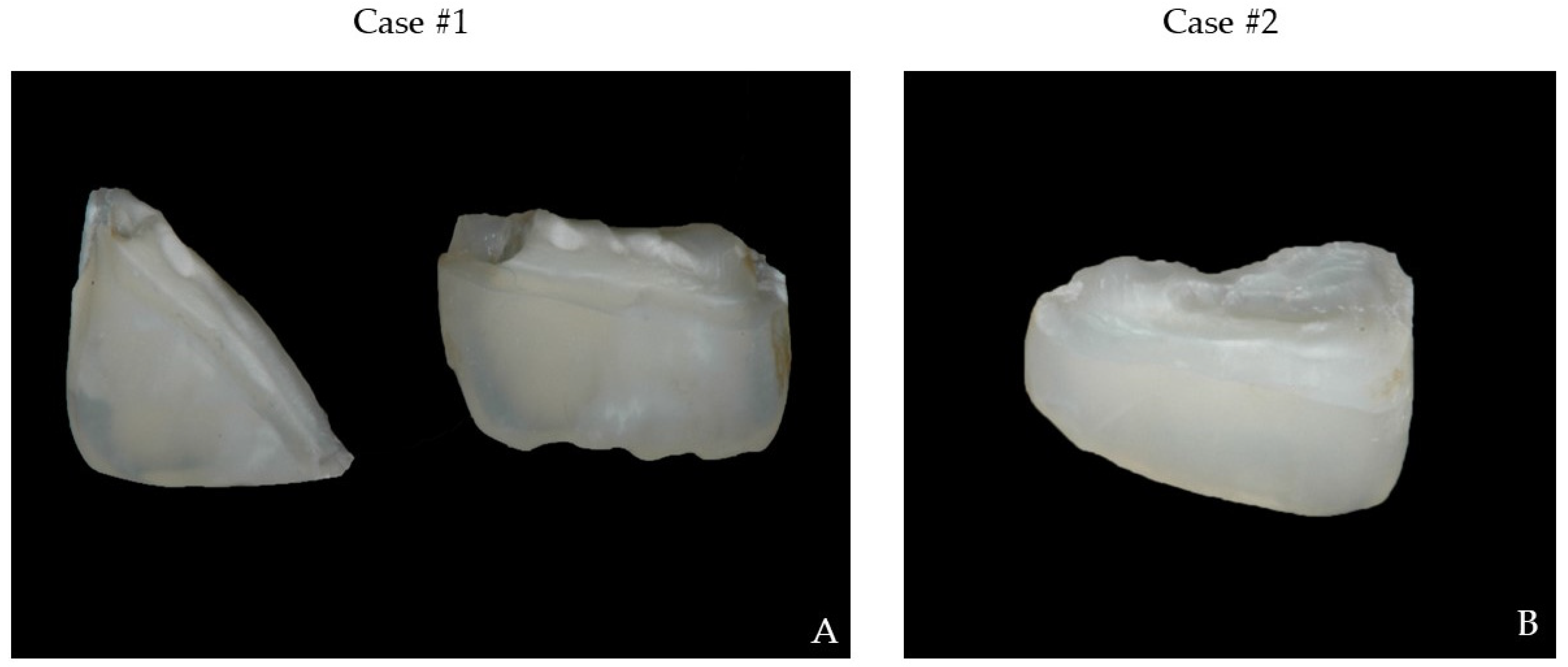
2. Presentation of Cases
2.1. Diagnosis
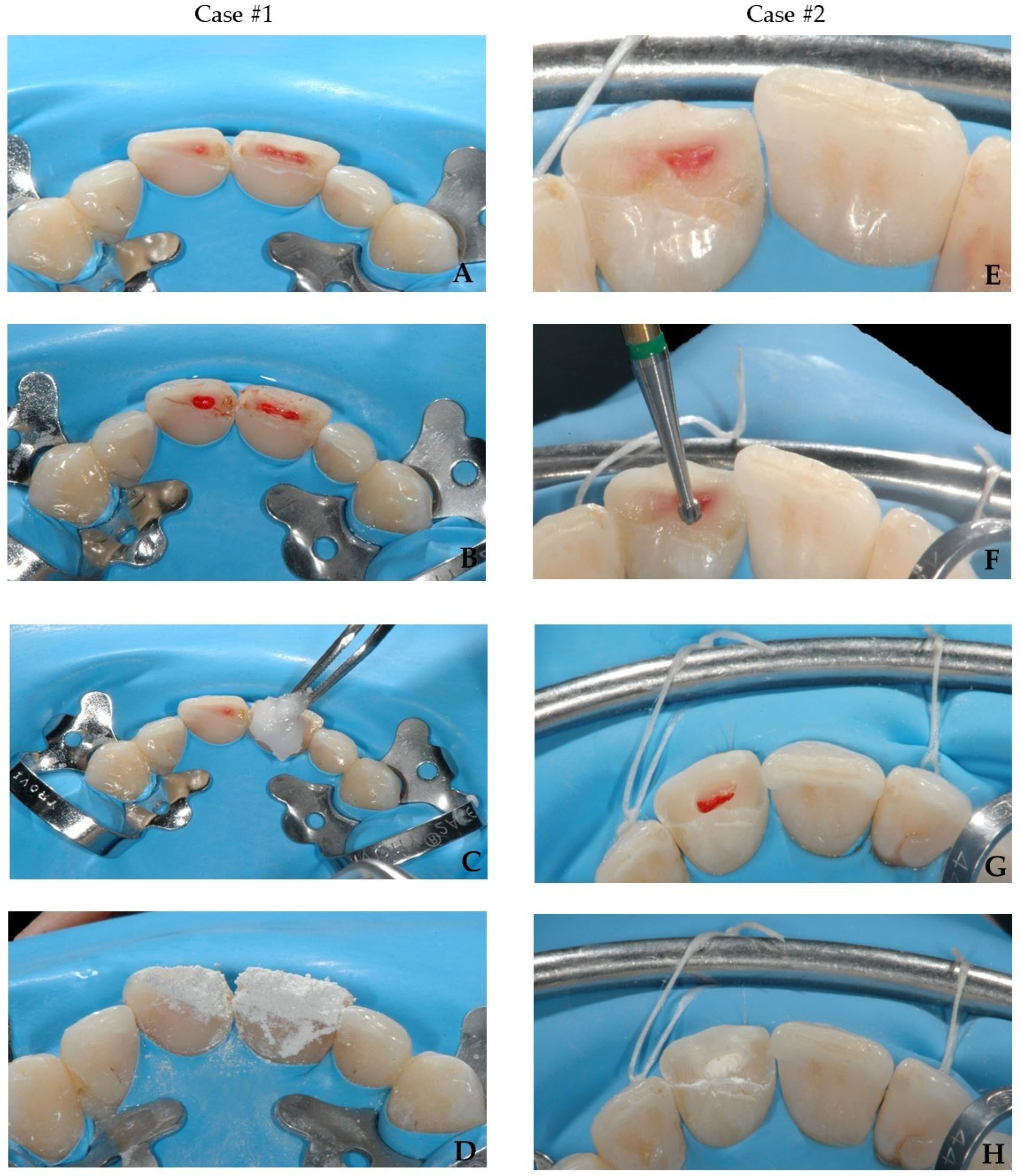
2.2. Pulp Treatment Option
2.3. Preparation of Operatory Field
2.4. Choice of Materials
2.5. Restorative Procedure
2.6. Occlusion Adjustment
2.7. Finishing and Polishing
2.8. Follow-Up Visits and Prognosis
3. Prognosis and Future Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bourguignon, C.; Cohenca, N.; Lauridsen, E.; Flores, M.T.; O’Connell, A.C.; Day, P.F.; Tsilingaridis, G.; Abbott, P.V.; Fouad, A.F.; Hicks, L.; et al. International Association of Dental Traumatology Guidelines for the Management of Traumatic Dental Injuries: 1. Fractures and Luxations. Dent. Traumatol. 2020, 36, 314–330. [Google Scholar] [CrossRef] [PubMed]
- Diangelis, A.J.; Andreasen, J.O.; Ebeleseder, K.A.; Kenny, D.J.; Trope, M.; Sigurdsson, A.; Andersson, L.; Bourguignon, C.; Flores, M.T.; Hicks, M.L.; et al. Guidelines for the Management of Traumatic Dental Injuries: 1. Fractures and Luxations of Permanent Teeth. Pediatr. Dent. 2017, 39, 401–411. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, V.; Logani, A.; Shah, N. Complicated Crown Fractures—Management and Treatment Options. Int. Endod. J. 2009, 42, 740–753. [Google Scholar] [CrossRef] [PubMed]
- Ojeda-Gutierrez, F.; Martinez-Marquez, B.; Arteaga-Larios, S.; Ruiz-Rodriguez, M.S.; Pozos-Guillen, A. Management and Followup of Complicated Crown Fractures in Young Patients Treated with Partial Pulpotomy. Case Rep. Dent. 2013, 2013, 597563. [Google Scholar] [CrossRef]
- Dharmani, C.K.; Pathak, A.; Sidhu, H.S. Prevalence of Traumatic Dental Injuries to Anterior Teeth in 8-12-Year-Old Schoolchildren of Patiala City, Punjab, India: An Epidemiological Study. Int. J. Clin. Pediatr. Dent. 2019, 12, 25–29. [Google Scholar] [CrossRef]
- Juneja, P.; Kulkarni, S.; Raje, S. Prevalence of Traumatic Dental Injuries and Their Relation with Predisposing Factors among 8-15 Years Old School Children of Indore City, India. Clujul Med. 2018, 91, 328–335. [Google Scholar] [CrossRef]
- Levin, L.; Day, P.F.; Hicks, L.; O’Connell, A.; Fouad, A.F.; Bourguignon, C.; Abbott, P.V. International Association of Dental Traumatology Guidelines for the Management of Traumatic Dental Injuries: General Introduction. Dent. Traumatol. 2020, 36, 309–313. [Google Scholar] [CrossRef]
- Gopikrishna, V.; Tinagupta, K.; Kandaswamy, D. Comparison of Electrical, Thermal, and Pulse Oximetry Methods for Assessing Pulp Vitality in Recently Traumatized Teeth. J. Endod. 2007, 33, 531–535. [Google Scholar] [CrossRef]
- Marinčák, D.; Doležel, V.; Přibyl, M.; Voborná, I.; Marek, I.; Šedý, J.; Žižka, R. Conservative Treatment of Complicated Crown Fracture and Crown-Root Fracture of Young Permanent Incisor—A Case Report with 24-Month Follow-Up. Children 2021, 8, 725. [Google Scholar] [CrossRef]
- Cohenca, N.; Silberman, A. Contemporary Imaging for the Diagnosis and Treatment of Traumatic Dental Injuries: A Review. Dent. Traumatol. Off. Publ. Int. Assoc. Dent. Traumatol. 2017, 33, 321–328. [Google Scholar] [CrossRef] [Green Version]
- Matoug-Elwerfelli, M.; ElSheshtawy, A.S.; Duggal, M.; Tong, H.J.; Nazzal, H. Vital Pulp Treatment for Traumatized Permanent Teeth: A Systematic Review. Int. Endod. J. 2022, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.T.; Xia, B.; Xu, Z.; Dou, G.; Lei, Y.; Yong, W. The Effect of Partial Pulpotomy with IRoot BP Plus in Traumatized Immature Permanent Teeth: A Randomized Prospective Controlled Trial. Dent. Traumatol. 2020, 36, 518–525. [Google Scholar] [CrossRef] [PubMed]
- Krastl, G.; Weiger, R.; Filippi, A.; Van Waes, H.; Ebeleseder, K.; Ree, M.; Connert, T.; Widbiller, M.; Tjäderhane, L.; Dummer, P.M.H.; et al. Endodontic Management of Traumatized Permanent Teeth: A Comprehensive Review. Int. Endod. J. 2021, 54, 1221–1245. [Google Scholar] [CrossRef] [PubMed]
- Cvek, M. Partial Pulpotomy in Crown—Fractured Incisors—Results 3 to 15 Years After Treatment. Acta Stomatol. Croat. 1993, 27, 167–173. [Google Scholar]
- Aguilar, P.; Linsuwanont, P. Vital Pulp Therapy in Vital Permanent Teeth with Cariously Exposed Pulp: A Systematic Review. J. Endod. 2011, 37, 581–587. [Google Scholar] [CrossRef]
- Haikal, L.; Ferraz Dos Santos, B.; Vu, D.-D.; Braniste, M.; Dabbagh, B. Biodentine Pulpotomies on Permanent Traumatized Teeth with Complicated Crown Fractures. J. Endod. 2020, 46, 1204–1209. [Google Scholar] [CrossRef]
- da Rosa, W.L.O.; Piva, E.; da Silva, A.F. Disclosing the Physiology of Pulp Tissue for Vital Pulp Therapy. Int. Endod. J. 2018, 51, 829–846. [Google Scholar] [CrossRef]
- Santos, J.M.; Pereira, J.F.; Marques, A.; Sequeira, D.B.; Friedman, S. Vital Pulp Therapy in Permanent Mature Posterior Teeth with Symptomatic Irreversible Pulpitis: A Systematic Review of Treatment Outcomes. Medicina 2021, 57, 573. [Google Scholar] [CrossRef]
- Mutluay, M.; Arikan, V.; Sari, S.; Kisa, Ü. Does Achievement of Hemostasis after Pulp Exposure Provide an Accurate Assessment of Pulp Inflammation? Pediatr. Dent. 2018, 40, 37–42. [Google Scholar]
- Asgary, S.; Parhizkar, A. Importance of ‘Time’ on ‘Haemostasis’ in Vital Pulp Therapy—Letter to the Editor. Eur. Endod. J. 2021, 6, 128–129. [Google Scholar] [CrossRef]
- Zanini, M.; Hennequin, M.; Cousson, P.Y. Which Procedures and Materials Could Be Applied for Full Pulpotomy in Permanent Mature Teeth? A Systematic Review. Acta Odontol. Scand. 2019, 77, 541–551. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Godoy, F.; Murray, P. Systemic Evaluation of Various Haemostatic Agents Following Local Application Prior to Direct Pulp Capping. Braz. J. Oral Sci. 2005, 4, 791–797. [Google Scholar] [CrossRef]
- AAE Position Statement on Vital Pulp Therapy. J. Endod. 2021, 47, 1340–1344. [CrossRef] [PubMed]
- Chen, Y.; Chen, X.; Zhang, Y.; Zhou, F.; Deng, J.; Zou, J.; Wang, Y. Materials for Pulpotomy in Immature Permanent Teeth: A Systematic Review and Meta-Analysis. BMC Oral Health 2019, 19, 227. [Google Scholar] [CrossRef] [PubMed]
- Till, D.; Galler, K. Current Recommendations for Vital Pulp Treatment. Dtsch. Zahnärztliche Zeitschrift Int. 2019, 1, 43–52. [Google Scholar]
- Graham, L.; Cooper, P.R.; Cassidy, N.; Nor, J.E.; Sloan, A.J.; Smith, A.J. The Effect of Calcium Hydroxide on Solubilisation of Bio-Active Dentine Matrix Components. Biomaterials 2006, 27, 2865–2873. [Google Scholar] [CrossRef] [PubMed]
- Hebling, J.; Lessa, F.C.R.; Nogueira, I.; Carvalho, R.M.; Costa, C.A.S. Cytotoxicity of Resin-Based Light-Cured Liners. Am. J. Dent. 2009, 22, 137–142. [Google Scholar]
- Jalan, A.L.; Warhadpande, M.M.; Dakshindas, D.M. A Comparison of Human Dental Pulp Response to Calcium Hydroxide and Biodentine as Direct Pulp-Capping Agents. J. Conserv. Dent. 2017, 20, 129–133. [Google Scholar] [CrossRef]
- Ravi, G.; Subramanyam, R. Possible Mechanisms of Lack of Dentin Bridge Formation in Response to Calcium Hydroxide in Primary Teeth. Dent. Hypotheses 2015, 6, 6–9. [Google Scholar] [CrossRef]
- Kolasa, M.; Szczepańska, J. Direct Pulp Capping in Permanent Teeth in Children—Tertiary Dentin Formation, Materials Used. Part II. Nowa Stomatol. 2018, 23, 78–83. [Google Scholar] [CrossRef]
- Malhotra, N.; Agarwal, A.; Mala, K. Mineral Trioxide Aggregate: A Review of Physical Properties. Compend. Contin. Educ. Dent. 2013, 34, e25–e32. [Google Scholar] [PubMed]
- Abedi-Amin, A.; Luzi, A.; Giovarruscio, M.; Paolone, G.; Darvizeh, A.; Agulló, V.V.; Sauro, S. Innovative Root-End Filling Materials Based on Calcium-Silicates and Calcium-Phosphates. J. Mater. Sci. Mater. Med. 2017, 28, 31. [Google Scholar] [CrossRef] [PubMed]
- Islam, I.; Chng, H.K.; Yap, A.U.J. Comparison of the Physical and Mechanical Properties of MTA and Portland Cement. J. Endod. 2006, 32, 193–197. [Google Scholar] [CrossRef] [PubMed]
- Kunert, M.; Lukomska-Szymanska, M. Bio-Inductive Materials in Direct and Indirect Pulp Capping—A Review Article. Materials 2020, 13, 1204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parirokh, M.; Torabinejad, M. Mineral Trioxide Aggregate: A Comprehensive Literature Review—Part III: Clinical Applications, Drawbacks, and Mechanism of Action. J. Endod. 2010, 36, 400–413. [Google Scholar] [CrossRef] [PubMed]
- Pelepenko, L.E.; Saavedra, F.; Bombarda, G.F.; Gomes, B.P.F.D.A.; De-Jesus-Soares, A.; Zaia, A.A.; Duarte, M.A.H.; Tanomaru-Filho, M.; Marciano, M.A. Dental Discoloration Caused by Grey-Mtaflow Cement: Analysis of Its Physicochemical, Biological and Antimicrobial Properties. J. Appl. Oral Sci. 2020, 28, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Salem-Milani, A.; Ghasemi, S.; Rahimi, S.; Ardalan-Abdollahi, A.; Asghari-Jafarabadi, M. The Discoloration Effect of White Mineral Trioxide Aggregate (WMTA), Calcium Enriched Mixture (CEM), and Portland Cement (PC) on Human Teeth. J. Clin. Exp. Dent. 2017, 9, e1397–e1401. [Google Scholar] [CrossRef]
- Możyńska, J.; Metlerski, M.; Lipski, M.; Nowicka, A. Tooth Discoloration Induced by Different Calcium Silicate-Based Cements: A Systematic Review of In Vitro Studies. J. Endod. 2017, 43, 1593–1601. [Google Scholar] [CrossRef]
- Camilleri, J. Color Stability of White Mineral Trioxide Aggregate in Contact with Hypochlorite Solution. J. Endod. 2014, 40, 436–440. [Google Scholar] [CrossRef]
- Jang, J.-H.; Kang, M.; Ahn, S.; Kim, S.; Kim, W.; Kim, Y.; Kim, E. Tooth Discoloration after the Use of New Pozzolan Cement (Endocem) and Mineral Trioxide Aggregate and the Effects of Internal Bleaching. J. Endod. 2013, 39, 1598–1602. [Google Scholar] [CrossRef]
- Marciano, M.A.; Camilleri, J.; Lucateli, R.L.; Costa, R.M.; Matsumoto, M.A.; Duarte, M.A.H. Physical, Chemical, and Biological Properties of White MTA with Additions of AlF(3). Clin. Oral Investig. 2019, 23, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Marciano, M.A.; Camilleri, J.; Costa, R.M.; Matsumoto, M.A.; Guimarães, B.M.; Duarte, M.A.H. Zinc Oxide Inhibits Dental Discoloration Caused by White Mineral Trioxide Aggregate Angelus. J. Endod. 2017, 43, 1001–1007. [Google Scholar] [CrossRef] [PubMed]
- Meraji, N.; Bolhari, B.; Sefideh, M.; Niavarzi, S. Prevention of Tooth Discoloration Due to Calcium-Silicate Cements: A Review. Dent. Hypotheses 2019, 10, 4–8. [Google Scholar] [CrossRef]
- Choi, Y.L.; Jang, Y.E.; Kim, B.S.; Kim, J.W.; Kim, Y. Pre-Application of Dentin Bonding Agent Prevents Discoloration Caused by Mineral Trioxide Aggregate. BMC Oral Health 2020, 20, 163. [Google Scholar] [CrossRef]
- Kadali, N.; Alla, R.K.; Guduri, V.; AV, R.; MC, S.S.; Raju, R.V. Mineral Trioxide Aggregate: An Overview of Composition, Properties and Clinical Applications. Int. J. Dent. Mater. 2020, 02, 11–18. [Google Scholar] [CrossRef]
- Arruda, R.A.A.; Cunha, R.S.; Miguita, K.B.; Silveira, C.F.M.; De Martin, A.S.; Pinheiro, S.L.; Rocha, D.G.P.; Bueno, C.E.S. Sealing Ability of Mineral Trioxide Aggregate (MTA) Combined with Distilled Water, Chlorhexidine, and Doxycycline. J. Oral Sci. 2012, 54, 233–239. [Google Scholar] [CrossRef]
- Jacinto, R.C.; Linhares-Farina, G.; da Sposito, O.S.; Zanchi, C.H.; Cenci, M.S. Influence of 2% Chlorhexidine on PH, Calcium Release and Setting Time of a Resinous MTA-Based Root-End Filling Material. Braz. Oral Res. 2015, 29, 1–6. [Google Scholar] [CrossRef]
- Nekoofar, M.H.; Adusei, G.; Sheykhrezae, M.S.; Hayes, S.J.; Bryant, S.T.; Dummer, P.M.H. The Effect of Condensation Pressure on Selected Physical Properties of Mineral Trioxide Aggregate. Int. Endod. J. 2007, 40, 453–461. [Google Scholar] [CrossRef]
- Musale, P.K.; Kothare, S.S.; Soni, A.S. Mineral Trioxide Aggregate Pulpotomy: Patient Selection and Perspectives. Clin. Cosmet. Investig. Dent. 2018, 10, 37–43. [Google Scholar] [CrossRef]
- Alqaderi, H.; Lee, C.-T.; Borzangy, S.; Pagonis, T.C. Coronal Pulpotomy for Cariously Exposed Permanent Posterior Teeth with Closed Apices: A Systematic Review and Meta-Analysis. J. Dent. 2016, 44, 1–7. [Google Scholar] [CrossRef]
- El-Meligy, O.A.S.; Avery, D.R. Comparison of Mineral Trioxide Aggregate and Calcium Hydroxide as Pulpotomy Agents in Young Permanent Teeth (Apexogenesis). Pediatr. Dent. 2006, 28, 399–404. [Google Scholar] [PubMed]
- Özgür, B.; Uysal, S.; Güngör, H.C. Partial Pulpotomy in Immature Permanent Molars After Carious Exposures Using Different Hemorrhage Control and Capping Materials. Pediatr. Dent. 2017, 39, 364–370. [Google Scholar] [PubMed]
- Witherspoon, D.E. Vital Pulp Therapy with New Materials: New Directions and Treatment Perspectives—Permanent Teeth. J. Endod. 2008, 34, S25–S28. [Google Scholar] [CrossRef] [PubMed]
- Qudeimat, M.A.; Barrieshi-Nusair, K.M.; Owais, A.I. Calcium Hydroxide vs Mineral Trioxide Aggregates for Partial Pulpotomy of Permanent Molars with Deep Caries. Eur. Arch. Paediatr. Dent. Off. J. Eur. Acad. Paediatr. Dent. 2007, 8, 99–104. [Google Scholar] [CrossRef]
- Siddiqui, S.H.; Mohamed, A.N. Calcific Metamorphosis: A Review. Int. J. Health Sci. 2016, 10, 437–442. [Google Scholar] [CrossRef]
- AlQhtani, F.A. Reattachment of a Dehydrated Tooth Fragment Using Retentive Holes. Cureus 2020, 12, e6640. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, Y.; Guler, C.; Sahin, H.; Eyuboglu, O. Evaluation of Tooth-Fragment Reattachment: A Clinical and Laboratory Study. Dent. Traumatol. 2010, 26, 308–314. [Google Scholar] [CrossRef] [PubMed]
- Toshihiro, K.; Rintaro, T. Rehydration of Crown Fragment 1 Year after Reattachment: A Case Report. Dent. Traumatol. Off. Publ. Int. Assoc. Dent. Traumatol. 2005, 21, 297–300. [Google Scholar] [CrossRef] [PubMed]
- Bissinger, R.; Müller, D.D.; Hickel, R.; Kühnisch, J. Survival Analysis of Adhesive Reattachments in Permanent Teeth with Crown Fractures after Dental Trauma. Dent. Traumatol. 2021, 37, 208–214. [Google Scholar] [CrossRef]
- Madhubala, A.; Tewari, N.; Mathur, V.P.; Bansal, K. Comparative Evaluation of Fracture Resistance Using Two Rehydration Protocols for Fragment Reattachment in Uncomplicated Crown Fractures. Dent. Traumatol. 2019, 35, 199–203. [Google Scholar] [CrossRef]
- Reis, A.; Kraul, A.; Francci, C.; de Assis, T.G.R.; Crivelli, D.D.; Oda, M.; Loguercio, A.D. Re-Attachment of Anterior Fractured Teeth: Fracture Strength Using Different Materials. Oper. Dent. 2002, 27, 621–627. [Google Scholar] [PubMed]
- Demarco, F.F.; Fay, R.-M.; Pinzon, L.M.; Powers, J.M. Fracture Resistance of Re-Attached Coronal Fragments—Influence of Different Adhesive Materials and Bevel Preparation. Dent. Traumatol. 2004, 20, 157–163. [Google Scholar] [CrossRef]
- Poubel, D.L.N.; Almeida, J.C.F.; Dias Ribeiro, A.P.; Maia, G.B.; Martinez, J.M.G.; Garcia, F.C.P. Effect of Dehydration and Rehydration Intervals on Fracture Resistance of Reattached Tooth Fragments Using a Multimode Adhesive. Dent. Traumatol. 2017, 33, 451–457. [Google Scholar] [CrossRef] [PubMed]
- Garcia, F.C.P.; Poubel, D.L.N.; Almeida, J.C.F.; Toledo, I.P.; Poi, W.R.; Guerra, E.N.S.; Rezende, L.V.M.L. Tooth Fragment Reattachment Techniques—A Systematic Review. Dent. Traumatol. 2018, 34, 135–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruschi-Alonso, R.C.; Alonso, R.C.B.; Correr, G.M.; Alves, M.C.; Lewgoy, H.R.; Sinhoreti, M.A.C.; Puppin-Rontani, R.M.; Correr-Sobrinho, L. Reattachment of Anterior Fractured Teeth: Effect of Materials and Techniques on Impact Strength. Dent. Traumatol. 2010, 26, 315–322. [Google Scholar] [CrossRef]
- Chazine, M.; Sedda, M.; Ounsi, H.F.; Paragliola, R.; Ferrari, M.; Grandini, S. Evaluation of the Fracture Resistance of Reattached Incisal Fragments Using Different Materials and Techniques. Dent. Traumatol. 2011, 27, 15–18. [Google Scholar] [CrossRef] [PubMed]
- Reis, A.; Francci, C.; Loguercio, A.D.; Carrilho, M.R.; Rodriques Filho, L.E. Re-Attachment of Anterior Fractured Teeth: Fracture Strength Using Different Techniques. Oper. Dent. 2001, 26, 287–294. [Google Scholar]
- Kang, H.; Chae, Y.; Lee, K.; Lee, H.; Choi, S.; Nam, O. Long-Term Outcome of Reattached Tooth Fragment in Permanent Anterior Teeth of Children and Adolescents. J. Korean Acad Pediatr. Dent. 2021, 48, 42–49. [Google Scholar] [CrossRef]
- Patni, P.; Jain, D.; Goel, G. A Holistic Approach to Management of Fractured Teeth Fragments: A Case Report. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2010, 109, e70–e74. [Google Scholar] [CrossRef]
- Sulwińska, M.; Szczesio, A.; Bołtacz-Rzepkowska, E. Bond Strength of a Resin Composite to MTA at Various Time Intervals and with Different Adhesive Strategies. Dent. Med. Probl. 2017, 54, 155–160. [Google Scholar] [CrossRef]
- Tunç, E.Ş.; Bayrak, Ş.; Eğilmez, T. The Evaluation of Bond Strength of a Composite and a Compomer to White Mineral Trioxide Aggregate with Two Different Bonding Systems. J. Endod. 2008, 34, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Bayrak, S.; Tunç, E.S.; Saroglu, I.; Egilmez, T. Shear Bond Strengths of Different Adhesive Systems to White Mineral Trioxide Aggregate. Dent. Mater. J. 2009, 28, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Krawczyk-Stuss, M.; Nowak, J.; Bołtacz-Rzepkowska, E. Bond Strength of Biodentine to a Resin-Based Composite at Various Acid Etching Times and with Different Adhesive Strategies. Dent. Med. Probl. 2019, 56, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Odabaş, M.E.; Bani, M.; Tirali, R.E. Shear Bond Strengths of Different Adhesive Systems to Biodentine. Sci. World J. 2013, 2013, 626103. [Google Scholar] [CrossRef]
- Hardan, L.; Mancino, D.; Bourgi, R.; Alvarado-Orozco, A.; Rodríguez-Vilchis, L.E.; Flores-Ledesma, A.; Cuevas-Suárez, C.E.; Lukomska-Szymanska, M.; Eid, A.; Danhache, M.-L.; et al. Bond Strength of Adhesive Systems to Calcium Silicate-Based Materials: A Systematic Review and Meta-Analysis of In Vitro Studies. Gels 2022, 8, 311. [Google Scholar] [CrossRef]
- Carretero, V.; Giner-Tarrida, L.; Peñate, L.; Arregui, M. Shear Bond Strength of Nanohybrid Composite to Biodentine with Three Different Adhesives. Coatings 2019, 9, 783. [Google Scholar] [CrossRef]
- Lopes, L.C.P.; Terada, R.S.S.; Tsuzuki, F.M.; Giannini, M.; Hirata, R. Heating and Preheating of Dental Restorative Materials-a Systematic Review. Clin. Oral Investig. 2020, 24, 4225–4235. [Google Scholar] [CrossRef]
- Sawai, M.A.; Bhardwaj, A.; Jafri, Z.; Sultan, N.; Daing, A. Tooth Polishing: The Current Status. J. Indian Soc. Periodontol. 2015, 19, 375–380. [Google Scholar] [CrossRef]
- Hecova, H.; Tzigkounakis, V.; Merglova, V.; Netolicky, J. A Retrospective Study of 889 Injured Permanent Teeth. Dent. Traumatol. Off. Publ. Int. Assoc. Dent. Traumatol. 2010, 26, 466–475. [Google Scholar] [CrossRef]
- Wang, G.; Wang, C.; Qin, M. Pulp Prognosis Following Conservative Pulp Treatment in Teeth with Complicated Crown Fractures-A Retrospective Study. Dent. Traumatol. Off. Publ. Int. Assoc. Dent. Traumatol. 2017, 33, 255–260. [Google Scholar] [CrossRef]
- Krastl, G.; Weiger, R. Vital Pulp Therapy after Trauma. Endod. Pract. Today 2014, 8, 293–300. [Google Scholar]
- Linsuwanont, P.; Wimonsutthikul, K.; Pothimoke, U.; Santiwong, B. Treatment Outcomes of Mineral Trioxide Aggregate Pulpotomy in Vital Permanent Teeth with Carious Pulp Exposure: The Retrospective Study. J. Endod. 2017, 43, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Taha, N.A.; Ahmad, M.B.; Ghanim, A. Assessment of Mineral Trioxide Aggregate Pulpotomy in Mature Permanent Teeth with Carious Exposures. Int. Endod. J. 2017, 50, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Qudeimat, M.A.; Alyahya, A.; Hasan, A.A. Mineral Trioxide Aggregate Pulpotomy for Permanent Molars with Clinical Signs Indicative of Irreversible Pulpitis: A Preliminary Study. Int. Endod. J. 2017, 50, 126–134. [Google Scholar] [CrossRef] [PubMed]
- Taha, N.A.; Khazali, M.A. Partial Pulpotomy in Mature Permanent Teeth with Clinical Signs Indicative of Irreversible Pulpitis: A Randomized Clinical Trial. J. Endod. 2017, 43, 1417–1421. [Google Scholar] [CrossRef]
- Martos, J.; Koller, C.D.; Silveira, L.F.M.; Cesar-Neto, J.B. Crown Fragment Reattachment in Anterior-Fractured Tooth: A Five-Year Follow-Up. Eur. J. Gen. Dent. 2012, 1, 112–115. [Google Scholar] [CrossRef]
- de Lima, M.D.; Martins, J.F.; de Moura, M.S.; de Area Leao, V.L.; de Deus, L.D.F.A.; Moura, D.D.S. Reattachment of Fractured Fragment of an Anterior Tooth: Case Report and Nine-Year Follow-Up. Gen. Dent. 2011, 59, e192–e195. [Google Scholar]
- Scribante, A.; Dermenaki Farahani, M.R.; Marino, G.; Matera, C.; Rodriguez y Baena, R.; Lanteri, V.; Butera, A. Biomimetic Effect of Nano-Hydroxyapatite in Demineralized Enamel before Orthodontic Bonding of Brackets and Attachments: Visual, Adhesion Strength, and Hardness in In Vitro Tests. Biomed Res. Int. 2020, 2020, 6747498. [Google Scholar] [CrossRef]
- Butera, A.; Gallo, S.; Pascadopoli, M.; Montasser, M.A.; Abd El Latief, M.H.; Modica, G.G.; Scribante, A. Home Oral Care with Biomimetic Hydroxyapatite vs. Conventional Fluoridated Toothpaste for the Remineralization and Desensitizing of White Spot Lesions: Randomized Clinical Trial. Int. J. Environ. Res. Public Health 2022, 19, 8676. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Vital Pulp Therapy (VPT) Intervention | Description of the Method | Indication |
|---|---|---|
| Direct pulp capping (DPC) | (1) Placement of protective pulp capping material directly over the exposure | A recent and pinpoint-sized exposed vital pulp |
| Partial pulpotomy (PP) | (1) Partial removal of the coronal pulp; (2) Hemostasis; (3) Placement of a pulp capping material. | Pulp exposure treated within 14 days after trauma, caries-free, open apex or thin dentinal walls, and vital and asymptomatic pulp |
| Full (complete) pulpotomy (CP) | (1) Removal of the entire coronal pulp to the level of canal orifices; (2) Hemostasis; (3) Placement of a pulp capping material. | More than 2 week lapse between trauma and treatment, extensive pulp exposure |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Radwanski, M.; Caporossi, C.; Lukomska-Szymanska, M.; Luzi, A.; Sauro, S. Complicated Crown Fracture of Permanent Incisors: A Conservative Treatment Case Report and a Narrative Review. Bioengineering 2022, 9, 481. https://doi.org/10.3390/bioengineering9090481
Radwanski M, Caporossi C, Lukomska-Szymanska M, Luzi A, Sauro S. Complicated Crown Fracture of Permanent Incisors: A Conservative Treatment Case Report and a Narrative Review. Bioengineering. 2022; 9(9):481. https://doi.org/10.3390/bioengineering9090481
Chicago/Turabian StyleRadwanski, Mateusz, Corrado Caporossi, Monika Lukomska-Szymanska, Arlinda Luzi, and Salvatore Sauro. 2022. "Complicated Crown Fracture of Permanent Incisors: A Conservative Treatment Case Report and a Narrative Review" Bioengineering 9, no. 9: 481. https://doi.org/10.3390/bioengineering9090481