
Emerging Trends in Magnetic Resonance Fingerprinting for Quantitative Biomedical Imaging Applications: A Review
 , , , , and
, , , , and
Abstract
:1. Introduction
1.1. Overview of MRF
1.2. Related Works
1.3. Contributions
2. Emerging Trends in MRF Pulse Sequences
3. Emerging Trends in MRF Sequence Optimization
- Define metrics to measure the encoding capabilities of MRF acquisition strategies.
- Choose the algorithm that will be used to optimize the sequence parameters.
4. MRF Dictionary Generation
5. Emerging Trends in MRF Reconstruction
5.1. Dictionary-Based MRF Reconstructions
5.2. Dictionary- and Model-Based MRF Reconstructions
5.3. Deep Learning-Based MRF Reconstructions
5.4. Other MRF Reconstruction Frameworks
6. Emerging Trends in MRF Applications
6.1. Cardiac Imaging
6.2. Brain Imaging
6.3. Musculoskeletal Imaging
6.4. Abdomen Imaging
6.5. Radiotherapy, Tumors, and Cancer
6.6. Fat–Water Separation
7. Discussion and Future Outlook
8. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Jaberipour, M.; Soliman, H.; Sahgal, A.; Sadeghi-Naini, A. A priori prediction of local failure in brain metastasis after hypo-fractionated stereotactic radiotherapy using quantitative MRI and machine learning. Sci. Rep. 2021, 11, 21620. [Google Scholar] [CrossRef] [PubMed]
- Tippareddy, C.; Onyewadume, L.; Sloan, A.E.; Wang, G.M.; Patil, N.T.; Hu, S.; Barnholtz-Sloan, J.S.; Boyacıoğlu, R.; Gulani, V.; Sunshine, J.; et al. Novel 3D magnetic resonance fingerprinting radiomics in adult brain tumors: A feasibility study. Eur. Radiol. 2022, 33, 836–844. [Google Scholar] [CrossRef] [PubMed]
- Dastmalchian, S.; Kilinc, O.; Onyewadume, L.; Tippareddy, C.; McGivney, D.; Ma, D.; Griswold, M.; Sunshine, J.; Gulani, V.; Barnholtz-Sloan, J.S.; et al. Radiomic analysis of magnetic resonance fingerprinting in adult brain tumors. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 683–693. [Google Scholar] [CrossRef] [PubMed]
- Raynauld, J.-P.; Martel-Pelletier, J.; Berthiaume, M.-J.; Beaudoin, G.; Choquette, D.; Haraoui, B.; Tannenbaum, H.; Meyer, J.M.; Beary, J.F.; Cline, G.A.; et al. Long term evaluation of disease progression through the quantitative magnetic resonance imaging of symptomatic knee osteoarthritis patients: Correlation with clinical symptoms and radiographic changes. Arthritis Res. Ther. 2005, 8, R21. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.; Daducci, A.; He, Y.; Schiavi, S.; Seguin, C.; Smith, R.E.; Yeh, C.-H.; Zhao, T.; O’Donnell, L.J. Quantitative mapping of the brain’s structural connectivity using diffusion MRI tractography: A review. Neuroimage 2022, 249, 118870. [Google Scholar] [CrossRef] [PubMed]
- Zerunian, M.; Pucciarelli, F.; Caruso, D.; Polici, M.; Masci, B.; Guido, G.; de Santis, D.; Polverari, D.; Principessa, D.; Benvenga, A.; et al. Artificial intelligence based image quality enhancement in liver MRI: A quantitative and qualitative evaluation. Radiol. Med. 2022, 127, 1098–1105. [Google Scholar] [CrossRef]
- Ding, H.; Velasco, C.; Ye, H.; Lindner, T.; Grech-Sollars, M.; O’Callaghan, J.; Hiley, C.; Chouhan, M.; Niendorf, T.; Koh, D.-M.; et al. Current Applications and Future Development of Magnetic Resonance Fingerprinting in Diagnosis, Characterization, and Response Monitoring in Cancer. Cancers 2021, 13, 4742. [Google Scholar] [CrossRef]
- Ma, D.; Gulani, V.; Seiberlich, N.; Liu, K.; Sunshine, J.L.; Duerk, J.L.; Griswold, M.A. Magnetic resonance fingerprinting. Nature 2013, 495, 187–192. [Google Scholar] [CrossRef]
- Bipin Mehta, B.; Coppo, S.; Frances McGivney, D.; Ian Hamilton, J.; Chen, Y.; Jiang, Y.; Ma, D.; Seiberlich, N.; Gulani, V.; Alan Griswold, M. Magnetic resonance fingerprinting: A technical review. Magn. Reson. Med. 2019, 81, 25–46. [Google Scholar] [CrossRef]
- Poorman, M.E.; Martin, M.N.; Ma, D.; McGivney, D.F.; Gulani, V.; Griswold, M.A.; Keenan, K.E. Magnetic resonance fingerprinting Part 1: Potential uses, current challenges, and recommendations. J. Magn. Reson. Imaging 2020, 51, 675–692. [Google Scholar] [CrossRef]
- McGivney, D.F.; Boyacıoğlu, R.; Jiang, Y.; Poorman, M.E.; Seiberlich, N.; Gulani, V.; Keenan, K.E.; Griswold, M.A.; Ma, D. Magnetic resonance fingerprinting review part 2: Technique and directions. J. Magn. Reson. Imaging 2020, 51, 993–1007. [Google Scholar] [CrossRef]
- Hsieh, J.J.L.; Svalbe, I. Magnetic resonance fingerprinting: From evolution to clinical applications. J. Med. Radiat. Sci. 2020, 67, 333–344. [Google Scholar] [CrossRef]
- Cruz, G.; Jaubert, O.; Botnar, R.M.; Prieto, C. Cardiac Magnetic Resonance Fingerprinting: Technical Developments and Initial Clinical Validation. Curr. Cardiol. Rep. 2019, 21, 91. [Google Scholar] [CrossRef]
- Eck, B.L.; Flamm, S.D.; Kwon, D.H.; Tang, W.H.W.; Vasquez, C.P.; Seiberlich, N. Cardiac magnetic resonance fingerprinting: Trends in technical development and potential clinical applications. Prog. Nucl. Magn. Reson. Spectrosc. 2021, 122, 11–22. [Google Scholar] [CrossRef]
- Velasco, C.; Fletcher, T.J.; Botnar, R.M.; Prieto, C. Artificial intelligence in cardiac magnetic resonance fingerprinting. Front. Cardiovasc. Med. 2022, 9, 1009131. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Lu, L.; Zhu, T.; Ma, D. Technical overview of magnetic resonance fingerprinting and its applications in radiation therapy. Med. Phys. 2022, 49, 2846–2860. [Google Scholar] [CrossRef] [PubMed]
- Tippareddy, C.; Zhao, W.; Sunshine, J.L.; Griswold, M.; Ma, D.; Badve, C. Magnetic resonance fingerprinting: An overview. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 4189–4200. [Google Scholar] [CrossRef] [PubMed]
- Ganter, C. Off-resonance effects in the transient response of SSFP sequences. Magn. Reson. Med. 2004, 52, 368–375. [Google Scholar] [CrossRef]
- Jiang, Y.; Ma, D.; Seiberlich, N.; Gulani, V.; Griswold, M.A. MR fingerprinting using fast imaging with steady state precession (FISP) with spiral readout. Magn. Reson. Med. 2015, 76, 1621–1631. [Google Scholar] [CrossRef] [PubMed]
- Assländer, J.; Novikov, D.S.; Lattanzi, R.; Sodickson, D.K.; Cloos, M.A. Hybrid-state free precession in nuclear magnetic resonance. Commun. Phys. 2019, 2, 73. [Google Scholar] [CrossRef]
- Cloos, M.A.; Knoll, F.; Zhao, T.; Block, K.T.; Bruno, M.; Wiggins, G.C.; Sodickson, D.K. Multiparametric imaging with heterogeneous radiofrequency fields. Nat. Commun. 2016, 7, 12445. [Google Scholar] [CrossRef] [PubMed]
- Flassbeck, S.; Schmidt, S.; Bachert, P.; Ladd, M.E.; Schmitter, S. Flow MR fingerprinting. Magn. Reson. Med. 2019, 81, 2536–2550. [Google Scholar] [CrossRef] [PubMed]
- Boyacioglu, R.; Wang, C.; Ma, D.; McGivney, D.F.; Yu, X.; Griswold, M.A. 3D magnetic resonance fingerprinting with quadratic RF phase. Magn. Reson. Med. 2021, 85, 2084–2094. [Google Scholar] [CrossRef] [PubMed]
- Afzali, M.; Mueller, L.; Sakaie, K.; Hu, S.; Chen, Y.; Szczepankiewicz, F.; Griswold, M.A.; Jones, D.K.; Ma, D. MR Fingerprinting with b-Tensor Encoding for Simultaneous Quantification of Relaxation and Diffusion in a Single Scan. Magn. Reson. Med. 2022, 88, 2043–2057. [Google Scholar] [CrossRef] [PubMed]
- Wyatt, C.R.; Barbara, T.M.; Guimaraes, A.R. T1ρ magnetic resonance fingerprinting. NMR Biomed. 2020, 33, e4284. [Google Scholar] [CrossRef]
- Jiang, Y.; Ma, D.; Jerecic, R.; Duerk, J.; Seiberlich, N.; Gulani, V.; Griswold, M.A. MR fingerprinting using the quick echo splitting NMR imaging technique. Magn. Reson. Med. 2017, 77, 979–988. [Google Scholar] [CrossRef]
- Cohen, O.; Rosen, M.S. Algorithm comparison for schedule optimization in MR fingerprinting. Magn. Reson. Imaging 2017, 41, 15–21. [Google Scholar] [CrossRef]
- Sommer, K.; Amthor, T.; Doneva, M.; Koken, P.; Meineke, J.; Börnert, P. Towards predicting the encoding capability of MR fingerprinting sequences. Magn. Reson. Imaging 2017, 41, 7–14. [Google Scholar] [CrossRef]
- Kara, D.; Fan, M.; Hamilton, J.; Griswold, M.; Seiberlich, N.; Brown, R. Parameter map error due to normal noise and aliasing artifacts in MR fingerprinting. Magn. Reson. Med. 2019, 81, 3108–3123. [Google Scholar] [CrossRef]
- Jordan, S.P.; Hu, S.; Rozada, I.; McGivney, D.F.; Boyacioğlu, R.; Jacob, D.C.; Huang, S.; Beverland, M.; Katzgraber, H.G.; Troyer, M.; et al. Automated design of pulse sequences for magnetic resonance fingerprinting using physics-inspired optimization. Proc. Natl. Acad. Sci. USA 2021, 118, e2020516118. [Google Scholar] [CrossRef]
- Aarts, E.H.L.; van Laarhoven, P.J.M. Simulated annealing: An introduction. Stat. Neerl. 1989, 43, 31–52. [Google Scholar] [CrossRef]
- Glynn, P.W. Stochastic approximation for Monte Carlo optimization. In Proceedings of the 18th Conference on Winter Simulation—WSC’86, Washington, DC, USA, 8–10 December 1986; ACM Press: New York, NY, USA, 1986; pp. 356–365. [Google Scholar] [CrossRef]
- Zhao, B.; Haldar, J.P.; Liao, C.; Ma, D.; Jiang, Y.; Griswold, M.A.; Setsompop, K.; Wald, L.L. Optimal experiment design for magnetic resonance fingerprinting: Cramér-rao bound meets spin dynamics. IEEE Trans. Med. Imaging 2019, 38, 844–861. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.K.; Watkins, L.E.; Anderson, T.I.; Buonincontri, G.; Hargreaves, B.A. Flexible and efficient optimization of quantitative sequences using automatic differentiation of Bloch simulations. Magn. Reson. Med. 2019, 82, 1438–1451. [Google Scholar] [CrossRef] [PubMed]
- Crafts, E.S.; Lu, H.; Ye, H.; Wald, L.L.; Zhao, B. An efficient approach to optimal experimental design for magnetic resonance fingerprinting with B-splines. Magn. Reson. Med. 2022, 88, 239–253. [Google Scholar] [CrossRef] [PubMed]
- Kang, B.; Kim, B.; Park, H.; Heo, H. Learning-based optimization of acquisition schedule for magnetization transfer contrast MR fingerprinting. NMR Biomed. 2022, 35, e4662. [Google Scholar] [CrossRef]
- Cohen, O.; Otazo, R. Global deep learning optimization of chemical exchange saturation transfer magnetic resonance fingerprinting acquisition schedule. NMR Biomed. 2023, 36, e4954. [Google Scholar] [CrossRef]
- Weigel, M. Extended phase graphs: Dephasing, RF pulses, and echoes—Pure and simple. J. Magn. Reson. Imaging 2015, 41, 266–295. [Google Scholar] [CrossRef]
- Malik, S.J.; Teixeira, R.P.A.G.; Hajnal, J.V. Extended phase graph formalism for systems with magnetization transfer and exchange. Magn. Reson. Med. 2018, 80, 767–779. [Google Scholar] [CrossRef]
- Ostenson, J.; Smith, D.S.; Does, M.D.; Damon, B.M. Slice-selective extended phase graphs in gradient-crushed, transient-state free precession sequences: An application to MR fingerprinting. Magn. Reson. Med. 2020, 84, 3409–3422. [Google Scholar] [CrossRef] [PubMed]
- Weigel, M.; Schwenk, S.; Kiselev, V.G.; Scheffler, K.; Hennig, J. Extended phase graphs with anisotropic diffusion. J. Magn. Reson. 2010, 205, 276–285. [Google Scholar] [CrossRef]
- Gao, X.; Kiselev, V.G.; Lange, T.; Hennig, J.; Zaitsev, M. Three-dimensional spatially resolved phase graph framework. Magn. Reson. Med. 2021, 86, 551–560. [Google Scholar] [CrossRef]
- Guenthner, C.; Amthor, T.; Doneva, M.; Kozerke, S. A unifying view on extended phase graphs and Bloch simulations for quantitative MRI. Sci. Rep. 2021, 11, 21289. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Hu, Y. Learned Tensor Low-CP-Rank and Bloch Response Manifold Priors for Non-Cartesian MRF Reconstruction. IEEE Trans. Med. Imaging 2023, 42, 3702–3714. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Li, P.; Chen, H.; Zou, L.; Wang, H. High-Quality MR Fingerprinting Reconstruction Using Structured Low-Rank Matrix Completion and Subspace Projection. IEEE Trans. Med. Imaging 2022, 41, 1150–1164. [Google Scholar] [CrossRef] [PubMed]
- McGivney, D.F.; Pierre, E.; Ma, D.; Jiang, Y.; Saybasili, H.; Gulani, V.; Griswold, M.A. SVD Compression for Magnetic Resonance Fingerprinting in the Time Domain. IEEE Trans. Med. Imaging 2014, 33, 2311–2322. [Google Scholar] [CrossRef] [PubMed]
- Cauley, S.F.; Setsompop, K.; Ma, D.; Jiang, Y.; Ye, H.; Adalsteinsson, E.; Griswold, M.A.; Wald, L.L. Fast group matching for MR fingerprinting reconstruction. Magn. Reson. Med. 2015, 74, 523–528. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Zhang, J.; Cui, D.; Xie, J.; Lyu, M.; Hui, E.S.; Wu, E.X. Magnetic Resonance Fingerprinting Using a Fast Dictionary Searching Algorithm: MRF-ZOOM. IEEE Trans. Biomed. Eng. 2019, 66, 1526–1535. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.S.; Kim, S.; Yoo, D.; Shin, T.H.; Kim, H.; Gomes, M.D.; Kim, S.H.; Pines, A.; Cheon, J. Distance-dependent magnetic resonance tuning as a versatile MRI sensing platform for biological targets. Nat. Mater. 2017, 16, 537–542. [Google Scholar] [CrossRef]
- Bar-Hillel, A.; Hertz, T.; Shental, N.; Weinshall, D. Learning distance functions using equivalence relations. In Proceedings of the Twentieth International Conference on International Conference on Machine Learning, in ICML’03, Washington DC, USA, 21–24 August 2003; AAAI Press: Washington, DC, USA, 2003; pp. 11–18. [Google Scholar]
- Davies, M.; Puy, G.; Vandergheynst, P.; Wiaux, Y. A Compressed Sensing Framework for Magnetic Resonance Fingerprinting. SIAM J. Imaging Sci. 2014, 7, 2623–2656. [Google Scholar] [CrossRef]
- Mazor, G.; Weizman, L.; Tal, A.; Eldar, Y.C. Low-rank magnetic resonance fingerprinting. Med. Phys. 2018, 45, 4066–4084. [Google Scholar] [CrossRef]
- Zhao, B. Model-based iterative reconstruction for magnetic resonance fingerprinting. In Proceedings of the 2015 IEEE International Conference on Image Processing (ICIP), Quebec City, QC, Canada, 27–30 September 2015; pp. 3392–3396. [Google Scholar] [CrossRef]
- Zhao, B.; Setsompop, K.; Adalsteinsson, E.; Gagoski, B.; Ye, H.; Ma, D.; Jiang, Y.; Ellen Grant, P.; Griswold, M.A.; Wald, L.L. Improved magnetic resonance fingerprinting reconstruction with low-rank and subspace modeling. Magn. Reson. Med. 2018, 79, 933–942. [Google Scholar] [CrossRef]
- Assländer, J.; Cloos, M.A.; Knoll, F.; Sodickson, D.K.; Hennig, J.; Lattanzi, R. Low rank alternating direction method of multipliers reconstruction for MR fingerprinting. Magn. Reson. Med. 2018, 79, 83–96. [Google Scholar] [CrossRef] [PubMed]
- Boux, F.; Forbes, F.; Arbel, J.; Lemasson, B.; Barbier, E.L. Bayesian Inverse Regression for Vascular Magnetic Resonance Fingerprinting. IEEE Trans. Med. Imaging 2021, 40, 1827–1837. [Google Scholar] [CrossRef]
- McGivney, D.; Deshmane, A.; Jiang, Y.; Ma, D.; Badve, C.; Sloan, A.; Gulani, V.; Griswold, M. Bayesian estimation of multicomponent relaxation parameters in magnetic resonance fingerprinting. Magn. Reson. Med. 2018, 80, 159–170. [Google Scholar] [CrossRef]
- Cohen, O.; Zhu, B.; Rosen, M.S. MR fingerprinting Deep RecOnstruction NEtwork (DRONE). Magn. Reson. Med. 2018, 80, 885–894. [Google Scholar] [CrossRef]
- Barbieri, M.; Lee, P.K.; Brizi, L.; Giampieri, E.; Solera, F.; Castellani, G.; Hargreaves, B.A.; Testa, C.; Lodi, R.; Remondini, D. Circumventing the curse of dimensionality in magnetic resonance fingerprinting through a deep learning approach. NMR Biomed. 2022, 35, e4670. [Google Scholar] [CrossRef] [PubMed]
- Cabini, R.F.; Barzaghi, L.; Cicolari, D.; Arosio, P.; Carrazza, S.; Figini, S.; Filibian, M.; Gazzano, A.; Krause, R.; Mariani, M.; et al. Fast deep learning reconstruction techniques for preclinical magnetic resonance fingerprinting. NMR Biomed. 2024, 37, e5028. [Google Scholar] [CrossRef]
- Soyak, R.; Navruz, E.; Ersoy, E.O.; Cruz, G.; Prieto, C.; King, A.P.; Unay, D.; Oksuz, I. Channel Attention Networks for Robust MR Fingerprint Matching. IEEE Trans. Biomed. Eng. 2022, 69, 1398–1405. [Google Scholar] [CrossRef] [PubMed]
- Fang, Z.; Chen, Y.; Hung, S.C.; Zhang, X.; Lin, W.; Shen, D. Submillimeter MR fingerprinting using deep learning–based tissue quantification. Magn. Reson. Med. 2020, 84, 579–591. [Google Scholar] [CrossRef]
- Lu, H.; Ye, H.; Wald, L.L.; Zhao, B. Accelerated MR Fingerprinting with Low-Rank and Generative Subspace Modeling. arXiv 2023, arXiv:2305.10651. [Google Scholar]
- Chen, D.; Davies, M.E.; Golbabaee, M. Deep Unrolling for Magnetic Resonance Fingerprinting. In Proceedings of the 2022 IEEE 19th International Symposium on Biomedical Imaging (ISBI), Kolkata, India, 28–31 March 2022; pp. 1–4. [Google Scholar] [CrossRef]
- Tang, S.; Fernandez-Granda, C.; Lannuzel, S.; Bernstein, B.; Lattanzi, R.; Cloos, M.; Knoll, F.; Assländer, J. Multicompartment magnetic resonance fingerprinting. Inverse Probl. 2018, 34, 094005. [Google Scholar] [CrossRef]
- Nagtegaal, M.; Koken, P.; Amthor, T.; Doneva, M. Fast multi-component analysis using a joint sparsity constraint for MR fingerprinting. Magn. Reson. Med. 2020, 83, 521–534. [Google Scholar] [CrossRef]
- Deshmane, A.; McGivney, D.F.; Ma, D.; Jiang, Y.; Badve, C.; Gulani, V.; Seiberlich, N.; Griswold, M.A. Partial volume mapping using magnetic resonance fingerprinting. NMR Biomed. 2019, 32, e4082. [Google Scholar] [CrossRef]
- Hamilton, J.I.; Currey, D.; Rajagopalan, S.; Seiberlich, N. Deep learning reconstruction for cardiac magnetic resonance fingerprinting T1 and T2 mapping. Magn. Reson. Med. 2021, 85, 2127–2135. [Google Scholar] [CrossRef] [PubMed]
- Cruz, G.; Jaubert, O.; Schneider, T.; Botnar, R.M.; Prieto, C. Rigid motion-corrected magnetic resonance fingerprinting. Magn. Reson. Med. 2019, 81, 947–961. [Google Scholar] [CrossRef] [PubMed]
- Cruz, G.; Qi, H.; Jaubert, O.; Kuestner, T.; Schneider, T.; Botnar, R.M.; Prieto, C. Generalized low-rank nonrigid motion-corrected reconstruction for MR fingerprinting. Magn. Reson. Med. 2022, 87, 746–763. [Google Scholar] [CrossRef] [PubMed]
- Lu, H.; Ye, H.; Zhao, B. Improved Balanced Steady-State Free Precession Based MR Fingerprinting with Deep Autoencoders. In Proceedings of the 2022 44th Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Glasgow, UK, 11–15 July 2022; pp. 3029–3034. [Google Scholar] [CrossRef]
- Coronado, R.; Cruz, G.; Castillo-Passi, C.; Tejos, C.; Uribe, S.; Prieto, C.; Irarrazaval, P. A Spatial Off-Resonance Correction in Spirals for Magnetic Resonance Fingerprinting. IEEE Trans. Med. Imaging 2021, 40, 3832–3842. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Doneva, M.; Meineke, J.; Amthor, T.; Karasan, E.; Tan, F.; Tamir, J.I.; Yu, S.X.; Lustig, M. High-fidelity direct contrast synthesis from magnetic resonance fingerprinting. Magn. Reson. Med. 2023, 90, 2116–2129. [Google Scholar] [CrossRef] [PubMed]
- Nykänen, O.; Nevalainen, M.; Casula, V.; Isosalo, A.; Inkinen, S.I.; Nikki, M.; Lattanzi, R.; Cloos, M.A.; Nissi, M.J.; Nieminen, M.T. Deep-Learning-Based Contrast Synthesis from MRF Parameter Maps in the Knee Joint. J. Magn. Reson. Imaging 2023, 58, 559–568. [Google Scholar] [CrossRef]
- Cruz, G.; Jaubert, O.; Qi, H.; Bustin, A.; Milotta, G.; Schneider, T.; Koken, P.; Doneva, M.; Botnar, R.M.; Prieto, C. 3D free-breathing cardiac magnetic resonance fingerprinting. NMR Biomed. 2020, 33, e4370. [Google Scholar] [CrossRef] [PubMed]
- Rashid, I.; Al-Kindi, S.; Rajagopalan, V.; Walker, J.; Rajagopalan, S.; Seiberlich, N.; Hamilton, J.I. Synthetic multi-contrast late gadolinium enhancement imaging using post-contrast magnetic resonance fingerprinting. NMR Biomed. 2024, 37, e5043. [Google Scholar] [CrossRef] [PubMed]
- Jaubert, O.; Cruz, G.; Bustin, A.; Schneider, T.; Lavin, B.; Koken, P.; Hajhosseiny, R.; Doneva, M.; Rueckert, D.; Botnar, R.M.; et al. Water–fat Dixon cardiac magnetic resonance fingerprinting. Magn. Reson. Med. 2020, 83, 2107–2123. [Google Scholar] [CrossRef] [PubMed]
- Velasco, C.; Cruz, G.; Lavin, B.; Hua, A.; Fotaki, A.; Botnar, R.M.; Prieto, C. Simultaneous T1, T2, and T1ρ cardiac magnetic resonance fingerprinting for contrast agent–free myocardial tissue characterization. Magn. Reson. Med. 2022, 87, 1992–2002. [Google Scholar] [CrossRef]
- Fan, H.; Bunker, L.; Wang, Z.; Durfee, A.Z.; Lin, D.; Yedavalli, V.; Ge, Y.; Zhou, X.J.; Hillis, A.E.; Lu, H. Simultaneous perfusion, diffusion, T2*, and T1 mapping with MR fingerprinting. Magn. Reson. Med. 2024, 91, 558–569. [Google Scholar] [CrossRef] [PubMed]
- Cohen, O.; Yu, V.Y.; Tringale, K.R.; Young, R.J.; Perlman, O.; Farrar, C.T.; Otazo, R. CEST MR fingerprinting (CEST-MRF) for brain tumor quantification using EPI readout and deep learning reconstruction. Magn. Reson. Med. 2023, 89, 233–249. [Google Scholar] [CrossRef] [PubMed]
- Su, P.; Fan, H.; Liu, P.; Li, Y.; Qiao, Y.; Hua, J.; Lin, D.; Jiang, D.; Pillai, J.J.; Hillis, A.E.; et al. MR fingerprinting ASL: Sequence characterization and comparison with dynamic susceptibility contrast (DSC) MRI. NMR Biomed. 2020, 33, e4202. [Google Scholar] [CrossRef]
- Keil, V.C.; Bakoeva, S.P.; Jurcoane, A.; Doneva, M.; Amthor, T.; Koken, P.; Mädler, B.; Lüchters, G.; Block, W.; Wüllner, U.; et al. A pilot study of magnetic resonance fingerprinting in Parkinson’s disease. NMR Biomed. 2020, 33, e4389. [Google Scholar] [CrossRef]
- Lahiri, A.; Fessler, J.A.; Hernandez-Garcia, L. Optimizing MRF-ASL scan design for precise quantification of brain hemodynamics using neural network regression. Magn. Reson. Med. 2020, 83, 1979–1991. [Google Scholar] [CrossRef]
- Kurzawski, J.W.; Cencini, M.; Peretti, L.; Gómez, P.A.; Schulte, R.F.; Donatelli, G.; Cosottini, M.; Cecchi, P.; Costagli, M.; Retico, A.; et al. Retrospective rigid motion correction of three-dimensional magnetic resonance fingerprinting of the human brain. Magn. Reson. Med. 2020, 84, 2606–2615. [Google Scholar] [CrossRef]
- Yu, Z.; Madelin, G.; Sodickson, D.K.; Cloos, M.A. Simultaneous proton magnetic resonance fingerprinting and sodium MRI. Magn. Reson. Med. 2020, 83, 2232–2242. [Google Scholar] [CrossRef]
- Sharafi, A.; Zibetti, M.V.W.; Chang, G.; Cloos, M.; Regatte, R.R. 3D magnetic resonance fingerprinting for rapid simultaneous T1, T2, and T1ρ volumetric mapping of human articular cartilage at 3 T. NMR Biomed. 2022, 35, e4800. [Google Scholar] [CrossRef]
- Li, Q.; Cao, X.; Ye, H.; Liao, C.; He, H.; Zhong, J. Ultrashort echo time magnetic resonance fingerprinting (UTE-MRF) for simultaneous quantification of long and ultrashort T2 tissues. Magn. Reson. Med. 2019, 82, 1359–1372. [Google Scholar] [CrossRef]
- Sharafi, A.; Medina, K.; Zibetti, M.W.V.; Rao, S.; Cloos, M.A.; Brown, R.; Regatte, R.R. Simultaneous T1, T2, and T1ρ relaxation mapping of the lower leg muscle with MR fingerprinting. Magn. Reson. Med. 2021, 86, 372–381. [Google Scholar] [CrossRef]
- Koolstra, K.; Webb, A.G.; Veeger, T.T.J.; Kan, H.E.; Koken, P.; Börnert, P. Water–fat separation in spiral magnetic resonance fingerprinting for high temporal resolution tissue relaxation time quantification in muscle. Magn. Reson. Med. 2020, 84, 646–662. [Google Scholar] [CrossRef]
- Cencini, M.; Biagi, L.; Kaggie, J.D.; Schulte, R.F.; Tosetti, M.; Buonincontri, G. Magnetic resonance fingerprinting with dictionary-based fat and water separation (DBFW MRF): A multi-component approach. Magn. Reson. Med. 2019, 81, 3032–3045. [Google Scholar] [CrossRef] [PubMed]
- Sharafi, A.; Zibetti, M.V.W.; Chang, G.; Cloos, M.A.; Regatte, R.R. Simultaneous bilateral T1, T2, and T1ρ relaxation mapping of the hip joint with magnetic resonance fingerprinting. NMR Biomed. 2022, 35, e4651. [Google Scholar] [CrossRef] [PubMed]
- Cloos, M.A.; Assländer, J.; Abbas, B.; Fishbaugh, J.; Babb, J.S.; Gerig, G.; Lattanzi, R. Rapid Radial T1 and T2 Mapping of the Hip Articular Cartilage with Magnetic Resonance Fingerprinting. J. Magn. Reson. Imaging 2019, 50, 810–815. [Google Scholar] [CrossRef] [PubMed]
- Panda, A.; Chen, Y.; Ropella-Panagis, K.; Ghodasara, S.; Stopchinski, M.; Seyfried, N.; Wright, K.; Seiberlich, N.; Griswold, M.; Gulani, V. Repeatability and reproducibility of 3D MR fingerprinting relaxometry measurements in normal breast tissue. J. Magn. Reson. Imaging 2019, 50, 1133–1143. [Google Scholar] [CrossRef] [PubMed]
- Nolte, T.; Gross-Weege, N.; Doneva, M.; Koken, P.; Elevelt, A.; Truhn, D.; Kuhl, C.; Schulz, V. Spiral blurring correction with water–fat separation for magnetic resonance fingerprinting in the breast. Magn. Reson. Med. 2020, 83, 1192–1207. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.S.; Boyacioglu, R.; Bolding, R.; MacAskill, C.; Chen, Y.; Griswold, M.A. Free-Breathing Abdominal Magnetic Resonance Fingerprinting Using a Pilot Tone Navigator. J. Magn. Reson. Imaging 2021, 54, 1138–1151. [Google Scholar] [CrossRef] [PubMed]
- Serrao, E.M.; Kessler, D.A.; Carmo, B.; Beer, L.; Brindle, K.M.; Buonincontri, G.; Gallagher, F.A.; Gilbert, F.J.; Godfrey, E.; Graves, M.J.; et al. Magnetic resonance fingerprinting of the pancreas at 1.5 T and 3.0 T. Sci. Rep. 2020, 10, 17563. [Google Scholar] [CrossRef]
- Hermann, I.; Chacon-Caldera, J.; Brumer, I.; Rieger, B.; Weingärtner, S.; Schad, L.R.; Zöllner, F.G. Magnetic resonance fingerprinting for simultaneous renal T1 and T2* mapping in a single breath-hold. Magn. Reson. Med. 2020, 83, 1940–1948. [Google Scholar] [CrossRef] [PubMed]
- Velasco, C.; Cruz, G.; Jaubert, O.; Lavin, B.; Botnar, R.M.; Prieto, C. Simultaneous comprehensive liver T1, T2, T1ρ, and fat fraction characterization with MR fingerprinting. Magn. Reson. Med. 2022, 87, 1980–1991. [Google Scholar] [CrossRef]
- Kaggie, J.D.; Graves, M.J.; Gallagher, F.A.; Deen, S.; Kessler, D.A.; McLean, M.A.; Buonincontri, G.; Schulte, R.F.; Addley, H.; Sala, E.; et al. Feasibility of Quantitative Magnetic Resonance Fingerprinting in Ovarian Tumors for T1 and T2 Mapping in a PET/MR Setting. IEEE Trans. Radiat. Plasma Med. Sci. 2019, 3, 509–515. [Google Scholar] [CrossRef] [PubMed]
- Koolstra, K.; Beenakker, J.-W.M.; Koken, P.; Webb, A.; Börnert, P. Cartesian MR fingerprinting in the eye at 7T using compressed sensing and matrix completion-based reconstructions. Magn. Reson. Med. 2019, 81, 2551–2565. [Google Scholar] [CrossRef]
- Hamilton, J.I.; Jiang, Y.; Chen, Y.; Ma, D.; Lo, W.-C.; Griswold, M.; Seiberlich, N. MR fingerprinting for rapid quantification of myocardial T1, T2, and proton spin density. Magn. Reson. Med. 2017, 77, 1446–1458. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, J.I.; Jiang, Y.; Ma, D.; Chen, Y.; Lo, W.; Griswold, M.; Seiberlich, N. Simultaneous multislice cardiac magnetic resonance fingerprinting using low rank reconstruction. NMR Biomed. 2019, 32, e4041. [Google Scholar] [CrossRef]
- Hamilton, J.I.; Pahwa, S.; Adedigba, J.; Frankel, S.; O’Connor, G.; Thomas, R.; Walker, J.R.; Killinc, O.; Lo, W.-C.; Batesole, J.; et al. Simultaneous Mapping of T1 and T2 Using Cardiac Magnetic Resonance Fingerprinting in a Cohort of Healthy Subjects at 1.5T. J. Magn. Reson. Imaging 2020, 52, 1044–1052. [Google Scholar] [CrossRef]
- Hamilton, J.I.; Jiang, Y.; Eck, B.; Griswold, M.; Seiberlich, N. Cardiac cine magnetic resonance fingerprinting for combined ejection fraction, T1 and T2 quantification. NMR Biomed. 2020, 33, 8. [Google Scholar] [CrossRef]
- Rumac, S.; Pavon, A.G.; Hamilton, J.I.; Rodrigues, D.; Seiberlich, N.; Schwitter, J.; van Heeswijk, R.B. Cardiac MR fingerprinting with a short acquisition window in consecutive patients referred for clinical CMR and healthy volunteers. Sci. Rep. 2022, 12, 18705. [Google Scholar] [CrossRef]
- Rieger, B.; Akçakaya, M.; Pariente, J.C.; Llufriu, S.; Martinez-Heras, E.; Weingärtner, S.; Schad, L.R. Time efficient whole-brain coverage with MR Fingerprinting using slice-interleaved echo-planar-imaging. Sci. Rep. 2018, 8, 6667. [Google Scholar] [CrossRef] [PubMed]
- Ma, D.; Jiang, Y.; Chen, Y.; McGivney, D.; Mehta, B.; Gulani, V.; Griswold, M. Fast 3D magnetic resonance fingerprinting for a whole-brain coverage. Magn. Reson. Med. 2018, 79, 2190–2197. [Google Scholar] [CrossRef] [PubMed]
- Menon, R.G.; Monga, A.; Kijowski, R.; Regatte, R.R. Characterization of Age-Related and Sex-Related Differences of Relaxation Parameters in the Intervertebral Disc Using MR-Fingerprinting. J. Magn. Reson. Imaging 2023. [Google Scholar] [CrossRef] [PubMed]
- Mickevicius, N.J.; Kim, J.P.; Zhao, J.; Morris, Z.S.; Hurst, N.J.; Glide-Hurst, C.K. Toward magnetic resonance fingerprinting for low-field MR-guided radiation therapy. Med. Phys. 2021, 48, 6930–6940. [Google Scholar] [CrossRef]
- Panda, A.; Chen, Y.; Ropella-Panagis, K.; Ghodasara, S.; Stopchinski, M.; Seyfried, N.; Wright, K.; Seiberlich, N.; Griswold, M.; Gulani, V. MR Fingerprinting and ADC Mapping for Characterization of Lesions in the Transition Zone of the Prostate Gland. Radiology 2019, 292, 685–694. [Google Scholar] [CrossRef]
- Panda, A.; O’Connor, G.; Lo, W.C.; Jiang, Y.; Margevicius, S.; Schluchter, M.; Ponsky, L.E.; Gulani, V. Targeted Biopsy Validation of Peripheral Zone Prostate Cancer Characterization With Magnetic Resonance Fingerprinting and Diffusion Mapping. Investig. Radiol. 2019, 54, 485–493. [Google Scholar] [CrossRef]
- Zibetti, M.V.W.; Herman, G.T.; Regatte, R.R. Fast data-driven learning of parallel MRI sampling patterns for large scale problems. Sci. Rep. 2021, 11, 19312. [Google Scholar] [CrossRef]
- Radhakrishna, C.G.; Ciuciu, P. Jointly Learning Non-Cartesian k-Space Trajectories and Reconstruction Networks for 2D and 3D MR Imaging through Projection. Bioengineering 2023, 10, 158. [Google Scholar] [CrossRef]
- Wang, G.; Luo, T.; Nielsen, J.-F.; Noll, D.C.; Fessler, J.A. B-Spline Parameterized Joint Optimization of Reconstruction and K-Space Trajectories (BJORK) for Accelerated 2D MRI. IEEE Trans. Med. Imaging 2022, 41, 2318–2330. [Google Scholar] [CrossRef]
- Stolk, C.C.; Sbrizzi, A. Understanding the Combined Effect of k-Space Undersampling and Transient States Excitation in MR Fingerprinting Reconstructions. IEEE Trans. Med. Imaging 2019, 38, 2445–2455. [Google Scholar] [CrossRef] [PubMed]
- Sarracanie, M. Fast Quantitative Low-Field Magnetic Resonance Imaging With OPTIMUM—Optimized Magnetic Resonance Fingerprinting Using a Stationary Steady-State Cartesian Approach and Accelerated Acquisition Schedules. Investig. Radiol. 2022, 57, 263–271. [Google Scholar] [CrossRef]
- O’Reilly, T.; Börnert, P.; Liu, H.; Webb, A.; Koolstra, K. 3D magnetic resonance fingerprinting on a low-field 50 mT point-of-care system prototype: Evaluation of muscle and lipid relaxation time mapping and comparison with standard techniques. Magn. Reson. Mater. Phys. Biol. Med. 2023, 36, 499–512. [Google Scholar] [CrossRef]
- Campbell-Washburn, A.E.; Jiang, Y.; Körzdörfer, G.; Nittka, M.; Griswold, M.A. Feasibility of MR fingerprinting using a high-performance 0.55 T MRI system. Magn. Reson. Imaging 2021, 81, 88–93. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Hamilton, J.; Jiang, Y.; Seiberlich, N. Assessment of MRF for simultaneous T1 and T2 quantification and water–fat separation in the liver at 0.55 T. Magn. Reson. Mater. Phys. Biol. Med. 2023, 36, 513–523. [Google Scholar] [CrossRef] [PubMed]
- Buonincontri, G.; Schulte, R.F.; Cosottini, M.; Tosetti, M. Spiral MR fingerprinting at 7T with simultaneous B1 estimation. Magn. Reson. Imaging 2017, 41, 1–6. [Google Scholar] [CrossRef]
- Cervelli, R.; Cencini, M.; Buonincontri, G.; Campana, F.; Cacciato Insilla, A.; Aringhieri, G.; de Simone, P.; Boggi, U.; Campani, D.; Tosetti, M.; et al. 7-T MRI of explanted liver and ex-vivo pancreatic specimens: Prospective study protocol of radiological-pathological correlation feasibility (the EXLIPSE project). Eur. Radiol. Exp. 2020, 4, 58. [Google Scholar] [CrossRef] [PubMed]
- Perlman, O.; Zhu, B.; Zaiss, M.; Rosen, M.S.; Farrar, C.T. An end-to-end AI-based framework for automated discovery of rapid CEST/MT MRI acquisition protocols and molecular parameter quantification (AutoCEST). Magn. Reson. Med. 2022, 87, 2792–2810. [Google Scholar] [CrossRef]
- Gu, Y.; Wang, L.; Yang, H.; Wu, Y.; Kim, K.; Zhu, Y.; Androjna, C.; Zhu, X.; Chen, Y.; Zhong, K.; et al. Three-dimensional high-resolution T1 and T2 mapping of whole macaque brain at 9.4 T using magnetic resonance fingerprinting. Magn. Reson. Med. 2022, 87, 2901–2913. [Google Scholar] [CrossRef]
- Jiang, Y.; Ma, D.; Keenan, K.E.; Stupic, K.F.; Gulani, V.; Griswold, M.A. Repeatability of magnetic resonance fingerprinting T1 and T2 estimates assessed using the ISMRM/NIST MRI system phantom. Magn. Reson. Med. 2017, 78, 1452–1457. [Google Scholar] [CrossRef]
- Shridhar Konar, A.; Qian, E.; Geethanath, S.; Buonincontri, G.; Obuchowski, N.A.; Fung, M.; Gomez, P.; Schulte, R.; Cencini, M.; Tosetti, M.; et al. Quantitative imaging metrics derived from magnetic resonance fingerprinting using ISMRM/NIST MRI system phantom: An international multicenter repeatability and reproducibility study. Med. Phys. 2021, 48, 2438–2447. [Google Scholar] [CrossRef]
- Lo, W.; Bittencourt, L.K.; Panda, A.; Jiang, Y.; Tokuda, J.; Seethamraju, R.; Tempany-Afdhal, C.; Obmann, V.; Wright, K.; Griswold, M.; et al. Multicenter Repeatability and Reproducibility of MR Fingerprinting in Phantoms and in Prostatic Tissue. Magn. Reson. Med. 2022, 88, 1818–1827. [Google Scholar] [CrossRef] [PubMed]
- Buonincontri, G.; Biagi, L.; Retico, A.; Cecchi, P.; Cosottini, M.; Gallagher, F.A.; Gómez, P.A.; Graves, M.J.; McLean, M.A.; Riemer, F.; et al. Multi-site repeatability and reproducibility of MR fingerprinting of the healthy brain at 1.5 and 3.0 T. Neuroimage 2019, 195, 362–372. [Google Scholar] [CrossRef] [PubMed]
- Körzdörfer, G.; Kirsch, R.; Liu, K.; Pfeuffer, J.; Hensel, B.; Jiang, Y.; Ma, D.; Gratz, M.; Bär, P.; Bogner, W.; et al. Reproducibility and Repeatability of MR Fingerprinting Relaxometry in the Human Brain. Radiology 2019, 292, 429–437. [Google Scholar] [CrossRef] [PubMed]
- Fujita, S.; Cencini, M.; Buonincontri, G.; Takei, N.; Schulte, R.F.; Fukunaga, I.; Uchida, W.; Hagiwara, A.; Kamagata, K.; Hagiwara, Y.; et al. Simultaneous relaxometry and morphometry of human brain structures with 3D magnetic resonance fingerprinting: A multicenter, multiplatform, multifield-strength study. Cereb. Cortex 2023, 33, 729–739. [Google Scholar] [CrossRef]
- Keenan, K.E.; Ainslie, M.; Barker, A.J.; Boss, M.A.; Cecil, K.M.; Charles, C.; Chenevert, T.L.; Clarke, L.; Evelhoch, J.L.; Finn, P.; et al. Quantitative magnetic resonance imaging phantoms: A review and the need for a system phantom. Magn. Reson. Med. 2018, 79, 48–61. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ref. | Author | Year | Trends in MRF Pulse Sequences | Trends in MRF Pulse Sequence Optimization | Trends in MRF Dictionary Generation | Trends in Dictionary Matching | Trends in Model-Based MRF Reconstruction | Trends in Deep Learning-Based MRF Reconstruction | Application |
|---|---|---|---|---|---|---|---|---|---|
| [9] | Bipin Mehta | 2019 | ✓ | ✓ | ✓ | ✓ | |||
| [10] | Megan E Poorman | 2020 | ✓ | ✓ | ✓ | ||||
| [11] | Debra F. McGivney | 2020 | ✓ | ✓ | ✓ | ✓ | |||
| [12] | Jean J. L. Hsieh | 2020 | ✓ | ✓ | ✓ | ✓ | |||
| [17] | Charit Tippareddy | 2021 | ✓ | ✓ | ✓ | ||||
| Present Paper | Anmol Monga | 2023 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| REF | PARAMETRIC MAPS | CONTRIBUTION | APPLICATION |
|---|---|---|---|
| [75] | T1 and T2 | Introduced a 3D cardiac MRF technique with respiratory motion compensation, enabling T1/T2 myocardial mapping in a single free-breathing scan | Cardiac |
| [76] | T1 and T2 | Demonstrated the feasibility of generating multi-contrast synthetic Late Gadolinium Enhancement (LGE) images using MRF-derived post-contrast T1 and T2 maps | |
| [77] | T1, T2, M0, and FF | Applied an MRF approach to quantify water- and fat-specific T1 and T2, M0 estimation, and Fat Fraction (FF) maps for cardiac imaging in a single breath-hold exam | |
| [78] | T1, T2, and T1ρ | Proposed a 2D MRF method for cardiac imaging, offering simultaneous T1, T2, and T1ρ mapping using an ECG-triggered GRE sequence with inversion recovery pulses | |
| [79] | and T1 maps | Utilized an MRF technique to simultaneously estimate perfusion, diffusion, T2*, and T1 maps | Brain |
| [80] | Water T1 relaxation (T1w) map Water T2 relaxation (T2w) map Amide exchange rate (ksw) map Amide volume fraction (fs) map Semi-solid exchange rate (kssw) map Semi-solid volume fraction (fss) map | Applied CEST-MRF with EPI readout and DRONE deep learning reconstruction for accurate brain tumor quantification | |
| [81] | CBF, BAT, T1, and B1+ | Identified the crucial impact of TR patterns on MRF-ASL data, highlighting a sinusoidal pattern with a 125 TR period as the most consistently effective for spatial estimation | |
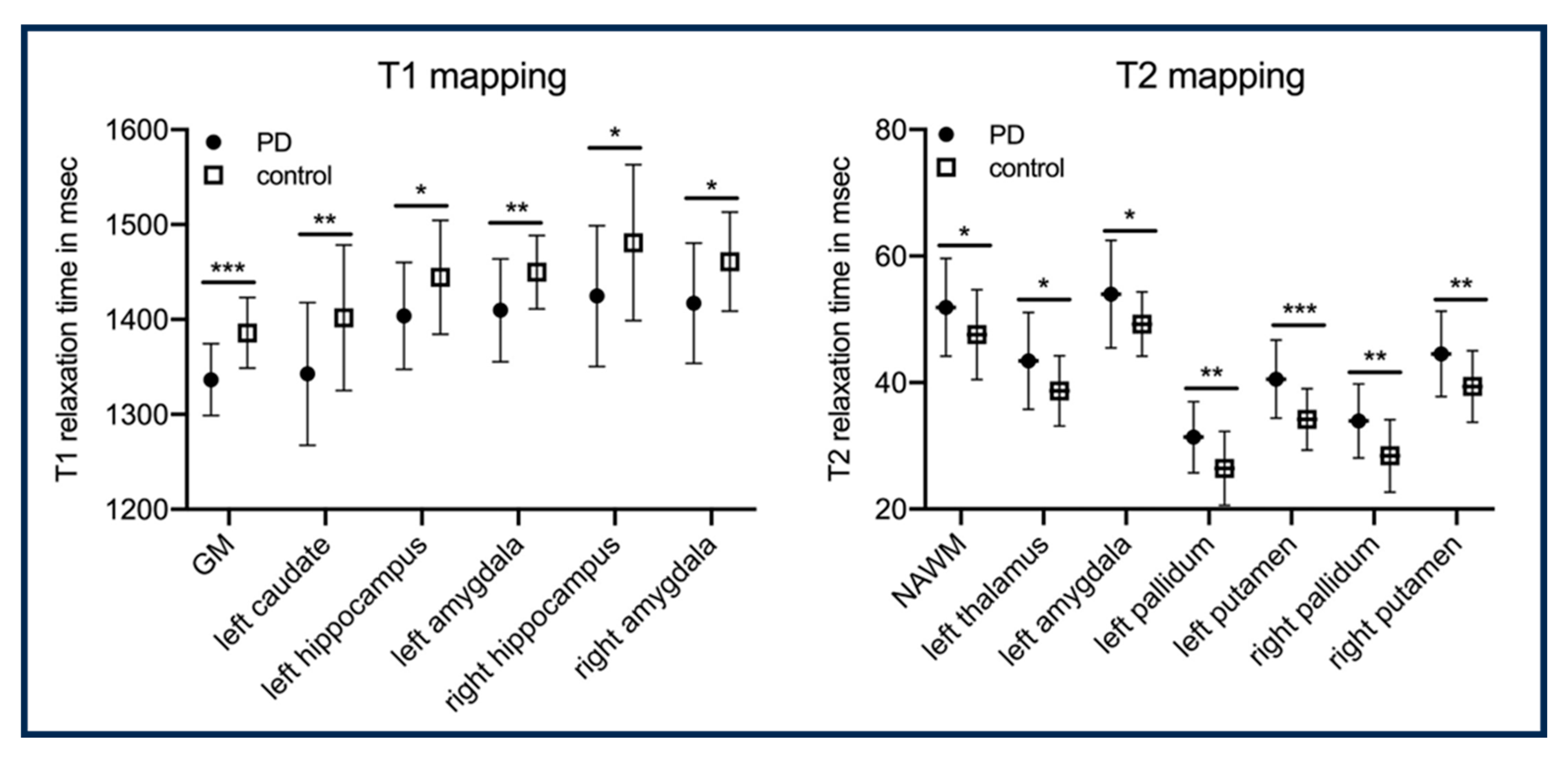
| [82] | T1 and T2 | Demonstrated the capability of MRF-derived T1 and T2 maps in accurately identifying Parkinson’s disease and assessing disease severity | |
| [83] | Perfusion, CBVa, BAT, MTR, and T1 | Optimized ASL labeling durations using the Cramer–Rao Lower Bound to enhance MRF-ASL signal sensitivity for brain hemodynamic quantification | |
| [84] | T1 and T2 | Presented a 3D spiral projection acquisition with various interleaving spirals to increase robustness to rigid motion, revealing a significant improvement in motion-corrected quantitative maps compared to the motionless reference | |
| [85] | T1, T2, PD, and sodium density | Introduced a simultaneous 2D imaging method for proton T1, T2, proton density, and sodium density, utilizing a golden-angle radial trajectory without adversely affecting image quality for both protons and sodium | |
| [86] | T1, T2, T1ρ, and B1+ | Developed a fast 3D-MRF technique for simultaneous T1, T2, and T1ρ mapping in knee cartilage, revealing elevated T1ρ in mild osteoarthritis with excellent repeatability | Musculoskeletal system |
| [87] | T1 and T2 | A UTE-based MRF sequence was implemented to quantify T1 and T2 for muscle, bone, ligaments, and tendons | |
| [88] | PD, T1, T2, and T1ρ | Implemented an MRF sequence demonstrating rapid, simultaneous estimation of accurate PD, T1, T2, and T1ρ maps of the lower leg muscle | |
| [89] | T1 and T2 | An MRF acquisition is proposed that measures T1 and T2, which minimizes biases introduced by fat | |
| [90] | FF, off-resonance, B1+, and T1 | Introduced an MRF approach, DBFW, utilizing RF spoiling to estimate T1 in water, T1 in fat, and FF maps, and it has four times faster acquisition than three-echo DIXON MRF | |
| [91] | T1, T2, and T1ρ | Demonstrated the feasibility of MRF for simultaneous bilateral mapping of T1, T2, and T1ρ in the hip joint | |
| [92] | PD, T1, and T2 | Presented an MRF technique that facilitates simultaneous measurement of PD, T1, and T2 maps for six radial hip sections | |
| [93] | T1 and T2 | Assessed the use of the 3D MRF technique for simultaneous T1 and T2 mapping in breast tissues | Breast tissues |
| [94] | T1 and T2 | Introduced three-point Dixon water–fat separation within the spiral MRF framework, enabling correction of fat-blurring using the CPR technique | |
| [95] | T1 and T2 | Introduced a 3D abdominal MRF technique using a gated pilot tone (PT) navigator for simultaneous quantification of T1 and T2 without breath holding | Abdominal |
| [96] | T1 and T2 | Demonstrated the feasibility of free-breathing pancreatic MRF at 1.5T and 3T, employing a spiral acquisition with oversampling of the center of k-space to mitigate in-plane motion artifacts | |
| [97] | T1 and | Two-dimensional MRF sequence based on echo planar imaging was proposed using variable flip angles, TEs, and TRs, along with non-selective inversion pulses | Kidneys |
| [98] | T1, T2, T1ρ, and FF | Applied a gradient-echo liver MRF technique to enable simultaneous and comprehensive mapping of T1, T2, T1ρ, and FF in a single breath-hold scan | Liver tissue |
| [99] | T1 and T2 | Verified the feasibility of T1 and T2 MRF for improving ovarian tumor detection, highlighting quantification capability without assessing its impact on detection compared to qualitative imaging | Ovaries |
| [100] | T1 and T2 | Employed MRF to rapidly quantify relaxation times in the human eye at 7 T, achieving significant scan time reduction while maintaining detailed parameter maps without visible loss | Human eye |
| k-Space Trajectory | Advantages | Disadvantages |
|---|---|---|
| Cartesian | Easy and fast to reconstruct, with compatibility across all scanners | Inefficient k-space coverage and longer scan time, increased sensitivity to motion and susceptibility artifacts, and rapid switching of gradient coil can cause gradient heating and noise |
| Radial | Well-controlled linear trajectories, constant gradients, and fast readouts | Less k-space coverage and susceptible to gradient moment artifacts |
| Spiral | Better k-space coverage, short TEs, and relatively fast readouts | Susceptible to Eddy currents, with less precise trajectories |
| Rosette | mapping | The implementation of Rosette trajectories is computationally complex, and limited compatibility and hardware constraints are observed in older MRI scanners |
| Echo Planar Imaging (EPI) | Better k-space coverage compared to Cartesian acquisition | Long readouts and TEs, usually used for lower-resolution acquisitions |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Monga, A.; Singh, D.; de Moura, H.L.; Zhang, X.; Zibetti, M.V.W.; Regatte, R.R. Emerging Trends in Magnetic Resonance Fingerprinting for Quantitative Biomedical Imaging Applications: A Review. Bioengineering 2024, 11, 236. https://doi.org/10.3390/bioengineering11030236
Monga A, Singh D, de Moura HL, Zhang X, Zibetti MVW, Regatte RR. Emerging Trends in Magnetic Resonance Fingerprinting for Quantitative Biomedical Imaging Applications: A Review. Bioengineering. 2024; 11(3):236. https://doi.org/10.3390/bioengineering11030236
Chicago/Turabian StyleMonga, Anmol, Dilbag Singh, Hector L. de Moura, Xiaoxia Zhang, Marcelo V. W. Zibetti, and Ravinder R. Regatte. 2024. "Emerging Trends in Magnetic Resonance Fingerprinting for Quantitative Biomedical Imaging Applications: A Review" Bioengineering 11, no. 3: 236. https://doi.org/10.3390/bioengineering11030236