
Machine Learning Evaluation of Biliary Atresia Patients to Predict Long-Term Outcome after the Kasai Procedure

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Laboratory Tests
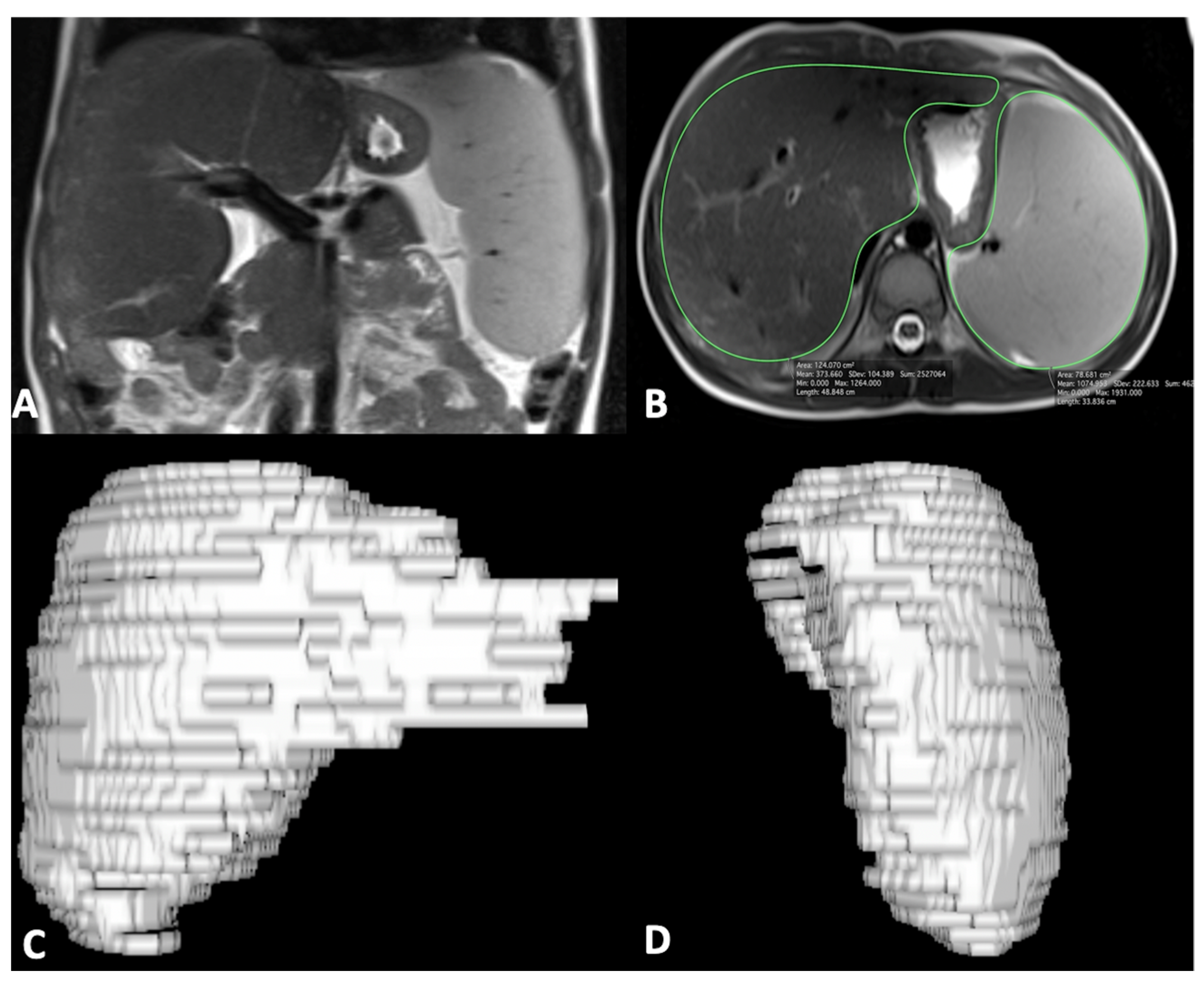
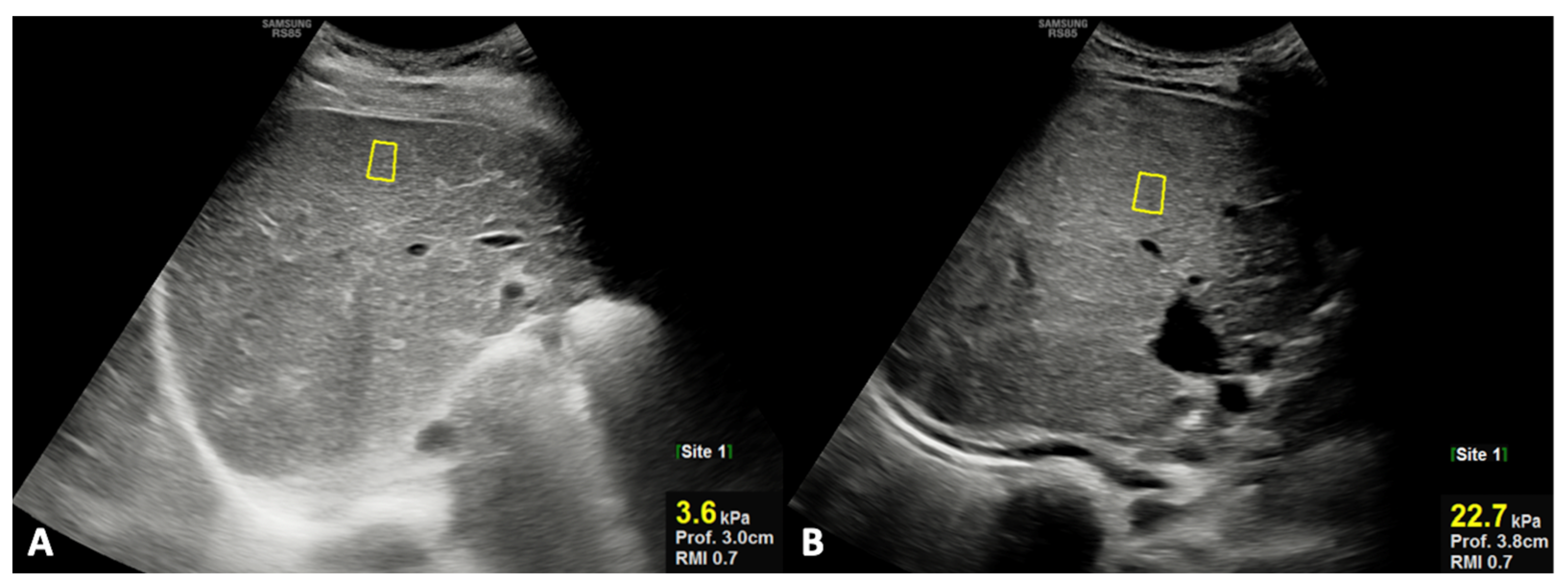
2.3. US and MR Imaging Acquisition and Processing
2.4. Statistical Analysis
2.5. Machine Learning: Tools and Algorithms
3. Results
3.1. Patient Population
3.2. Descriptive Analysis
3.3. Machine Learning
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Maity, N.G.; Das, S. Machine learning for improved diagnosis and prognosis in healthcare. In Proceedings of the 2017 IEEE Aerospace Conference, Big Sky, MT, USA, 4–11 March 2017; pp. 1–9. [Google Scholar]
- Cerri, R.; Da Silva, R.R.O.; De Carvalho, A.C.P.L.F. Comparing methods for multilabel classification of proteins using machine learning techniques. Lect. Notes Comput. Sci. 2009, 5676 LNBI, 109–120. [Google Scholar]
- Daldrup-Link, H. Artificial intelligence applications for pediatric oncology imaging. Pediatr. Radiol. 2019, 49, 1384–1390. [Google Scholar] [CrossRef] [PubMed]
- Booz, C.; Yel, I.; Wichmann, J.L.; Boettger, S.; Al Kamali, A.; Albrecht, M.H.; Martin, S.S.; Lenga, L.; Huizinga, N.A.; D’Angelo, T.; et al. Artificial intelligence in bone age assessment: Accuracy and efficiency of a novel fully automated algorithm compared to the Greulich-Pyle method. Eur. Radiol. Exp. 2020, 4, 6. [Google Scholar] [CrossRef]
- Scruggs, B.A.; Paulchan, R.V.; Kalpathy-Cramer, J.; Chiang, M.F.; Peter Campbell, J. Artificial intelligence in retinopathy of prematurity diagnosis. Transl. Vis. Sci. Technol. 2020, 9, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ricciardi, C.; Cantoni, V.; Green, R.; Improta, G.; Cesarelli, M. Is It Possible to Predict Cardiac Death? In Proceedings of the Mediterranean Conference on Medical and Biological Engineering and Computing, São Francisco, Portugal, 26–28 September 2019; Springer: Cham, Switzerland; 2019; pp. 847–854. [Google Scholar]
- Ricciardi, C.; Valente, A.S.; Edmund, K.; Cantoni, V.; Green, R.; Fiorillo, A.; Picone, I.; Santini, S.; Cesarelli, M. Linear discriminant analysis and principal component analysis to predict coronary artery disease. Health Inform. J. 2020, 26, 2181–2192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ricciardi, C.; Amboni, M.; De Santis, C.; Ricciardelli, G.; Improta, G.; Iuppariello, L.; D’Addio, G.; Barone, P.; Cesarelli, M. Classifying Different Stages of Parkinson’s Disease Through Random Forests. In Proceedings of the Mediterranean Conference on Medical and Biological Engineering and Computing, São Francisco, Portugal, 26–28 September 2019; Springer: Cham, Switzerland, 2019; pp. 1155–1162. [Google Scholar]
- Cantoni, V.; Green, R.; Ricciardi, C.; Assante, R.; Zampella, E.; Nappi, C.; Gaudieri, V.; Mannarino, T.; Genova, A.; De Simini, G.; et al. A machine learning-based approach to directly compare the diagnostic accuracy of myocardial perfusion imaging by conventional and cadmium-zinc telluride SPECT. J. Nucl. Cardiol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Scrutinio, D.; Ricciardi, C.; Donisi, L.; Losavio, E.; Battista, P.; Guida, P.; Cesarelli, M.; Pagano, G.; D’Addio, G. Machine learning to predict mortality after rehabilitation among patients with severe stroke. Sci. Rep. 2020, 10, 20127. [Google Scholar] [CrossRef] [PubMed]
- Improta, G.; Ricciardi, C.; Amato, F.; D’Addio, G.; Cesarelli, M.; Romano, M. Efficacy of Machine Learning in Predicting the Kind of Delivery by Cardiotocography. In Proceedings of the Mediterranean Conference on Medical and Biological Engineering and Computing, São Francisco, Portugal, 26–28 September 2019; Springer: Cham, Switzerland, 2019; pp. 793–799. [Google Scholar]
- Hartley, J.L.; Davenport, M.; Kelly, D.A. Biliary atresia. Lancet 2009, 374, 1704–1713. [Google Scholar] [CrossRef]
- Neto, B.; Borges-Dias, M.; Trindade, E.; Estevão-Costa, J.; Campos, J.M. Biliary Atresia-Clinical Series. GE Port. J. Gastroenterol. 2018, 25, 68–73. [Google Scholar] [CrossRef] [Green Version]
- Govindarajan, K.K. Biliary atresia: Where do we stand now? World J. Hepatol. 2016, 8, 1593. [Google Scholar] [CrossRef]
- Feldman, A.G.; Mack, C.L. Biliary Atresia: Clinical Lessons Learned. J. Pediatr. Gastroenterol. Nutr. 2015, 61, 167–175. [Google Scholar] [CrossRef] [PubMed]
- Baumann, U.; Ure, B. Biliary atresia. Clin. Res. Hepatol. Gastroenterol. 2012, 36, 257–259. [Google Scholar] [CrossRef] [PubMed]
- Nio, M.; Wada, M.; Sasaki, H.; Tanaka, H.; Okamura, A. Risk factors affecting late-presenting liver failure in adult patients with biliary atresia. J. Pediatr. Surg. 2012, 47, 2179–2183. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.S.; Ong, S.Y.; Foo, H.W.; Wong, S.Y.; Kong, C.X.; Seah, R.B.; Ng, R.T. Chronic liver disease is universal in children with biliary atresia living with native liver. World J. Gastroenterol. 2017, 23, 7776–7784. [Google Scholar] [CrossRef]
- Jeon, T.Y.; Yoo, S.-Y.; Kim, J.H.; Eo, H.; Lee, S.-K. Serial ultrasound findings associated with early liver transplantation after Kasai portoenterostomy in biliary atresia. Clin. Radiol. 2013, 68, 588–594. [Google Scholar] [CrossRef]
- Takahashi, A.; Hatakeyama, S.I.; Kuroiwa, M.; Suzuki, N.; Toki, F.; Suzuki, M.; Suehiro, T.; Shimura, T.; Kuwano, H. Time-course changes in the liver of biliary atresia patients on magnetic resonance imaging. Pediatr. Int. 2009, 51, 66–70. [Google Scholar] [CrossRef]
- Caruso, M.; Cuocolo, R.; Di Dato, F.; Mollica, C.; Vallone, G.; Romeo, V.; Petretta, M.; Liuzzi, R.; Mainenti, P.P.; Iorio, R.; et al. Ultrasound, shear-wave elastography, and magnetic resonance imaging in native liver survivor patients with biliary atresia after Kasai portoenterostomy: Correlation with medical outcome after treatment. Acta Radiol. 2020, 61, 1300–1308. [Google Scholar] [CrossRef]
- Caruso, M.; Di Dato, F.; Mollica, C.; Vallone, G.; Romeo, V.; Liuzzi, R.; Mainenti, P.P.; Petretta, M.; Iorio, R.; Brunetti, A.; et al. Imaging prediction with ultrasound and MRI of long-term medical outcome in native liver survivor patients with biliary atresia after kasai portoenterostomy: A pilot study. Abdom. Radiol. 2021, 46, 2595–2603. [Google Scholar] [CrossRef]
- Ng, V.L.; Haber, B.H.; Magee, J.C.; Miethke, A.; Murray, K.F.; Michail, S.; Karpen, S.J.; Kerkar, N.; Molleston, J.P.; Romero, R.; et al. Medical Status of 219 Children with Biliary Atresia Surviving Long-Term with Their Native Livers: Results from a North American Multicenter Consortium. J. Pediatr. 2014, 165, 539–546.e2. [Google Scholar] [CrossRef] [Green Version]
- Konuş, O.L.; Ozdemir, A.; Akkaya, A.; Erbaş, G.; Celik, H.; Işik, S. Normal liver, spleen, and kidney dimensions in neonates, infants, and children: Evaluation with sonography. Am. J. Roentgenol. 1998, 171, 1693–1698. [Google Scholar] [CrossRef]
- Serai, S.D.; Trout, A.T.; Sirlin, C.B. Elastography to assess the stage of liver fibrosis in children: Concepts, opportunities, and challenges. Clin. Liver Dis. 2017, 9, 5–10. [Google Scholar] [CrossRef] [Green Version]
- Dillman, J.R.; Heider, A.; Bilhartz, J.L.; Smith, E.A.; Keshavarzi, N.; Rubin, J.M.; Lopez, M.J. Ultrasound shear wave speed measurements correlate with liver fibrosis in children. Pediatr. Radiol. 2015, 45, 1480–1488. [Google Scholar] [CrossRef]
- Lurie, Y.; Webb, M.; Cytter-Kuint, R.; Shteingart, S.; Lederkremer, G.Z. Non-invasive diagnosis of liver fibrosis and cirrhosis. World J. Gastroenterol. 2015, 21, 11567–11583. [Google Scholar] [CrossRef]
- Tang, A.; Cloutier, G.; Szeverenyi, N.M.; Sirlin, C.B. Ultrasound Elastography and MR Elastography for Assessing Liver Fibrosis: Part 2, Diagnostic Performance, Confounders, and Future Directions. Am. J. Roentgenol. 2015, 205, 33–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Der Vorst, J.R.; Van Dam, R.M.; Van Stiphout, R.S.A.; Van Den Broek, M.A.; Hollander, I.H.; Kessels, A.G.H.; Dejong, C.H.C. Virtual Liver Resection and Volumetric Analysis of the Future Liver Remnant using Open Source Image Processing Software. World J. Surg. 2010, 34, 2426–2433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chawla, N.V.; Bowyer, K.W.; Hall, L.O.; Kegelmeyer, W.P. SMOTE: Synthetic Minority Over-sampling Technique. J. Artif. Intell. Res. 2002, 16, 321–357. [Google Scholar] [CrossRef]
- Wong, S.C.; Gatt, A.; Stamatescu, V.; McDonnell, M.D. Understanding Data Augmentation for Classification: When to Warp? In Proceedings of the 2016 International Conference on Digital Image Computing: Techniques and Applications (DICTA), Gold Coast, QLD, Australia, 30 November–2 December 2016. [Google Scholar]
- Witten, I.H.; Hall, M.A. Practical Machine Learning, 3rd ed.; Packt Publishing Ltd.: Birmingham, UK, 2016. [Google Scholar]
- Al-Aidaroos, K.M.; Abu Bakar, A.; Othman, Z. Naïve Bayes variants in classification learning. In Proceedings of the 2010 International Conference on Information Retrieval & Knowledge Management (CAMP), Shah Alam, Malaysia, 17–18 March 2010; pp. 276–281. [Google Scholar]
- Vapnik, V.N. An overview of statistical learning theory. IEEE Trans. Neural Netw. 1999, 10, 988–999. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, T.T. Performance evaluation of classification algorithms by k-fold and leave-one-out cross validation. Pattern Recognit. 2015, 48, 2839–2846. [Google Scholar] [CrossRef]
- Hossin, M.; Sulaiman, M.N. A Review on Evaluation Metrics for Data Classification Evaluations. Int. J. Data Min. Knowl. Manag. Process. 2015, 5, 01–11. [Google Scholar] [CrossRef]
- Tougui, I.; Jilbab, A.; El Mhamdi, J. Heart disease classification using data mining tools and machine learning techniques. Health Technol. 2020, 10, 1137–1144. [Google Scholar] [CrossRef]
- Ricciardi, C.; Donisi, L.; Cesarelli, G.; Pagano, G.; Coccia, A.; D’addio, G. Feasibility of Machine Learning applied to Poincaré Plot Analysis on Patients with CHF. In Proceedings of the 2020 11th Conference of the European Study Group on Cardiovascular Oscillations (ESGCO), Pisa, Italy, 27–29 April 2020; pp. 16–17. [Google Scholar]
- Donisi, L.; Ricciardi, C.; Cesarelli, G.; Pagano, G.; Amitrano, F.; D’addio, G. Machine Learning applied on Poincaré Analyisis to discriminate different cardiac issues. In Proceedings of the 2020 11th Conference of the European Study Group on Cardiovascular Oscillations (ESGCO), Pisa, Italy, 27–29 April 2020; pp. 17–18. [Google Scholar]
- Hahn, S.M.; Kim, S.; Park, K.I.; Han, S.J.; Koh, H. Clinical benefit of liver stiffness measurement at 3 months after Kasai hepatoportoenterostomy to predict the liver related events in biliary atresia. PLoS ONE 2013, 8, e80652. [Google Scholar] [CrossRef] [Green Version]
- Jain, V.; Burford, C.; Alexander, E.C.; Sutton, H.; Dhawan, A.; Joshi, D.; Davenport, M.; Heaton, N.; Hadzic, N.; Samyn, M. Prognostic markers at adolescence in patients requiring liver transplantation for biliary atresia in adulthood. J. Hepatol. 2019, 71, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Hanquinet, S.; Courvoisier, D.S.; Rougemont, A.L.; Wildhaber, B.E.; Merlini, L.; McLin, V.A.; Anooshiravani, M. Acoustic radiation force impulse sonography in assessing children with biliary atresia for liver transplantation. Pediatr. Radiol. 2016, 46, 1011–1016. [Google Scholar] [CrossRef] [PubMed]
- Yan, H.; Du, L.; Zhou, J.; Li, Y.; Lei, J.; Liu, J.; Luo, Y. Diagnostic performance and prognostic value of elastography in patients with biliary atresia and after hepatic portoenterostomy: Protocol for a systematic review and meta-analysis. BMJ Open 2021, 11, e042129. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Peng, C.; Wang, K.; Wu, D.; Yan, J.; Tu, W.; Chen, Y. The utility of shear wave elastography and serum biomarkers for diagnosing biliary atresia and predicting clinical outcomes. Eur. J. Pediatr. 2021. [Google Scholar] [CrossRef]
- Tsamardinos, I.; Rakhshani, A.; Lagani, V. Performance-Estimation Properties of Cross-Validation-Based Protocols with Simultaneous Hyper-Parameter Optimization. Int. J. Artif. Intell. Tools 2015, 24, 1540023. [Google Scholar] [CrossRef]
- Mannarino, T.; Assante, R.; Ricciardi, C.; Zampella, E.; Nappi, C.; Gaudieri, V.; Mainolfi, C.G.; Di Vaia, E.; Petretta, M.; Cesarelli, M.; et al. Head-to-head comparison of diagnostic accuracy of stress-only myocardial perfusion imaging with conventional and cadmium-zinc telluride single-photon emission computed tomography in women with suspected coronary artery disease. J. Nucl. Cardiol. 2021, 28, 888–897. [Google Scholar] [CrossRef]
- Ricciardi, C.; Cuocolo, R.; Verde, F.; Improta, G.; Stanzione, A.; Romeo, V.; Maurea, S.; D’Armiento, M.; Sarno, L.; Guida, M.; et al. Resolution Resampling of Ultrasound Images in Placenta Previa Patients: Influence on Radiomics Data Reliability and Usefulness for Machine Learning. In Proceedings of the European Medical and Biological Engineering Conference, Portorož, Slovenia, 29 November–3 December 2020; Springer: Cham, Switzerland; 2020; pp. 1011–1018. [Google Scholar]
- Davendralingam, N.; Sebire, N.J.; Arthurs, O.J.; Shelmerdine, S.C. Artificial intelligence in paediatric radiology: Future opportunities. Br. J. Radiol. 2021, 94, 20200975. [Google Scholar] [CrossRef]
- Rajpurkar, P.; Irvin, J.; Zhu, K.; Yang, B.; Mehta, H.; Duan, T.; Ding, D.; Bagul, A.; Ball, R.L.; Langlotz, C.; et al. CheXNet: Radiologist-level pneumonia detection on chest X-rays with deep learning. arXiv 2017, arXiv:1711.05225. [Google Scholar]
- Cherukuri, V.; Ssenyonga, P.; Warf, B.C.; Kulkarni, A.V.; Monga, V.; Schiff, S.J. Learning Based Segmentation of CT Brain Images: Application to Postoperative Hydrocephalic Scans. IEEE Trans. Biomed. Eng. 2018, 65, 1871–1884. [Google Scholar]
- Larson, D.B.; Chen, M.C.; Lungren, M.P.; Halabi, S.S.; Stence, N.V.; Langlotz, C.P. Performance of a Deep-learning neural network Model in assessing skeletal Maturity on Pediatric hand radiographs 1 PEDIATRIC IMAGING: Neural Network to Assess Skeletal Maturity on Pediatric Hand Radiographs Larson et al. Materials and Methods Data Acquisit. Radiology 2018, 287, 313–322. [Google Scholar] [CrossRef] [PubMed]
- Reismann, J.; Romualdi, A.; Kiss, N.; Minderjahn, M.I.; Kallarackal, J.; Schad, M.; Reismann, M. Diagnosis and classification of pediatric acute appendicitis by artificial intelligence methods: An investigator-independent approach. PLoS ONE 2019, 14, e0222030. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.; Chen, Y.; Yuan, M.; Gerstein, M.; Li, T.; Liang, H.; Froehlich, T.; Lu, L. The development of a practical artificial intelligence tool for diagnosing and evaluating autism spectrum disorder: Multicenter study. JMIR Med. Inform. 2020, 8, e15767. [Google Scholar] [CrossRef] [PubMed]
- He, L.; Li, H.; Dudley, J.A.; Maloney, T.C.; Brady, S.L.; Somasundaram, E.; Trout, A.T.; Dillman, J.R. Machine learning prediction of liver stiffness using clinical and T2-Weighted MRI radiomic data. Am. J. Roentgenol. 2019, 213, 592–601. [Google Scholar] [CrossRef] [PubMed]
- Hoshino, E.; Hayashi, K.; Suzuki, M.; Obatake, M.; Urayama, K.Y.; Nakano, S.; Taura, Y.; Nio, M.; Takahashi, O. An iPhone application using a novel stool color detection algorithm for biliary atresia screening. Pediatr. Surg. Int. 2017, 33, 1115–1121. [Google Scholar] [CrossRef] [PubMed]
- Angelico, R.; Liccardo, D.; Paoletti, M.; Pietrobattista, A.; Basso, M.S.; Mosca, A.; Safarikia, S.; Grimaldi, C.; Saffioti, M.C.; Candusso, M.; et al. A novel mobile phone application for infant stool color recognition: An easy and effective tool to identify acholic stools in newborns. J. Med. Screen. 2020, 28, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Zhou, W.; Yang, Y.; Yu, C.; Liu, J.; Duan, X.; Weng, Z.; Chen, D.; Liang, Q.; Qing, F.; Zhou, J.; et al. An ensembled deep learning model outperforms human experts in diagnosing biliary atresia from sonographic gallbladder images. medRxiv 2020, 12, 1259. [Google Scholar]
- Stanzione, A.; Ricciardi, C.; Cuocolo, R.; Romeo, V.; Petrone, J.; Sarnataro, M.; Mainenti, P.P.; Improta, G.; De Rosa, F.; Insabato, L.; et al. MRI Radiomics for the Prediction of Fuhrman Grade in Clear Cell Renal Cell Carcinoma: A Machine Learning Exploratory Study. J. Digit. Imaging 2020, 33, 879–887. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| # | Sex | Age (years) | Medical Status * | Laboratory Abnormalities ° | CLD Complications |
|---|---|---|---|---|---|
| 1 | M | 6 | Ideal | - | - |
| 2 | M | 13 | Ideal | - | - |
| 3 | F | 10 | Ideal | - | - |
| 4 | M | 9 | Ideal | - | - |
| 5 | F | 13 | Ideal | - | - |
| 6 | M | 6 | Ideal | - | - |
| 7 | M | 5 | Ideal | - | - |
| 8 | F | 9 | Ideal | - | - |
| 9 | M | 14 | Ideal | - | - |
| 10 | M | 11 | Non-ideal | AST, ALT, WBC, PLT | Portal hypertension, cholangitis |
| 11 | M | 9 | Non-ideal | AST, ALT, GGT, WBC, PLT | Portal hypertension |
| 12 | M | 25 | Non-ideal | TB, PLT | Portal hypertension |
| # | Sex | Age (years) | Medical Status at Initial Evaluation * | Laboratory Abnormalities at Re-Evaluation | CLD Complications at Re-Evaluation | Long-Term Medical Outcome |
|---|---|---|---|---|---|---|
| 1 | M | 13 | Ideal | TB | - | Non-ideal |
| 2 | M | 10 | Ideal | TB | - | Non-ideal |
| 3 | M | 12 | Ideal | TB | Cholangitis | Non-ideal |
| 4 | M | 5 | Ideal | ALT, PLT | - | Non-ideal |
| 5 | F | 14 | Ideal | TB | Cholangitis | Non-ideal |
| 6 | F | 6 | Ideal | WBC | - | Non-ideal |
| 7 | M | 6 | Non-ideal a | TB, PLT | Portal hypertension | Clinical progression |
| 8 | M | 5 | Non-ideal b | WBC | - | Clinical progression |
| 9 | F | 7 | Non-ideal c | AST, ALT, WBC, | - | Clinical progression |
| 10 | F | 10 | Non-ideal d | TB | - | Clinical progression |
| 11 | M | 7 | Non-ideal e | WBC | - | Clinical progression |
| 12 | F | 7 | Non-ideal f | TB | - | Clinical progression |
| - | Parameter | Group 1 (Mean ± SD) | Group 2 (Mean ± SD) | p-Value |
|---|---|---|---|---|
| Laboratory | AST (IU/L) | 31 ± 11 | 40 ± 25 | 0.443 |
| ALT (IU/L) | 29 ± 21 | 33 ± 20 | 0.291 | |
| GGT (IU/L) | 23 ± 19 | 25 ± 22 | 0.887 | |
| TB (mg/dL) | 0.38 ± 0.34 | 0.74 ± 0.25 | 0.001 | |
| DB (mg/dL) | 0.13 ± 0.09 | 0.29 ± 0.12 | 0.001 | |
| INR | 1.06 ± 0.07 | 1.12 ± 0.11 | 0.198 | |
| Albumin (g/dL) | 4.74 ± 0.24 | 4.44 ± 0.50 | 0.114 | |
| WBC (cells/mm3) | 6567 ± 2293 | 6122 ± 1873 | 0.551 | |
| PLT (cells/mm3) | 242083 ± 115800 | 188667 ± 93292 | 0.378 | |
| US | Portal vein (mm) | 9.75 ± 1.60 | 9.08 ± 2.11 | 0.932 |
| Liver diameter (mm) | 129.17 ± 23.53 | 114.00 ± 21.56 | 0.078 | |
| Spleen diameter (mm) | 118.00 ± 23.83 | 124.92 ± 25.65 | 0.443 | |
| Liver stiffness (kPa) | 5.95 ± 1.28 | 10.47 ± 7.32 | 0.020 | |
| MR | Portal vein (mm) | 9.92 ± 1.38 | 8.75 ± 2.05 | 0.198 |
| Liver volume (cm3) | 923.46 ± 250.47 | 823.97 ± 282.75 | 0.242 | |
| Spleen volume (cm3) | 300.64 ± 199.82 | 356.17 ± 142.86 | 0.198 |
| Algorithms | Accuracy (%) | Sensitivity (%) | Specificity (%) | AUCROC |
|---|---|---|---|---|
| RF | 95.8 | 95.8 | 95.8 | 0.991 |
| NB | 72.9 | 62.5 | 83.3 | 0.866 |
| kNN | 93.8 | 91.7 | 95.8 | 0.997 |
| SVM | 89.6 | 87.5 | 91.7 | 0.896 |
| Mean performance | 88.0 | 84.4 | 91.7 | 0.937 |
| Algorithms | Accuracy (%) | Sensitivity (%) | Specificity (%) | AUCROC |
|---|---|---|---|---|
| RF | 79.2 | 79.2 | 79.2 | 0.868 |
| NB | 64.6 | 41.7 | 87.5 | 0.642 |
| kNN | 79.2 | 70.8 | 87.5 | 0.818 |
| SVM | 75.0 | 70.8 | 79.2 | 0.750 |
| Mean performance | 74.5 | 65.6 | 83.4 | 0.769 |
| Algorithms | Accuracy (%) | Sensitivity (%) | Specificity (%) | AUCROC |
|---|---|---|---|---|
| RF | 79.2 | 79.2 | 79.2 | 0.878 |
| NB | 60.4 | 41.7 | 79.2 | 0.677 |
| kNN | 83.3 | 83.3 | 83.3 | 0.908 |
| SVM | 83.3 | 83.3 | 83.3 | 0.833 |
| Mean performance | 76.6 | 71.9 | 81.3 | 0.824 |
| Algorithms | Accuracy | Sensitivity | Specificity | AUCROC | Features Selected |
|---|---|---|---|---|---|
| RF | 100 | 100 | 100 | 1 | TB, US liver diameter, MR portal vein diameter |
| NB | 100 | 100 | 100 | 1 | TB, DB |
| kNN | 100 | 100 | 100 | 1 | TB, DB, WBC, US Stiffness, MR portal vein diameter |
| SVM | 93.3 | 100 | 87.5 | 0.938 | TB, INR |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caruso, M.; Ricciardi, C.; Delli Paoli, G.; Di Dato, F.; Donisi, L.; Romeo, V.; Petretta, M.; Iorio, R.; Cesarelli, G.; Brunetti, A.; et al. Machine Learning Evaluation of Biliary Atresia Patients to Predict Long-Term Outcome after the Kasai Procedure. Bioengineering 2021, 8, 152. https://doi.org/10.3390/bioengineering8110152
Caruso M, Ricciardi C, Delli Paoli G, Di Dato F, Donisi L, Romeo V, Petretta M, Iorio R, Cesarelli G, Brunetti A, et al. Machine Learning Evaluation of Biliary Atresia Patients to Predict Long-Term Outcome after the Kasai Procedure. Bioengineering. 2021; 8(11):152. https://doi.org/10.3390/bioengineering8110152
Chicago/Turabian StyleCaruso, Martina, Carlo Ricciardi, Gregorio Delli Paoli, Fabiola Di Dato, Leandro Donisi, Valeria Romeo, Mario Petretta, Raffaele Iorio, Giuseppe Cesarelli, Arturo Brunetti, and et al. 2021. "Machine Learning Evaluation of Biliary Atresia Patients to Predict Long-Term Outcome after the Kasai Procedure" Bioengineering 8, no. 11: 152. https://doi.org/10.3390/bioengineering8110152