
Pelvic Ring Fractures: A Biomechanical Comparison of Sacral and Lumbopelvic Fixation Techniques
 , ,
, ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Finite Element Model of Lumbar Spine Pelvis
2.2. Simulation of Pelvic Ring Fracture
2.3. Simulating the Instrumentation of Pelvic Ring Fracture
- L5-Ilium posterior screw fixation without cross connectors (L5_PF_WO_CC): Bilateral posterior screw fixation was performed from L5-Ilium. The pedicle screws were connected to spinal rods.
- L5-Ilium posterior screw fixation with cross connectors (L5_PF_W_CC): Bilateral posterior screw fixation was performed from L5-Ilium. The pedicle screws were connected to spinal rods. A cross connector was placed at the S1 level to connect the two rods.
- TITS fixation at S1 and S2 level (S1_TITS_S2_TITS): TITS fixation was simulated at the S1 and S2 levels.
- IS fixation at S1 and TITS fixation at S2 level (S1_IS_S2_TITS): A TITS fixation was simulated at the S2 level, and an ilio-sacral screw (IS) fixation was performed at the S1 level.
- Double transiliac rod and screw fixation (DTSF): Two traditional iliac screws were placed bilaterally. A horizontal rod was used to connect the iliac screws.
2.4. Loading and Boundary Conditions
2.5. Data Analyses
3. Results
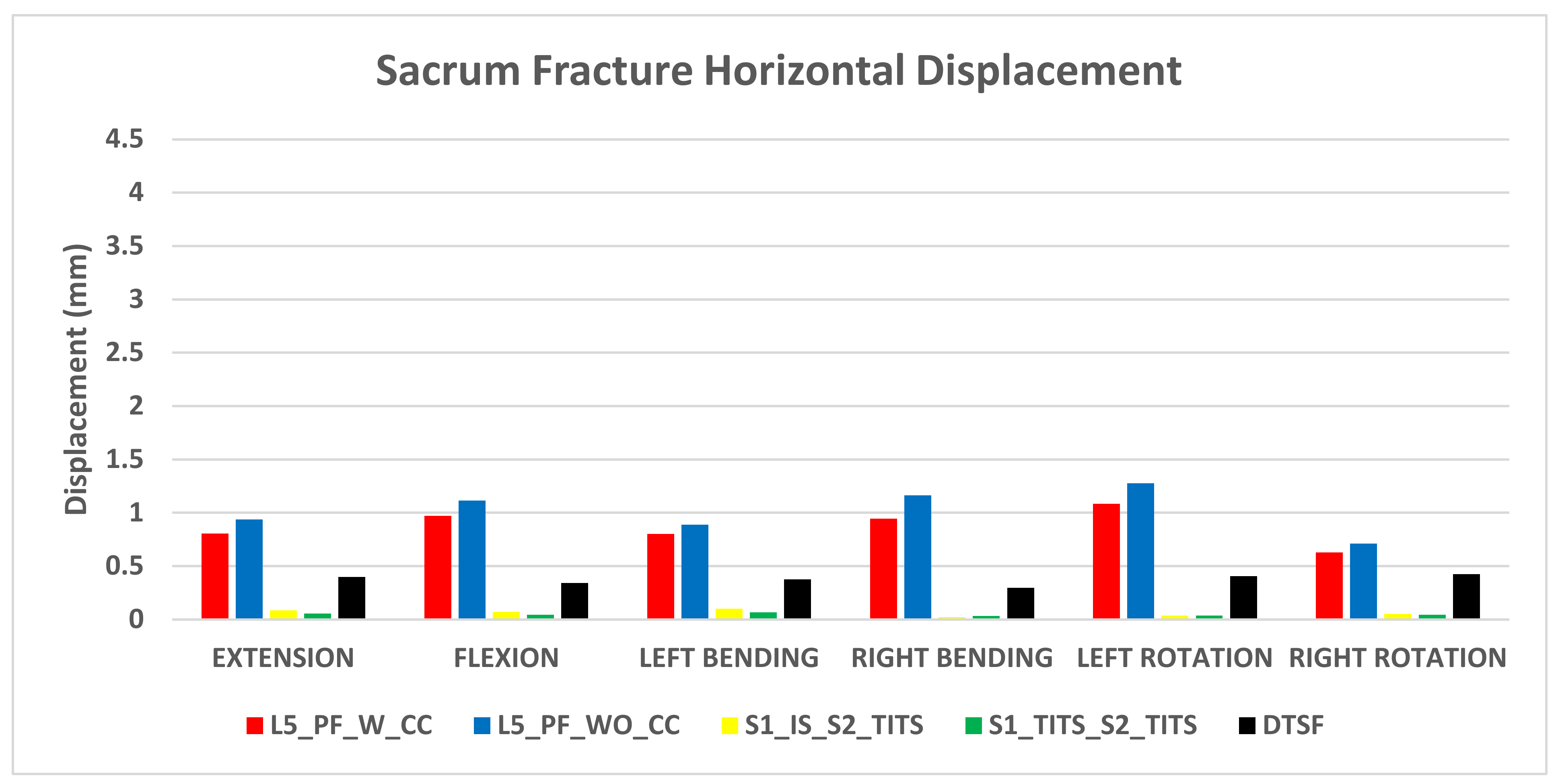
3.1. Stabilization at the Sacral Fracture Region (Figure 4 and Figure 5)


3.2. Stabilization at the Pubic Rami Fracture Region (Figure 6 and Figure 7)


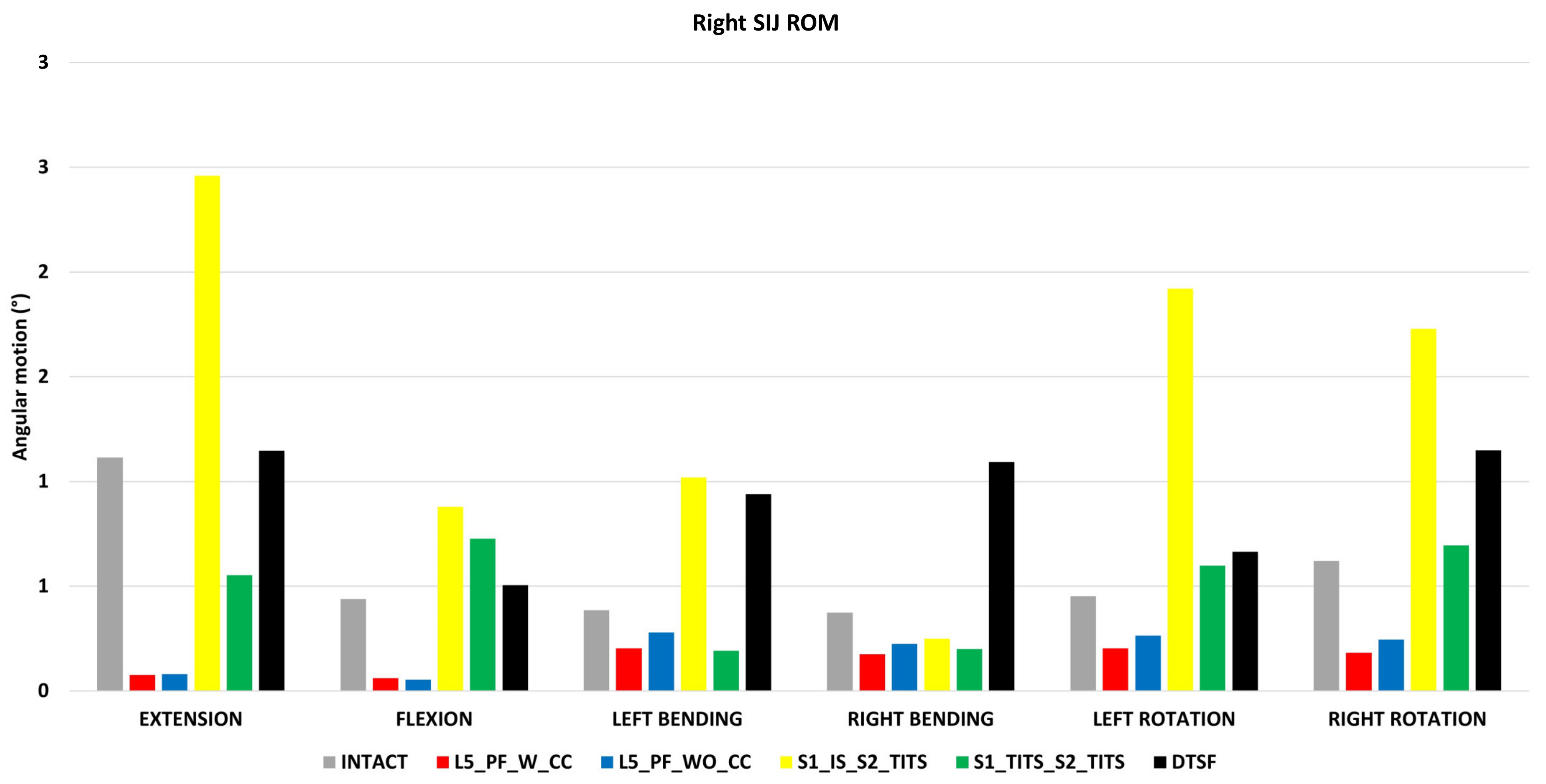
3.3. Sacroiliac Joint (SIJ) Range of Motion (ROM) (Figure 8)

3.4. ROM at the L5-S1 Level (Figure 9)

3.5. Overall ROM for L1-S1 (Figure 10)

3.6. Peak von Mises Stresses at the L5-S1 Intervertebral Disc (Figure 11)

3.7. Stress on the Implants (Table 2)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Von Mises Stress (MPa) | ||||||
|---|---|---|---|---|---|---|
| Extension | Flexion | Left Bending | Right Bending | Left Rotation | Right Rotation | |
| L5_PF_W_CC | 310.2 | 251.7 | 368.8 | 209 | 279.3 | 266.8 |
| Left Rod | Left Rod | Left Rod | Left Rod | Left Rod | Left Rod | |
| Between L5 & ilium Tulip | Between L5 & ilium Tulip | Between L5 & ilium Tulip | Between L5 & ilium Tulip | Between L5 & ilium Tulip | Between L5 & ilium Tulip | |
| L5_PF_WO_CC | 308.2 | 287.9 | 403 | 212.4 | 307.6 | 307.3 |
| Left Rod | Left Rod | Left Rod | Left Rod | Left Rod | Left Rod | |
| Between L5 & ilium Tulip | Between L5 & ilium Tulip | Between L5 & ilium Tulip | Between L5 & ilium Tulip | Between L5 & ilium Tulip | Between L5 & ilium Tulip | |
| S1_IS_S2_TITS | 114.2 | 132.1 | 155.3 | 86.17 | 154.8 | 168.2 |
| TITS | TITS | TITS | TITS | TITS | TITS | |
| S1_TITS_S2_TITS | 194 | 188.9 | 243.6 | 200.3 | 188.1 | 218.2 |
| Top TITS | Top TITS | Top TITS | Top TITS | Top TITS | Top TITS | |
| DTSF | 75.76 | 81.97 | 71.3 | 114.4 | 94.15 | 99.15 |
| Top Rod | Top Rod | Top Rod | Top Rod | Top Rod | Top Rod | |
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Davis, D.D.; Foris, L.A.; Kane, S.M.; Waseem, M. Pelvic Fracture. In StatPearls; StatPearls Publishing LLC: Treasure Island, FL, USA, 2021. [Google Scholar]
- Rommens, P.M.; Hofmann, A. Comprehensive classification of fragility fractures of the pelvic ring: Recommendations for surgical treatment. Injury 2013, 44, 1733–1744. [Google Scholar] [CrossRef] [PubMed]
- Grotz, M.R.; Allami, M.K.; Harwood, P.; Pape, H.C.; Krettek, C.; Giannoudis, P.V. Open pelvic fractures: Epidemiology, current concepts of management and outcome. Injury 2005, 36, 1–13. [Google Scholar] [CrossRef]
- Isler, B.; Ganz, R. Classification of pelvic ring injuries. Injury 1996, 27 (Suppl. 1), 3–12. [Google Scholar] [CrossRef]
- Simonian, P.T.; Routt, M.L., Jr.; Harrington, R.M.; Tencer, A.F. Internal fixation of the unstable anterior pelvic ring: A biomechanical comparison of standard plating techniques and the retrograde medullary superior pubic ramus screw. J. Orthop. Trauma 1994, 8, 476–482. [Google Scholar] [CrossRef]
- Elzohairy, M.M.; Salama, A.M. Open reduction internal fixation versus percutaneous iliosacral screw fixation for unstable posterior pelvic ring disruptions. Orthop. Traumatol. Surg. Res. 2017, 103, 223–227. [Google Scholar] [CrossRef] [PubMed]
- Yinger, K.; Scalise, J.; Olson, S.A.; Bay, B.K.; Finkemeier, C.G. Biomechanical comparison of posterior pelvic ring fixation. J. Orthop. Trauma 2003, 17, 481–487. [Google Scholar] [CrossRef] [PubMed]
- Kerschbaum, M.; Hausmann, N.; Worlicek, M.; Pfeifer, C.; Nerlich, M.; Schmitz, P. Patient-related outcome of unstable pelvic ring fractures stabilized with a minimal invasive screw-rod system. Health Qual. Life Outcomes 2017, 15, 248. [Google Scholar] [CrossRef]
- Yuan, B.M.; Huang, G.; Zheng, S.; Yu, T.; Zhao, J.W. A screw view model of navigation guided minimal invasive percutaneous pelvic screws insertion for lateral compression pelvic ring injuries: A case report. Medicine 2020, 99, e21755. [Google Scholar] [CrossRef]
- Routt, M.L., Jr.; Kregor, P.J.; Simonian, P.T.; Mayo, K.A. Early results of percutaneous iliosacral screws placed with the patient in the supine position. J. Orthop. Trauma 1995, 9, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Schweitzer, D.; Zylberberg, A.; Córdova, M.; Gonzalez, J. Closed reduction and iliosacral percutaneous fixation of unstable pelvic ring fractures. Injury 2008, 39, 869–874. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.; Ren, X.; Cui, Y.; Cheng, X.; Peng, S.; Hou, Z.; Han, Y. Biomechanical study of three kinds of internal fixation for the treatment of sacroiliac joint disruption using biomechanical test and finite element analysis. J. Orthop. Surg. Res. 2018, 13, 152. [Google Scholar] [CrossRef] [PubMed]
- Toda, K.; Yagata, Y.; Kikuchi, T.; Takigawa, T.; Ito, Y. Minimally Invasive Surgery for Unstable Pelvic Ring Fractures: Transiliac Rod and Screw Fixation. Acta Med. Okayama 2020, 74, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Allen, B.L., Jr.; Ferguson, R.L. The Galveston technique for L rod instrumentation of the scoliotic spine. Spine 1982, 7, 276–284. [Google Scholar] [CrossRef]
- Acklin, Y.P.; Zderic, I.; Richards, R.G.; Schmitz, P.; Gueorguiev, B.; Grechenig, S. Biomechanical investigation of four different fixation techniques in sacrum Denis type II fracture with low bone mineral density. J. Orthop. Res. 2018, 36, 1624–1629. [Google Scholar] [CrossRef] [PubMed]
- Hu, P.; Wu, T.; Wang, H.-Z.; Qi, X.-Z.; Yao, J.; Cheng, X.-D.; Chen, W.; Zhang, Y.-Z. Biomechanical Comparison of Three Internal Fixation Techniques for Stabilizing Posterior Pelvic Ring Disruption: A 3D Finite Element Analysis. Orthop. Surg. 2019, 11, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Zhang, S.; Sun, T.; Wang, D.; Lian, W.; Tan, J.; Zou, D.; Zhao, Y. Mechanical comparison between lengthened and short sacroiliac screws in sacral fracture fixation: A finite element analysis. Orthop. Traumatol. Surg. Res. 2013, 99, 601–606. [Google Scholar] [CrossRef] [PubMed]
- Schwab, F.; Ungar, B.; Blondel, B.; Buchowski, J.; Coe, J.; Deinlein, D.; DeWald, C.; Mehdian, H.; Shaffrey, C.; Tribus, C.; et al. Scoliosis Research Society-Schwab adult spinal deformity classification: A validation study. Spine 2012, 37, 1077–1082. [Google Scholar] [CrossRef]
- Kumaran, Y.; Nishida, N.; Tripathi, S.; Mumtaz, M.; Sakai, T.; Elgafy, H.; Goel, V.K. Effects of Sacral Slope Changes on the Intervertebral Disc and Hip Joint: A Finite Element Analysis. World Neurosurg. 2023, 176, e32–e39. [Google Scholar] [CrossRef]
- Nishida, N.; Mumtaz, M.; Tripathi, S.; Kumaran, Y.; Kelkar, A.; Sakai, T.; Goel, V.K. The Effect of Posterior Lumbar Interbody Fusion in Lumbar Spine Stenosis with Diffuse Idiopathic Skeletal Hyperostosis: A Finite Element Analysis. World Neurosurg. 2023, 176, e371–e379. [Google Scholar] [CrossRef] [PubMed]
- Goel, V.K.; Grauer, J.N.; Patel, T.; Biyani, A.; Sairyo, K.; Vishnubhotla, S.; Matyas, A.; Cowgill, I.; Shaw, M.; Long, R.; et al. Effects of charité artificial disc on the implanted and adjacent spinal segments mechanics using a hybrid testing protocol. Spine 2005, 30, 2755–2764. [Google Scholar] [CrossRef]
- Dalstra, M.; Huiskes, R.; van Erning, L. Development and validation of a three-dimensional finite element model of the pelvic bone. J. Biomech. Eng. 1995, 117, 272–278. [Google Scholar] [CrossRef] [PubMed]
- Momeni Shahraki, N.; Fatemi, A.; Goel, V.K.; Agarwal, A. On the Use of Biaxial Properties in Modeling Annulus as a Holzapfel-Gasser-Ogden Material. Front. Bioeng. Biotechnol. 2015, 3, 69. [Google Scholar] [CrossRef] [PubMed]
- Lindsey, D.P.; Kiapour, A.; Yerby, S.A.; Goel, V.K. Sacroiliac Joint Fusion Minimally Affects Adjacent Lumbar Segment Motion: A Finite Element Study. Int. J. Spine Surg. 2015, 9, 64. [Google Scholar] [CrossRef] [PubMed]
- Ivanov, A.A.; Kiapour, A.; Ebraheim, N.A.; Goel, V. Lumbar fusion leads to increases in angular motion and stress across sacroiliac joint: A finite element study. Spine 2009, 34, E162–E169. [Google Scholar] [CrossRef]
- Joukar, A.; Shah, A.; Kiapour, A.; Vosoughi, A.S.; Duhon, B.; Agarwal, A.K.; Elgafy, H.; Ebraheim, N.; Goel, V.K. Sex Specific Sacroiliac Joint Biomechanics during Standing Upright: A Finite Element Study. Spine 2018, 43, E1053–E1060. [Google Scholar] [CrossRef] [PubMed]
- Tripathi, S. Finite Element Analyses of Stabilization of Sacral Fractures (Zone I Denis Fracture) under One Leg Standing Stance; University of Toledo: Toledo, OH, USA, 2021. [Google Scholar]
- Nishida, N.; Mumtaz, M.; Tripathi, S.; Kelkar, A.; Kumaran, Y.; Sakai, T.; Goel, V.K. Biomechanical analysis of laminectomy, laminoplasty, posterior decompression with instrumented fusion, and anterior decompression with fusion for the kyphotic cervical spine. Int. J. Comput. Assist. Radiol. Surg. 2022, 17, 1531–1541. [Google Scholar] [CrossRef]
- Nishida, N.; Tripathi, S.; Mumtaz, M.; Kelkar, A.; Kumaran, Y.; Sakai, T.; Goel, V.K. Soft Tissue Injury in Cervical Spine Is a Risk Factor for Intersegmental Instability: A Finite Element Analysis. World Neurosurg. 2022, 164, e358–e366. [Google Scholar] [CrossRef] [PubMed]
- Guerado, E.; Cervan, A.M.; Cano, J.R.; Giannoudis, P.V. Spinopelvic injuries. Facts and controversies. Injury 2018, 49, 449–456. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Peng, Y.; Du, C.; Tang, P. Biomechanical study of four kinds of percutaneous screw fixation in two types of unilateral sacroiliac joint dislocation: A finite element analysis. Injury 2014, 45, 2055–2059. [Google Scholar] [CrossRef]
- Turbucz, M.; Pokorni, A.J.; Bigdon, S.F.; Hajnal, B.; Koch, K.; Szoverfi, Z.; Lazary, A.; Eltes, P.E. Patient-specific bone material modelling can improve the predicted biomechanical outcomes of sacral fracture fixation techniques: A comparative finite element study. Injury 2023, 54, 111162. [Google Scholar] [CrossRef]
- Engelmann, C. [Reconstructive surgery of the bronchi in inflammatory lesions]. Zentralbl. Chir. 1989, 114, 286–296. [Google Scholar] [PubMed]
- Bastian, J.D.; Bergmann, M.; Schwyn, R.; Keel, M.J.; Benneker, L.M. Assessment of the Breakaway Torque at the Posterior Pelvic Ring in Human Cadavers. J. Investig. Surg. 2015, 28, 328–333. [Google Scholar] [CrossRef]
- Kim, C.H.; Kim, J.W. Plate versus sacroiliac screw fixation for treating posterior pelvic ring fracture: A Systematic review and meta-analysis. Injury 2020, 51, 2259–2266. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.W.; Oh, C.W.; Oh, J.K.; Kyung, H.S.; Park, K.H.; Yoon, S.D.; Yoon, S.H. The incidence of and factors affecting iliosacral screw loosening in pelvic ring injury. Arch. Orthop. Trauma Surg. 2016, 136, 921–927. [Google Scholar] [CrossRef] [PubMed]
- Salazar, D.; Lannon, S.; Pasternak, O.; Schiff, A.; Lomasney, L.; Mitchell, E.; Stover, M. Investigation of bone quality of the first and second sacral segments amongst trauma patients: Concerns about iliosacral screw fixation. J. Orthop. Traumatol. 2015, 16, 301–308. [Google Scholar] [CrossRef] [PubMed]
- Moed, B.R.; Geer, B.L. S2 iliosacral screw fixation for disruptions of the posterior pelvic ring: A report of 49 cases. J. Orthop. Trauma 2006, 20, 378–383. [Google Scholar] [CrossRef] [PubMed]
- Griffin, D.R.; Starr, A.J.; Reinert, C.M.; Jones, A.L.; Whitlock, S. Vertically unstable pelvic fractures fixed with percutaneous iliosacral screws: Does posterior injury pattern predict fixation failure? J. Orthop. Trauma 2006, 20, S30–S36, discussion S6. [Google Scholar] [CrossRef] [PubMed]
- Eastman, J.G.; Shelton, T.J.; Routt, M.L.C., Jr.; Adams, M.R. Posterior pelvic ring bone density with implications for percutaneous screw fixation. Eur. J. Orthop. Surg. Traumatol. 2021, 31, 383–389. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.C.; Jin, H.M.; Yan, Y.Z.; Chen, J.; Wang, K.; Wang, J.L.; Zhang, Z.J.; Wu, A.M.; Wang, X.Y. Biomechanical Role of the Thoracolumbar Ligaments of the Posterior Ligamentous Complex: A Finite Element Study. World Neurosurg. 2018, 112, e125–e133. [Google Scholar] [CrossRef]
- Rommens, P.M.; Arand, C.; Hofmann, A.; Wagner, D. When and How to Operate Fragility Fractures of the Pelvis? Indian. J. Orthop. 2019, 53, 128–137. [Google Scholar] [CrossRef]
- König, M.A.; Jehan, S.; Boszczyk, A.A.; Boszczyk, B.M. Surgical management of U-shaped sacral fractures: A systematic review of current treatment strategies. Eur. Spine J. 2012, 21, 829–836. [Google Scholar] [CrossRef] [PubMed]
- Chon, C.S.; Jeong, J.H.; Kang, B.; Kim, H.S.; Jung, G.H. Computational simulation study on ilio-sacral screw fixations for pelvic ring injuries and implications in Asian sacrum. Eur. J. Orthop. Surg. Traumatol. 2018, 28, 439–444. [Google Scholar] [CrossRef] [PubMed]
- Wakely, P.E., Jr.; Giacomantonio, M. Fine needle aspiration cytology of metastatic malignant rhabdoid tumor. Acta Cytol. 1986, 30, 533–537. [Google Scholar] [PubMed]
- Jazini, E.; Klocke, N.; Tannous, O.; Johal, H.S.; Hao, J.; Salloum, K.; Gelb, D.E.; Nascone, J.W.; Belin, E.; Hoshino, C.M.; et al. Does Lumbopelvic Fixation Add Stability? A Cadaveric Biomechanical Analysis of an Unstable Pelvic Fracture Model. J. Orthop. Trauma 2017, 31, 37–46. [Google Scholar] [CrossRef]
- Wenning, K.E.; Yilmaz, E.; Schildhauer, T.A.; Hoffmann, M.F. Comparison of lumbopelvic fixation and iliosacral screw fixation for the treatment of bilateral sacral fractures. J. Orthop. Surg. Res. 2021, 16, 604. [Google Scholar] [CrossRef] [PubMed]
- Virk, S.S.; Niedermeier, S.; Yu, E.; Khan, S.N. Adjacent segment disease. Orthopedics 2014, 37, 547–555. [Google Scholar] [CrossRef] [PubMed]
- Kumaran, Y.; Shah, A.; Katragadda, A.; Padgaonkar, A.; Zavatsky, J.; McGuire, R.; Serhan, H.; Elgafy, H.; Goel, V.K. Iatrogenic muscle damage in transforaminal lumbar interbody fusion and adjacent segment degeneration: A comparative finite element analysis of open and minimally invasive surgeries. Eur. Spine J. 2021, 30, 2622–2630. [Google Scholar] [CrossRef] [PubMed]
- Halawi, M.J. Pelvic ring injuries: Surgical management and long-term outcomes. J. Clin. Orthop. Trauma 2016, 7, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Z.M.; Yu, B.S.; Chen, H.; Aladin, D.M.; Zhang, K.B.; Zhang, J.F.; Liu, H.; Luk, K.D.; Lu, W.W. Effect of iliac screw insertion depth on the stability and strength of lumbo-iliac fixation constructs: An anatomical and biomechanical study. Spine 2009, 34, E565–E572. [Google Scholar] [CrossRef]
- Akesen, B.; Wu, C.; Mehbod, A.A.; Sokolowski, M.; Transfeldt, E.E. Revision of loosened iliac screws: A biomechanical study of longer and bigger screws. Spine 2008, 33, 1423–1428. [Google Scholar] [CrossRef]



| Component | Material Properties | Constitute Relation | Element Type |
|---|---|---|---|
| Vertebral Cortical Bone (17,554 nodes and 9123 elements) | E = 12,000 MPa | Isotropic, Elastic | 8 Node Brick Element (C3D8) |
| v = 0.3 | |||
| Vertebral Cancellous Bone (41,357 nodes and 202,515 elements) | E = 100 MPa | Isotropic, Elastic | 4 Node Tetrahedral Element (C3D4) |
| v = 0.2 | |||
| Pelvis Cortical Bone (Sacrum, Ilium) (26,490 nodes and 26,762 elements) | E = 17,000 MPa | Isotropic, Elastic | 4 Node Tetrahedral Element (C3D4) |
| v = 0.3 | |||
| Sacrum Cancellous Bone (16,891 nodes and 70,679 elements) | Heterogenous | Isotropic, Elastic | 4 Node Tetrahedral Element (C3D4) |
| Ilium Cancellous Bone (20,083 nodes and 96,912 elements) | E = 70 MPa | Isotropic, Elastic | |
| v = 0.2 | 4 Node Tetrahedral Element (C3D4) | ||
| Femur Cortical Bone (31,776 nodes and 31,776 elements) | E = 17,000 MPa | Isotropic, Elastic | 4 Node Tetrahedral Element (C3D4) |
| v = 0.29 | |||
| Femur Cancellous Bone (64,486 nodes and 334,529 elements) | E = 100 MPa | Isotropic, Elastic | 4 Node Tetrahedral Element (C3D4) |
| v = 0.2 | |||
| Ground Substance of Annulus Fibrosis (24,320 nodes and 18,480 elements) | c10 = 0.035 | ||
| k1 = 0.296 | Hyper elastic anisotropic (HGO) | 8 Node Brick Element (C3D8) | |
| k2 = 65 | |||
| Nucleus Pulposus (14,326 nodes and 11,088 elements) | E = 1 MPa | Isotropic, Elastic | 8 Node Brick Element (C3D8) |
| v = 0.499 | |||
| Anterior Longitudinal (636 nodes and 553 elements) | 7.8 MPa (<12%), 20 MPa (>12%) | Non-linear Hypo elastic | Truss Element (T3D2) |
| Posterior Longitudinal (636 nodes and 553 elements) | 10 MPa (<11%), 20 MPa (>11%) | Non-linear Hypo elastic | Truss Element (T3D2) |
| Ligamentum Flavum (48 nodes and 24 elements) | 15 MPa (<6.2%), 19.5 MPa (>6.2%) | Non-linear Hypo elastic | Truss Element (T3D2) |
| Intertransverse (66 nodes and 33 elements) | 10 MPa (<18%), 58.7 MPa (>18%) | Non-linear Hypo elastic | Truss Element (T3D2) |
| Interspinous (60 nodes and 30 elements) | 10 MPa (<14%), 11.6 MPa (>14%) | Non-linear Hypo elastic | Truss Element (T3D2) |
| Supraspinous (45 nodes and 23 elements) | 8 MPa (<20%), 15 MPa (>20%) | Non-linear Hypo elastic | Truss Element (T3D2) |
| Capsular (45 nodes and 23 elements) | 7.5 MPa (<25%), 32.9 MPa (>25%) | Non-linear Hypo elastic | Truss Element (T3D2) |
| Anterior SIJ (52 nodes and 26 elements) | 125 MPa (5%), 325 MPa (>10%), 316 MPa (>15%) | Non-linear Hypo elastic | Truss Element (T3D2) |
| Short Posterior SI (20 nodes and 10 elements) | 43 MPa (5%), 113 MPa (>10%), 110 MPa (>15%) | Non-linear Hypo elastic | Truss Element (T3D2) |
| Long Posterior SI (32 nodes and 16 elements) | 150 MPa (5%), 391 MPa (>10%), 381 MPa (>15%) | Non-linear Hypo elastic | Truss Element (T3D2) |
| Interosseous (45 nodes and 23 elements) | 40 MPa (5%), 105 MPa (>10%), 102 MPa (>15%) | Non-linear Hypo elastic | Truss Element (T3D2) |
| Sacrospinous (32 nodes and 16 elements) | 304 MPa (5%), 792 MPa (>10%), 771 MPa (>15%) | Non-linear Hypo elastic | Truss Element (T3D2) |
| Sacrotuberous Ligament (58 nodes and 29 elements) | 326 MPa (5%), 848 MPa (>10%), 826 MPa (>15%) | Non-linear Hypo elastic | Truss Element (T3D2) |
| Gluteus Maximus | k = 344 N/mm | Connector Element | |
| Gluteus Medius | k = 779 N/mm | Connector Element | |
| Gluteus Minimus | k = 660 N/mm | Connector Element | |
| Psoas Major | k = 100 N/mm | Connector Element | |
| Adductor Magnus | k = 257 N/mm | Connector Element | |
| Adductor Longus | k = 134 N/mm | Connector Element | |
| Adductor Brevis | k = 499 N/mm | Connector Element | |
| Rods (Titanium) | E = 120,000 MPa | Isotropic, Elastic | Hexahedral Element |
| v = 0.3 | |||
| Pedicle Screws (Titanium) | E = 120,000 MPa | Isotropic, Elastic | Hexahedral Element |
| v = 0.3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tripathi, S.; Nishida, N.; Soehnlen, S.; Kelkar, A.; Kumaran, Y.; Seki, T.; Sakai, T.; Goel, V.K. Pelvic Ring Fractures: A Biomechanical Comparison of Sacral and Lumbopelvic Fixation Techniques. Bioengineering 2024, 11, 348. https://doi.org/10.3390/bioengineering11040348
Tripathi S, Nishida N, Soehnlen S, Kelkar A, Kumaran Y, Seki T, Sakai T, Goel VK. Pelvic Ring Fractures: A Biomechanical Comparison of Sacral and Lumbopelvic Fixation Techniques. Bioengineering. 2024; 11(4):348. https://doi.org/10.3390/bioengineering11040348
Chicago/Turabian StyleTripathi, Sudharshan, Norihiro Nishida, Sophia Soehnlen, Amey Kelkar, Yogesh Kumaran, Toshihiro Seki, Takashi Sakai, and Vijay K. Goel. 2024. "Pelvic Ring Fractures: A Biomechanical Comparison of Sacral and Lumbopelvic Fixation Techniques" Bioengineering 11, no. 4: 348. https://doi.org/10.3390/bioengineering11040348