
A New Mathematical Numerical Model to Evaluate the Risk of Thrombosis in Three Clinical Ventricular Assist Devices




Abstract
:1. Introduction
2. Materials and Methods
2.1. Studied VADs and Geometries
2.2. Residence Time and Non-physiological Shear Stress
2.3. Activated Platelets and Thrombotic Clots Risk
2.3.1. Resting Platelets, Activated Platelets and Coagulant Factors
2.3.2. Thrombotic Clots and Thrombosis Obstruct Flow
2.3.3. Thresholds and Initialization
2.4. CFD Methods
2.5. Mesh Details and Sensitivity Analysis
2.6. Rotor Position Independent Verification
3. Results
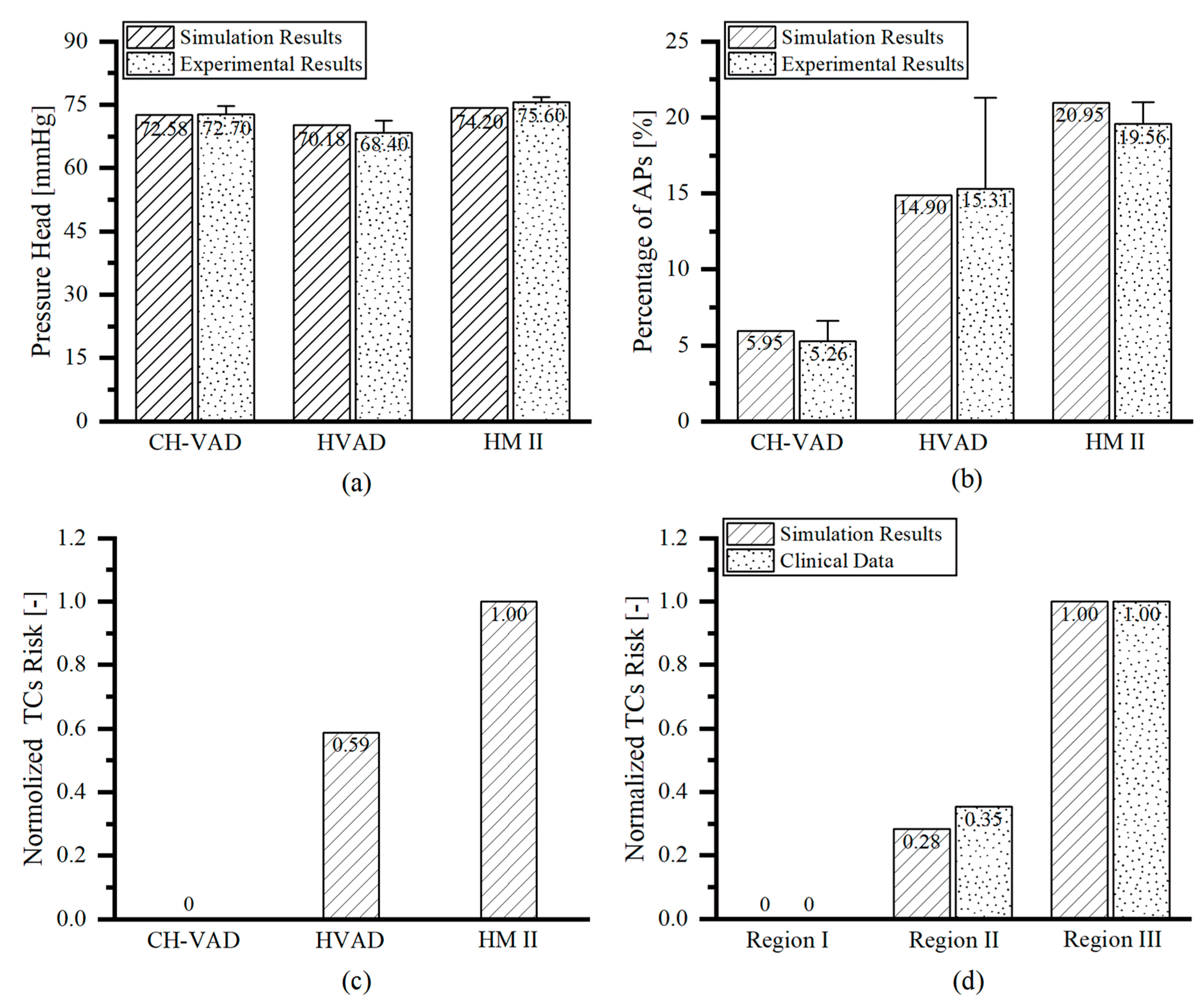
3.1. Hemodynamic Results and Simulation Results Validation
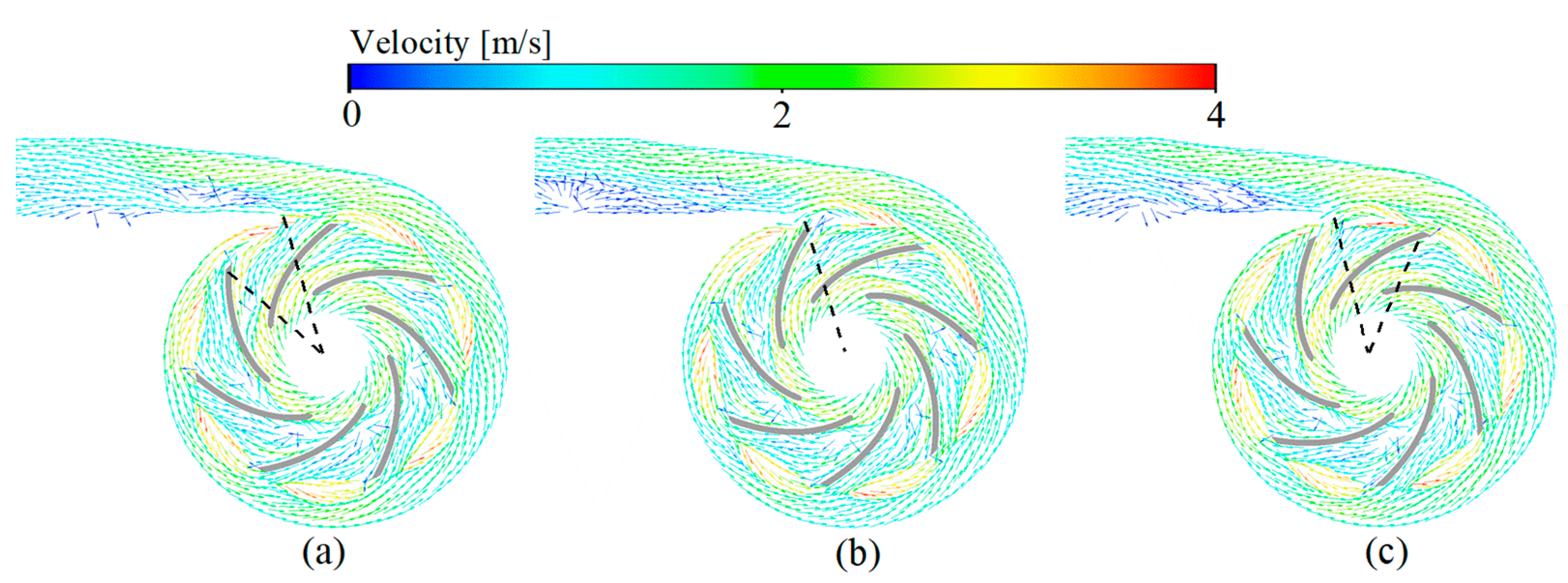
3.2. Velocity Fields
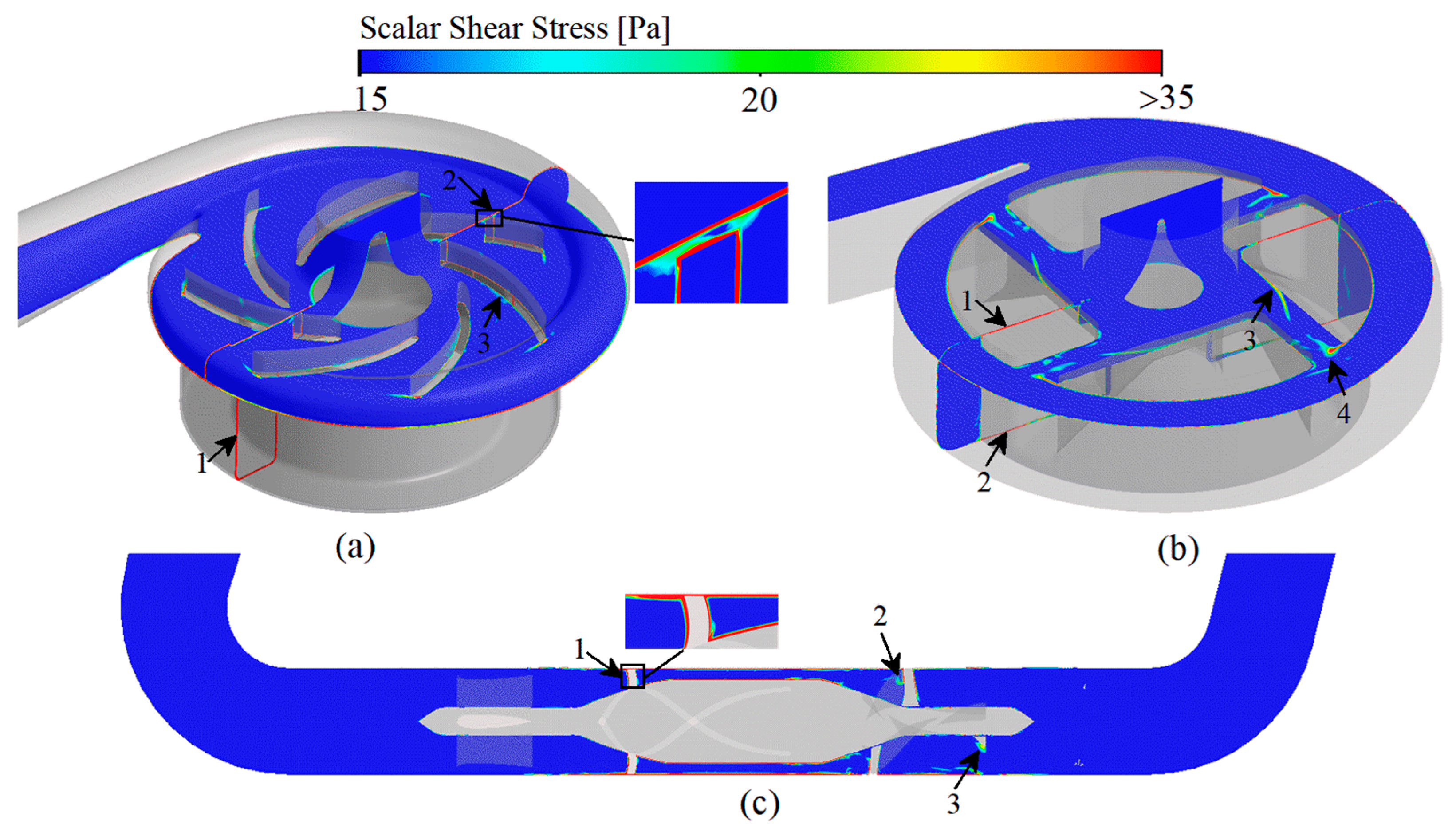
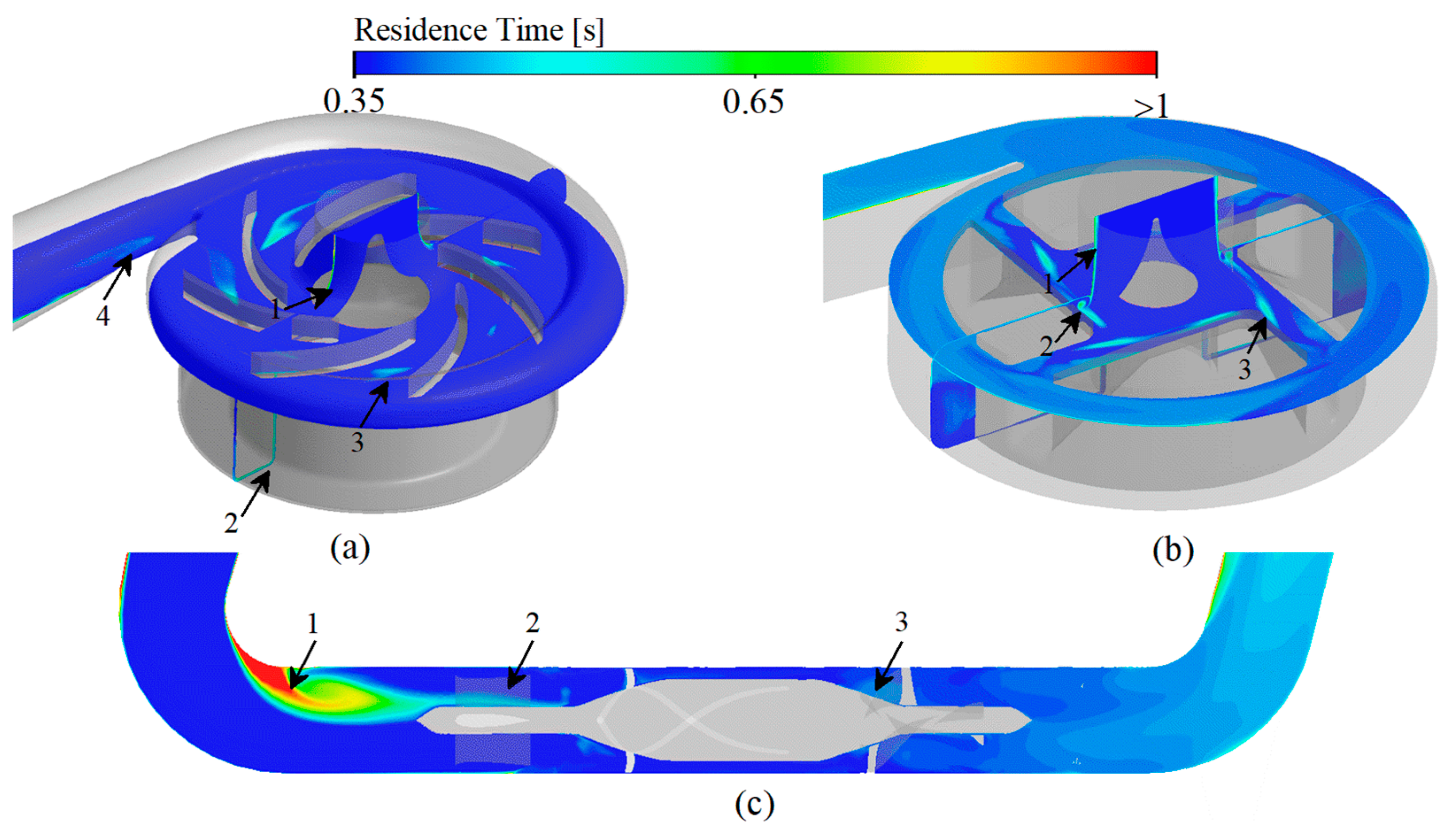
3.3. Scalar Shear Stress and Residence Time
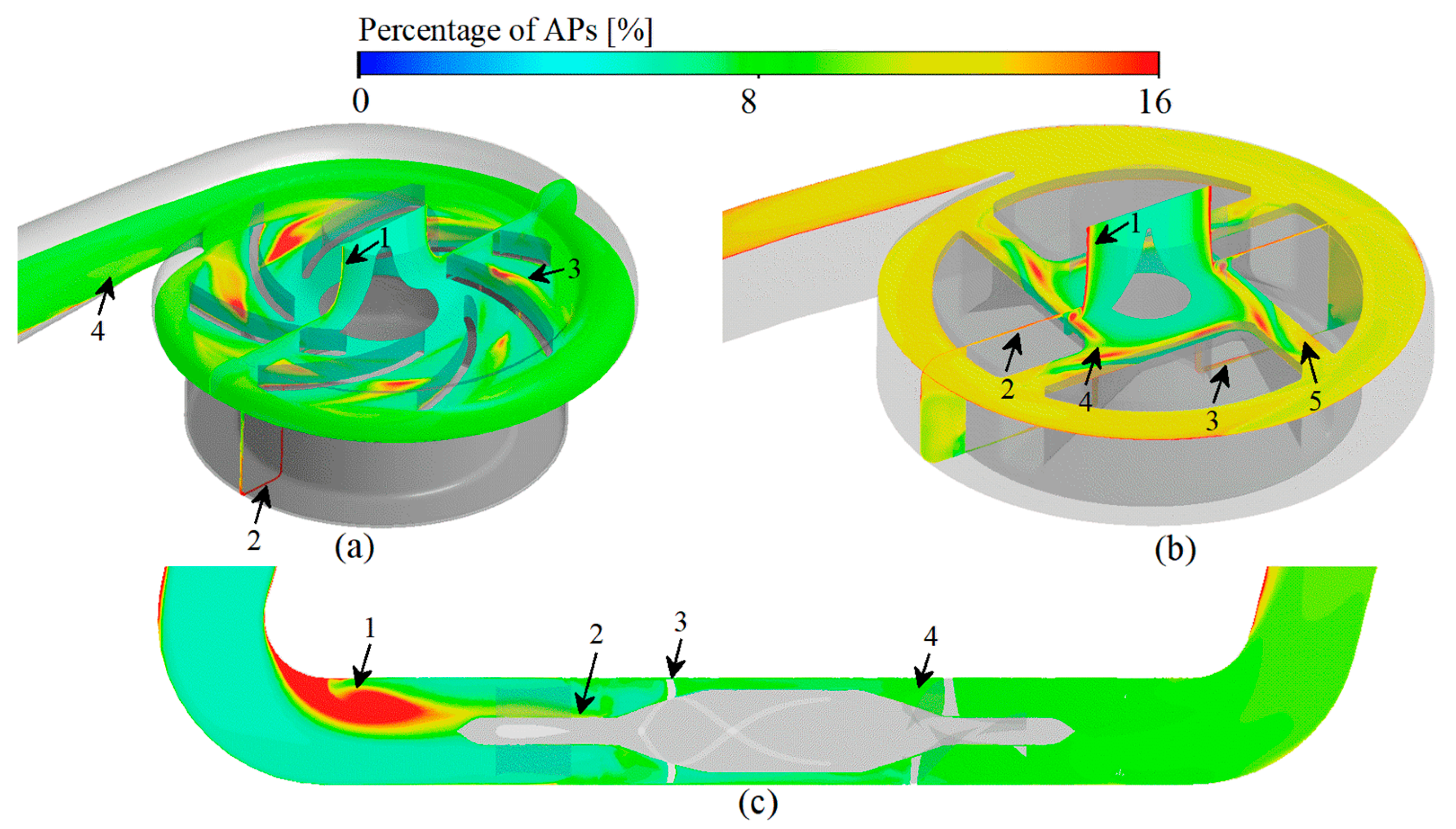
3.4. Platelet Activation Assessment
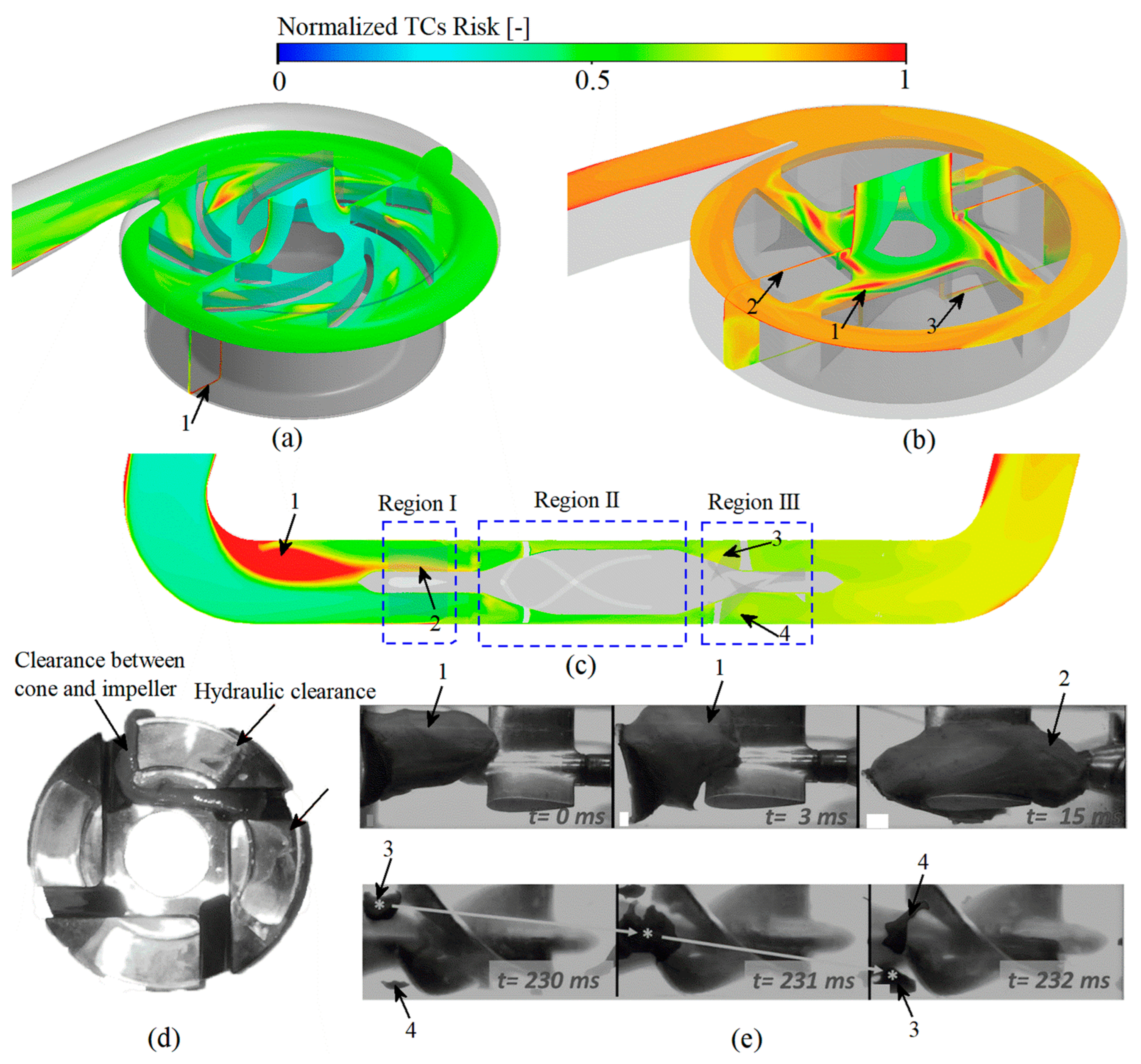
3.5. Thrombosis Risk Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Uriel, N.; Han, J.; Morrison, K.A.; Nahumi, N.; Yuzefpolskaya, M.; Garan, A.R.; Duong, J.; Colombo, P.C.; Takayama, H.; Thomas, S.; et al. Device thrombosis in HeartMate II continuous-flow left ventricular assist devices: A multifactorial phenomenon. J. Hear. Lung Transplant. 2014, 33, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Starling, R.C.; Moazami, N.; Silvestry, S.C.; Ewald, G.; Rogers, J.G.; Milano, C.A.; Rame, J.E.; Acker, M.A.; Blackstone, E.H.; Ehrlinger, J.; et al. Unexpected Abrupt Increase in Left Ventricular Assist Device Thrombosis. N. Engl. J. Med. 2014, 370, 33–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Najjar, S.S.; Slaughter, M.S.; Pagani, F.D.; Starling, R.C.; McGee, E.C.; Eckman, P.; Tatooles, A.J.; Moazami, N.; Kormos, R.L.; Hathaway, D.R.; et al. An analysis of pump thrombus events in patients in the HeartWare ADVANCE bridge to trans-plant and continued access protocol trial. J. Heart Lung Transpl. 2014, 33, 23–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schalit, I.; Espinoza, A.; Pettersen, F.J.; Thiara, A.P.; Karlsen, H.; Sørensen, G.; Fosse, E.; Fiane, A.E.; Fiane, A.E. Accelerometer Detects Pump Thrombosis and Thromboembolic Events in an In vitro HVAD Cir-cuit. ASAIO J. 2018, 64, 601–609. [Google Scholar] [CrossRef] [PubMed]
- Aaronson, K.D.; Slaughter, M.S.; Miller, L.W.; McGee, E.C.; Cotts, W.G.; Acker, M.A.; Jessup, M.L.; Gregoric, I.D.; Loyalka, P.; Frazier, O.H.; et al. Use of an Intrapericardial, Continuous-Flow, Centrifugal Pump in Patients Awaiting Heart Transplantation. Circulation 2012, 125, 3191–3200. [Google Scholar] [CrossRef] [Green Version]
- Para, A.; Bark, D.; Lin, A.; Ku, D. Rapid Platelet Accumulation Leading to Thrombotic Occlusion. Ann. Biomed. Eng. 2011, 39, 1961–1971. [Google Scholar] [CrossRef]
- Chen, Z.; Mondal, N.; Ding, J.; Koenig, S.C.; Slaughter, M.S.; Wu, Z.J. Paradoxical Effect of Nonphysiological Shear Stress on Platelets and von Willebrand Factor. Artif. Organs 2016, 40, 659–668. [Google Scholar] [CrossRef] [Green Version]
- Holme, P.A.; Ørvim, U.; Hamers, M.J.A.G.; Solum, N.O.; Brosstad, F.R.; Barstad, R.M.; Sakariassen, K.S. Shear-Induced Platelet Activation and Platelet Microparticle Formation at Blood Flow Conditions as in Arteries with a Severe Stenosis. Arter. Thromb. Vasc. Biol. 1997, 17, 646–653. [Google Scholar] [CrossRef]
- Chen, Z.; Mondal, N.K.; Ding, J.; Koenig, S.C.; Slaughter, M.S.; Griffith, B.P.; Wu, Z.J. Activation and shedding of platelet glycoprotein IIb/IIIa under non-physiological shear stress. Mol. Cell. Biochem. 2015, 409, 93–101. [Google Scholar] [CrossRef] [Green Version]
- Balasubramanian, V.; Slack, S.M. Effects of Fibrinogen Residence Time and Shear Rate on the Morphology and Procoagulant Activity of Human Platelets Adherent to Polymeric Biomaterials. ASAIO J. 2001, 47, 354–360. [Google Scholar] [CrossRef]
- Ding, J.; Chen, Z.; Niu, S.; Zhang, J.; Mondal, N.K.; Griffith, B.P.; Wu, Z.J. Quantification of Shear-Induced Platelet Activation: High Shear Stresses for Short Exposure Time. Artif. Organs 2015, 39, 576–583. [Google Scholar] [CrossRef] [PubMed]
- Brown, C.H.; Leverett, L.B.; Lewis, C.W.; Alfrey, C.P.; Hellums, J.D. Morphological, biochemical, and functional changes in human platelets subjected to shear stress. J. Lab. Clin. Med. 1975, 86, 462–671. [Google Scholar] [PubMed]
- Rayz, V.L.; Boussel, L.; Ge, L.; Leach, J.R.; Martin, A.J.; Lawton, M.T.; McCulloch, C.; Saloner, D. Flow Residence Time and Regions of Intraluminal Thrombus Deposition in Intracranial Aneurysms. Ann. Biomed. Eng. 2010, 38, 3058–3069. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delgado-Montero, A.; Martinez-Legazpi, P.; Desco, M.M.; Rodríguez-Pérez, D.; Díaz-Otero, F.; Rossini, L.; del Villar, C.P.; Rodríguez-González, E.; Chazo, C.; Benito, Y.; et al. Blood Stasis Imaging Predicts Cerebral Microembolism during Acute Myocardial Infarction. J. Am. Soc. Echocardiogr. 2020, 33, 389–398. [Google Scholar] [CrossRef] [PubMed]
- Blum, C.; Groß-Hardt, S.; Steinseifer, U.; Neidlin, M. An Accelerated Thrombosis Model for Computational Fluid Dynamics Simulations in Rotary Blood Pumps. Cardiovasc. Eng. Technol. 2022, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Marom, G.; Bluestein, D. Lagrangian methods for blood damage estimation in cardiovascular devices—How numerical implementation affects the results. Expert Rev. Med. Devices 2016, 13, 113–122. [Google Scholar] [CrossRef] [Green Version]
- Yin, W.; Alemu, Y.; Affeld, K.; Jesty, J.; Bluestein, D. Flow-induced platelet activation in bileaflet and monoleaflet mechanical heart valves. Ann. Biomed. Eng. 2004, 32, 1058–1066. [Google Scholar] [CrossRef] [Green Version]
- Bluestein, D.; Chandran, K.B.; Manning, K.B. Towards Non-thrombogenic Performance of Blood Recirculating Devices. Ann. Biomed. Eng. 2010, 38, 1236–1256. [Google Scholar] [CrossRef]
- Wu, J.; Yun, B.M.; Fallon, A.M.; Hanson, S.R.; Aidun, C.K.; Yoganathan, A.P. Numerical Investigation of the Effects of Channel Geometry on Platelet Activation and Blood Damage. Ann. Biomed. Eng. 2011, 39, 897–910. [Google Scholar] [CrossRef] [Green Version]
- Chivukula, V.K.; Beckman, J.A.; Prisco, A.R.; Lin, S.; Dardas, T.F.; Cheng, R.; Farris, S.D.; Smith, J.W.; Mokadam, N.A.; Mahr, C.; et al. Small Left Ventricular Size Is an Independent Risk Factor for Ventricular Assist Device Thrombosis. ASAIO J. 2019, 65, 152–159. [Google Scholar] [CrossRef]
- Fiusco, F.; Broman, L.M.; Prahl Wittberg, L. Blood Pumps for Extracorporeal Membrane Oxygenation: Plate-let Activation During Different Operating Conditions. ASAIO J. 2022, 68, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Dai, W.F.; Wu, P.; Liu, G.M. A two-phase flow approach for modeling blood stasis and estimating the throm-bosis potential of a ventricular assist device. Int. J. Artif. Organs 2021, 44, 471–480. [Google Scholar] [CrossRef] [PubMed]
- Liao, S.; Wu, E.; Neidlin, M.; Li, Z.-Y.; Simpson, B.; Gregory, S. The Influence of Rotary Blood Pump Speed Modulation on the Risk of Intraventricular Thrombosis. Artif. Organs 2018, 42, 943–953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, J.; Chen, Z.; Griffith, B.P.; Wu, Z.J. Computational characterization of flow and blood damage potential of the new maglev CH-VAD pump versus the HVAD and HeartMate II pumps. Int. J. Artif. Organs 2020, 43, 653–662. [Google Scholar] [CrossRef] [PubMed]
- Prisco, A.R.; Aliseda, A.; Beckman, J.A.; Mokadam, N.A.; Mahr, C.; Garcia, G.J.M. Impact of LVAD Implantation Site on Ventricular Blood Stagnation. ASAIO J. 2017, 63, 392–400. [Google Scholar] [CrossRef]
- Berk, Z.B.K.; Zhang, J.; Chen, Z.; Tran, D.; Griffith, B.P.; Wu, Z.J. Evaluation of in vitro hemolysis and platelet activation of a newly developed maglev LVAD and two clinically used LVADs with human blood. Artif. Organs 2019, 43, 870–879. [Google Scholar] [CrossRef]
- Menichini, C.; Xu, X.Y. Mathematical modeling of thrombus formation in idealized models of aortic dissection: Initial findings and potential applications. J. Math. Biol. 2016, 73, 1205–1226. [Google Scholar] [CrossRef] [Green Version]
- Taylor, J.O.; Meyer, R.S.; Deutsch, S.; Manning, K.B. Development of a computational model for macroscopic predictions of device-induced throm-bosis. Biomech. Model Mechanobiol. 2016, 15, 1713–1731. [Google Scholar] [CrossRef]
- Wu, W.-T.; Jamiolkowski, M.A.; Wagner, W.; Aubry, N.; Massoudi, M.; Antaki, J.F. Multi-Constituent Simulation of Thrombus Deposition. Sci. Rep. 2017, 7, srep42720. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Smith, P.A.; Handy, K.M.; Conger, J.L.; Spangler, T.; Lin, F.; Chen, C.; Costas, G.; Elgalad, A.; Sampaio, L.C. In vivo Hemodynamic Evaluation of an Implantable Left Ventricular Assist Device in a Long-term Anti-coagulation Regimen. In Proceedings of the 2020 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Montreal, QC, Canada, 20–24 July 2020; IEEE: New York, NY, USA, 2020; pp. 2589–2593. [Google Scholar] [CrossRef]
- Wu, Z.; Antaki, J.F.; Burgreen, G.W.; Butler, K.C.; Thomas, D.C.; Griffith, B.P. Fluid Dynamic Characterization of Operating Conditions for Continuous Flow Blood Pumps. ASAIO J. 1999, 45, 442–449. [Google Scholar] [CrossRef]
- Taskin, M.E.; Fraser, K.H.; Zhang, T.; Wu, C.; Griffith, B.P.; Wu, Z.J. Evaluation of Eulerian and Lagrangian Models for Hemolysis Estimation. ASAIO J. 2012, 58, 363–372. [Google Scholar] [CrossRef] [PubMed]
- Arvand, A.; Hormes, M.; Reul, H. A Validated Computational Fluid Dynamics Model to Estimate Hemolysis in a Rotary Blood Pump. Artif. Organs 2005, 29, 531–540. [Google Scholar] [CrossRef] [PubMed]
- Ge, L.; Dasi, L.P.; Sotiropoulos, F.; Yoganathan, A.P. Characterization of Hemodynamic Forces Induced by Mechanical Heart Valves: Reynolds vs. Viscous Stresses. Ann. Biomed. Eng. 2008, 36, 276–297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiegmann, L.; Boës, S.; de Zélicourt, D.; Thamsen, B.; Daners, M.S.; Meboldt, M.; Kurtcuoglu, V. Blood Pump Design Variations and Their Influence on Hydraulic Performance and Indicators of Hemocompatibility. Ann. Biomed. Eng. 2017, 46, 417–428. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Chen, Z.; Zhang, J.; Zhang, X.; Wu, Z.J. Modeling Clot Formation of Shear-Injured Platelets in Flow by a Dissipative Particle Dynamics Method. Bull. Math. Biol. 2020, 82, 1–20. [Google Scholar] [CrossRef]
- Page, T.C.; Light, W.R.; Hellums, J.D. Prediction of microcirculatory oxygen transport by erythro-cyte/hemoglobin solution mixtures. Microvasc Res. 1998, 56, 113–126. [Google Scholar] [CrossRef]
- Menichini, C.; Cheng, Z.; Gibbs, R.G.J.; Xu, X.Y. Predicting false lumen thrombosis in patient-specific models of aortic dissection. J. R. Soc. Interface 2016, 13, 20160759. [Google Scholar] [CrossRef] [Green Version]
- Leiderman, K.; Fogelson, A.L. Grow with the flow: A spatial-temporal model of platelet deposition and blood coagulation under flow. Math. Med. Biol. A J. IMA 2011, 28, 47–84. [Google Scholar] [CrossRef] [Green Version]
- Goodman, P.D.; Barlow, E.T.; Crapo, P.M.; Mohammad, S.F.; Solen, K.A. Computational Model of Device-Induced Thrombosis and Thromboembolism. Ann. Biomed. Eng. 2005, 33, 780–797. [Google Scholar] [CrossRef]
- Chen, Z.; Jena, S.K.; Giridharan, G.A.; Koenig, S.C.; Slaughter, M.S.; Griffith, B.P.; Wu, Z.J. Flow features and device-induced blood trauma in CF-VADs under a pulsatile blood flow condition: A CFD comparative study. Int. J. Numer. Methods Biomed. Eng. 2018, 34, e2924. [Google Scholar] [CrossRef]
- Fraser, K.; Zhang, T.; Taskin, M.E.; Griffith, B.P.; Wu, Z.J. A Quantitative Comparison of Mechanical Blood Damage Parameters in Rotary Ventricular Assist Devices: Shear Stress, Exposure Time and Hemolysis Index. J. Biomech. Eng. 2012, 134, 081002–08100211. [Google Scholar] [CrossRef] [PubMed]
- Hellums, J.D. 1993 Whitaker lecture: Biorheology in thrombosis research. Ann. Biomed. Eng. 1994, 22, 445–455. [Google Scholar] [CrossRef] [PubMed]
- Wurzinger, L.J.; Opitz, R.; Blasberg, P.; Schmid-Schönbein, H. Platelet and coagulation parameters following millisecond exposure to laminar shear stress. Thromb. Haemost. 1985, 54, 381–386. [Google Scholar] [CrossRef]
- Sakariassen, K.S.; Holme, P.A.; Ørvim, U.; Barstad, R.M.; Solum, N.O.; Brosstad, F.R. Shear-induced platelet activation and platelet microparticle formation in native human blood. Thromb. Res. 1998, 92, S33–S41. [Google Scholar] [CrossRef]
- Jian-ning, Z.; Bergeron, A.L.; Yu, Q.; Sun, C.; McBride, L.; Bray, P.F.; Dong, J.F. Duration of exposure to high fluid shear stress is critical in shear-induced platelet activation-aggregation. Thromb. Haemost. 2003, 90, 672–678. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colantuoni, G.; Heliums, J.D.; Moake, J.L.; Alfrey, C.P. THE RESPONSE OF HUMAN PLATELETS TO SHEAR STRESS AT SHORT EXPOSURE TIMES. ASAIO J. 1977, 23, 626–630. [Google Scholar] [CrossRef] [PubMed]
- Chivukula, V.K.; Beckman, J.A.; Li, S.; Masri, S.C.; Levy, W.C.; Lin, S.; Cheng, R.K.; Farris, S.D.; Wood, G.; Dardas, T.F.; et al. Left Ventricular Assist Device Inflow Cannula Insertion Depth Influences Thrombosis Risk. ASAIO J. 2020, 66, 766–773. [Google Scholar] [CrossRef]
- Chivukula, V.K.; Beckman, J.A.; Prisco, A.R.; Dardas, T.; Lin, S.; Smith, J.W.; Mokadam, N.A.; Aliseda, A.; Mahr, C. Left Ventricular Assist Device Inflow Cannula Angle and Thrombosis Risk. Circ. Hear. Fail. 2018, 11, e004325. [Google Scholar] [CrossRef]
- Zhang, J.; Koert, A.; Gellman, B.; Gempp, T.M.; Dasse, K.A.; Gilbert, R.J.; Griffith, B.P.; Wu, Z.J. Optimization of a Miniature Maglev Ventricular Assist Device for Pediatric Circulatory Support. ASAIO J. 2007, 53, 23–31. [Google Scholar] [CrossRef]
- Zhang, J.; Gellman, B.; Koert, A.; Dasse, K.A.; Gilbert, R.J.; Griffith, B.P.; Wu, Z.J. Computational and Experimental Evaluation of the Fluid Dynamics and Hemocompatibility of the CentriMag Blood Pump. Artif. Organs 2006, 30, 168–177. [Google Scholar] [CrossRef]
- Berg, N.; Fuchs, L.; Wittberg, L.P. Flow Characteristics and Coherent Structures in a Centrifugal Blood Pump. Flow Turbul. Combust. 2018, 102, 469–483. [Google Scholar] [CrossRef] [Green Version]
- Rowlands, G.W.; Pagani, F.D.; Antaki, J.F. Classification of the Frequency, Severity, and Propagation of Thrombi in the HeartMate II Left Ventricular Assist Device. ASAIO J. 2020, 66, 992–999. [Google Scholar] [CrossRef] [PubMed]
- Xenos, M.; Girdhar, G.; Alemu, Y.; Jesty, J.; Slepian, M.; Einav, S.; Bluestein, D. Device Thrombogenicity Emulator (DTE)—Design optimization methodology for cardiovascular devices: A study in two bileaflet MHV designs. J. Biomech. 2010, 43, 2400–2409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rowlands, G.W.; Antaki, J.F. High-speed visualization of ingested, ejected, adherent, and disintegrated thrombus in contemporary ventricular assist devices. Artif. Organs 2020, 44, E459–E469. [Google Scholar] [CrossRef]
- Chen, Z.; Zhang, J.; Li, T.; Tran, D.; Griffith, B.P.; Wu, Z.J. The impact of shear stress on device-induced platelet hemostatic dysfunction relevant to thrombosis and bleeding in mechanically assisted circulation. Artif. Organs 2019, 44, E201–E213. [Google Scholar] [CrossRef]
- Chen, Z.; Mondal, N.; Zheng, S.; Koenig, S.C.; Slaughter, M.S.; Griffith, B.P.; Wu, Z.J. High shear induces platelet dysfunction leading to enhanced thrombotic propensity and diminished hemostatic capacity. Platelets 2017, 30, 112–119. [Google Scholar] [CrossRef]
- Andrews, R.K.; Berndt, M.C. Platelet physiology and thrombosis. Thromb. Res. 2004, 114, 447–453. [Google Scholar] [CrossRef]
- Boraschi, A.; Bozzi, S.; Thamsen, B.; Granegger, M.; Wiegmann, L.; Pappalardo, F.; Slepian, M.J.; Kurtcuoglu, V.; Redaelli, A.; De Zélicourt, D.; et al. Thrombotic Risk of Rotor Speed Modulation Regimes of Contemporary Centrifugal Continuous-flow Left Ventricular Assist Devices. ASAIO J. 2021, 67, 737–745. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, Y.; Wang, H.; Xi, Y.; Sun, A.; Deng, X.; Chen, Z.; Fan, Y. A New Mathematical Numerical Model to Evaluate the Risk of Thrombosis in Three Clinical Ventricular Assist Devices. Bioengineering 2022, 9, 235. https://doi.org/10.3390/bioengineering9060235
Li Y, Wang H, Xi Y, Sun A, Deng X, Chen Z, Fan Y. A New Mathematical Numerical Model to Evaluate the Risk of Thrombosis in Three Clinical Ventricular Assist Devices. Bioengineering. 2022; 9(6):235. https://doi.org/10.3390/bioengineering9060235
Chicago/Turabian StyleLi, Yuan, Hongyu Wang, Yifeng Xi, Anqiang Sun, Xiaoyan Deng, Zengsheng Chen, and Yubo Fan. 2022. "A New Mathematical Numerical Model to Evaluate the Risk of Thrombosis in Three Clinical Ventricular Assist Devices" Bioengineering 9, no. 6: 235. https://doi.org/10.3390/bioengineering9060235