
Mandibular Titanium Miniplates Change the Biomechanical Behaviour of the Mandible in the Case of Facial Trauma: A Three-Dimensional Finite Element Analysis
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
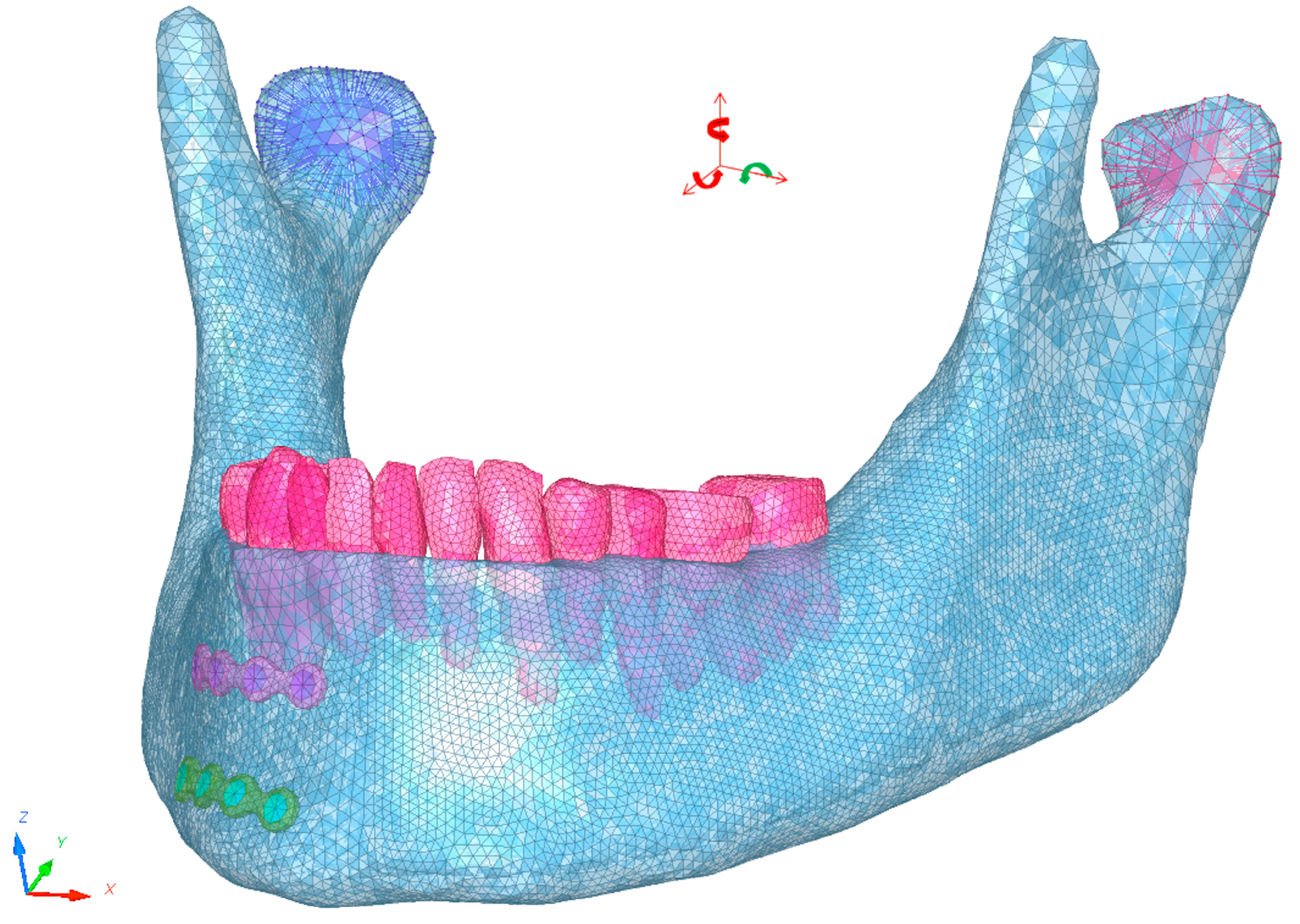
2.1. Model Description
2.2. Contact Conditions
2.3. Boundary Conditions
2.4. Material Data
2.5. Trauma Simulation
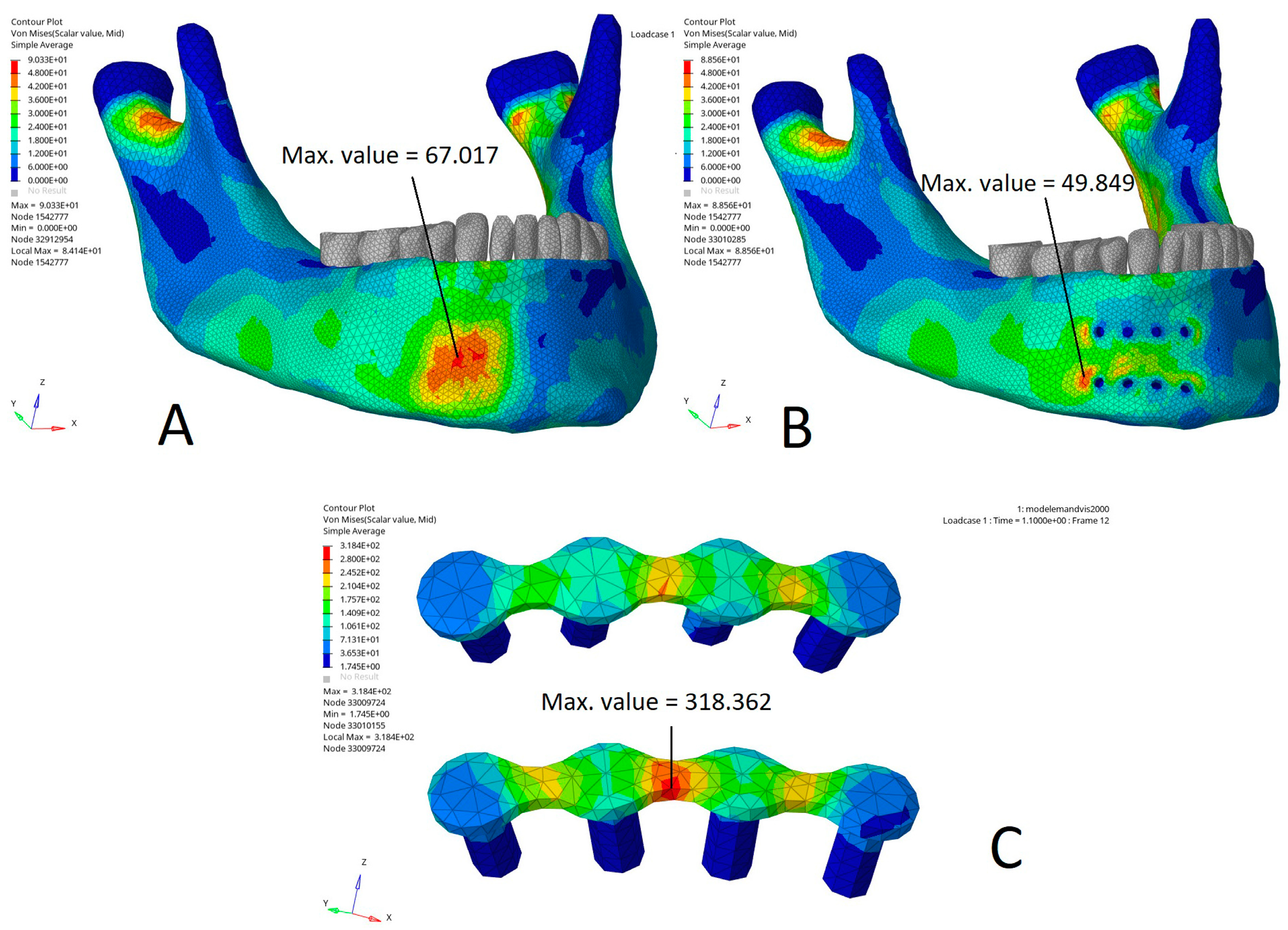
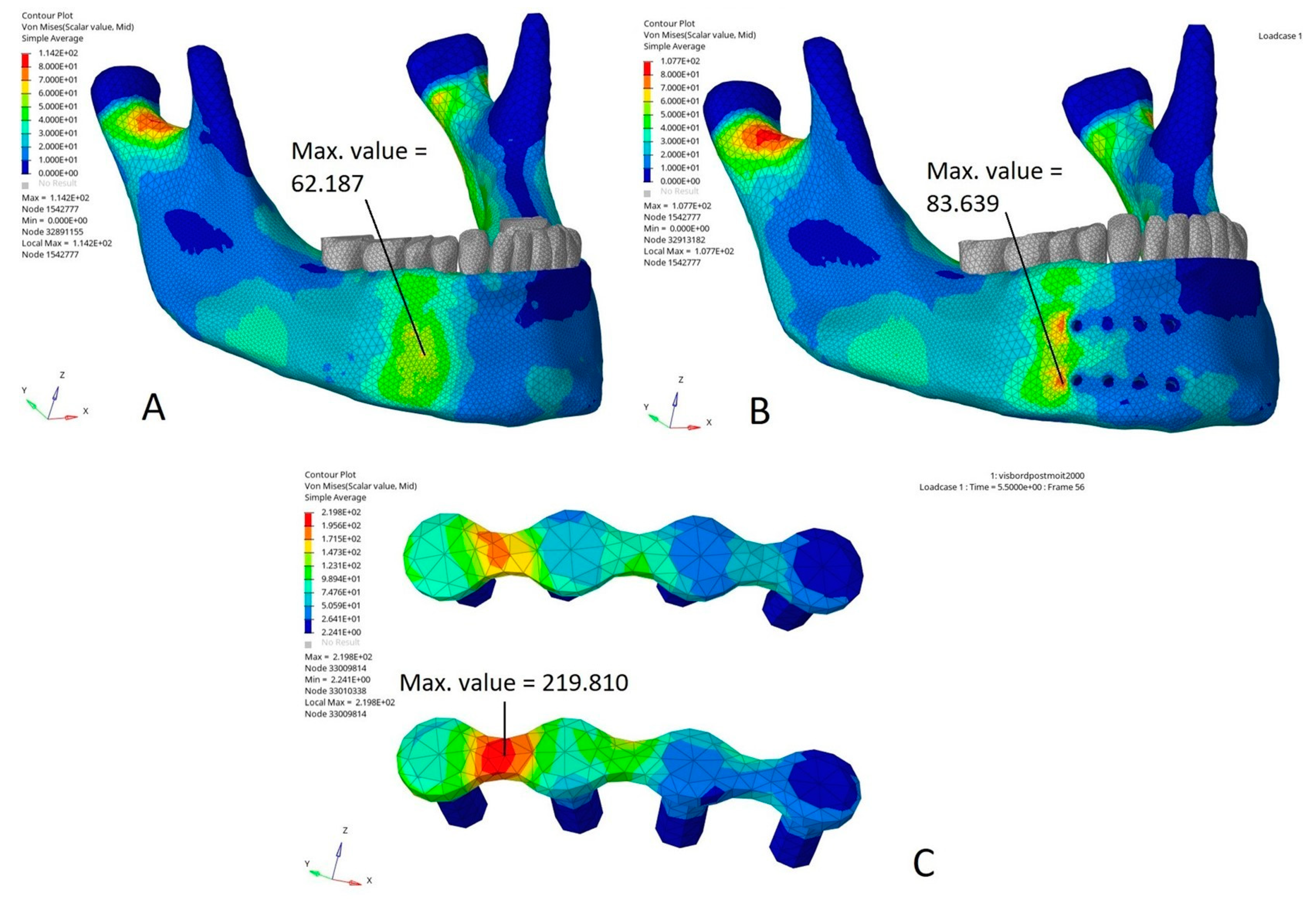
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Gareb, B.; Roossien, C.C.; van Bakelen, N.B.; Verkerke, G.J.; Vissink, A.; Bos, R.R.M.; van Minnen, B. Comparison of the Mechanical Properties of Biodegradable and Titanium Osteosynthesis Systems Used in Oral and Maxillofacial Surgery. Sci. Rep. 2020, 10, 18143. [Google Scholar] [CrossRef]
- Brown, J.S.; Trotter, M.; Cliffe, J.; Ward-Booth, R.P.; Williams, E.D. The Fate of Miniplates in Facial Trauma and Orthognathic Surgery: A Retrospective Study. Br. J. Oral Maxillofac. Surg. 1989, 27, 306–315. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, V.; Chhabra, P.; Dover, M.S. Removal of Miniplates in Maxillofacial Surgery: A Follow-up Study. J. Oral Maxillofac. Surg. 2005, 63, 756–760. [Google Scholar] [CrossRef] [PubMed]
- Mosbah, M.R.; Oloyede, D.; Koppel, D.A.; Moos, K.F.; Stenhouse, D. Miniplate Removal in Trauma and Orthognathic Surgery—A Retrospective Study. Int. J. Oral Maxillofac. Surg. 2003, 32, 148–151. [Google Scholar] [CrossRef]
- Park, H.-C.; Kim, S.-G.; Oh, J.-S.; You, J.-S.; Kim, W.-G. Mini-Plate Removal in Maxillofacial Trauma Patients during a Five-Year Retrospective Study. J. Korean Assoc. Oral Maxillofac. Surg. 2016, 42, 182–186. [Google Scholar] [CrossRef] [PubMed]
- Graillon, N.; Guyot, L.; Sigaux, N.; Louvrier, A.; Trost, O.; Lutz, J.-C.; Foletti, J.-M. Do Mandibular Miniplates Increase the Risk of Complex Fracture in Facial Trauma Recurrence? Case Series. J. Cranio-Maxillofac. Surg. 2020, 49, 613–619. [Google Scholar] [CrossRef]
- Elrasheed, A.; Toma, Q.; Cousin, G.C.S. Mandibular Fractures That Have Healed Are Not Weakened Permanently: Series of Nine Patients Who Sustained Mandibular Fractures at Different Sites on Two Separate Occasions. Br. J. Oral Maxillofac. Surg. 2011, 49, 209–212. [Google Scholar] [CrossRef]
- Agir, H.; Moore, M.H.; David, D.J.; McLean, N.R.; Cooter, R. Fracture Patterns and Bone Healing in Recurrent Mandibular Fractures: A Clinical Study of 13 Patients. Plast. Reconstr. Surg. 2005, 116, 427–436; discussion 437–439. [Google Scholar] [CrossRef]
- Olson, R.A.; Fonseca, R.J.; Zeitler, D.L.; Osbon, D.B. Fractures of the Mandible: A Review of 580 Cases. J. Oral Maxillofac. Surg. 1982, 40, 23–28. [Google Scholar] [CrossRef]
- Sadhu Reddipogu, J.; Lightfoot, E.; Scott, C.; Thomas, M. Recurrent Mandibular Fractures: A Retrospective Study over 17 Years on Aetiology, Demographics, Fracture Patterns, and Management. Int. J. Oral Maxillofac. Surg. 2021, 50, 1596–1602. [Google Scholar] [CrossRef]
- Foletti, J.M.; Bruneau, S.; Farisse, J.; Thiery, G.; Chossegros, C.; Guyot, L. Screening for psychiatric risk factors in a facial trauma patients. Validating a questionnaire. Rev. Stomatol. Chir. Maxillofac. Chir. Orale 2014, 115, 343–348. [Google Scholar] [CrossRef] [PubMed]
- McCoy, A.M.; Como, J.J.; Greene, G.; Laskey, S.L.; Claridge, J.A. A Novel Prospective Approach to Evaluate Trauma Recidivism: The Concept of the Past Trauma History. J. Trauma Acute Care Surg. 2013, 75, 116–121. [Google Scholar] [CrossRef] [PubMed]
- Abraham, P.J.; Abraham, M.N.; Griffin, R.L.; Tanner, L.; Jansen, J.O. Evaluation of Injury Recidivism Using the Electronic Medical Record. J. Surg. Res. 2021, 267, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Hwang, K. Field Management of Facial Injuries in Sports. J. Craniofac. Surg. 2020, 31, e179. [Google Scholar] [CrossRef]
- Beret, M.; Nicot, R.; Roland-Billecart, T.; Ramdane, N.; Ferri, J.; Schlund, M. Impacted Lower Third Molar Relationship with Mandibular Angle Fracture Complications. J. Stomatol. Oral Maxillofac. Surg. 2021, 123, 149–154. [Google Scholar] [CrossRef] [PubMed]
- Ogilvie, M.P.; Pereira, B.M.T.; Ryan, M.L.; Panthaki, Z.J. Emergency Department Assessment and Management of Facial Trauma from War-Related Injuries. J. Craniofac. Surg. 2010, 21, 1002–1008. [Google Scholar] [CrossRef]
- Graillon, N.; Guyot, L.; Thollon, L.; Godio-Raboutet, Y.; Roux, M.-K.L.; Foletti, J.-M. Do Mandibular Titanium Miniplates Affect the Biomechanical Behaviour of the Mandible? A Preliminary Experimental Study. J. Stomatol. Oral Maxillofac. Surg. 2022, 123, e675–e681. [Google Scholar] [CrossRef]
- Foletti, J.M.; Martinez, V.; Haen, P.; Godio-Raboutet, Y.; Guyot, L.; Thollon, L. Finite Element Analysis of the Human Orbit. Behavior of Titanium Mesh for Orbital Floor Reconstruction in Case of Trauma Recurrence. J. Stomatol. Oral Maxillofac. Surg. 2019, 120, 91–94. [Google Scholar] [CrossRef]
- Zhong, S.; Shi, Q.; Sun, Y.; Yang, S.; Van Dessel, J.; Gu, Y.; Chen, X.; Lübbers, H.-T.; Politis, C. Biomechanical Comparison of Locking and Non-Locking Patient-Specific Mandibular Reconstruction Plate Using Finite Element Analysis. J. Mech. Behav. Biomed. Mater. 2021, 124, 104849. [Google Scholar] [CrossRef]
- Tuchtan, L.; Piercecchi-Marti, M.-D.; Bartoli, C.; Boisclair, D.; Adalian, P.; Léonetti, G.; Behr, M.; Thollon, L. Forces Transmission to the Skull in Case of Mandibular Impact. Forensic Sci. Int. 2015, 252, 22–28. [Google Scholar] [CrossRef]
- Schneider, D.C.; Nahum, A.M. Impact Studies of Facial Bones and Skull; SAE International: Warrendale, PA, USA, 1972; p. 720965. [Google Scholar]
- Viano, D.C.; Casson, I.R.; Pellman, E.J.; Bir, C.A.; Zhang, L.; Sherman, D.C.; Boitano, M.A. Concussion in Professional Football: Comparison with Boxing Head Impacts—Part 10. Neurosurgery 2005, 57, 1154–1172; discussion 1154–1172. [Google Scholar] [CrossRef] [PubMed]
- Duggal, I.; Sidhu, M.S.; Chawla, A.; Dabas, A.; Dhimole, V.K. Effects of Miniplate Anchored Herbst Appliance on Skeletal, Dental and Masticatory Structures of the Craniomandibular Apparatus: A Finite Element Study. Int. Orthod. 2021, 19, 301–309. [Google Scholar] [CrossRef] [PubMed]
- de Mello Santos, L.S.; Rossi, A.C.; Freire, A.R.; Matoso, R.I.; Caria, P.H.F.; Prado, F.B. Finite-Element Analysis of 3 Situations of Trauma in the Human Edentulous Mandible. J. Oral Maxillofac. Surg. 2015, 73, 683–691. [Google Scholar] [CrossRef]
- Ayali, A.; Bilginaylar, K. Evaluating the Biomechanical Effects of Implant Diameter in Case of Facial Trauma to an Edentulous Atrophic Mandible: A 3D Finite Element Analysis. Head Face Med. 2017, 13, 5. [Google Scholar] [CrossRef] [PubMed]
- Antic, S.; Saveljic, I.; Nikolic, D.; Jovicic, G.; Filipovic, N.; Rakocevic, Z.; Djuric, M. Does the Presence of an Unerupted Lower Third Molar Influence the Risk of Mandibular Angle and Condylar Fractures? Int. J. Oral Maxillofac. Surg. 2016, 45, 588–592. [Google Scholar] [CrossRef]
- Bezerra, T.P.; Silva Junior, F.I.; Scarparo, H.C.; Costa, F.W.G.; Studart-Soares, E.C. Do Erupted Third Molars Weaken the Mandibular Angle after Trauma to the Chin Region? A 3D Finite Element Study. Int. J. Oral Maxillofac. Surg. 2013, 42, 474–480. [Google Scholar] [CrossRef]
- Arora, L.; Bhardwaj, S.; Hashmi, G.S.; Anwar, S.F.; Rahman, S.A. Finite Element Analysis (FEA) of Perpendicular Plating versus Conventional Plating in Mandibular Symphysis Fracture. J. Maxillofac. Oral Surg. 2020, 19, 143–148. [Google Scholar] [CrossRef]
- Carlos, H.-V.; Marta, B.L.; Orlando, P.M.; Samuel, U.E.; Sader, R.; Seifert, L.B. Stress Distribution Is Susceptible to the Angle of the Osteotomy in the High Oblique Sagittal Osteotomy (HOSO): Biomechanical Evaluation Using Finite Element Analyses. Comput. Methods Biomech. Biomed. Eng. 2021, 24, 67–75. [Google Scholar] [CrossRef]
- Koper, D.C.; Leung, C.A.W.; Smeets, L.C.P.; Laeven, P.F.J.; Tuijthof, G.J.M.; Kessler, P.A.W.H. Topology Optimization of a Mandibular Reconstruction Plate and Biomechanical Validation. J. Mech. Behav. Biomed. Mater. 2021, 113, 104157. [Google Scholar] [CrossRef]
- Liokatis, P.; Tzortzinis, G.; Gerasimidis, S.; Smolka, W. Finite Element Analysis of Different Titanium Miniplates: Evaluation of Three-Dimensional Designs Applied on Condylar Neck Fractures. J. Stomatol. Oral Maxillofac. Surg. 2021, 123, 184–190. [Google Scholar] [CrossRef]
- Pavlychuk, T.; Chernogorskyi, D.; Chepurnyi, Y.; Neff, A.; Kopchak, A. Biomechanical Evaluation of Type p Condylar Head Osteosynthesis Using Conventional Small-Fragment Screws Reinforced by a Patient Specific Two-Component Plate. Head Face Med. 2020, 16, 25. [Google Scholar] [CrossRef] [PubMed]
- Ramos, A.; Semedo, T.; Mesnard, M. Study of Fixation of a Mandibular Plate for Favourable Fractures of the Mandibular Angle: Numerical Predictions. Br. J. Oral Maxillofac. Surg. 2020, 58, 652–658. [Google Scholar] [CrossRef] [PubMed]
- Savoldelli, C.; Ehrmann, E.; Tillier, Y. Biomechanical Assessment of Different Fixation Methods in Mandibular High Sagittal Oblique Osteotomy Using a Three-Dimensional Finite Element Analysis Model. Sci. Rep. 2021, 11, 8755. [Google Scholar] [CrossRef] [PubMed]
- Kılınç, Y.; Zor, Z.F.; Tümer, M.K.; Erkmen, E.; Kurt, A. Does the Angulation of the Mandibular Third Molar Influence the Fragility of the Mandibular Angle after Trauma to the Mandibular Body? A Three-Dimensional Finite-Element Study. Comput. Methods Biomech. Biomed. Eng. 2018, 21, 488–497. [Google Scholar] [CrossRef]
- Liu, Y.-F.; Wang, R.; Baur, D.A.; Jiang, X.-F. A Finite Element Analysis of the Stress Distribution to the Mandible from Impact Forces with Various Orientations of Third Molars. J. Zhejiang Univ. Sci. B 2018, 19, 38–48. [Google Scholar] [CrossRef]
- Takada, H.; Abe, S.; Tamatsu, Y.; Mitarashi, S.; Saka, H.; Ide, Y. Three-Dimensional Bone Microstructures of the Mandibular Angle Using Micro-CT and Finite Element Analysis: Relationship between Partially Impacted Mandibular Third Molars and Angle Fractures. Dent. Traumatol. 2006, 22, 18–24. [Google Scholar] [CrossRef]
- Champy, M.; Loddé, J.P.; Schmitt, R.; Jaeger, J.H.; Muster, D. Mandibular Osteosynthesis by Miniature Screwed Plates via a Buccal Approach. J. Maxillofac. Surg. 1978, 6, 14–21. [Google Scholar] [CrossRef]
- Nygaard, R.M.; Marek, A.P.; Daly, S.R.; Van Camp, J.M. Violent Trauma Recidivism: Does All Violence Escalate? Eur. J. Trauma Emerg. Surg. 2018, 44, 851–858. [Google Scholar] [CrossRef]
- Bahney, C.S.; Zondervan, R.L.; Allison, P.; Theologis, A.; Ashley, J.W.; Ahn, J.; Miclau, T.; Marcucio, R.S.; Hankenson, K.D. Cellular Biology of Fracture Healing. J. Orthop. Res. 2019, 37, 35–50. [Google Scholar] [CrossRef] [PubMed]
- Marsell, R.; Einhorn, T.A. The Biology of Fracture Healing. Injury 2011, 42, 551–555. [Google Scholar] [CrossRef]
- Wieja, F.; Jacobs, G.; Stein, S.; Kopp, A.; van Gaalen, K.; Kröger, N.; Zinser, M. Development and Validation of a Parametric Human Mandible Model to Determine Internal Stresses for the Future Design Optimization of Maxillofacial Implants. J. Mech. Behav. Biomed. Mater. 2021, 125, 104893. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.-M.; Chan, M.-Y.; Hsu, J.-T.; Su, K.-C. Biomechanical Analysis of Subcondylar Fracture Fixation Using Miniplates at Different Positions and of Different Lengths. BMC Oral Health 2021, 21, 543. [Google Scholar] [CrossRef] [PubMed]
- Kargarnejad, S.; Ghalichi, F.; Pourgol-Mohammad, M.; Garajei, A. Mandibular Reconstruction System Reliability Analysis Using Probabilistic Finite Element Method. Comput. Methods Biomech. Biomed. Eng. 2021, 24, 1437–1449. [Google Scholar] [CrossRef] [PubMed]
- WĄdoŁowski, P.; KrzesiŃski, G.; Gutowski, P. Finite Element Analysis of Mini-Plate Stabilization of Human Mandible Angle Fracture—A Comparative Study. Acta Bioeng. Biomech. 2020, 22, 105–116. [Google Scholar] [CrossRef]
- Peng, L.; Bai, J.; Zeng, X.; Zhou, Y. Comparison of Isotropic and Orthotropic Material Property Assignments on Femoral Finite Element Models under Two Loading Conditions. Med. Eng. Phys. 2006, 28, 227–233. [Google Scholar] [CrossRef]
- Parr, N.M.; Passalacqua, N.V.; Skorpinski, K. Investigations Into Age-Related Changes in the Human Mandible. J. Forensic Sci. 2017, 62, 1586–1591. [Google Scholar] [CrossRef]
- Lyu, H.; Dong, Y.; Zhou, W.; Wang, C.; Jiang, H.; Wang, P.; Sun, Y. Incidence and Clinical Characteristics of Fall-Related Injuries among Older Inpatients at a Tertiary Grade a Hospital in Shandong Province from 2018 to 2020. BMC Geriatr. 2022, 22, 632. [Google Scholar] [CrossRef]
- Cleveland, C.N.; Kelly, A.; DeGiovanni, J.; Ong, A.A.; Carr, M.M. Maxillofacial Trauma in Children: Association between Age and Mandibular Fracture Site. Am. J. Otolaryngol. 2021, 42, 102874. [Google Scholar] [CrossRef]
- Giordano, V.; Franco, J.S.; Koch, H.A.; Labronici, P.J.; Pires, R.E.S.; Amaral, N.P.D. Age-Related Changes in Bone Architecture. Rev. Col. Bras. Cir. 2016, 43, 276–285. [Google Scholar] [CrossRef]
- Schnitzler, C.M.; Mesquita, J.M. Cortical Porosity in Children Is Determined by Age-Dependent Osteonal Morphology. Bone 2013, 55, 476–486. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Young’s Modulus (MPa) | Poisson ‘s Ratio | Initial Density (g/cm3) | |
|---|---|---|---|
| Compact bone | 13,000 | 0.3 | 1.85 |
| Cancellous bone | 56 | 0.3 | 1.5 |
| Teeth | 18,600 | 0.31 | 1.8 |
| Titanium | 114,000 | 0.34 | 4.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Graillon, N.; Foletti, J.-M.; Godio-Raboutet, Y.; Guyot, L.; Varazzani, A.; Thollon, L. Mandibular Titanium Miniplates Change the Biomechanical Behaviour of the Mandible in the Case of Facial Trauma: A Three-Dimensional Finite Element Analysis. Bioengineering 2023, 10, 994. https://doi.org/10.3390/bioengineering10090994
Graillon N, Foletti J-M, Godio-Raboutet Y, Guyot L, Varazzani A, Thollon L. Mandibular Titanium Miniplates Change the Biomechanical Behaviour of the Mandible in the Case of Facial Trauma: A Three-Dimensional Finite Element Analysis. Bioengineering. 2023; 10(9):994. https://doi.org/10.3390/bioengineering10090994
Chicago/Turabian StyleGraillon, Nicolas, Jean-Marc Foletti, Yves Godio-Raboutet, Laurent Guyot, Andrea Varazzani, and Lionel Thollon. 2023. "Mandibular Titanium Miniplates Change the Biomechanical Behaviour of the Mandible in the Case of Facial Trauma: A Three-Dimensional Finite Element Analysis" Bioengineering 10, no. 9: 994. https://doi.org/10.3390/bioengineering10090994