1. Introduction
Especially in the case of complicated bone fractures, a simple plaster cast is often not enough to ensure good stiffening of the bone fragments. In such cases, a procedure called osteosynthesis, which serves to fix the individual fracture fragments to each other again in their original position and to re-stabilize the bone that has become unstable due to the fracture is used [
1,
2]. Typical areas of application are the stabilization of bones after fractures, stiffening operations on joints (arthrodesis) or on the spine (spondylodesis) and after osteotomy, a surgical technique in which bones are specifically cut to correct misalignments, e.g., the correction of hallux valgus [
3,
4]. The aim of osteosynthesis is therefore a stable fixation of the bone fragments to ensure a good healing of the fracture, to avoid of misalignments and to allow a partial or complete loading of the treated bones for an early functional post-treatment.
Osteosynthesis is done by surgical implementation of implants. Nowadays, a large number of various implants and techniques are available [
5,
6,
7,
8,
9]. The focus in this paper is the screw osteosynthesis.
Table 1 gives a short overview of the remaining types of osteosynthesis. In screw osteosynthesis, the bone fragments are fixed with screws [
10,
11] and are mostly based on the lag screw principal [
12]. Here, the screw thread only engages the fracture part far from the head, while the screw slides freely in the bone near the head. This anchorage of the screw leads to the desired compression of the fragments [
13,
14]. This technique is often used for fractures close to a joint and for osteotomies in the forefoot. Today, many different screws are available, e.g., the Herbert screw, which creates the necessary compression by using two different thread pitches [
15,
16,
17]. Besides lag screws, position screws are also used [
18,
19]. With position screws, a thread is cut in all fragments and thus the fragments are held in position without compression.
These screws are typically made of stainless steel [
20], titanium [
21,
22,
23] or biodegradable/bioabsorbable synthetic materials [
24,
25,
26,
27,
28,
29]. The advantages of screws made of bioabsorbable material include no implant removal required, no interference with MRI and no interference with future revision surgery if required. A major disadvantage of biodegradable screws is failure during insertion due to less stability compared to metal screws, e.g., in anterior cruciate ligament (ACL) reconstruction [
30,
31]. Furthermore, in some cases a foreign body reaction may occur [
32].
Table 1.
Overview of the remaining types of osteosynthesis.
Table 1.
Overview of the remaining types of osteosynthesis.
| Types of Osteosynthesis | Description |
|---|
| Kirschner-wire osteosynthesis | After reposition, the bone fragments are fixed with K-wires [33]. This type of osteosynthesis is suitable for fractures of small bones [34,35]. |
| Tension-belt osteosynthesis | The principal of the tension-belt osteosynthesis is based on the fundamentals of reinforced concrete construction. In osteosynthesis, the compressive-resistant bone is combined with a tension-resistant wire [36,37,38]. |
| Intramedullary nail osteosynthesis | In this method, a nail is placed intramedullary in the centre of the fractured bone and therefore it is a very load-table treatment for bone fractures [39,40,41,42]. |
| Compound osteosynthesis | Due to osteoporosis, the fixation strength of implants is often drastically reduced. To increase stability, the principal of augmentation is applied [43]. In this process, areas with low bone density are filled with special bone cements to prevent the implant from breaking out [44,45]. |
| External fixation | External fixation is primarily used for temporary stabilization of polytraumatized patients. In contrast to the other methods described, external fixation uses wires or screws that are attached to the bone fragments from the outside. [46,47,48]. |
| Plate osteosynthesis | In plate osteosynthesis, a plate adapted to the size of the bone is placed over the exposed fracture and attached to all bone fragments with screws. This is how the plate provides stabilization of the bone [49,50,51]. |
Besides metal or biodegradable materials, such screws can also be made from cortical human donor bone [
52]. These allogenic screws have very good osteoconductive properties and are therefore vascularized after 6 weeks and no longer visible on X-ray after 1 year [
53,
54]. These screws can be used as position screws for osteotomies, e.g., in hand, foot and knee surgery or as anchor screws for sutures and tendons and are available from 3.5 mm to 5 mm [
53]. One can imagine that it is difficult to manufacture conventional screw drives like cross slot, hexalobular or internal hexagon in cortical bone screws as small micro cutters are required. Therefore, an easily manufacturable screw drive is needed for allogenic cortical bone screws. Common drives in allogenic bone screws are, on the one hand, an external hexagon, which is robust and easy to manufacture, but does not allow the screw to be screwed in completely. The other is a type of claw clutch, which is also easy to manufacture and allows a the screw to be screwed in completely, but the threads are interrupted in the area of the driver [
53].
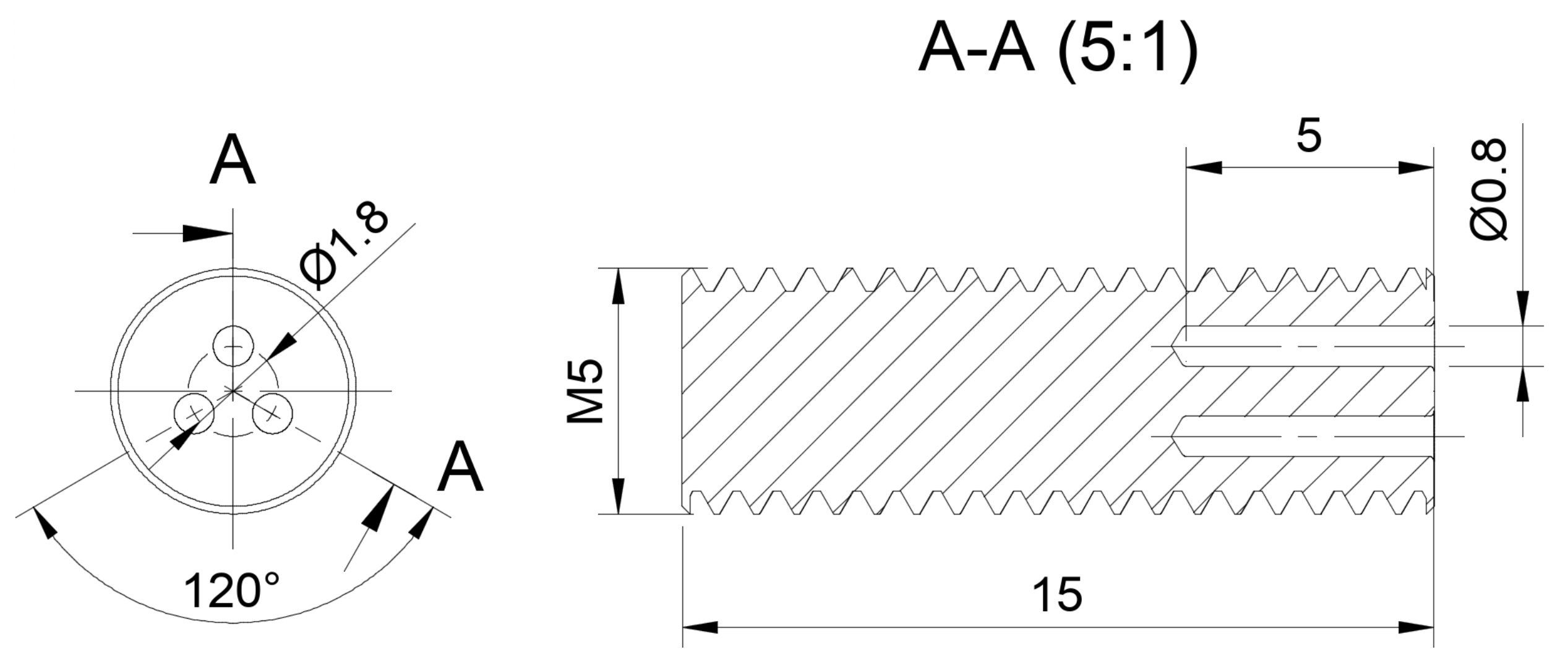
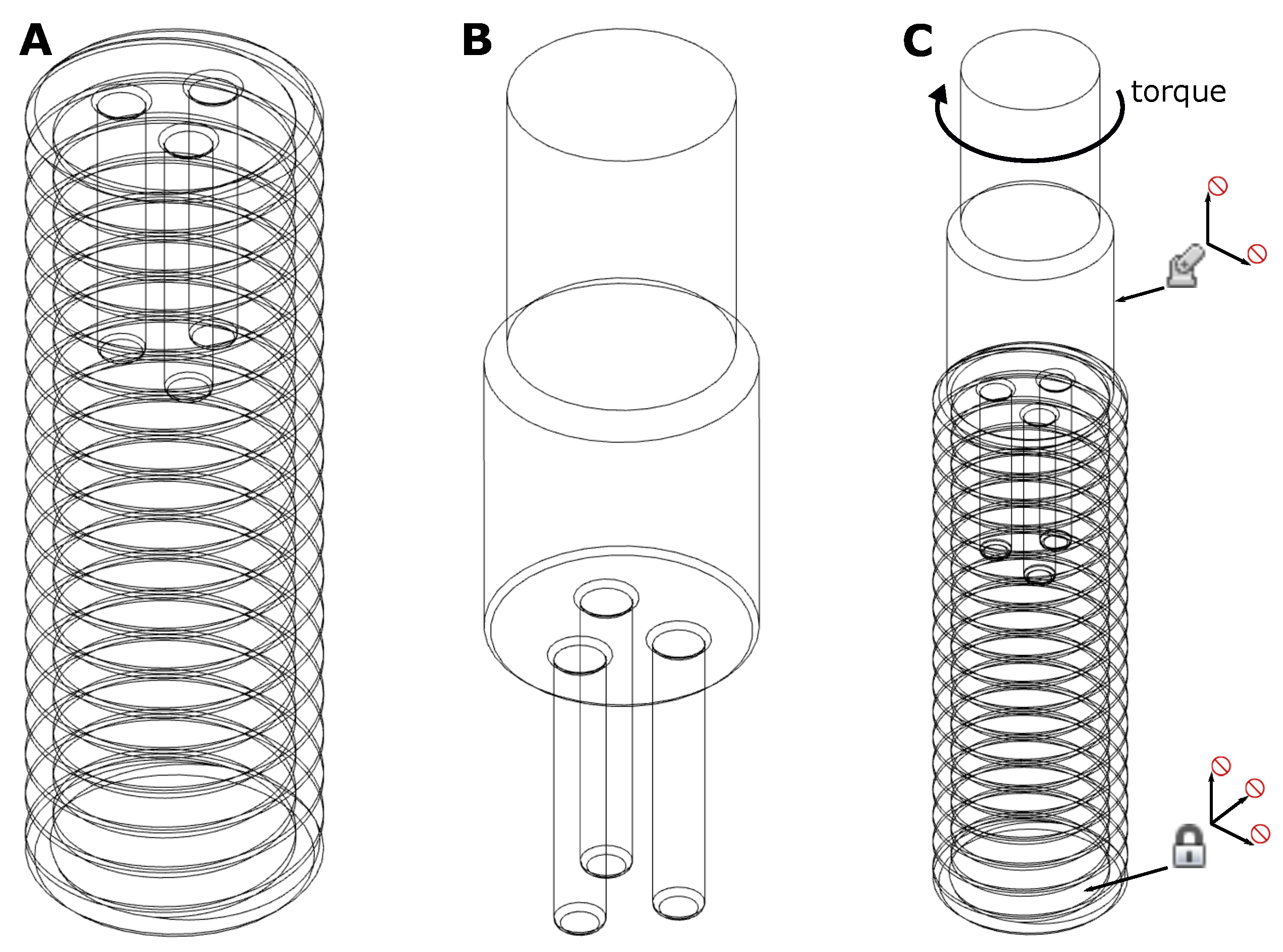
In this paper we introduce a novel, easy-to-manufacture screw drive for allogenic headless bone screws made of cortical human bone, which is fully internal and thus allows the screw to be fully inserted and has a thread along its entire length. In order to evaluate the strength of this drive, we performed simulations using the Finite-Element method (FEM) [
55,
56,
57,
58,
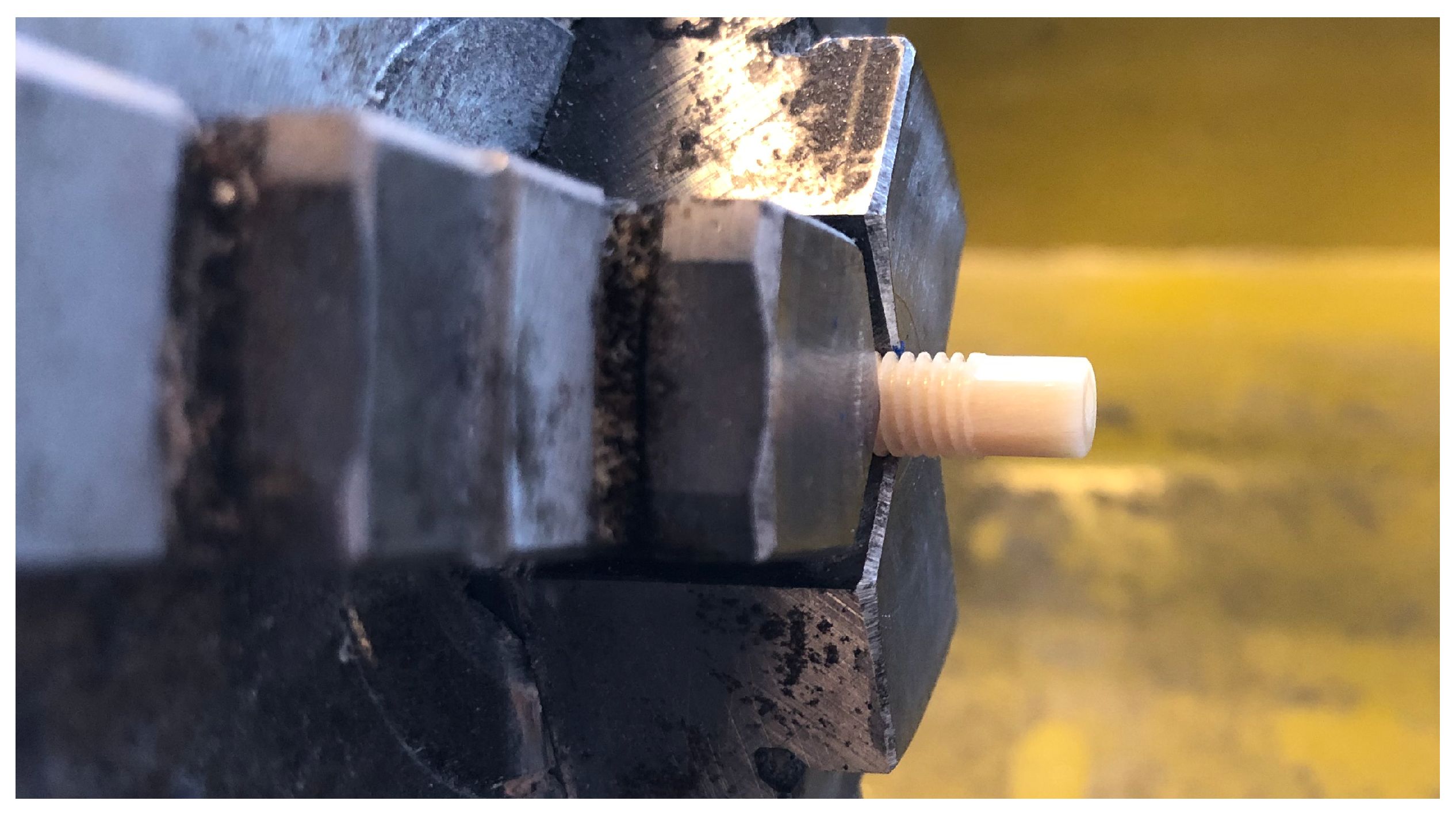
59]. Furthermore, we validated the simulation using a screw made of human cortical donor bone produced by Surgebright (Neulichtenberg, Austria) [
53]. Finally, we tested the novel screw drive experimentally on custom-made prototypes and compared the simulation results of the novel drive with simulation results of conventional drives. The validation of the simulation gave good results, so that the FEM-simulation allowed a fairly accurate prediction at which load and at which point the screw was likely to break. Compared to other conventional screw drives, the drive presented here has similar strength and is easy to manufacture.
4. Discussion
In this paper we describe a simple screw drive for use in allogenic headless position screws made of human cortical bone. The screw drive is completely internal, i.e., no threads are removed, and it allows the screw to be fully inserted. Since it consists of only simple bores, this drive is easy to manufacture, which is crucial for allogenic screws.
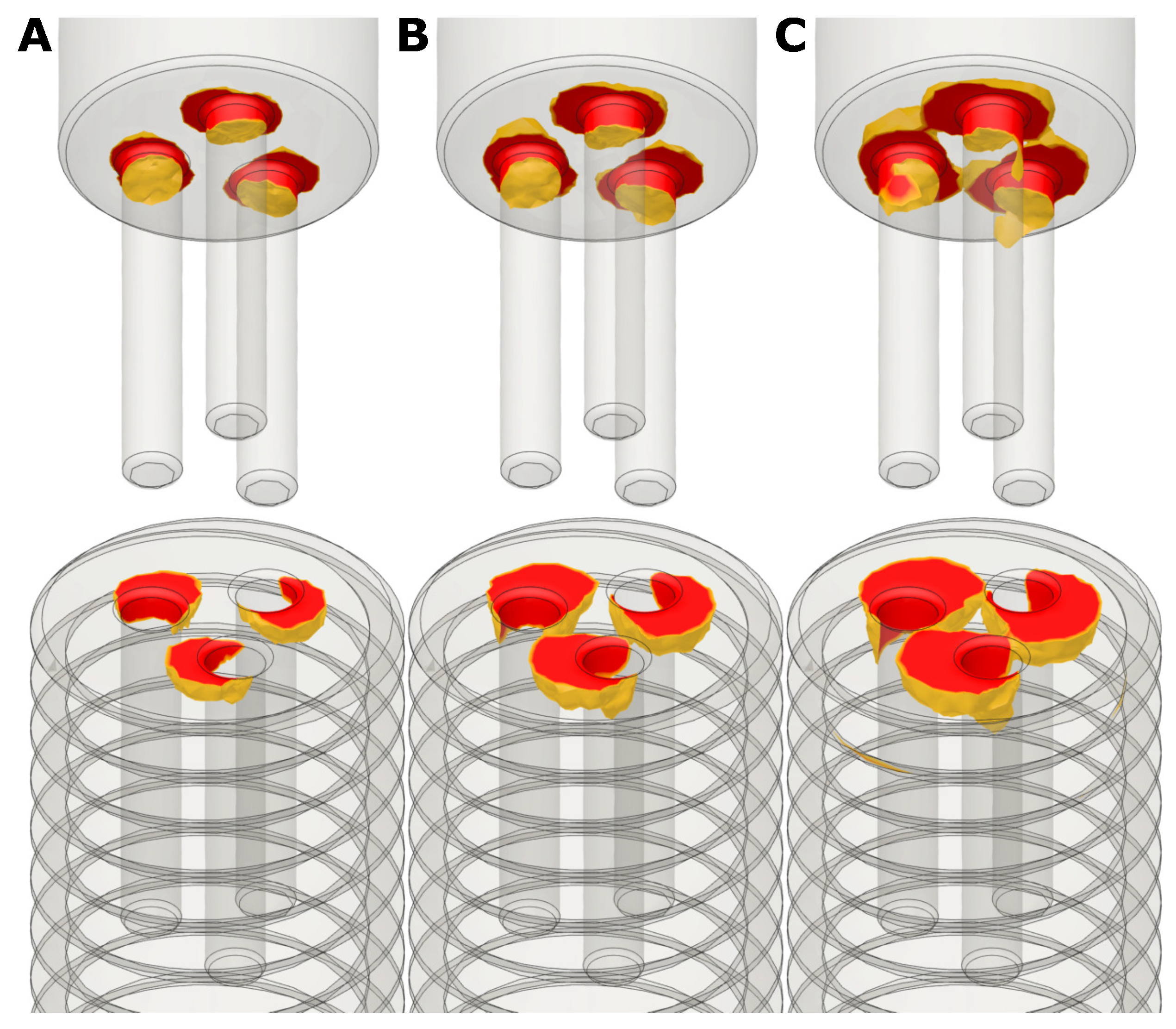
In order to investigate the stability of the presented 3-bore drive, we performed simulations using the Finite-Element method. For simplicity, a linear, isotropic FEM was used. Since we want to find the torque that the screw can just withstand, i.e., the yield point should not be reached, we remain in the linear range of the stress-strain diagram. This approach is therefore a good approximation [
62]. Nevertheless, a non-linear, orthotropic FEM-study would probably provide more accurate results and reduce singularities. However, the problem to be solved would be much more complex and therefore require more computing power. Furthermore, the simulation software used, Autodesk Fusion 360, does not support orthotropic materials in an FEM study.The comparison between simulation and experiment has shown that this approach is a sufficiently good approximation.
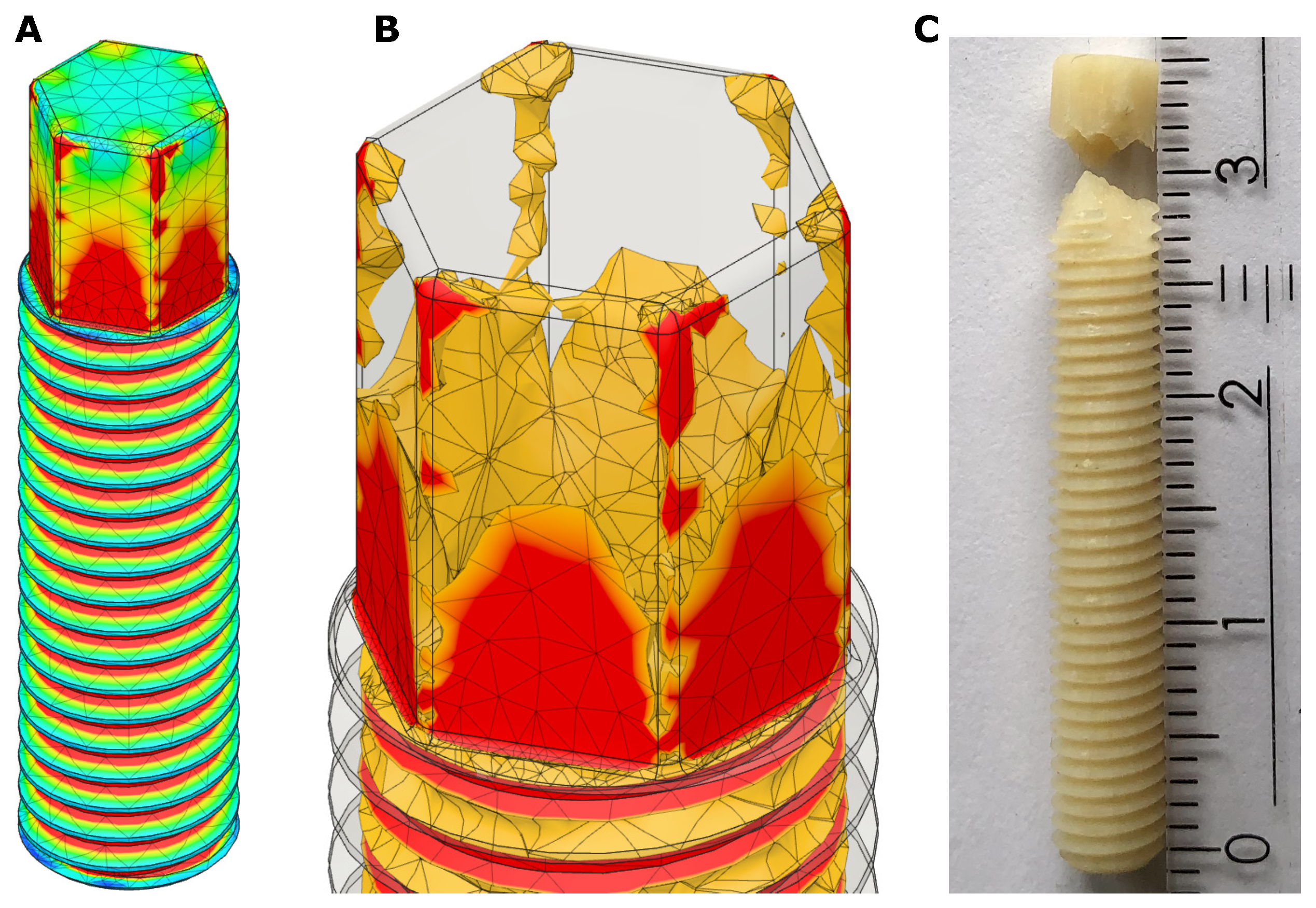
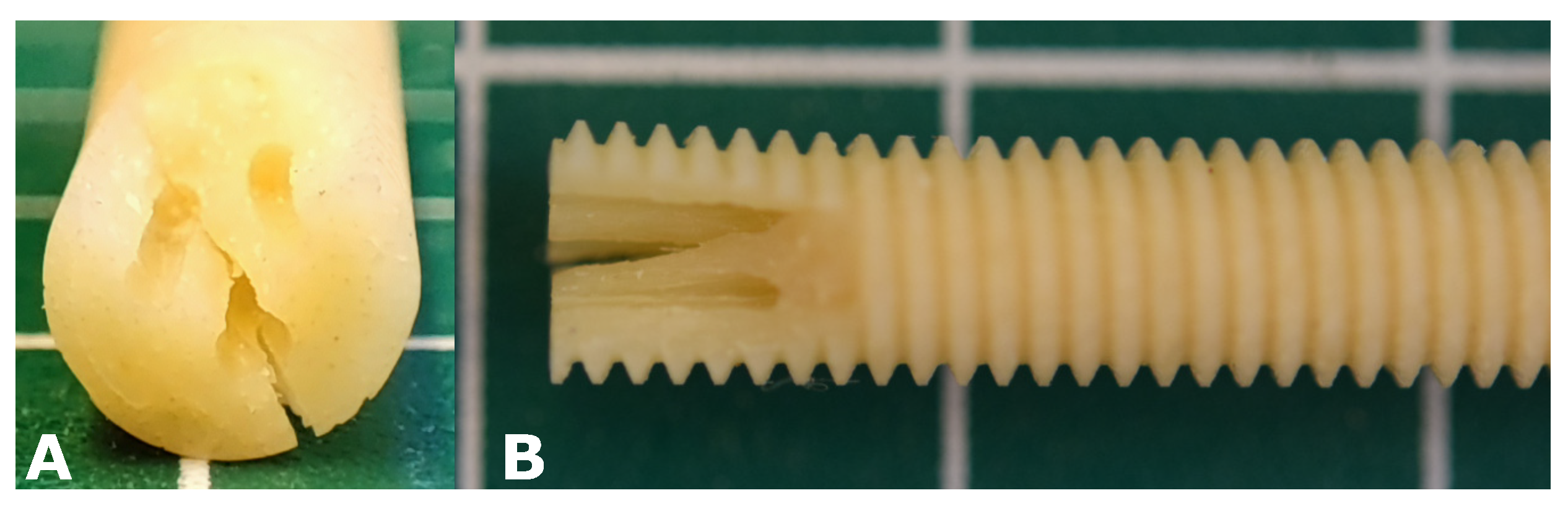
Since the problem investigated is a so-called contact problem, singularities occur at the contact points between screw and insertion tool and at edges with small radius. The stresses at these points are unrealistic high and therefore the maximum stress values were not considered. Here it is more important to see how far very high stresses extend over the component to get an impression of the stability. A validation of the simulation with a real prototype screw showed that the simulation reproduces the real behaviour well. One can conclude, that or simulation allows a fairly good estimation at which torque and at witch point the screw will fail.
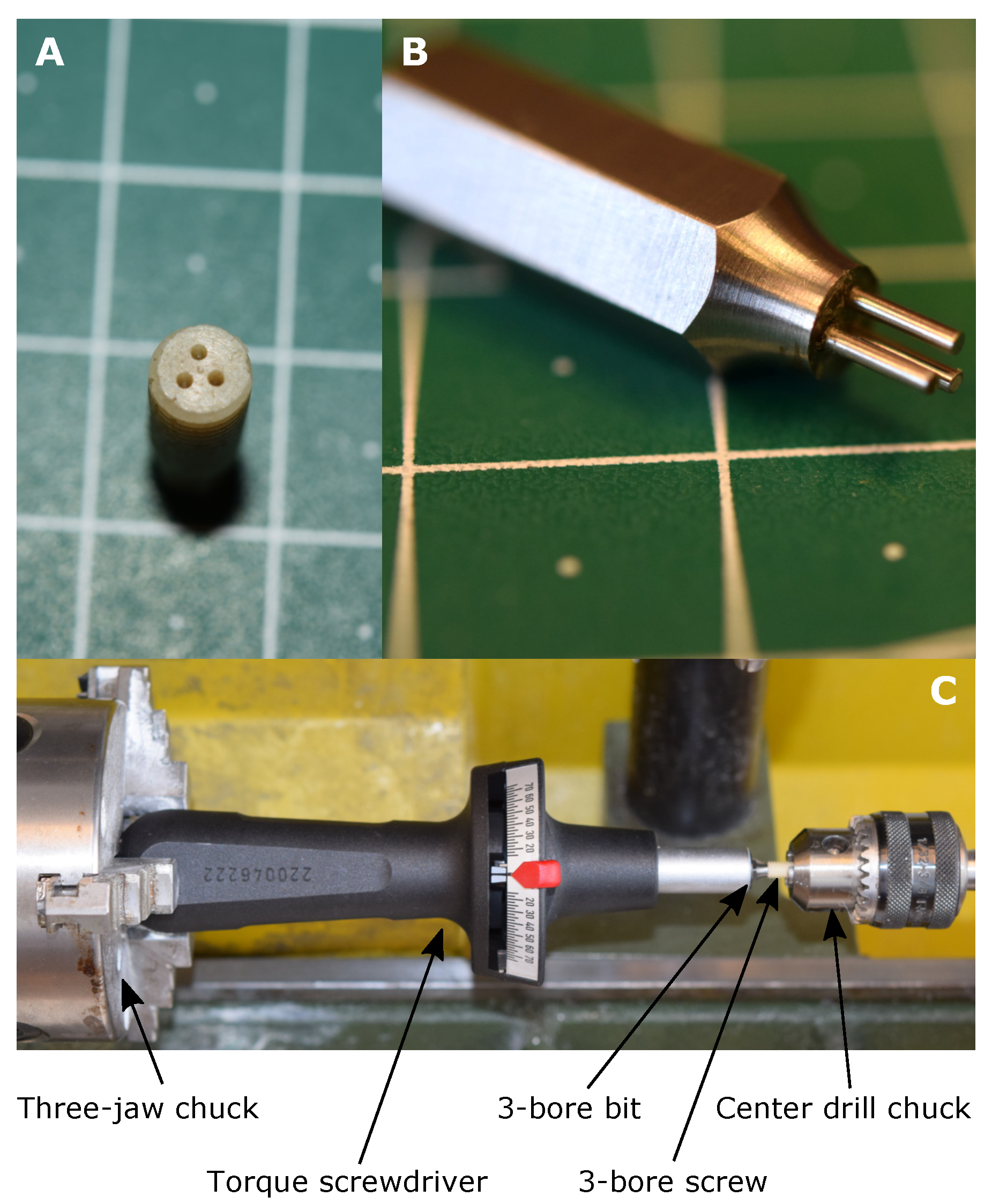
In addition to the FEM simulations of the 3-bore drive, an experimental verification was carried out using custom-made prototype screws made from human cortical bone. The FEM-simulation predicted a failure torque between 200 Nmm and 300 Nmm, the experimentally determined failure torque is 232.5 Nmm, so it can be concluded that the results of the simulation and the experiment match very well. However, the mean experimental failure torque of 232.5 Nmm is in the lower range of the prediction of the simulation.
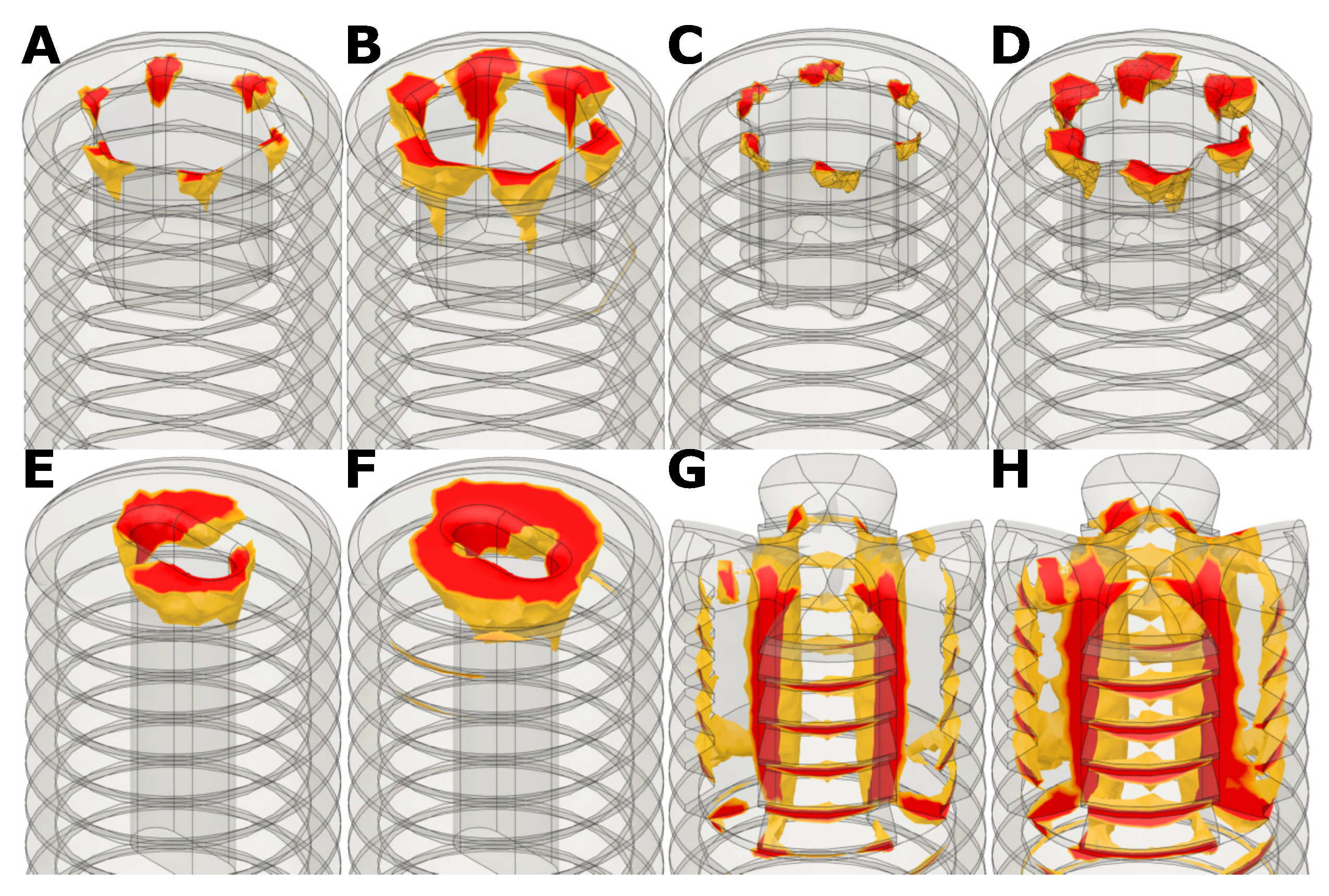
Comparisons of simulations with conventional screw drives showed, that the 3-bore drive has similar failure torques when used in allogenic cortical screws. The advantage of the 3-bore drive in allogenic screws is the simple manufacturing process. As one can imagine, it is difficult to manufacture a hex key drive or a hexalobular drive in cortical bone because the manufacturing process requires small and fragile micro cutters to achieve small radii e.g., for the hexalobular (Torx) drive. Therefore, the manufacturing process for conventional screw drives in cortical bone is difficult and time consuming.
The absolute value of the failure torque of the 3-bore drive is not very high at approximately 200 Nmm to 300 Nmm, since these screws are used as position screws, i.e., the screw is turned into a pre-cut thread, the occurring torques are rather low. Nevertheless, caution should be exercised when screwing in a screw with the suggested 3-bore drive.
We focused on screws with a diameter of 5 mm as this is the minimal diameter where this screw drive works properly. If the diameter gets smaller, there is not enough material inside the screw. A screw size of 5 mm is common for allogenic bone screws [
53]. One can imagine that the 3-bore drive becomes more effective if the screw diameter is increased because there is more material inside the screw. The reasonable maximum screw size is about 8 mm, as the cortical portion of the raw bone is too thin for larger screw sizes. For an 8 mm screw with 1.5 mm bores, the simulated failure torque would be about 1200 Nmm. Therefore, the 3-bore drive represents a very stable, fully internal screw drive especially for larger, e.g., 8 mm, allogenic bone screws that can be used e.g., for fixation of a tendon graft where higher failure torques are required.
Furthermore, it must be emphasized that the proposed 3-bore drive is only intended for use in allogenic screws made of cortical bone. The 3-bore drive is not suitable for screws made of stainless steel, titanium or synthetic material, as conventional drives have better performance and are more stable.
Finally,
Table 6 gives a brief overview over all presented screw drives regarding torque, manufacturing and the possibility of full screw-in. Compared to the external hexagon or the claw clutch, the 3-bore drive has a lower failure torque, but the external hexagon does not allow the screw to be fully screwed in. The claw clutch allows the screw to be fully screwed in, but part of the thread is removed, which is not the case with the 3-bore drive. The internal hexagon and the hexalobular drive have a similar failure torque, but are very difficult to produce in a cortical bone screw. The slot drive allows for complete screw-in and is also easy to manufacture, but the failure torque is lower compared to the other drives.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}







