

Development of the AI Pipeline for Corneal Opacity Detection
 , ,
, ,
Abstract
:1. Introduction
1.1. Shortage of Ophthalmologists in Developing Countries
1.2. Device Used in This Study
1.3. Application Example of Deep Learning to Ophthalmology
1.4. Potential Problems with Deep Learning: Eye Diseases
1.5. Corneal Opacity Detection Research Using Deep Learning
1.6. Motivation for Study
1.7. Purpose of Study
2. Materials and Methods
2.1. Ethical Approval
2.2. Device to Capture the Anterior Segment Videos
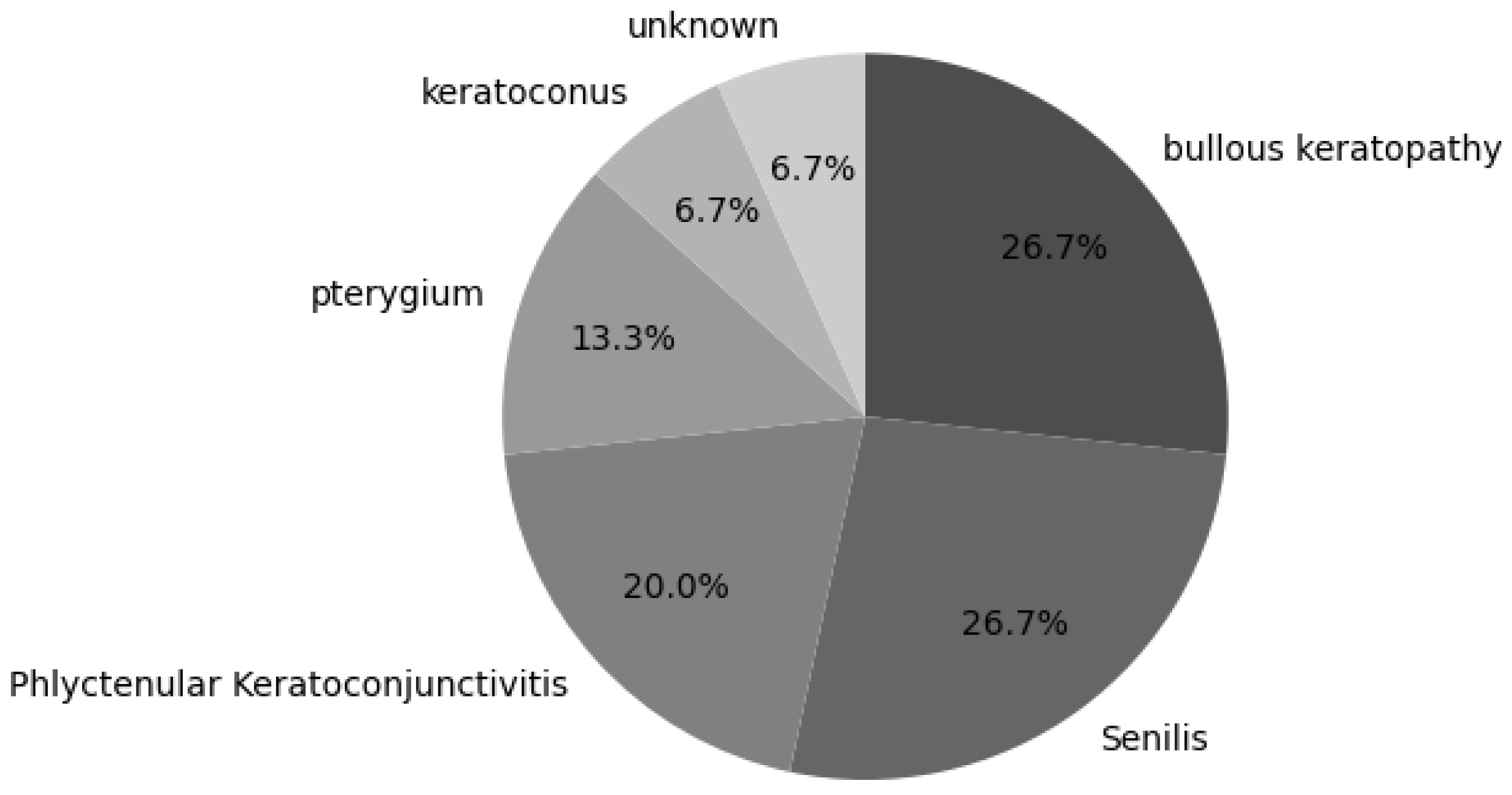
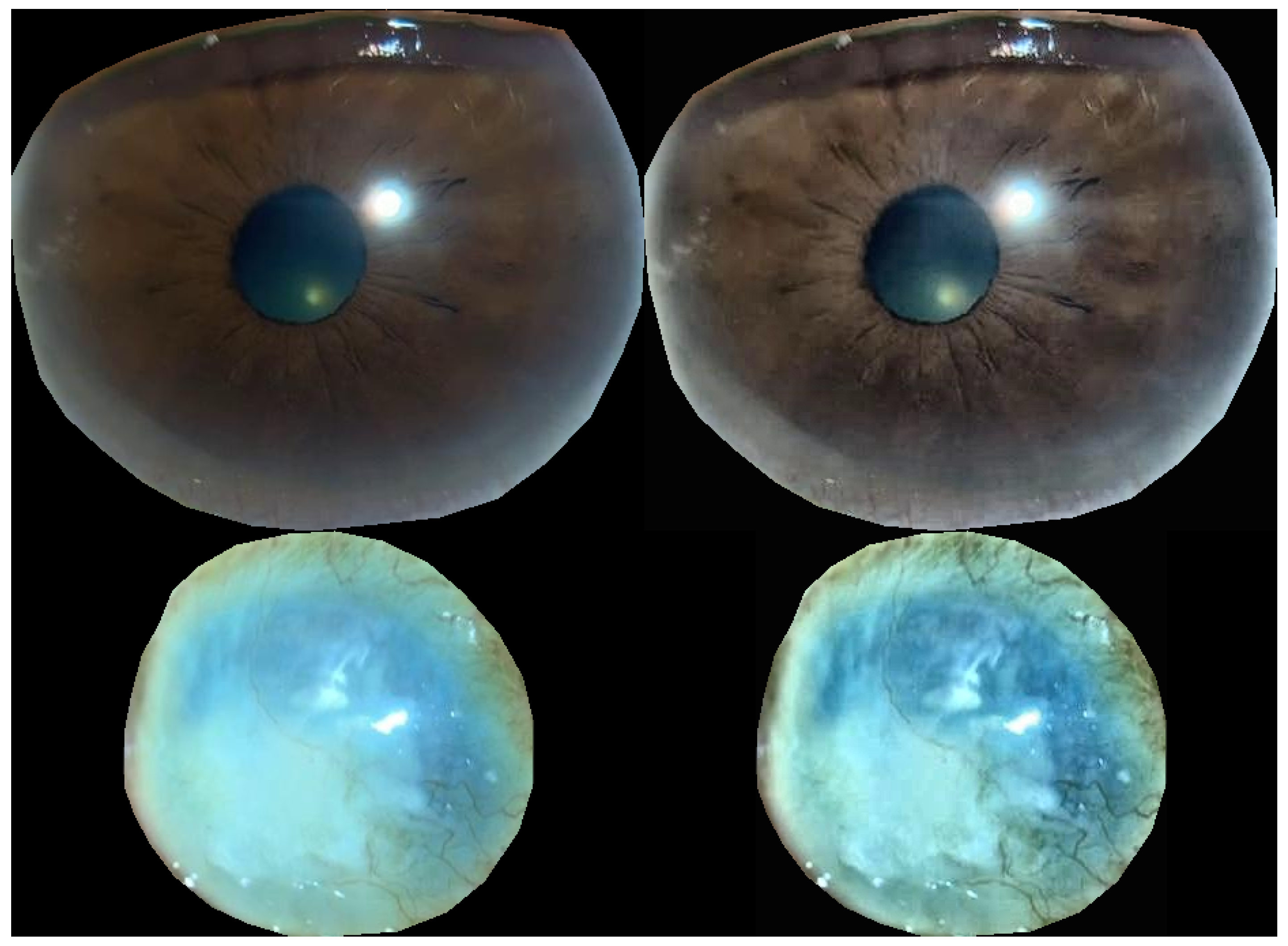
2.3. Method to Build the Dataset
2.4. Deep Learning for Corneal Opacity Detection
2.5. Improved Deep Learning for Corneal Opacity Detection
2.6. Hyperparameters for Training
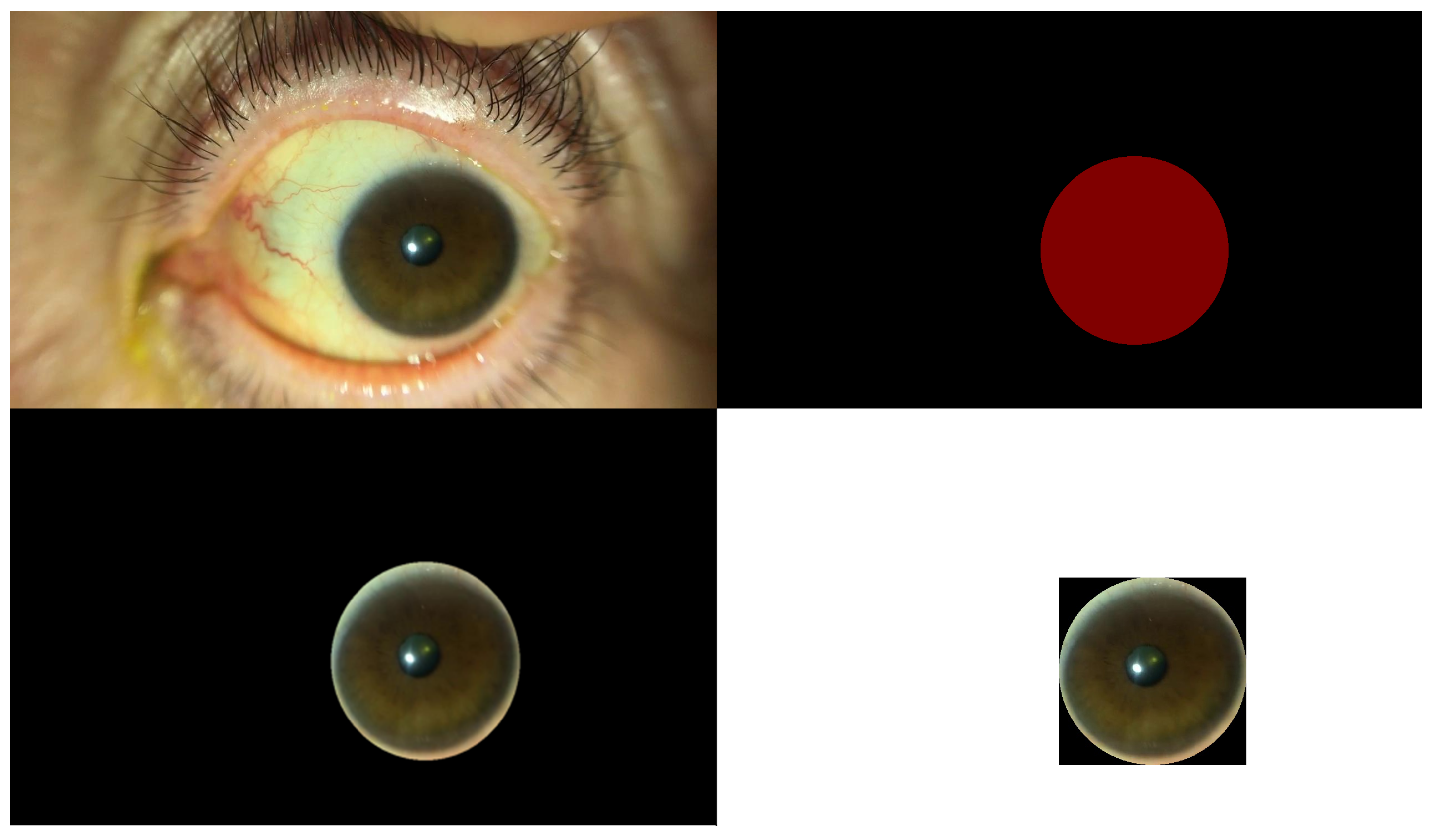
2.7. Semantic Segmentation
2.8. Hyperparameters for Semantic Segmentation
2.9. Data Augmentation Methods for Semantic Segmentation
2.10. Environment for Study
3. Results
4. Discussions
Limitations of This Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Resnikoff, S.; Felch, W.; Gauthier, T.; Spivey, B. The number of ophthalmologists in practice and training worldwide: A growing gap despite more than 200,000 practitioners. Br. J. Ophthalmol. 2012, 96, 783–787. [Google Scholar] [CrossRef] [PubMed]
- Schwab, L.; Whitfield, R., Jr. Appropriate ophthalmic surgical technology in developing nations. Ophthalmic Surg. Lasers Imaging Retin. 2013, 13, 991–993. [Google Scholar] [CrossRef]
- Singh, J.; Kabbara, S.; Conway, M.; Peyman, G.; Ross, R.D. Innovative Diagnostic Tools for Ophthalmology in Low-Income Countries. In Novel Diagnostic Methods in Ophthalmology; IntechOpen: London, UK, 2019. [Google Scholar]
- Chirambo, M.C. The role of Western ophthalmologists in dealing with cataract blindness in developing countries. Doc. Ophthalmol. 1992, 81, 349–350. [Google Scholar] [CrossRef] [PubMed]
- Smart Eye Camera: Ophthalmic Exams via Your Smartphone Anywhere, Anytime. Available online: https://ouiinc.jp (accessed on 10 January 2024).
- Handayani, A.T.; Valentina, C.; Suryaningrum, I.G.A.R.; Megasafitri, P.D.; Juliari, I.G.A.M.; Pramita, I.A.A.; Nakayama, S.; Shimizu, E.; Triningrat, A.A.M.P. Interobserver Reliability of Tear Break-Up Time Examination Using “Smart Eye Camera” in Indonesian Remote Area. Clin. Ophthalmol. 2023, 17, 2097–2107. [Google Scholar] [CrossRef] [PubMed]
- Andhare, P.; Ramasamy, K.; Ramesh, R.; Shimizu, E.; Nakayama, S.; Gandhi, P. A study establishing sensitivity and accuracy of smartphone photography in ophthalmologic community outreach programs: Review of a smart eye camera. Indian J. Ophthalmol. 2023, 71, 2416–2420. [Google Scholar] [CrossRef]
- Yazu, H.; Shimizu, E.; Okuyama, S.; Katahira, T.; Aketa, N.; Yokoiwa, R.; Sato, Y.; Ogawa, Y.; Fujishima, H. Evaluation of Nuclear Cataract with Smartphone-Attachable Slit-Lamp Device. Diagnostics 2020, 10, 576. [Google Scholar] [CrossRef]
- Shimizu, E.; Yazu, H.; Aketa, N.; Yokoiwa, R.; Sato, S.; Yajima, J.; Katayama, T.; Sato, R.; Tanji, M.; Sato, Y.; et al. A Study Validating the Estimation of Anterior Chamber Depth and Iridocorneal Angle with Portable and Non-Portable Slit-Lamp Microscopy. Sensors 2021, 21, 1436. [Google Scholar] [CrossRef]
- Yazu, H.; Shimizu, E.; Sato, S.; Aketa, N.; Katayama, T.; Yokoiwa, R.; Sato, Y.; Fukagawa, K.; Ogawa, Y.; Tsubota, K.; et al. Clinical Observation of Allergic Conjunctival Diseases with Portable and Recordable Slit-Lamp Device. Diagnostics 2021, 11, 535. [Google Scholar] [CrossRef]
- Shimizu, E.; Yazu, H.; Aketa, N.; Yokoiwa, R.; Sato, S.; Katayama, T.; Hanyuda, A.; Sato, Y.; Ogawa, Y.; Tsubota, K. Smart Eye Camera: A Validation Study for Evaluating the Tear Film Breakup Time in Human Subjects. Transl. Vis. Sci. Technol. 2021, 10, 28. [Google Scholar] [CrossRef]
- Shimizu, E.; Ogawa, Y.; Yazu, H.; Aketa, N.; Yang, F.; Yamane, M.; Sato, Y.; Kawakami, Y.; Tsubota, K. “Smart Eye Camera”: An innovative technique to evaluate tear film breakup time in a murine dry eye disease model. PLoS ONE 2019, 14, e0215130. [Google Scholar] [CrossRef]
- Sengupta, S.; Singh, A.; Leopold, H.; Gulati, T.; Lakshminarayanan, V. Ophthalmic diagnosis using deep learning with fundus images—A critical review. Artif. Intell. Med. 2020, 102, 101758. [Google Scholar] [CrossRef]
- Xu, B.; Chiang, M.; Chaudhary, S.; Kulkarni, S.; Pardeshi, A.; Varma, R. Deep Learning Classifiers for Automated Detection of Gonioscopic Angle Closure Based on Anterior Segment OCT Images. Am. J. Ophthalmol. 2019, 208, 273–280. [Google Scholar] [CrossRef]
- Christopher, M.; Bowd, C.; Belghith, A.; Goldbaum, M.; Weinreb, R.; Fazio, M.; Girkin, C.; Liebmann, J.; Zangwill, L. Deep Learning Approaches Predict Glaucomatous Visual Field Damage from OCT Optic Nerve Head En Face Images and Retinal Nerve Fiber Layer Thickness Maps. Ophthalmology 2019, 127, 346–356. [Google Scholar] [CrossRef]
- Wanichwecharungruang, B.; Kaothanthong, N.; Pattanapongpaiboon, W.; Chantangphol, P.; Seresirikachorn, K.; Srisuwanporn, C.; Parivisutt, N.; Grzybowski, A.; Theeramunkong, T.; Ruamviboonsuk, P. Deep Learning for Anterior Segment Optical Coherence Tomography to Predict the Presence of Plateau Iris. Transl. Vis. Sci. Technol. 2021, 10, 7. [Google Scholar] [CrossRef]
- Zheng, C.; Xie, X.; Wang, Z.; Li, W.; Chen, J.; Qiao, T.; Qian, Z.; Liu, H.; Liang, J.; Chen, X. Development and validation of deep learning algorithms for automated eye laterality detection with anterior segment photography. Sci. Rep. 2021, 11, 586. [Google Scholar] [CrossRef]
- Chase, C.; Elsawy, A.; Eleiwa, T.; Ozcan, E.; Tolba, M.; Shousha, M. Comparison of Autonomous AS-OCT Deep Learning Algorithm and Clinical Dry Eye Tests in Diagnosis of Dry Eye Disease. Clin. Ophthalmol. 2021, 15, 4281–4289. [Google Scholar] [CrossRef]
- Thakur, A.; Goldbaum, M.; Yousefi, S. Predicting Glaucoma before Onset Using Deep Learning. Ophthalmol. Glaucoma 2020, 3, 262–268. [Google Scholar] [CrossRef]
- Iao, W.; Zhang, W.; Wang, X.; Wu, Y.; Lin, D.; Lin, H. Deep Learning Algorithms for Screening and Diagnosis of Systemic Diseases Based on Ophthalmic Manifestations: A Systematic Review. Diagnostics 2023, 13, 900. [Google Scholar] [CrossRef]
- Madhura Prakash, M.; Prasad, D.K.; Kulkarni, M.S.; Spoorthi, K.; Venkatakrishnan, S. A Systematic Study of Deep Learning Architectures for Analysis of Glaucoma and Hypertensive Retinopathy. Int. J. Artif. Intell. Appl. 2022, 13, 33–49. [Google Scholar] [CrossRef]
- Rahimy, E. Deep learning applications in ophthalmology. Curr. Opin. Ophthalmol. 2018, 29, 254–260. [Google Scholar] [CrossRef] [PubMed]
- Aslam, T.; Shakir, S.; Wong, J.; Au, L.; Ashworth, J. Use of iris recognition camera technology for the quantification of corneal opacification in mucopolysaccharidoses. Br. J. Ophthalmol. 2012, 96, 1466–1468. [Google Scholar] [CrossRef]
- Sharif, M.; Qahwaji, R.; Ipson, S.; Brahma, A. Medical image classification based on artificial intelligence approaches: A practical study on normal and abnormal confocal corneal images. Appl. Soft Comput. 2015, 36, 269–282. [Google Scholar] [CrossRef]
- Shanthi, S.; Aruljyothi, L.; Balasundaram, M.; Janakiraman, A.; Nirmala, D.; Pyingkodi, M. Artificial intelligence applications in different imaging modalities for corneal topography. Surv. Ophthalmol. 2021, 67, 801–816. [Google Scholar] [CrossRef]
- Xie, Y.; Zhao, L.; Yang, X.; Wu, X.; Yang, Y.; Huang, X.; Liu, F.; Xu, J.; Lin, L.; Lin, H.; et al. Screening Candidates for Refractive Surgery with Corneal Tomographic-Based Deep Learning. JAMA Ophthalmol. 2020, 138, 519–526. [Google Scholar] [CrossRef]
- Tan, M.; Quoc, V.L. EfficientNet: Rethinking Model Scaling for Convolutional Neural Networks. arXiv 2019, arXiv:1905.11946. [Google Scholar]
- Zuiderveld, K. Contrast limited ADAPTIVE Histogram Equalization; In Graphics Gems Series: Graphics Gems; Academic Press: Cambridge, MA, USA, 1994; Volume IV, pp. 474–485. [Google Scholar]
- Ronneberger, O.; Fischer, P.; Brox, T. U-Net: Convolutional Networks for Biomedical Image Segmentation. In Medical Image Computing and Computer-Assisted Intervention–MICCAI 2015. MICCAI 2015; Lecture Notes in Computer Science; Navab, N., Hornegger, J., Wells, W., Frangi, A., Eds.; Springer: Cham, Switzerland, 2015; Volume 9351. [Google Scholar]
- Ueno, Y.; Oda, M.; Yamaguchi, T.; Fukuoka, H.; Nejima, R.; Kitaguchi, Y.; Miyake, M.; Akiyama, M.; Miyata, K.; Kashiwagi, K.; et al. Deep learning model for extensive smartphone-based diagnosis and triage of cataracts and multiple corneal diseases. Br. J. Ophthalmol. 2024. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Huang, Y.; Liu, Z.; Lai, W.; Long, E.; Zhang, K.; Jiang, J.; Lin, D.; Chen, K.; Yu, T.; et al. Universal artificial intelligence platform for collaborative management of cataracts. Br. J. Ophthalmol. 2019, 103, 1553–1560. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, E.; Tanji, M.; Nakayama, S.; Ishikawa, T.; Agata, N.; Yokoiwa, R.; Nishimura, H.; Khemlani, R.J.; Sato, S.; Hanyuda, A.; et al. AI-based diagnosis of nuclear cataract from slit-lamp videos. Sci. Rep. 2023, 13, 22046. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, E.; Ishikawa, T.; Tanji, M.; Agata, N.; Nakayama, S.; Nakahara, Y.; Yokoiwa, R.; Sato, S.; Hanyuda, A.; Ogawa, Y.; et al. Artificial intelligence to estimate the tear film breakup time and diagnose dry eye disease. Sci. Rep. 2023, 13, 5822. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Jiang, J.; Chen, K.; Chen, Q.; Zheng, Q.; Liu, X.; Weng, H.; Wu, S.; Chen, W. Preventing corneal blindness caused by keratitis using artificial intelligence. Nat. Commun. 2021, 12, 3738. [Google Scholar] [CrossRef] [PubMed]
- Hu, S.; Wang, X.; Wu, H.; Luan, X.; Qi, P.; Lin, Y.; He, X.; He, W. Unified Diagnosis Framework for Automated Nuclear Cataract Grading Based on Smartphone Slit-Lamp Images. IEEE Access 2020, 8, 174169–174178. [Google Scholar] [CrossRef]
- Son, K.Y.; Ko, J.; Kim, E.; Lee, S.Y.; Kim, M.J.; Han, J.; Shin, E.; Chung, T.Y.; Lim, D.H. Deep Learning-Based Cataract Detection and Grading from Slit-Lamp and Retro-Illumination Photographs: Model Development and Validation Study. Ophthalmol. Sci. 2022, 2, 100147. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Negative | Positive | Total | |
|---|---|---|---|
| train/val | 188 | 188 | 376 |
| test | 47 | 47 | 94 |
| Confusion Matrix | Value |
|---|---|
| True Positive | 45 |
| False Negative | 2 |
| False Positive | 2 |
| True Negative | 45 |
| Evaluation Index | Value |
|---|---|
| Sensitivity | 0.96 (95% CI. 0.97–0.99) |
| Specificity | 0.96 (95% CI. 0.97–0.99) |
| Accuracy | 0.96 (95% CI. 0.97–0.99) |
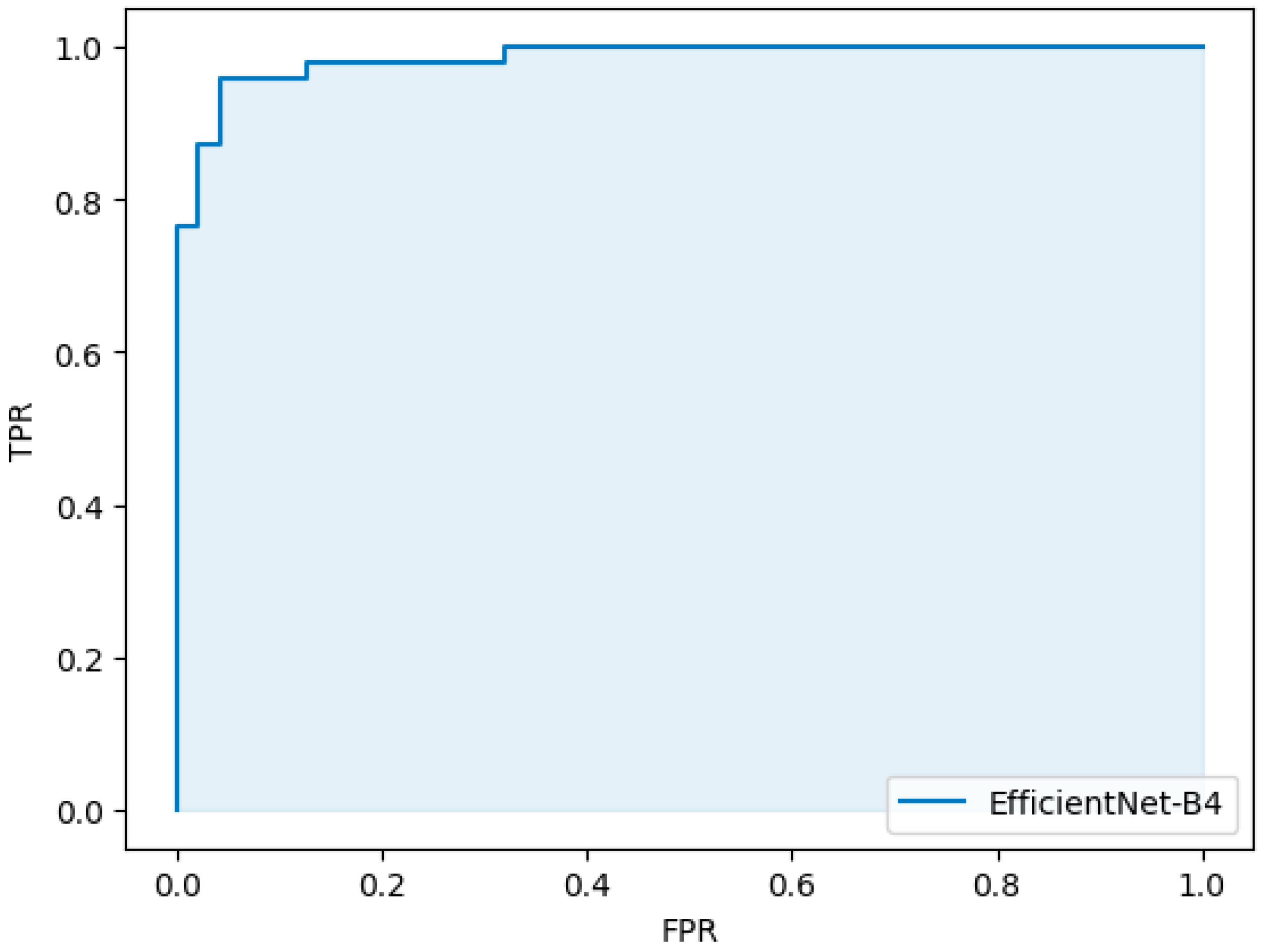
| AUC | 0.98 (95% CI. 0.98–0.99) |
| Evaluation Index | Value |
|---|---|
| dice | 0.94 |
| IoU | 0.94 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoshitsugu, K.; Shimizu, E.; Nishimura, H.; Khemlani, R.; Nakayama, S.; Takemura, T. Development of the AI Pipeline for Corneal Opacity Detection. Bioengineering 2024, 11, 273. https://doi.org/10.3390/bioengineering11030273
Yoshitsugu K, Shimizu E, Nishimura H, Khemlani R, Nakayama S, Takemura T. Development of the AI Pipeline for Corneal Opacity Detection. Bioengineering. 2024; 11(3):273. https://doi.org/10.3390/bioengineering11030273
Chicago/Turabian StyleYoshitsugu, Kenji, Eisuke Shimizu, Hiroki Nishimura, Rohan Khemlani, Shintaro Nakayama, and Tadamasa Takemura. 2024. "Development of the AI Pipeline for Corneal Opacity Detection" Bioengineering 11, no. 3: 273. https://doi.org/10.3390/bioengineering11030273