
Altered Functional Connectivity of Temporoparietal Lobe in Obstructive Sleep Apnea: A Resting-State fNIRS Study
 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
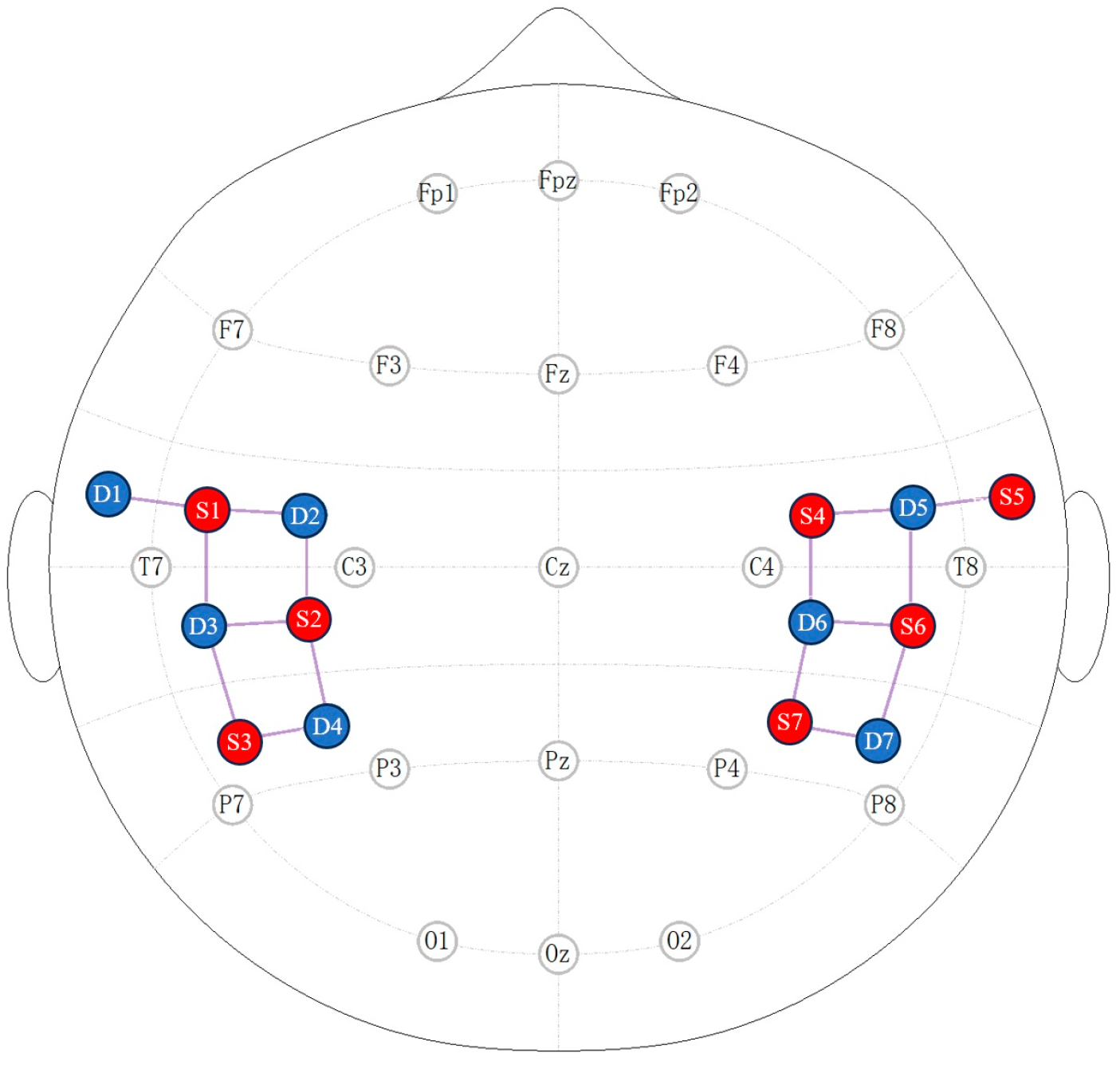
2.2. fNIRS Recording
2.3. Data Analysis
2.3.1. Preprocessing
2.3.2. Functional Connectivity
2.3.3. Graph Theory Analysis
2.3.4. Statistical Analysis
3. Results
3.1. Demographic Characteristics
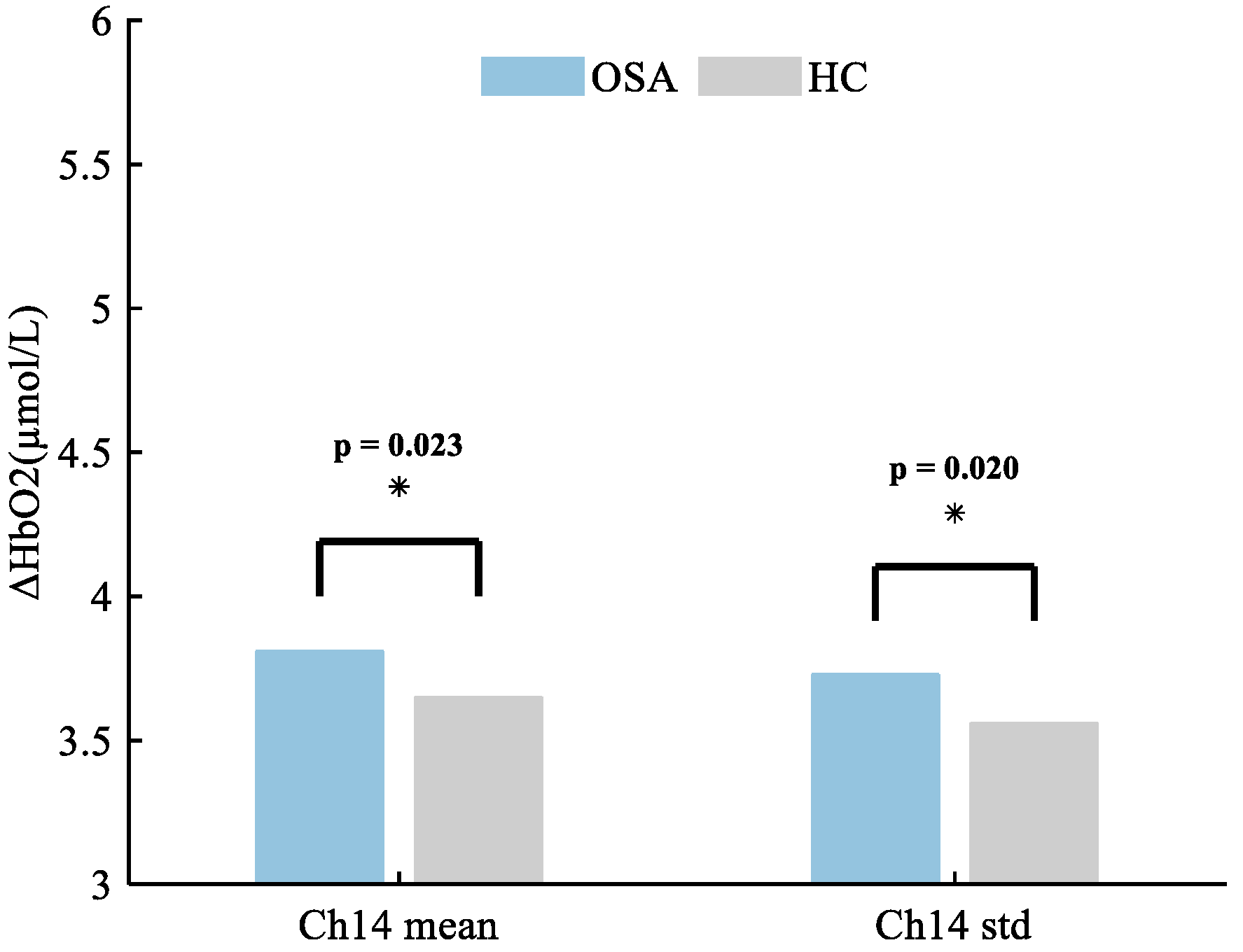
3.2. Changes in HbO2 Concentration between Patients with OSA and HCs
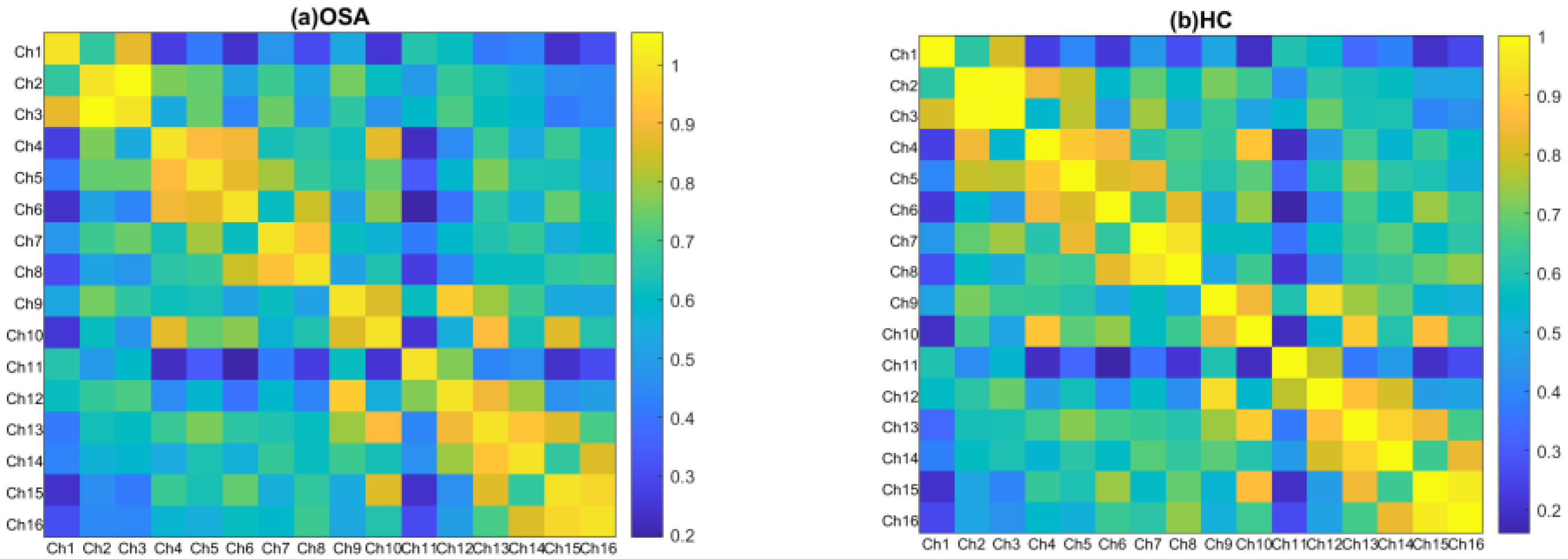
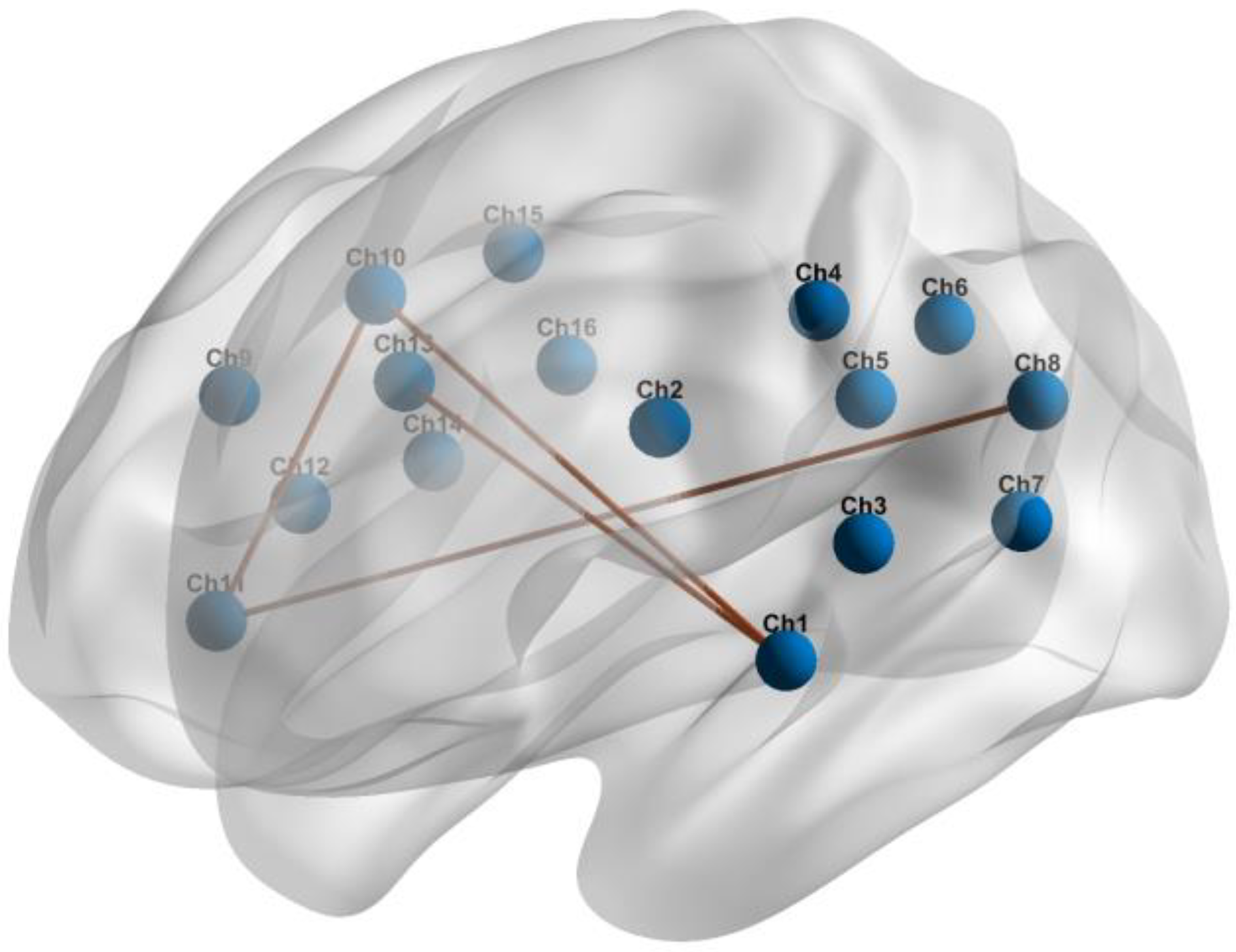
3.3. RSFC within the Temporoparietal Network between Patients with OSA and HCs
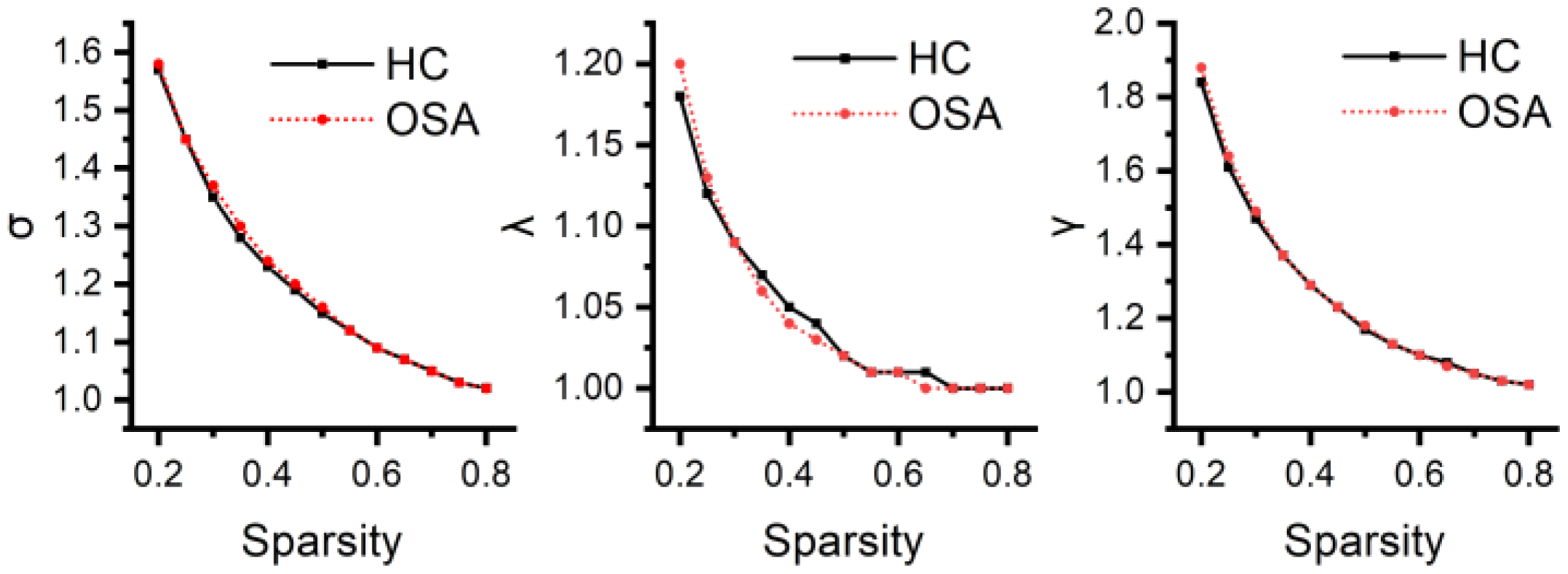
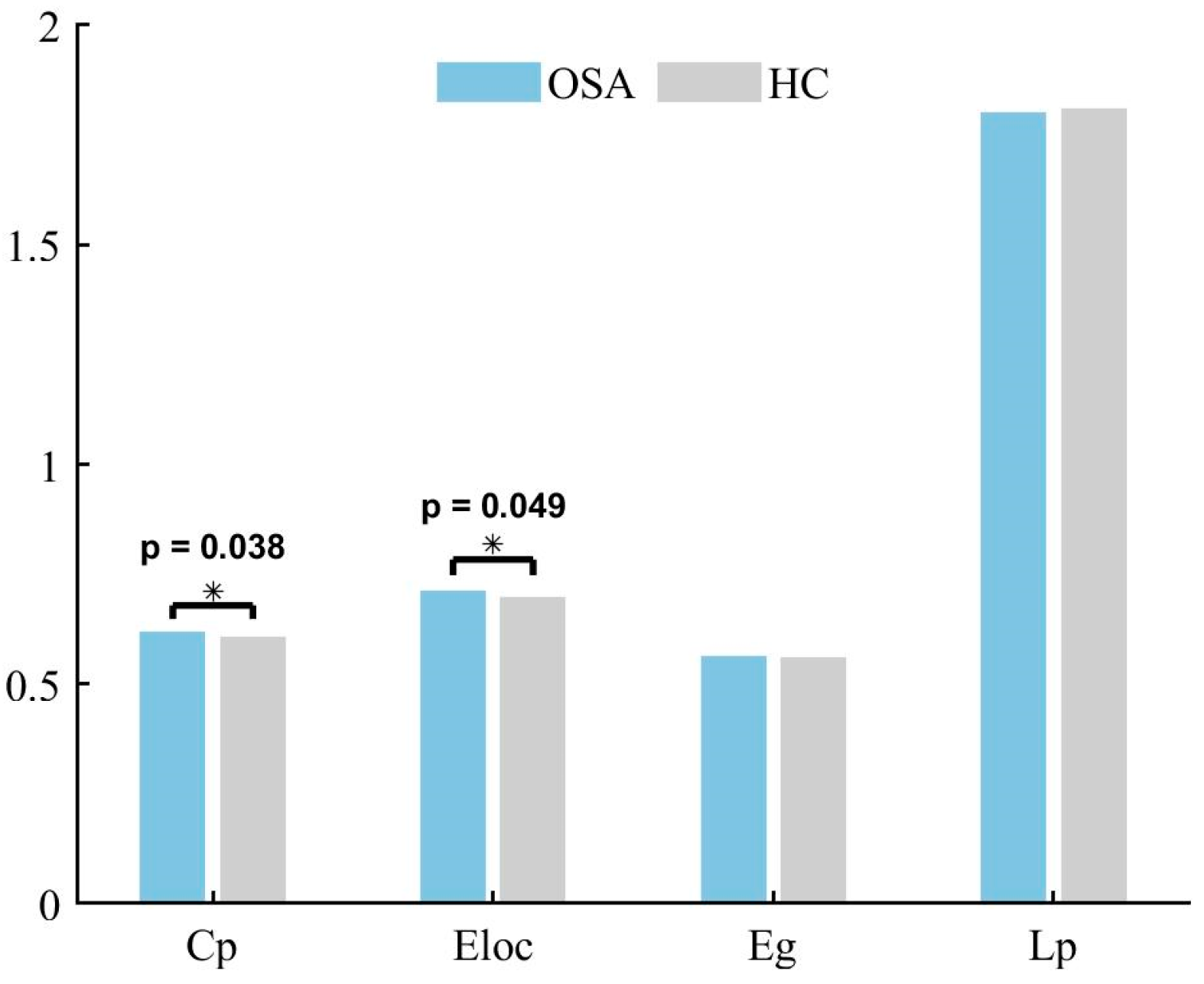
3.4. Differences in Global Network Metrics of the Temporoparietal Network
3.5. Differences in Regional Network Metrics of the Temporoparietal Network
3.6. Correlations between RSFC and AHI
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Young, T. Risk Factors for Obstructive Sleep Apnea in Adults. JAMA 2004, 291, 2013–2016. [Google Scholar] [CrossRef] [PubMed]
- Garbarino, S.; Bardwell, W.A.; Guglielmi, O.; Chiorri, C.; Bonanni, E.; Magnavita, N. Association of Anxiety and Depression in Obstructive Sleep Apnea Patients: A Systematic Review and Meta-Analysis. Behav. Sleep Med. 2020, 18, 35–57. [Google Scholar] [CrossRef] [PubMed]
- Franklin, K.A.; Lindberg, E. Obstructive Sleep Apnea Is a Common Disorder in the Population—A Review on the Epidemiology of Sleep Apnea. J. Thorac. Dis. 2015, 7, 1311–1322. [Google Scholar] [PubMed]
- Kario, K. Obstructive Sleep Apnea Syndrome and Hypertension: Ambulatory Blood Pressure. Hypertens. Res. 2009, 32, 428–432. [Google Scholar] [CrossRef] [PubMed]
- Somers, V.K.; White, D.P.; Amin, R.; Abraham, W.T.; Costa, F.; Culebras, A.; Daniels, S.; Floras, J.S.; Hunt, C.E.; Olson, L.J.; et al. Sleep Apnea and Cardiovascular Disease: An American Heart Association/American College of Cardiology Foundation Scientific Statement from the American Heart Association Council for High Blood Pressure Research Professional Education Committee, Council on Clinical Cardiology, Stroke Council, and Council on Cardiovascular Nursing in Collaboration with the National Heart, Lung, and Blood Institute National Center on Sleep Disorders Research (National Institutes of Health). Circulation 2008, 118, 1080–1111. [Google Scholar] [CrossRef] [PubMed]
- Bubu, O.M.; Andrade, A.G.; Umasabor-Bubu, O.Q.; Hogan, M.M.; Turner, A.D.; de Leon, M.J.; Ogedegbe, G.; Ayappa, I.; Jean-Louis G, G.; Jackson, M.L.; et al. Obstructive Sleep Apnea, Cognition and Alzheimer’s Disease: A Systematic Review Integrating Three Decades of Multidisciplinary Research. Sleep Med. Rev. 2020, 50, 101250. [Google Scholar] [CrossRef] [PubMed]
- Caporale, M.; Palmeri, R.; Corallo, F.; Muscarà, N.; Romeo, L.; Bramanti, A.; Marino, S.; Lo Buono, V. Cognitive Impairment in Obstructive Sleep Apnea Syndrome: A Descriptive Review. Sleep Breath. 2021, 25, 29–40. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Tang, S.; Lyu, X.; Yang, C.; Chen, X. Structural and Functional Brain Alterations in Obstructive Sleep Apnea: A Multimodal Meta-Analysis. Sleep Med. 2019, 54, 195–204. [Google Scholar] [CrossRef]
- Tahmasian, M.; Rosenzweig, I.; Eickhoff, S.B.; Sepehry, A.A.; Laird, A.R.; Fox, P.T.; Morrell, M.J.; Khazaie, H.; Eickhoff, C.R. Structural and Functional Neural Adaptations in Obstructive Sleep Apnea: An Activation Likelihood Estimation Meta-Analysis. Neurosci. Biobehav. Rev. 2016, 65, 142–156. [Google Scholar] [CrossRef]
- Baril, A.-A.; Martineau-Dussault, M.-È.; Sanchez, E.; André, C.; Thompson, C.; Legault, J.; Gosselin, N. Obstructive Sleep Apnea and the Brain: A Focus on Gray and White Matter Structure. Curr. Neurol. Neurosci. Rep. 2021, 21, 11. [Google Scholar] [CrossRef]
- Taylor, K.S.; Millar, P.J.; Murai, H.; Haruki, N.; Kimmerly, D.S.; Bradley, T.D.; Floras, J.S. Cortical Autonomic Network Gray Matter and Sympathetic Nerve Activity in Obstructive Sleep Apnea. Sleep 2018, 41, zsx208. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.-L.; Lu, C.-H.; Lin, H.-C.; Chen, P.-C.; Chou, K.-H.; Lin, W.-M.; Tsai, N.-W.; Su, Y.-J.; Friedman, M.; Lin, C.-P.; et al. White Matter Damage and Systemic Inflammation in Obstructive Sleep Apnea. Sleep 2015, 38, 361–370. [Google Scholar] [CrossRef]
- Brain Structural Changes in Obstructive Sleep Apnea. Sleep 2008, 31, 967–977. [CrossRef]
- Zacharias, H.U.; Weihs, A.; Habes, M.; Wittfeld, K.; Frenzel, S.; Rashid, T.; Stubbe, B.; Obst, A.; Szentkirályi, A.; Bülow, R.; et al. Association between Obstructive Sleep Apnea and Brain White Matter Hyperintensities in a Population-Based Cohort in Germany. JAMA Netw. Open 2021, 4, e2128225. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Yun, C.-H.; Thomas, R.J.; Lee, S.H.; Seo, H.S.; Cho, E.R.; Lee, S.K.; Yoon, D.W.; Suh, S.; Shin, C. Obstructive Sleep Apnea as a Risk Factor for Cerebral White Matter Change in a Middle-Aged and Older General Population. Sleep 2013, 36, 709–715. [Google Scholar] [CrossRef] [PubMed]
- Joo, E.Y.; Tae, W.S.; Lee, M.J.; Kang, J.W.; Park, H.S.; Lee, J.Y.; Suh, M.; Hong, S.B. Reduced Brain Gray Matter Concentration in Patients with Obstructive Sleep Apnea Syndrome. Sleep 2010, 33, 235–241. [Google Scholar] [CrossRef]
- Rosenzweig, I.; Glasser, M.; Crum, W.R.; Kempton, M.J.; Milosevic, M.; McMillan, A.; Leschziner, G.D.; Kumari, V.; Goadsby, P.; Simonds, A.K.; et al. Changes in Neurocognitive Architecture in Patients with Obstructive Sleep Apnea Treated with Continuous Positive Airway Pressure. EBioMedicine 2016, 7, 221–229. [Google Scholar] [CrossRef]
- Canessa, N.; Castronovo, V.; Cappa, S.F.; Aloia, M.S.; Marelli, S.; Falini, A.; Alemanno, F.; Ferini-Strambi, L. Obstructive Sleep Apnea: Brain Structural Changes and Neurocognitive Function before and after Treatment. Am. J. Respir. Crit. Care Med. 2011, 183, 1419–1426. [Google Scholar] [CrossRef]
- Hu, Z.; Liu, G.; Dong, Q.; Niu, H. Applications of Resting-State fNIRS in the Developing Brain: A Review from the Connectome Perspective. Front. Neurosci. 2020, 14, 476. [Google Scholar] [CrossRef]
- Li, S.; Hu, N.; Zhang, W.; Tao, B.; Dai, J.; Gong, Y.; Tan, Y.; Cai, D.; Lui, S. Dysconnectivity of Multiple Brain Networks in Schizophrenia: A Meta-Analysis of Resting-State Functional Connectivity. Front. Psychiatry 2019, 10, 482. [Google Scholar] [CrossRef]
- Pinti, P.; Tachtsidis, I.; Hamilton, A.; Hirsch, J.; Aichelburg, C.; Gilbert, S.; Burgess, P.W. The Present and Future Use of Functional Near-infrared Spectroscopy (fNIRS) for Cognitive Neuroscience. Ann. N. Y. Acad. Sci. 2020, 1464, 5–29. [Google Scholar] [CrossRef] [PubMed]
- Kong, L.; Li, H.; Shu, Y.; Liu, X.; Li, P.; Li, K.; Xie, W.; Zeng, Y.; Peng, D. Aberrant Resting-State Functional Brain Connectivity of Insular Subregions in Obstructive Sleep Apnea. Front. Neurosci. 2022, 15, 765775. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Chen, L.; Duan, W.; Li, H.; Kong, L.; Shu, Y.; Li, P.; Li, K.; Xie, W.; Zeng, Y.; et al. Abnormal Functional Connectivity of Hippocampal Subdivisions in Obstructive Sleep Apnea: A Resting-State Functional Magnetic Resonance Imaging Study. Front. Neurosci. 2022, 16, 850940. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.; Chen, L.; Li, H.; Xin, H.; Zhang, J.; Wei, Z.; Peng, D. Abnormal Resting-State Functional Connectivity of Amygdala Subregions in Patients with Obstructive Sleep Apnea. Neuropsychiatr. Dis. Treat. 2019, 15, 977–987. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.; Liu, G.; Luo, H.; Li, H.; Peng, Y.; Zong, D.; Ouyang, R. Aberrant Hippocampal Network Connectivity Is Associated with Neurocognitive Dysfunction in Patients with Moderate and Severe Obstructive Sleep Apnea. Front. Neurol. 2020, 11, 580408. [Google Scholar] [CrossRef] [PubMed]
- Archbold, K.H.; Borghesani, P.R.; Mahurin, R.K.; Kapur, V.K.; Landis, C.A. Neural Activation Patterns during Working Memory Tasks and OSA Disease Severity: Preliminary Findings. J. Clin. Sleep Med. 2009, 5, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Kheirandish-Gozal, L.; Yoder, K.; Kulkarni, R.; Gozal, D.; Decety, J. Preliminary Functional MRI Neural Correlates of Executive Functioning and Empathy in Children with Obstructive Sleep Apnea. Sleep 2014, 37, 587–592. [Google Scholar] [CrossRef] [PubMed]
- Prilipko, O.; Huynh, N.; Schwartz, S.; Tantrakul, V.; Kim, J.H.; Peralta, A.R.; Kushida, C.; Paiva, T.; Guilleminault, C. Task Positive and Default Mode Networks during a Parametric Working Memory Task in Obstructive Sleep Apnea Patients and Healthy Controls. Sleep 2011, 34, 293–301. [Google Scholar] [CrossRef] [PubMed]
- Zhao, M.; Chen, W.; Mo, X.; Yang, J.; Liu, H.; Shi, L.; Ma, H.; Jiang, Z. Abnormal Prefrontal Functional Network in Adult Obstructive Sleep Apnea: A Resting-state fNIRS Study. J. Sleep Res. 2023, 33, e14033. [Google Scholar] [CrossRef]
- Zhang, Z.; Schneider, M.; Fritschi, U.; Lehner, I.; Khatami, R. Near-Infrared Spectroscopy (NIRS) as a Useful Tool to Evaluate the Treatment Efficacy of Positive Airways Pressure Therapy in Patients with Obstructive Sleep Apnea Syndrome (OSAS): A Pilot Study. J. Innov. Opt. Health Sci. 2014, 7, 1450014. [Google Scholar] [CrossRef]
- Baillieul, S.; Wuyam, B.; Pérennou, D.; Tamisier, R.; Bailly, S.; Benmerad, M.; Piscicelli, C.; Le Roux-Mallouf, T.; Vergès, S.; Pépin, J.-L. A Randomized Sham-Controlled Trial on the Effect of Continuous Positive Airway Pressure Treatment on Gait Control in Severe Obstructive Sleep Apnea Patients. Sci. Rep. 2021, 11, 9329. [Google Scholar] [CrossRef]
- Zhang, Q.; Wang, D.; Qin, W.; Li, Q.; Chen, B.; Zhang, Y.; Yu, C. Altered Resting-State Brain Activity in Obstructive Sleep Apnea. Sleep 2013, 36, 651–659. [Google Scholar] [CrossRef] [PubMed]
- Erdoğan, S.B.; Yücel, M.A.; Akın, A. Analysis of Task-Evoked Systemic Interference in fNIRS Measurements: Insights from fMRI. NeuroImage 2014, 87, 490–504. [Google Scholar] [CrossRef] [PubMed]
- Hocke, L.; Oni, I.; Duszynski, C.; Corrigan, A.; Frederick, B.; Dunn, J. Automated Processing of fNIRS Data—A Visual Guide to the Pitfalls and Consequences. Algorithms 2018, 11, 67. [Google Scholar] [CrossRef] [PubMed]
- Seidel, O.; Carius, D.; Roediger, J.; Rumpf, S.; Ragert, P. Changes in Neurovascular Coupling during Cycling Exercise Measured by Multi-Distance fNIRS: A Comparison between Endurance Athletes and Physically Active Controls. Exp. Brain Res. 2019, 237, 2957–2972. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.; Xiao, F.; Shen, N.; Wang, Y.; Tang, J.; Luo, J.; Chen, W.; Chen, C. Protocol for Simultaneous EEG and fNIRS Measurement in Characterizing Brain State. Phenomics 2024. [Google Scholar] [CrossRef]
- Aasted, C.M.; Yücel, M.A.; Cooper, R.J.; Dubb, J.; Tsuzuki, D.; Becerra, L.; Petkov, M.P.; Borsook, D.; Dan, I.; Boas, D.A. Anatomical Guidance for Functional Near-Infrared Spectroscopy: AtlasViewer Tutorial. Neurophoton 2015, 2, 020801. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, M.; Mottola, L.; Quaresima, V. Principles, Techniques, and Limitations of Near Infrared Spectroscopy. Can. J. Appl. Physiol. 2004, 29, 463–487. [Google Scholar] [CrossRef] [PubMed]
- Hou, X.; Zhang, Z.; Zhao, C.; Duan, L.; Gong, Y.; Li, Z.; Zhu, C. NIRS-KIT: A MATLAB Toolbox for Both Resting-State and Task fNIRS Data Analysis. Neurophoton. 2021, 8, 010802. [Google Scholar] [CrossRef] [PubMed]
- Geng, S.; Liu, X.; Biswal, B.B.; Niu, H. Effect of Resting-State fNIRS Scanning Duration on Functional Brain Connectivity and Graph Theory Metrics of Brain Network. Front. Neurosci. 2017, 11, 392. [Google Scholar] [CrossRef]
- Wang, M.; Yuan, Z.; Niu, H. Reliability Evaluation on Weighted Graph Metrics of fNIRS Brain Networks. Quant. Imaging Med. Surg. 2019, 9, 832–841. [Google Scholar] [CrossRef] [PubMed]
- Ji, T.; Li, X.; Chen, J.; Ren, X.; Mei, L.; Qiu, Y.; Zhang, J.; Wang, S.; Xu, Z.; Li, H.; et al. Brain Function in Children with Obstructive Sleep Apnea: A Resting-State fMRI Study. Sleep 2021, 44, zsab047. [Google Scholar] [CrossRef] [PubMed]
- Qiu, K.; Mao, M.; Hu, Y.; Yi, X.; Zheng, Y.; Ying, Z.; Cheng, D.; Rao, Y.; Zhang, J.; Mu, X.; et al. Gender-Specific Association between Obstructive Sleep Apnea and Cognitive Impairment among Adults. Sleep Med. 2022, 98, 158–166. [Google Scholar] [CrossRef] [PubMed]
- Muñoz-Torres, Z.; Jiménez-Correa, U.; Montes-Rodríguez, C.J. Sex Differences in Brain Oscillatory Activity during Sleep and Wakefulness in Obstructive Sleep Apnea. J. Sleep Res. 2020, 29, e12977. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.; Cao, J.; Chen, J.; Wu, D.; Luo, K.; Shen, G.; Fang, Y.; Zhang, W.; Huang, G.; Su, X.; et al. Brain Morphology and Functional Connectivity Alterations in Patients with Severe Obstructive Sleep Apnea. Sleep Med. 2023, 111, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Dai, X.; Peng, D.-C.; Gong, H.-H.; Li, H.-J.; Nie, X.; Zhang, W. Altered Intrinsic Regional Brain Activity in Male Patients with Severe Obstructive Sleep Apnea: A Resting-State Functional Magnetic Resonance Imaging Study. Neuropsychiatr. Dis. Treat. 2014, 10, 1819. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Bai, Z.; He, Y.; Wu, Q. Relationship between Blood Amyloid A and Resting Magnetic Resonance Functional Brain Connections in Patients with Obstructive Sleep Apnea–Hypopnea Syndrome. Sleep Breath. 2023, 27, 477–485. [Google Scholar] [CrossRef] [PubMed]
- Li, H.-J.; Nie, X.; Gong, H.; Zhang, W.; Nie, S.; Peng, D.-C. Abnormal Resting-State Functional Connectivity within the Default Mode Network Subregions in Male Patients with Obstructive Sleep Apnea. Neuropsychiatr. Dis. Treat. 2016, 12, 203. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Fan, X.; Li, H.; Ye, C.; Yu, H.; Gong, H.; Zeng, X.; Peng, D.; Yan, L. Topological Reorganization of the Default Mode Network in Severe Male Obstructive Sleep Apnea. Front. Neurol. 2018, 9, 363. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Liu, Y.; Zhao, D.; Liu, B.; Zhang, H.; Huang, Z.; Babourina-Brooks, B.; Peet, A.C.; Zhang, L.; Feng, Y.; et al. Small-World Properties of the Whole-Brain Functional Networks in Patients with Obstructive Sleep Apnea-hypopnea Syndrome. Sleep Med. 2019, 62, 53–58. [Google Scholar] [CrossRef]
- Chen, L.-T.; Fan, X.-L.; Li, H.-J.; Nie, S.; Gong, H.-H.; Zhang, W.; Zeng, X.-J.; Long, P.; Peng, D.-C. Disrupted Small-World Brain Functional Network Topology in Male Patients with Severe Obstructive Sleep Apnea Revealed by Resting-State fMRI. Neuropsychiatr. Dis. Treat. 2017, 13, 1471–1482. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Cao, C.; Hu, B.; Li, D.; Sun, Y.; Wu, J.; Zhang, Q. Topological Regularization of Networks in Adult Patients with Moderate-to-Severe Obstructive Sleep Apnea-Hypopnea Syndrome: A Structural MRI Study. Nat. Sci. Sleep 2020, 12, 333–345. [Google Scholar] [CrossRef] [PubMed]
- Luo, Y.; Wang, D.; Liu, K.; Weng, J.; Guan, Y.; Chan, K.C.C.; Chu, W.C.W.; Shi, L. Brain Structure Network Analysis in Patients with Obstructive Sleep Apnea. PLoS ONE 2015, 10, e0139055. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.-T.; Fan, X.; Li, H.-J.; Ye, C.-L.; Yu, H.-H.; Xin, H.; Gong, H.; Peng, D.-C.; Yan, L. Aberrant Brain Functional Connectome in Patients with Obstructive Sleep Apnea. Neuropsychiatr. Dis. Treat. 2018, 14, 1059–1070. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Channel | Source | Detector | Region Label | Montreal Neurological Institute (MNI) | ||
|---|---|---|---|---|---|---|
| x | y | z | ||||
| Ch1 | S1 | D1 | Left superior temporal gyrus | −58 | −1 | −6 |
| Ch2 | S1 | D2 | Left precentral gyrus | −40 | 6 | 24 |
| Ch3 | S1 | D3 | Left superior temporal gyrus | −59 | −13 | 9 |
| Ch4 | S2 | D2 | Left inferior parietal lobule | −48 | −14 | 39 |
| Ch5 | S2 | D3 | Left supramarginal gyrus | −45 | −24 | 27 |
| Ch6 | S2 | D4 | Left supramarginal gyrus | −41 | −40 | 36 |
| Ch7 | S3 | D3 | Left middle temporal gyrus | −59 | −39 | 11 |
| Ch8 | S3 | D4 | Left angular gyrus | −48 | −50 | 26 |
| Ch9 | S4 | D5 | Right precentral gyrus | 53 | 6 | 24 |
| Ch10 | S4 | D6 | Right precentral gyrus | 45 | −12 | 37 |
| Ch11 | S5 | D5 | Right superior temporal gyrus | 61 | 2 | −6 |
| Ch12 | S6 | D5 | Right superior temporal gyrus | 60 | −11 | 9 |
| Ch13 | S6 | D6 | Right supramarginal gyrus | 52 | −22 | 25 |
| Ch14 | S6 | D7 | Right superior temporal gyrus | 72 | −42 | 13 |
| Ch15 | S7 | D6 | Right supramarginal gyrus | 56 | −43 | 41 |
| Ch16 | S7 | D7 | Right angular gyrus | 55 | −51 | 26 |
| Characteristics | Patients with OSA | HCs | p-Value |
|---|---|---|---|
| Age, years | 42.8 ± 7.91 | 42.1 ± 11.00 | 0.784 |
| BMI, kg/m2 | 25.2 ± 3.26 | 23.2 ± 2.68 | <0.01 |
| Gender, M/F | 95/53 | 90/60 | 0.451 |
| AHI, per hour | 2.02 ± 1.75 | 13.1 ± 9.98 | <0.01 |
| Smoking, Y/N | 136/12 | 140/10 | 0.623 |
| Drinking, Y/N | 120/28 | 117/33 | 0.530 |
| BAI | 25.5 | 26.2 | 0.285 |
| BDI | 4.95 | 5.23 | 0.399 |
| GAD-7 | 5.28 | 4.93 | 0.767 |
| FSS | 37.5 | 37.8 | 0.816 |
| ESS | 8.16 | 9.10 | 0.065 |
| PSQI | 3.41 | 3.63 | 0.530 |
| Channel | Nodal Betweenness Centrality | Nodal Degree Centrality | ||
|---|---|---|---|---|
| Z Statistic | p-Value | Z Statistic | p-Value | |
| Ch1 | 50.067 | 0.374 | 47.780 | 0.160 |
| Ch2 | 54.853 | 0.537 | 57.112 | 0.206 |
| Ch3 | 55.861 | 0.366 | 55.002 | 0.508 |
| Ch4 | 55.344 | 0.447 | 53.427 | 0.831 |
| Ch5 | 48.620 | 0.248 | 51.825 | 0.808 |
| Ch6 | 52.691 | 0.997 | 54.886 | 0.529 |
| Ch7 | 52.286 | 0.912 | 54.113 | 0.683 |
| Ch8 | 55.214 | 0.465 | 56.137 | 0.324 |
| Ch9 | 44.251 | 0.016 * | 48.283 | 0.210 |
| Ch10 | 51.412 | 0.719 | 51.818 | 0.807 |
| Ch11 | 54.338 | 0.567 | 50.584 | 0.547 |
| Ch12 | 51.023 | 0.638 | 53.365 | 0.845 |
| Ch13 | 45.029 | 0.030 * | 45.487 | 0.040 * |
| Ch14 | 53.695 | 0.772 | 52.622 | 0.988 |
| Ch15 | 58.372 | 0.104 | 52.924 | 0.944 |
| Ch16 | 54.497 | 0.600 | 54.414 | 0.621 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xiao, F.; Liu, M.; Wang, Y.; Zhou, L.; Luo, J.; Chen, C.; Chen, W. Altered Functional Connectivity of Temporoparietal Lobe in Obstructive Sleep Apnea: A Resting-State fNIRS Study. Bioengineering 2024, 11, 389. https://doi.org/10.3390/bioengineering11040389
Xiao F, Liu M, Wang Y, Zhou L, Luo J, Chen C, Chen W. Altered Functional Connectivity of Temporoparietal Lobe in Obstructive Sleep Apnea: A Resting-State fNIRS Study. Bioengineering. 2024; 11(4):389. https://doi.org/10.3390/bioengineering11040389
Chicago/Turabian StyleXiao, Fang, Minghui Liu, Yalin Wang, Ligang Zhou, Jingchun Luo, Chen Chen, and Wei Chen. 2024. "Altered Functional Connectivity of Temporoparietal Lobe in Obstructive Sleep Apnea: A Resting-State fNIRS Study" Bioengineering 11, no. 4: 389. https://doi.org/10.3390/bioengineering11040389