
Altered Microcirculation in Alzheimer’s Disease Assessed by Machine Learning Applied to Functional Thermal Imaging Data
 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
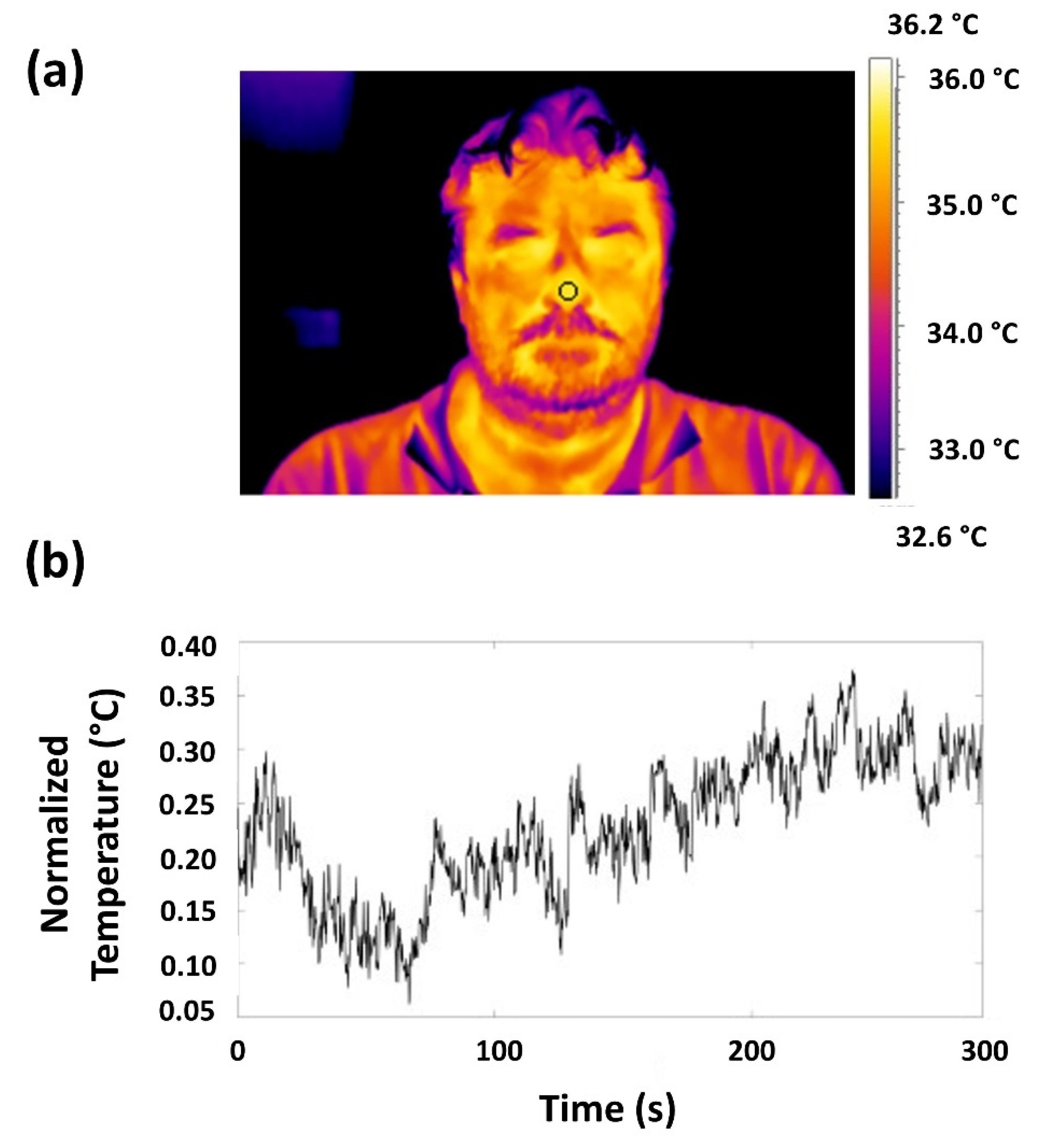
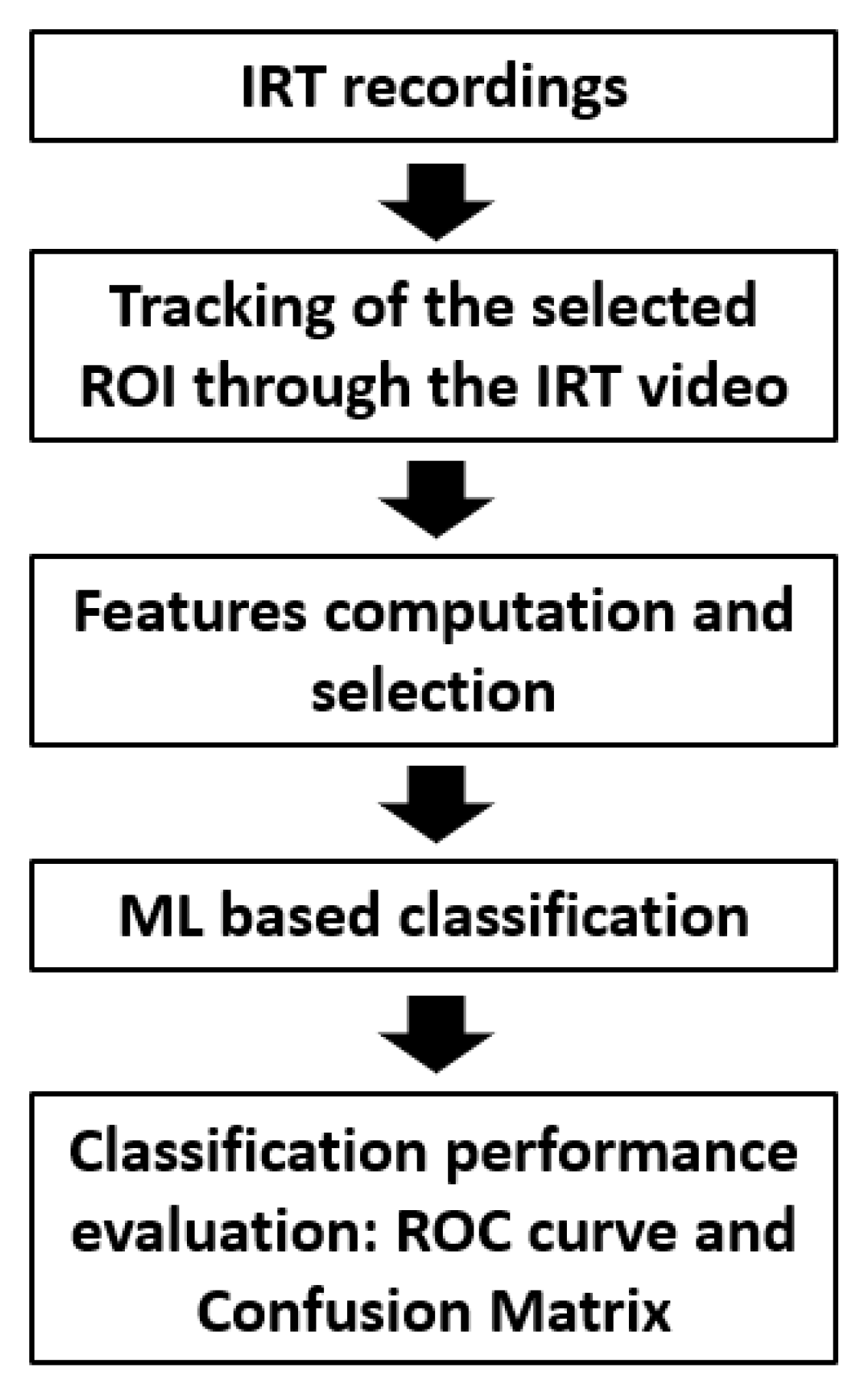
2.2. IRT Instrumentation and Thermal Signals Data Analysis
2.3. Multivariate Data-Driven Analysis and Statistical Inference
3. Results
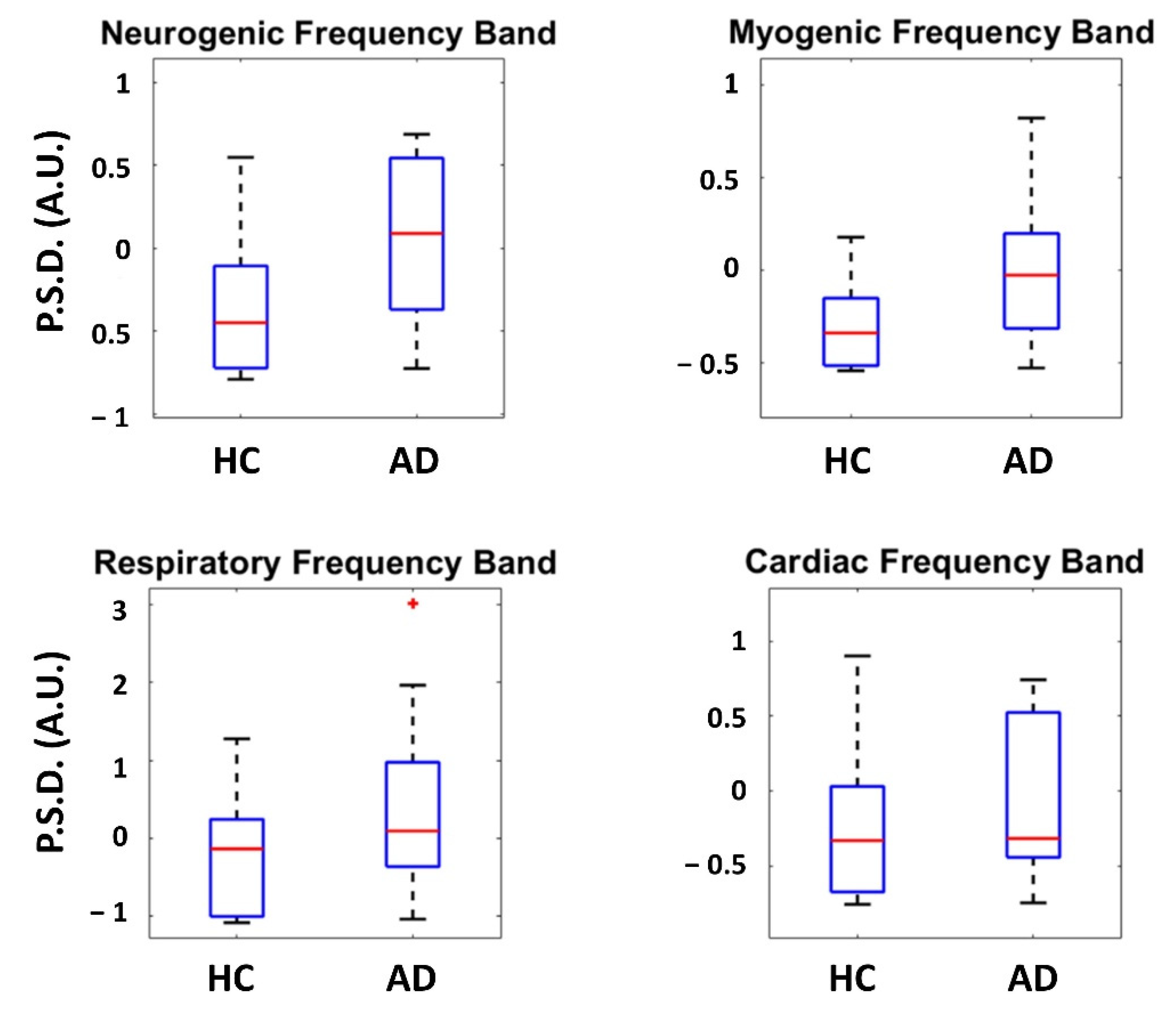
3.1. Inferential Statistics
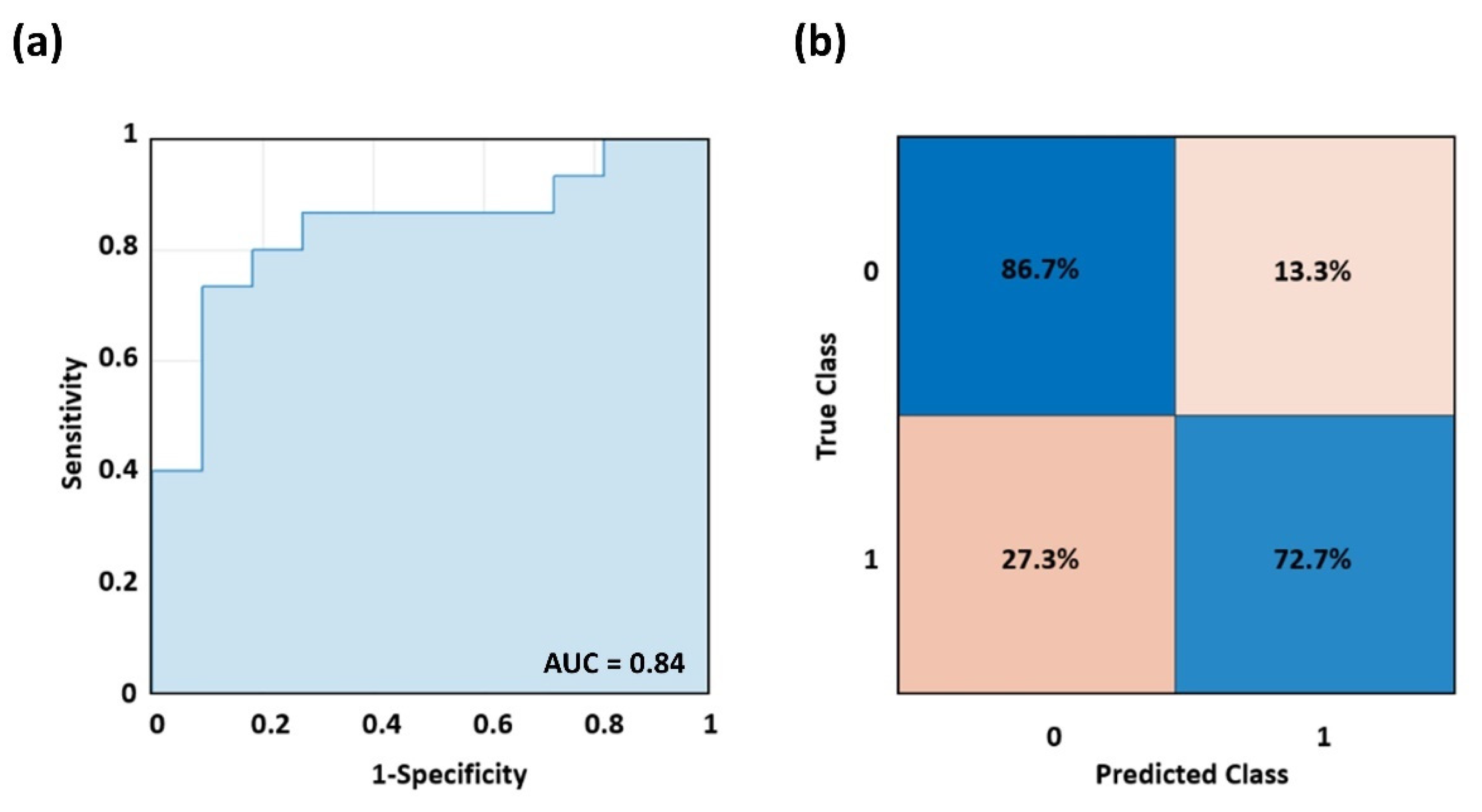
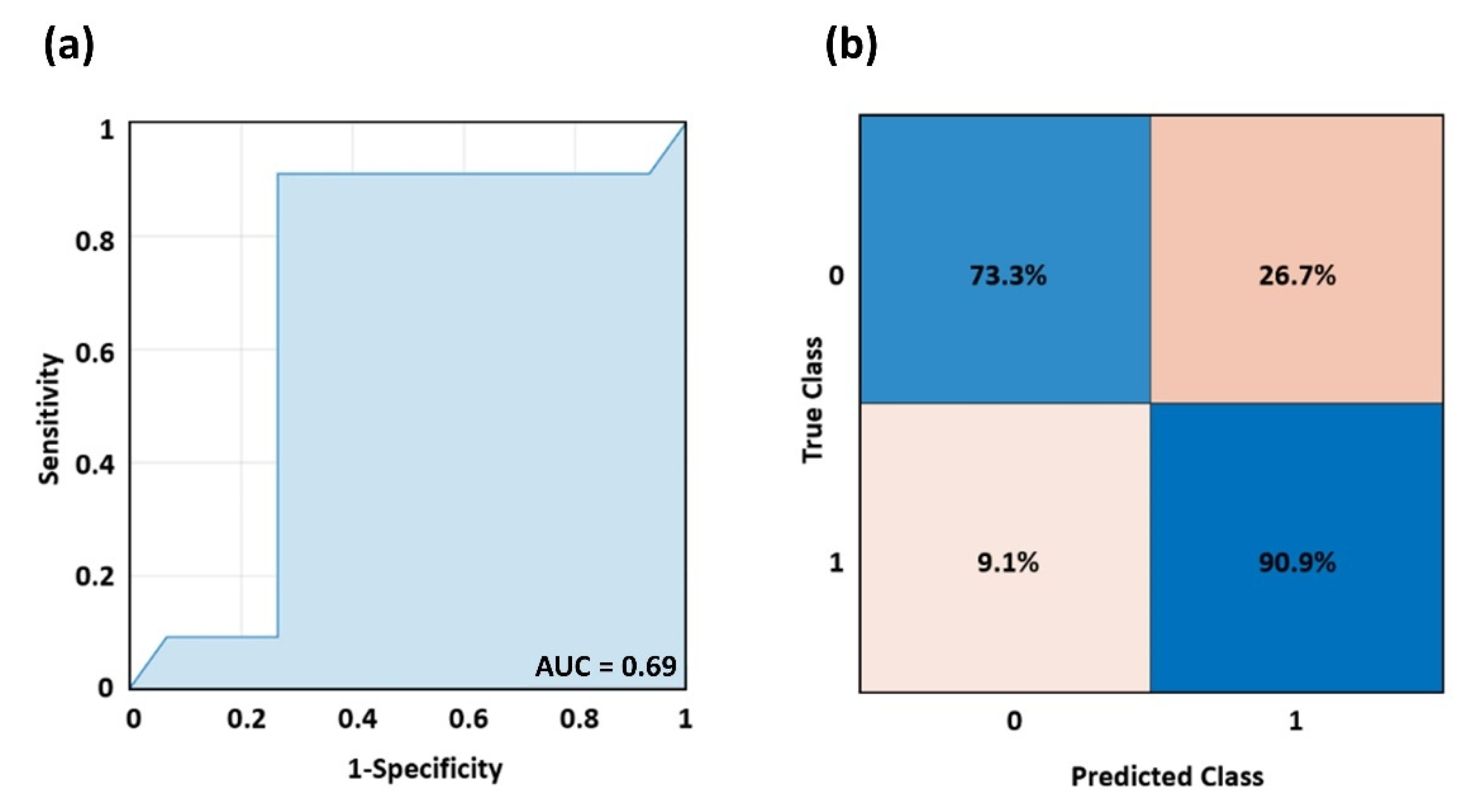
3.2. Machine Learning Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dubois, B.; Feldman, H.H.; Jacova, C.; DeKosky, S.T.; Barberger-Gateau, P.; Cummings, J.; Delacourte, A.; Galasko, D.; Gauthier, S.; Jicha, G. Research Criteria for the Diagnosis of Alzheimer’s Disease: Revising the NINCDS–ADRDA Criteria. Lancet Neurol. 2007, 6, 734–746. [Google Scholar] [CrossRef]
- Perpetuini, D.; Chiarelli, A.M.; Filippini, C.; Cardone, D.; Croce, P.; Rotunno, L.; Anzoletti, N.; Zito, M.; Zappasodi, F.; Merla, A. Working Memory Decline in Alzheimer’s Disease Is Detected by Complexity Analysis of Multimodal EEG-FNIRS. Entropy 2020, 22, 1380. [Google Scholar] [CrossRef] [PubMed]
- Sisodia, S.S.; Koo, E.H.; Beyreuther, K.; Unterbeck, A.; Price, D.L. Evidence That β-Amyloid Protein in Alzheimer’s Disease Is not Derived by Normal Processing. Science 1990, 248, 492–495. [Google Scholar] [CrossRef]
- Thomas, T.; Thomas, G.; McLendon, C.; Sutton, T.; Mullan, M. β-Amyloid-Mediated Vasoactivity and Vascular Endothelial Damage. Nature 1996, 380, 168–171. [Google Scholar] [CrossRef] [PubMed]
- Clark, E.A.; Leach, K.L.; Trojanowski, J.Q.; Lee, V.M. Characterization and Differential Distribution of the Three Major Human Protein Kinase C Isozymes (PKC Alpha, PKC Beta, and PKC Gamma) of the Central Nervous System in Normal and Alzheimer’s Disease Brains. Lab. Investig. J. Tech. Methods Pathol. 1991, 64, 35–44. [Google Scholar]
- Ferrarese, C.; Begni, B.; Canevari, C.; Zoia, C.; Piolti, R.; Frigo, M.; Appollonio, I.; Frattola, L. Glutamate Uptake Is Decreased in Platelets from Alzheimer’s Disease Patients. Ann. Neurol. 2000, 47, 641–643. [Google Scholar] [CrossRef]
- Zubenko, G.S.; Teply, I.; Winwood, E.; Huff, F.J.; Moossy, J.; Sunderland, T.; Martinez, A.J. Prospective Study of Increased Platelet Membrane Fluidity as a Risk Factor for Alzheimer’s Disease: Results at 5 Years. Am. J. Psychiatry 1996, 153, 420–423. [Google Scholar]
- Di Luca, M.; Pastorino, L.; Bianchetti, A.; Perez, J.; Vignolo, L.A.; Lenzi, G.L.; Trabucchi, M.; Cattabeni, F.; Padovani, A. Differential Level of Platelet Amyloid β Precursor Protein Isoforms: An Early Marker for Alzheimer Disease. Arch. Neurol. 1998, 55, 1195–1200. [Google Scholar] [CrossRef]
- Padovani, A.; Borroni, B.; Colciaghi, F.; Pettenati, C.; Cottini, E.; Agosti, C.; Lenzi, G.L.; Caltagirone, C.; Trabucchi, M.; Cattabeni, F. Abnormalities in the Pattern of Platelet Amyloid Precursor Protein Forms in Patients with Mild Cognitive Impairment and Alzheimer Disease. Arch. Neurol. 2002, 59, 71–75. [Google Scholar] [CrossRef]
- Borroni, B.; Volpi, R.; Martini, G.; Del Bono, R.; Archetti, S.; Colciaghi, F.; Akkawi, N.M.; Di Luca, M.; Romanelli, G.; Caimi, L. Peripheral Blood Abnormalities in Alzheimer Disease: Evidence for Early Endothelial Dysfunction. Alzheimer Dis. Assoc. Disord. 2002, 16, 150–155. [Google Scholar] [CrossRef]
- Khalil, Z.; LoGiudice, D.; Khodr, B.; Maruff, P.; Masters, C. Impaired Peripheral Endothelial Microvascular Responsiveness in Alzheimer’s Disease. J. Alzheimer’s Dis. 2007, 11, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Bernardi, L.; Berardesca, E. Measurement of Skin Blood Flow by Laser-Doppler Flowmetry. In Bioengineering of the Skin: Methods and Instrumentation; CRC Press: Boca Raton, FL, USA, 2007; ISBN 978-1-00-306896-9. [Google Scholar]
- Perpetuini, D.; Chiarelli, A.M.; Maddiona, L.; Rinella, S.; Bianco, F.; Bucciarelli, V.; Gallina, S.; Perciavalle, V.; Vinciguerra, V.; Merla, A. Multi-Site Photoplethysmographic and Electrocardiographic System for Arterial Stiffness and Cardiovascular Status Assessment. Sensors 2019, 19, 5570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iwamoto, T.; Kanetaka, H.; Takasaki, M.; Takazawa, K. Hemodynamic Changes in Alzheimer’s and Binswanger’s Diseases as Evaluated by Second-Derivative Finger Photoplethysmography. Geriatr. Gerontol. Int. 2003, 3, 243–249. [Google Scholar] [CrossRef]
- Gwak, M.; Sarrafzadeh, M.; Woo, E. Support for a Clinical Diagnosis of Mild Cognitive Impairment Using Photoplethysmography and Gait Sensors. In Proceedings of the APSIPA Annual Summit and Conference, Honolulu, HI, USA, 12–15 November 2018; Volume 2018, pp. 12–15. [Google Scholar]
- Affoo, R.H.; Foley, N.; Rosenbek, J.; Kevin Shoemaker, J.; Martin, R.E. Swallowing Dysfunction and Autonomic Nervous System Dysfunction in Alzheimer’s Disease: A Scoping Review of the Evidence. J. Am. Geriatr. Soc. 2013, 61, 2203–2213. [Google Scholar] [CrossRef] [PubMed]
- Algotsson, A.; Viitanen, M.; Winblad, B.; Solders, G. Autonomic Dysfunction in Alzheimer’s Disease. Acta Neurol. Scand. 1995, 91, 14–18. [Google Scholar] [CrossRef]
- Femminella, G.D.; Rengo, G.; Komici, K.; Iacotucci, P.; Petraglia, L.; Pagano, G.; De Lucia, C.; Canonico, V.; Bonaduce, D.; Leosco, D. Autonomic Dysfunction in Alzheimer’s Disease: Tools for Assessment and Review of the Literature. J. Alzheimer’s Dis. 2014, 42, 369–377. [Google Scholar] [CrossRef]
- Diamond, P.T.; Diamond, M.T. Thermoregulatory Behavior in Alzheimer’s Disease. J. Am. Geriatr. Soc. 1991, 39, 532. [Google Scholar] [CrossRef]
- Almeida, M.C.; Vizin, R.C.L.; Carrettiero, D.C. Current Understanding on the Neurophysiology of Behavioral Thermoregulation. Temperature 2015, 2, 483–490. [Google Scholar] [CrossRef]
- Carrettiero, D.C.; Santiago, F.E.; Motzko-Soares, A.C.P.; Almeida, M.C. Temperature and Toxic Tau in Alzheimer’s Disease: New Insights. Temperature 2015, 2, 491–498. [Google Scholar] [CrossRef]
- Klegeris, A.; Schulzer, M.; Harper, D.G.; McGeer, P.L. Increase in Core Body Temperature of Alzheimer’s Disease Patients as a Possible Indicator of Chronic Neuroinflammation: A Meta-Analysis. Gerontology 2007, 53, 7–11. [Google Scholar] [CrossRef]
- Weldemichael, D.A.; Grossberg, G.T. Circadian Rhythm Disturbances in Patients with Alzheimer’s Disease: A Review. Int. J. Alzheimer’s Dis. 2010, 2010, 716453. [Google Scholar] [CrossRef] [PubMed]
- Perpetuini, D.; Cardone, D.; Chiarelli, A.M.; Filippini, C.; Croce, P.; Zappasodi, F.; Rotunno, L.; Anzoletti, N.; Zito, M.; Merla, A. Autonomic Impairment in Alzheimer’s Disease Is Revealed by Complexity Analysis of Functional Thermal Imaging Signals during Cognitive Tasks. Physiol. Meas. 2019, 40, 034002. [Google Scholar] [CrossRef] [PubMed]
- Perpetuini, D.; Cardone, D.; Bucco, R.; Zito, M.; Merla, A. Assessment of the Autonomic Response in Alzheimer’s Patients During the Execution of Memory Tasks: A Functional Thermal Imaging Study. Curr. Alzheimer Res. 2018, 15, 951–958. [Google Scholar] [CrossRef] [PubMed]
- Kensinger, E.A.; Anderson, A.; Growdon, J.H.; Corkin, S. Effects of Alzheimer Disease on Memory for Verbal Emotional Information. Neuropsychologia 2004, 42, 791–800. [Google Scholar] [CrossRef]
- Vardasca, R.; Simoes, R. Current Issues in Medical Thermography. In Topics in Medical Image Processing and Computational Vision; Springer: Berlin/Heidelberg, Germany, 2013; pp. 223–237. [Google Scholar]
- Fernández-Cuevas, I.; Marins, J.C.B.; Lastras, J.A.; Carmona, P.M.G.; Cano, S.P.; García-Concepción, M.Á.; Sillero-Quintana, M. Classification of Factors Influencing the Use of Infrared Thermography in Humans: A Review. Infrared Phys. Technol. 2015, 71, 28–55. [Google Scholar] [CrossRef]
- Clay-Warner, J.; Robinson, D.T. Infrared Thermography as a Measure of Emotion Response. Emot. Rev. 2015, 7, 157–162. [Google Scholar] [CrossRef]
- Eysenck, M.W.; Derakshan, N.; Santos, R.; Calvo, M.G. Anxiety and Cognitive Performance: Attentional Control Theory. Emotion 2007, 7, 336. [Google Scholar] [CrossRef]
- Genno, H.; Ishikawa, K.; Kanbara, O.; Kikumoto, M.; Fujiwara, Y.; Suzuki, R.; Osumi, M. Using Facial Skin Temperature to Objectively Evaluate Sensations. Int. J. Ind. Ergon. 1997, 19, 161–171. [Google Scholar] [CrossRef]
- Salazar-López, E.; Domínguez, E.; Ramos, V.J.; de la Fuente, J.; Meins, A.; Iborra, O.; Gálvez, G.; Rodríguez-Artacho, M.A.; Gómez-Milán, E. The Mental and Subjective Skin: Emotion, Empathy, Feelings and Thermography. Conscious. Cogn. 2015, 34, 149–162. [Google Scholar] [CrossRef]
- Veltman, J.A.; Vos, W.K. Facial Temperature as a Measure of Operator State; CRC Press: Boca Raton, FL, USA, 2005. [Google Scholar]
- Anbar, M. Assessment of Physiologic and Pathologic Radiative Heat Dissipation Using Dynamic Infrared Imaging. Ann. N. Y. Acad. Sci. 2002, 972, 111–118. [Google Scholar] [CrossRef]
- Magalhaes, C.; Mendes, J.; Vardasca, R. Meta-Analysis and Systematic Review of the Application of Machine Learning Classifiers in Biomedical Applications of Infrared Thermography. Appl. Sci. 2021, 11, 842. [Google Scholar] [CrossRef]
- Vardasca, R.; Magalhaes, C.; Mendes, J. Biomedical Applications of Infrared Thermal Imaging: Current State of Machine Learning Classification. In Proceedings of the Multidisciplinary Digital Publishing Institute Proceedings, Medan, Indonesia, 11–14 December 2019; Volume 27, p. 46. [Google Scholar]
- Michie, D.; Spiegelhalter, D.J.; Taylor, C.C. Machine Learning, Neural and Statistical Classification; CiteSeer: Pennsylvania, PA, USA, 1994. [Google Scholar]
- Kohavi, R. A Study of Cross-Validation and Bootstrap for Accuracy Estimation and Model Selection. In Proceedings of the IJCAI, Montreal, QC, Canada, 19–21 August 1995; Volume 14, pp. 1137–1145. [Google Scholar]
- Duan, F.; Huang, Z.; Sun, Z.; Zhang, Y.; Zhao, Q.; Cichocki, A.; Yang, Z.; Solé-Casals, J. Topological Network Analysis of Early Alzheimer’s Disease Based on Resting-State EEG. IEEE Trans. Neural Syst. Rehabil. Eng. 2020, 28, 2164–2172. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.; He, L.; Zhang, Y.; Shen, L.; Chen, B. Interpretable Graph Convolutional Network Of Multi-Modality Brain Imaging For Alzheimer’s Disease Diagnosis. In Proceedings of the 2022 IEEE 19th International Symposium on Biomedical Imaging (ISBI), Kolkata, India, 28–31 March 2022; pp. 1–5. [Google Scholar]
- Zhang, Y.; Zhang, H.; Adeli, E.; Chen, X.; Liu, M.; Shen, D. Multiview Feature Learning with Multiatlas-Based Functional Connectivity Networks for MCI Diagnosis. In IEEE Transactions on Cybernetics; IEEE: Piscataway, NJ, USA, 2020. [Google Scholar]
- Zhang, Y.; Zhang, H.; Chen, X.; Liu, M.; Zhu, X.; Lee, S.-W.; Shen, D. Strength and Similarity Guided Group-Level Brain Functional Network Construction for MCI Diagnosis. Pattern Recognit. 2019, 88, 421–430. [Google Scholar] [CrossRef]
- Perpetuini, D.; Bucco, R.; Zito, M.; Merla, A. Study of Memory Deficit in Alzheimer’s Disease by Means of Complexity Analysis of FNIRS Signal. Neurophotonics 2018, 5, 011010. [Google Scholar] [CrossRef]
- Tanveer, M.; Richhariya, B.; Khan, R.U.; Rashid, A.H.; Khanna, P.; Prasad, M.; Lin, C.T. Machine Learning Techniques for the Diagnosis of Alzheimer’s Disease: A Review. ACM Trans. Multimed. Comput. Commun. Appl. (TOMM) 2020, 16, 1–35. [Google Scholar] [CrossRef]
- Geyer, M.J.; Jan, Y.-K.; Brienza, D.M.; Boninger, M.L. Using Wavelet Analysis to Characterize the Thermoregulatory Mechanisms of Sacral Skin Blood Flow. J. Rehabil. Res. Dev. 2004, 41, 797–806. [Google Scholar] [CrossRef] [PubMed]
- Perpetuini, D.; Formenti, D.; Iodice, P.; Cardone, D.; Filippini, C.; Chiarelli, A.M.; Michielon, G.; Trecroci, A.; Alberti, G.; Merla, A. Central and Peripheral Thermal Signatures of Brain-Derived Fatigue during Unilateral Resistance Exercise: A Preliminary Study. Biology 2022, 11, 322. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-Mental State”: A Practical Method for Grading the Cognitive State of Patients for the Clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Ring, E.F.J.; Ammer, K. Infrared Thermal Imaging in Medicine. Physiol. Meas. 2012, 33, R33. [Google Scholar] [CrossRef]
- Diakides, M.; Bronzino, J.D.; Peterson, D.R. Medical Infrared Imaging: Principles and Practices; CRC Press: Boca Raton, FL, USA, 2012; ISBN 1-4398-7250-3. [Google Scholar]
- Marins, J.C.B.; Formenti, D.; Costa, C.M.A.; de Andrade Fernandes, A.; Sillero-Quintana, M. Circadian and Gender Differences in Skin Temperature in Militaries by Thermography. Infrared Phys. Technol. 2015, 71, 322–328. [Google Scholar] [CrossRef]
- Perpetuini, D.; Cardone, D.; Filippini, C.; Chiarelli, A.M.; Merla, A. A Motion Artifact Correction Procedure for FNIRS Signals Based on Wavelet Transform and Infrared Thermography Video Tracking. Sensors 2021, 21, 5117. [Google Scholar] [CrossRef] [PubMed]
- Osisanwo, F.Y.; Akinsola, J.E.T.; Awodele, O.; Hinmikaiye, J.O.; Olakanmi, O.; Akinjobi, J. Supervised Machine Learning Algorithms: Classification and Comparison. Int. J. Comput. Trends Technol. (IJCTT) 2017, 48, 128–138. [Google Scholar]
- Zhang, S.; Li, X.; Zong, M.; Zhu, X.; Cheng, D. Learning k for Knn Classification. ACM Trans. Intell. Syst. Technol. (TIST) 2017, 8, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Rokach, L. Ensemble-Based Classifiers. Artif. Intell. Rev. 2010, 33, 1–39. [Google Scholar] [CrossRef]
- Esterman, M.; Tamber-Rosenau, B.J.; Chiu, Y.-C.; Yantis, S. Avoiding Non-Independence in FMRI Data Analysis: Leave One Subject Out. Neuroimage 2010, 50, 572–576. [Google Scholar] [CrossRef]
- Petersen, R.C. Mild Cognitive Impairment: Transition between Aging and Alzheimer’s Disease. NEUROLOGIA 2000, 15, 93–101. [Google Scholar] [CrossRef]
- Serrano-Pozo, A.; Frosch, M.P.; Masliah, E.; Hyman, B.T. Neuropathological Alterations in Alzheimer Disease. Cold Spring Harb. Perspect. Med. 2011, 1, a006189. [Google Scholar] [CrossRef]
- Chiarelli, A.M.; Perpetuini, D.; Croce, P.; Filippini, C.; Cardone, D.; Rotunno, L.; Anzoletti, N.; Zito, M.; Zappasodi, F.; Merla, A. Evidence of Neurovascular Un-Coupling in Mild Alzheimer’s Disease through Multimodal EEG-FNIRS and Multivariate Analysis of Resting-State Data. Biomedicines 2021, 9, 337. [Google Scholar] [CrossRef]
- Cicalese, P.A.; Li, R.; Ahmadi, M.B.; Wang, C.; Francis, J.T.; Selvaraj, S.; Schulz, P.E.; Zhang, Y. An EEG-FNIRS Hybridization Technique in the Four-Class Classification of Alzheimer’s Disease. J. Neurosci. Methods 2020, 336, 108618. [Google Scholar] [CrossRef]
- De la Torre, J.C.; Mussivan, T. Can Disturbed Brain Microcirculation Cause Alzheimer’s Disease? Neurol. Res. 1993, 15, 146–153. [Google Scholar] [CrossRef]
- Grammas, P. A Damaged Microcirculation Contributes to Neuronal Cell Death in Alzheimer’s Disease☆. Neurobiol. Aging 2000, 21, 199–205. [Google Scholar] [CrossRef]
- De la Torre, J.C. Impaired Brain Microcirculation May Trigger Alzheimer’s Disease. Neurosci. Biobehav. Rev. 1994, 18, 397–401. [Google Scholar] [CrossRef]
- Liguori, C.; Maestri, M.; Spanetta, M.; Placidi, F.; Bonanni, E.; Mercuri, N.B.; Guarnieri, B. Sleep-Disordered Breathing and the Risk of Alzheimer’s Disease. Sleep Med. Rev. 2021, 55, 101375. [Google Scholar] [CrossRef] [PubMed]
- Osorio, R.S.; Gumb, T.; Pirraglia, E.; Varga, A.W.; Lu, S.; Lim, J.; Wohlleber, M.E.; Ducca, E.L.; Koushyk, V.; Glodzik, L.; et al. Sleep-Disordered Breathing Advances Cognitive Decline in the Elderly. Neurology 2015, 84, 1964–1971. [Google Scholar] [CrossRef]
- Aharon-Peretz, J.; Harel, T.; Revach, M.; Ben-Haim, S.A. Increased Sympathetic and Decreased Parasympathetic Cardiac Innervation in Patients with Alzheimer’s Disease. Arch. Neurol. 1992, 49, 919–922. [Google Scholar] [CrossRef] [PubMed]
- Mellingsæter, M.R.; Wyller, T.B.; Ranhoff, A.H.; Bogdanovic, N.; Wyller, V.B. Reduced Sympathetic Response to Head-Up Tilt in Subjects with Mild Cognitive Impairment or Mild Alzheimer’s Dementia. DEE 2015, 5, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Prinz, P.N.; Christie, C.; Smallwood, R.; Vitaliano, P.; Bokan, J.; Vitiello, M.V.; Martin, D. Circadian Temperature Variation in Healthy Aged and in Alzheimer’s Disease. J. Gerontol. 1984, 39, 30–35. [Google Scholar] [CrossRef]
- Van Breemen, C.; Skarsgard, P.; Laher, I.; McManus, B.; Wang, X. Endothelium-Smooth Muscle Interactions in Blood Vessels. Clin. Exp. Pharmacol. Physiol. 1997, 24, 989–992. [Google Scholar] [CrossRef]
- Jung, D.H.; Kim, H.J.; Koh, K.S.; Oh, C.S.; Kim, K.-S.; Yoon, J.-H.; Chung, I.-H. Arterial Supply of the Nasal Tip in Asians. Laryngoscope 2000, 110, 308. [Google Scholar] [CrossRef]
- Alberdi, A.; Aztiria, A.; Basarab, A. On the Early Diagnosis of Alzheimer’s Disease from Multimodal Signals: A Survey. Artif. Intell. Med. 2016, 71, 1–29. [Google Scholar] [CrossRef]
- Raghavendra, U.; Acharya, U.R.; Adeli, H. Artificial Intelligence Techniques for Automated Diagnosis of Neurological Disorders. Eur. Neurol. 2019, 82, 41–64. [Google Scholar] [CrossRef] [PubMed]
- Basaia, S.; Agosta, F.; Wagner, L.; Canu, E.; Magnani, G.; Santangelo, R.; Filippi, M. Alzheimer’s Disease Neuroimaging Initiative Automated Classification of Alzheimer’s Disease and Mild Cognitive Impairment Using a Single MRI and Deep Neural Networks. NeuroImage Clin. 2019, 21, 101645. [Google Scholar] [CrossRef] [PubMed]
- Qi, Z.; Tian, Y.; Shi, Y. Robust Twin Support Vector Machine for Pattern Classification. Pattern Recognit. 2013, 46, 305–316. [Google Scholar] [CrossRef]
- Richhariya, B.; Tanveer, M.; Rashid, A.H.; Initiative, A.D.N. Diagnosis of Alzheimer’s Disease Using Universum Support Vector Machine Based Recursive Feature Elimination (USVM-RFE). Biomed. Signal Process. Control 2020, 59, 101903. [Google Scholar] [CrossRef]
- Malik, A.K.; Ganaie, M.A.; Tanveer, M.; Suganthan, P.N.; Initiative, A.D.N.I. Alzheimer’s Disease Diagnosis via Intuitionistic Fuzzy Random Vector Functional Link Network. In IEEE Transactions on Computational Social Systems; IEEE: Piscataway, NJ, USA, 2022. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Frequency Band | t-Stat | d.f. | p-Value |
|---|---|---|---|
| Neurogenic | −0.154 | 24 | 0.879 |
| Myogenic | 0.029 | 24 | 0.977 |
| Respiratory | −1.794 | 24 | 0.085 |
| Cardiac | −1.376 | 24 | 0.182 |
| ML Classifier | Accuracy | Sensitivity | Specificity |
|---|---|---|---|
| KNN | |||
| Fine | 53.8 | 46.7 | 63.6 |
| Medium | 57.7 | 80 | 27.3 |
| Coarse | 69.2 | 86.7 | 45.5 |
| Ensemble classifiers | |||
| Bagged Trees | 65.4 | 66.7 | 63.6 |
| Subspace Discriminant | 61.5 | 60 | 63.6 |
| SVM | |||
| Linear | 61.5 | 93.3 | 18.2 |
| Quadratic | 69.2 | 73.3 | 63.3 |
| Cubic | 61.5 | 73.3 | 45.5 |
| RBF | 79.7 | 72.7 | 86.7 |
| DTC | 82.1 | 90.9 | 73.3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perpetuini, D.; Filippini, C.; Zito, M.; Cardone, D.; Merla, A. Altered Microcirculation in Alzheimer’s Disease Assessed by Machine Learning Applied to Functional Thermal Imaging Data. Bioengineering 2022, 9, 492. https://doi.org/10.3390/bioengineering9100492
Perpetuini D, Filippini C, Zito M, Cardone D, Merla A. Altered Microcirculation in Alzheimer’s Disease Assessed by Machine Learning Applied to Functional Thermal Imaging Data. Bioengineering. 2022; 9(10):492. https://doi.org/10.3390/bioengineering9100492
Chicago/Turabian StylePerpetuini, David, Chiara Filippini, Michele Zito, Daniela Cardone, and Arcangelo Merla. 2022. "Altered Microcirculation in Alzheimer’s Disease Assessed by Machine Learning Applied to Functional Thermal Imaging Data" Bioengineering 9, no. 10: 492. https://doi.org/10.3390/bioengineering9100492