
Research on the Internal Flow Field of Left Atrial Appendage and Stroke Risk Assessment with Different Blood Models
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
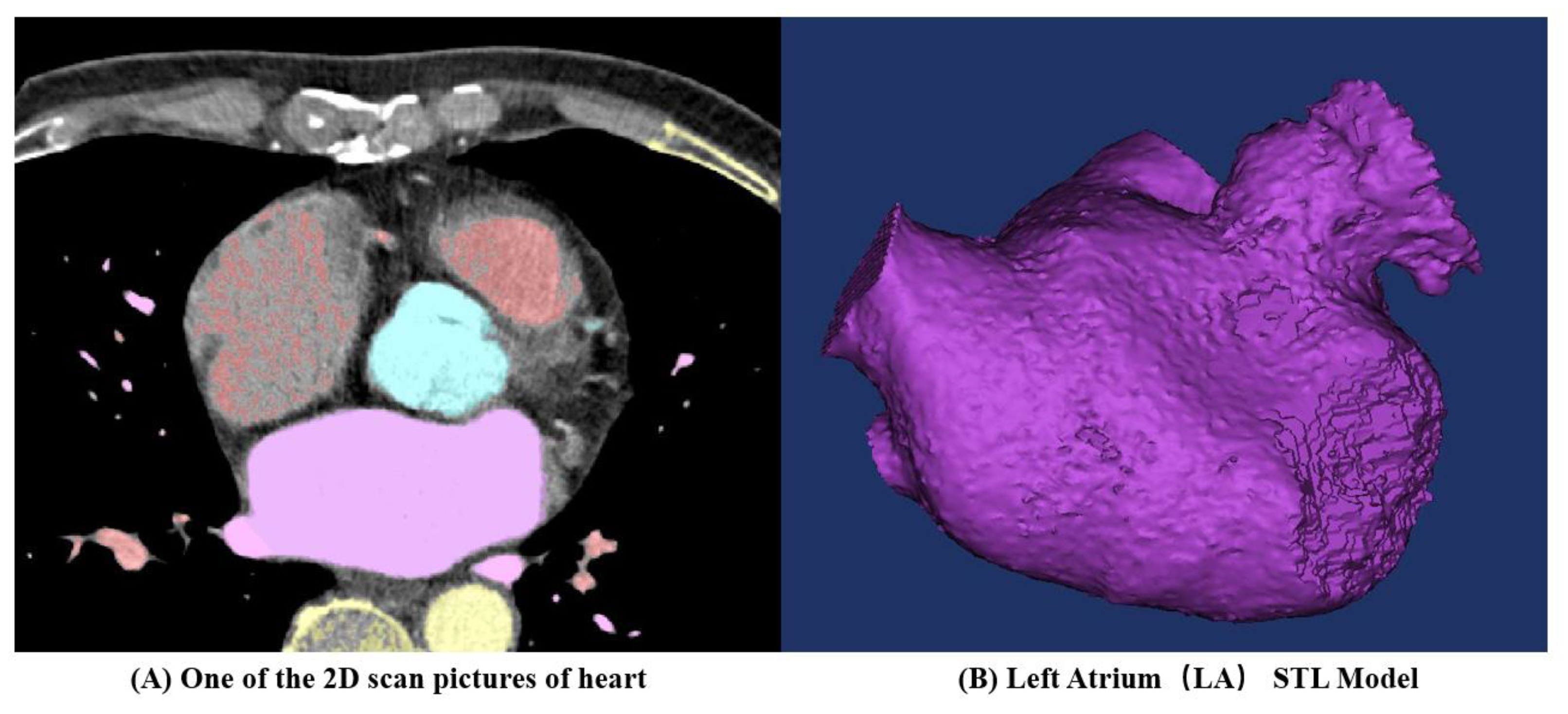
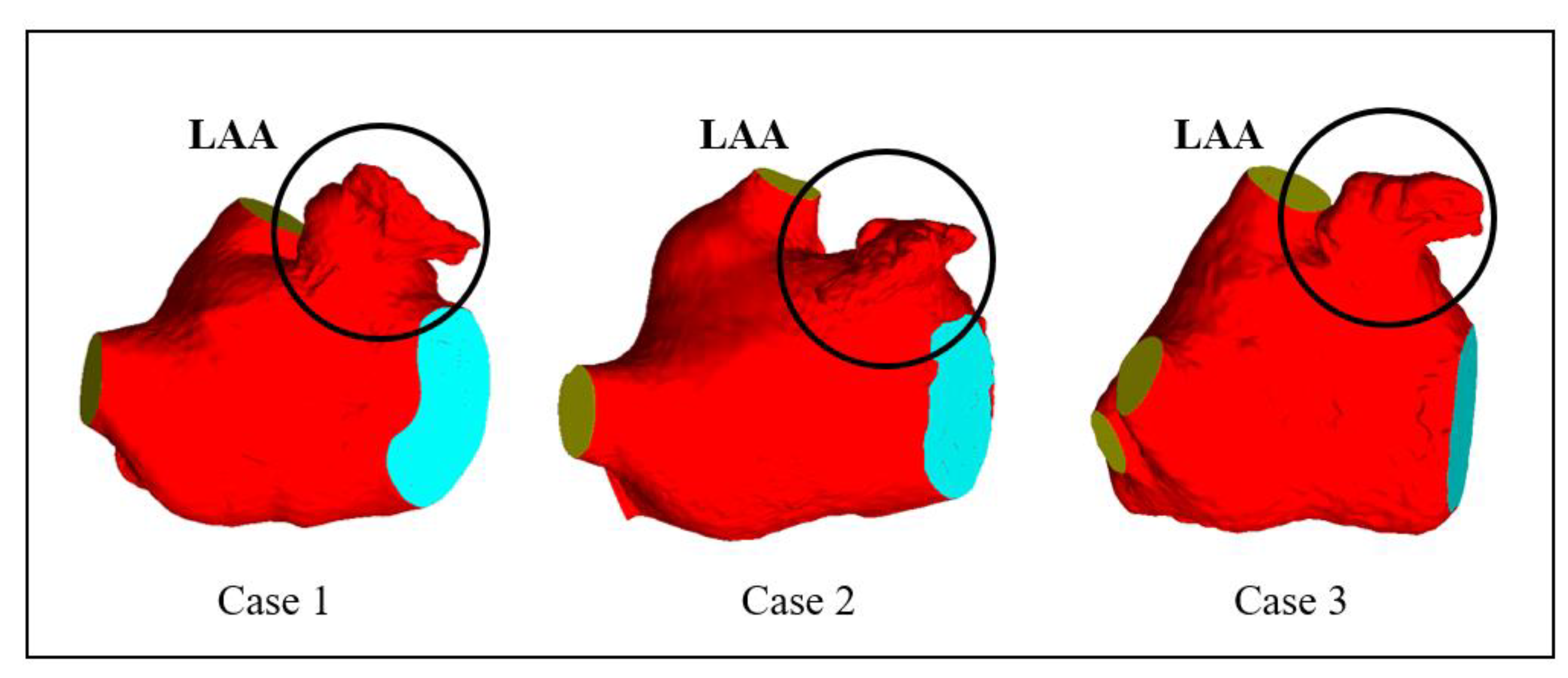
2.1. Geometric Models
2.2. Thrombosis Prediction Model
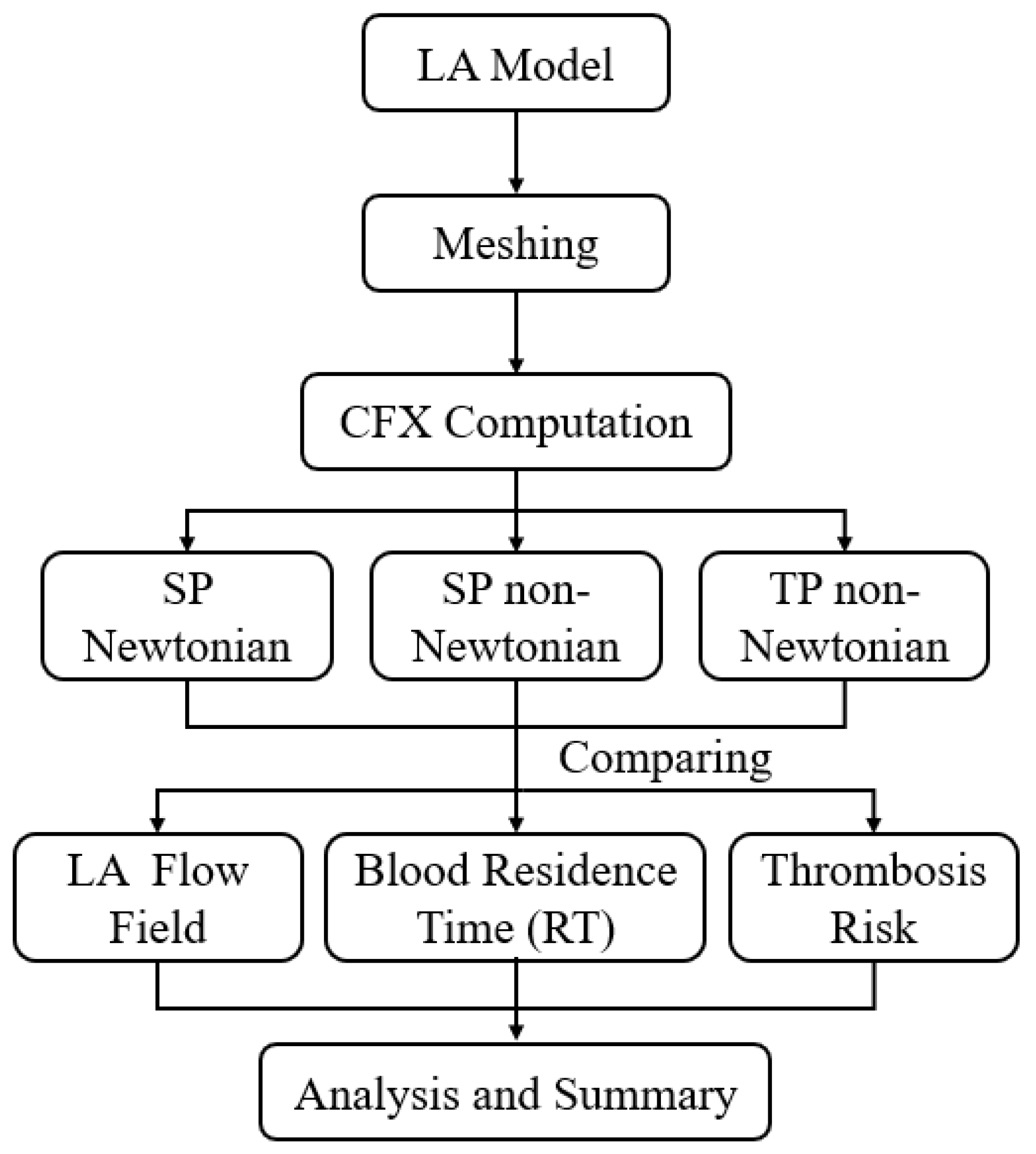
2.3. Solving Process
2.3.1. Single-Phase Newtonian Blood Flow Model
2.3.2. Single-Phase Non-Newtonian Blood Flow Model
2.3.3. Two-Phase Non-Newtonian Blood Model
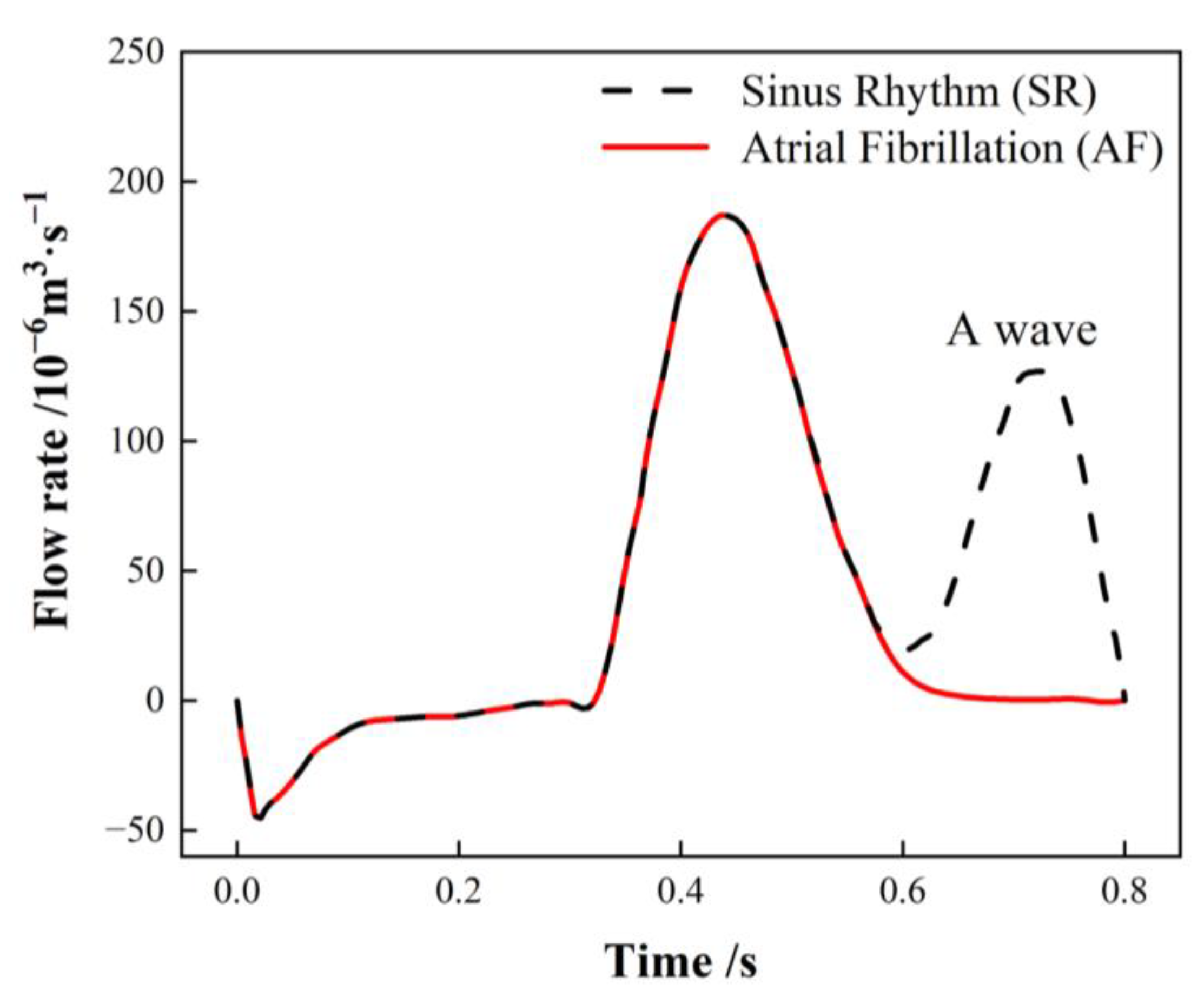
2.3.4. Boundary Condition
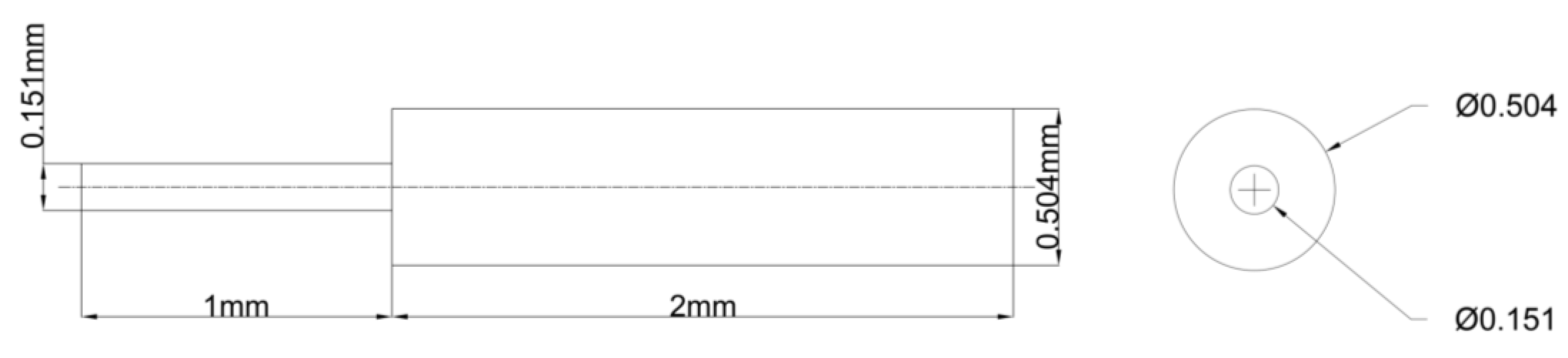
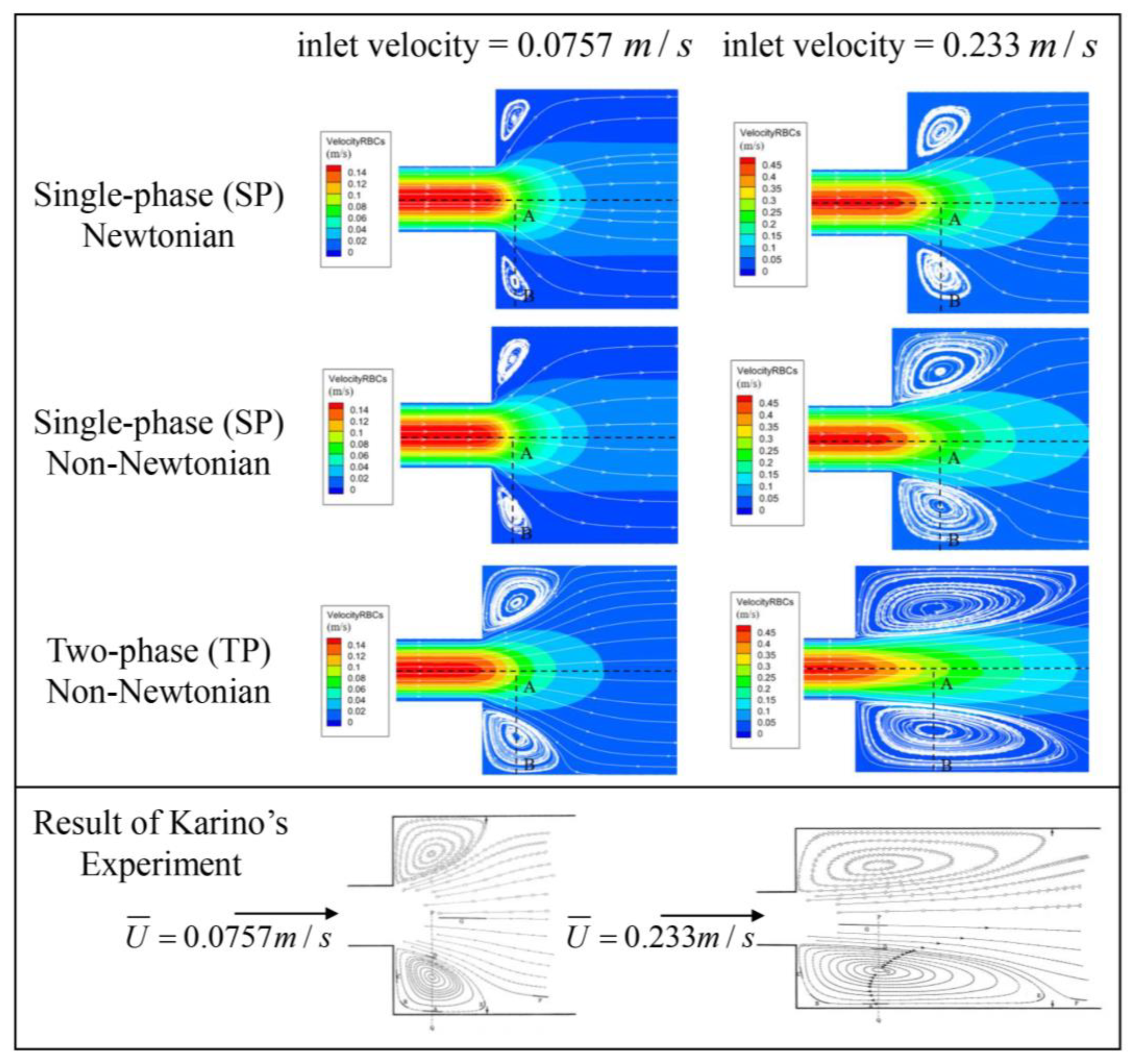
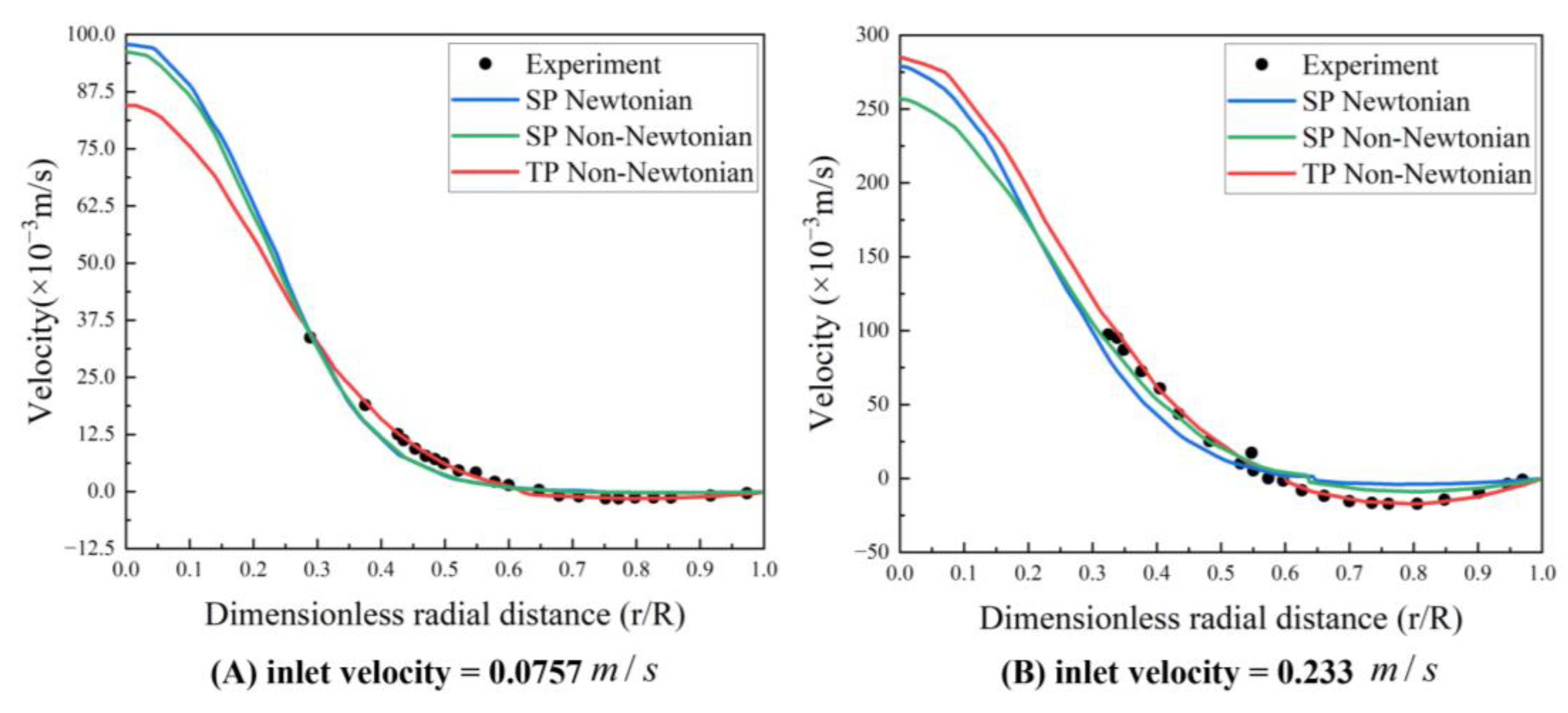
2.4. Blood Flow Model Verification
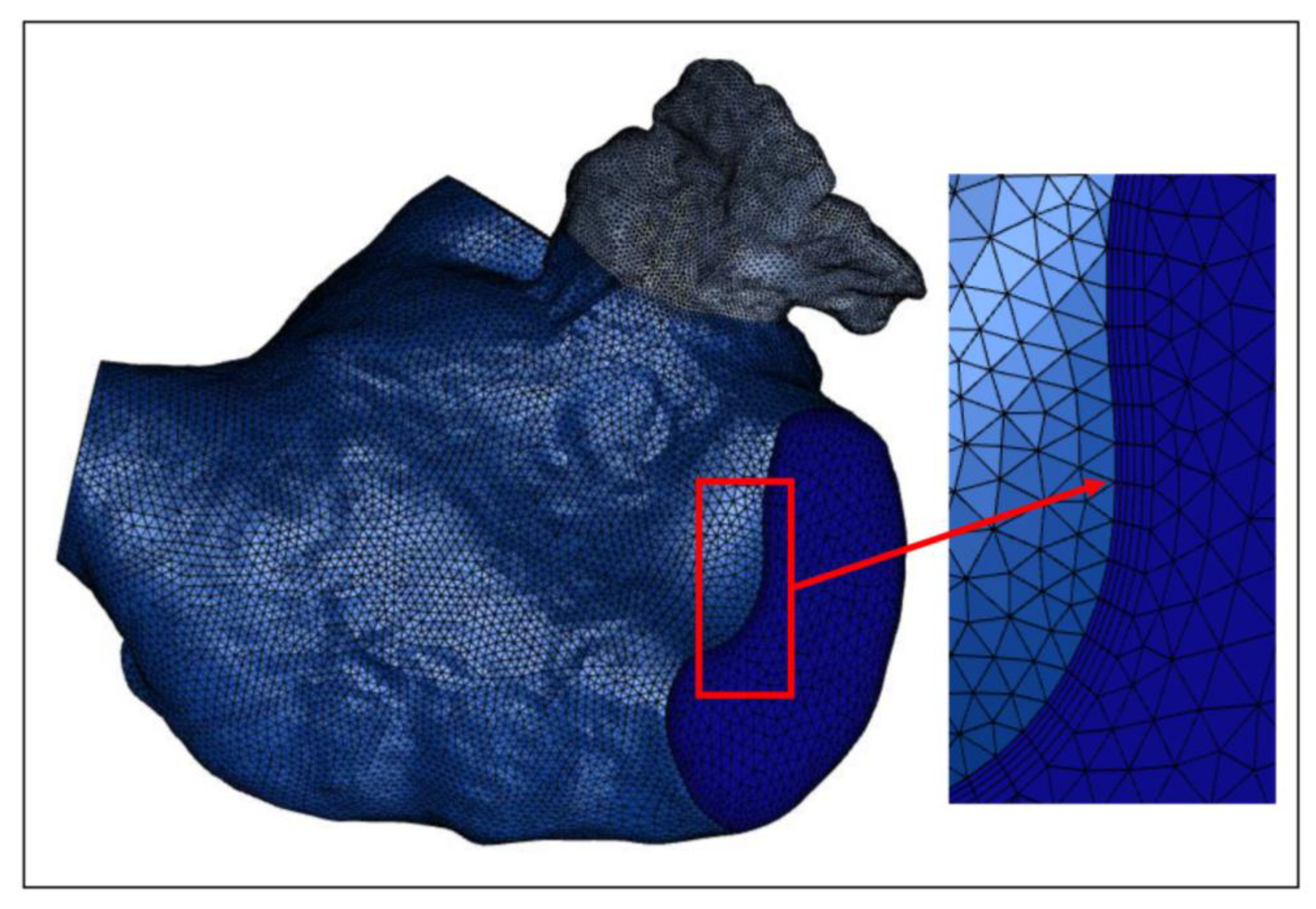
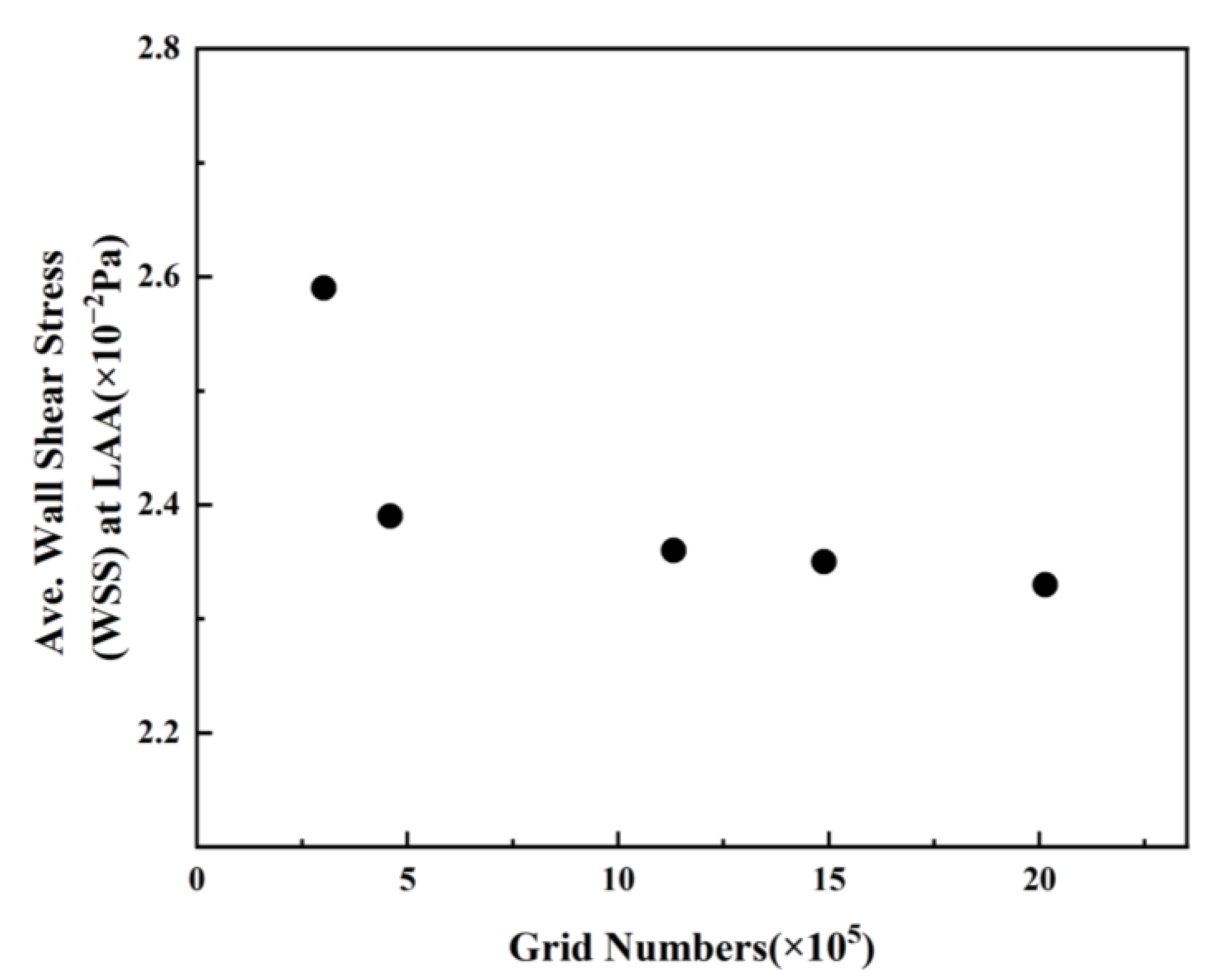
2.5. Meshing and Grid-Independence Verification
3. Result
3.1. Analysis of Influence of Blood Flow Models on Flow Field
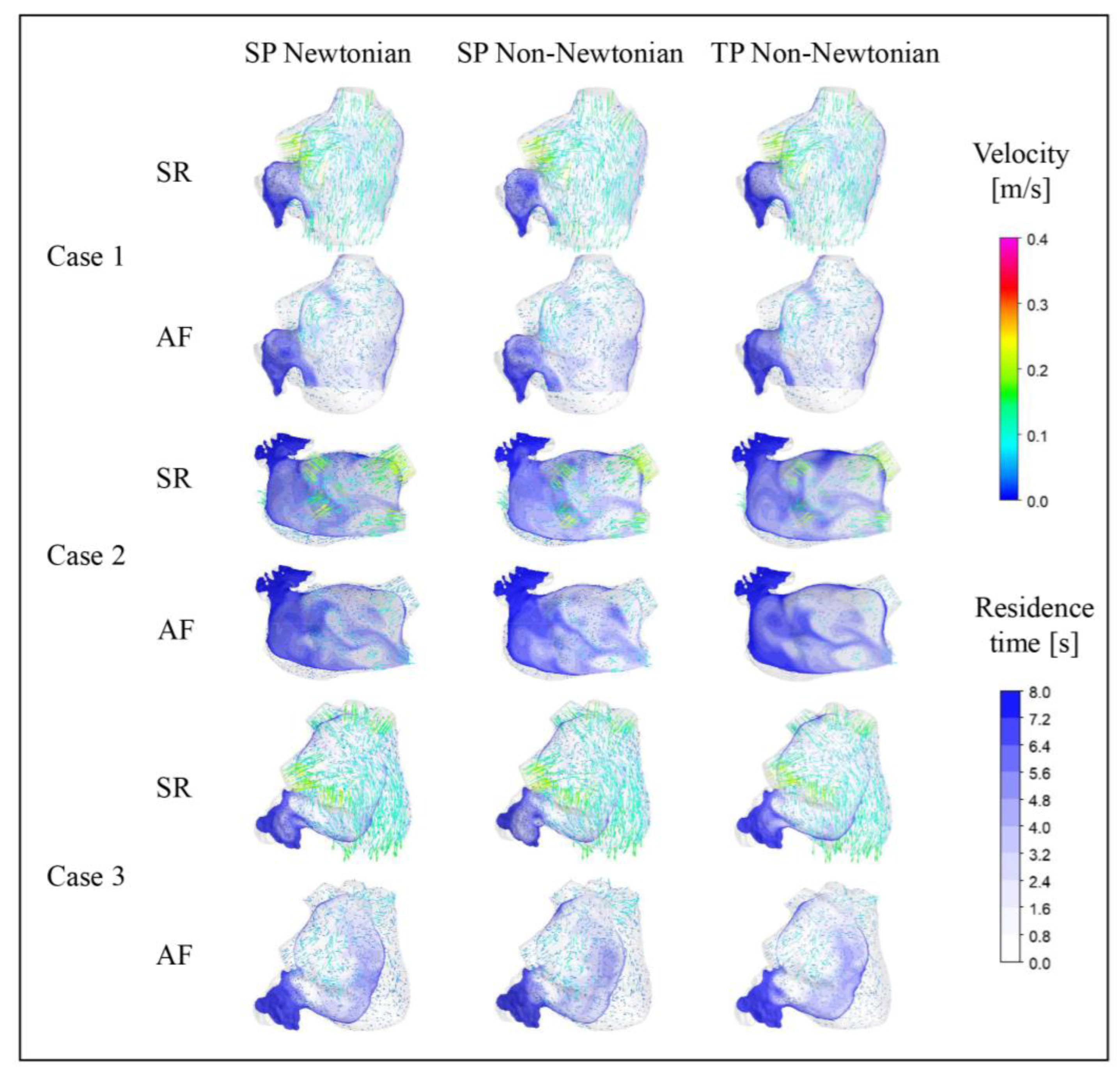
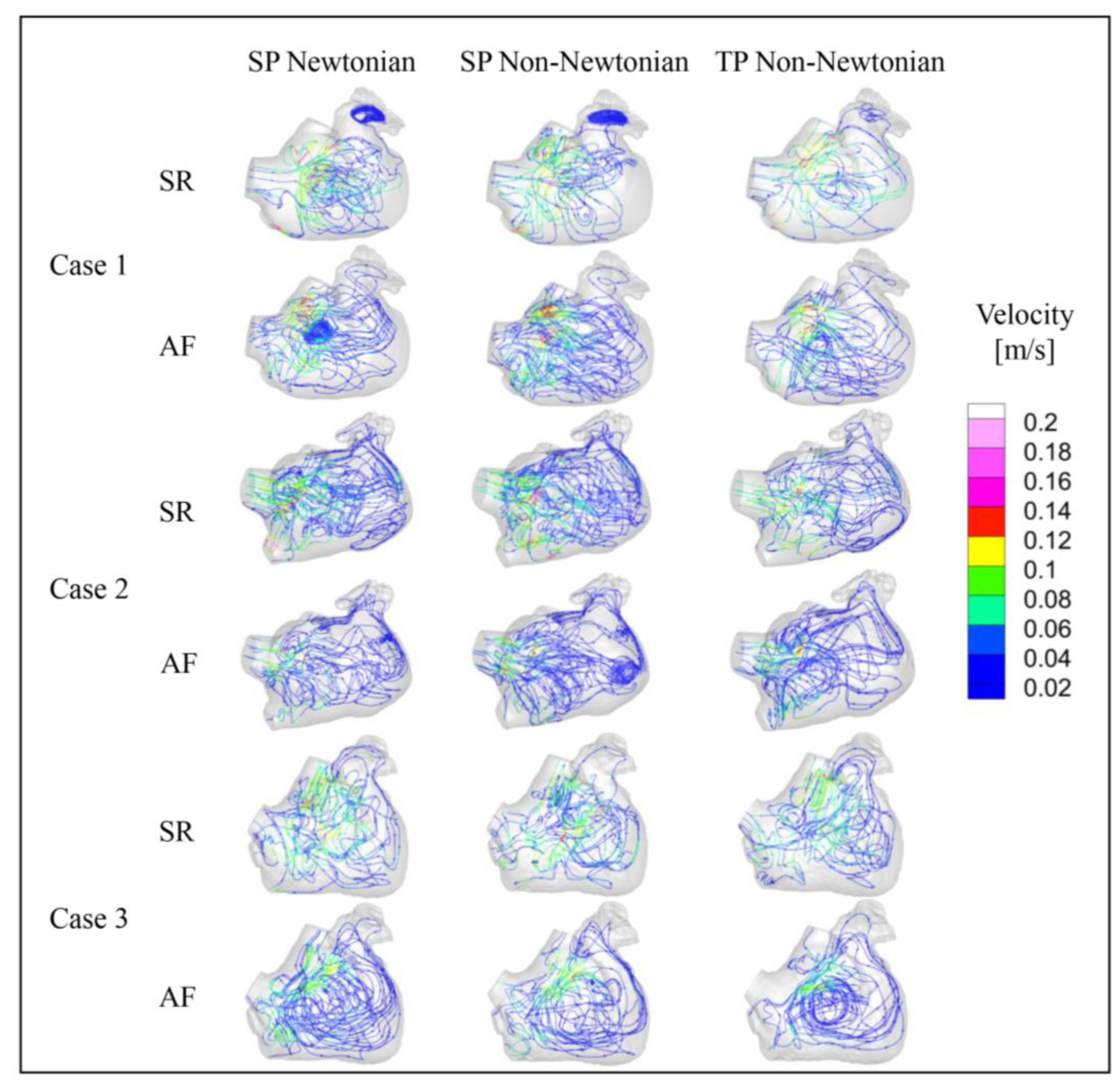
3.1.1. Effect of Blood Flow Models on Flow Field and Residence Time in Left Atrium
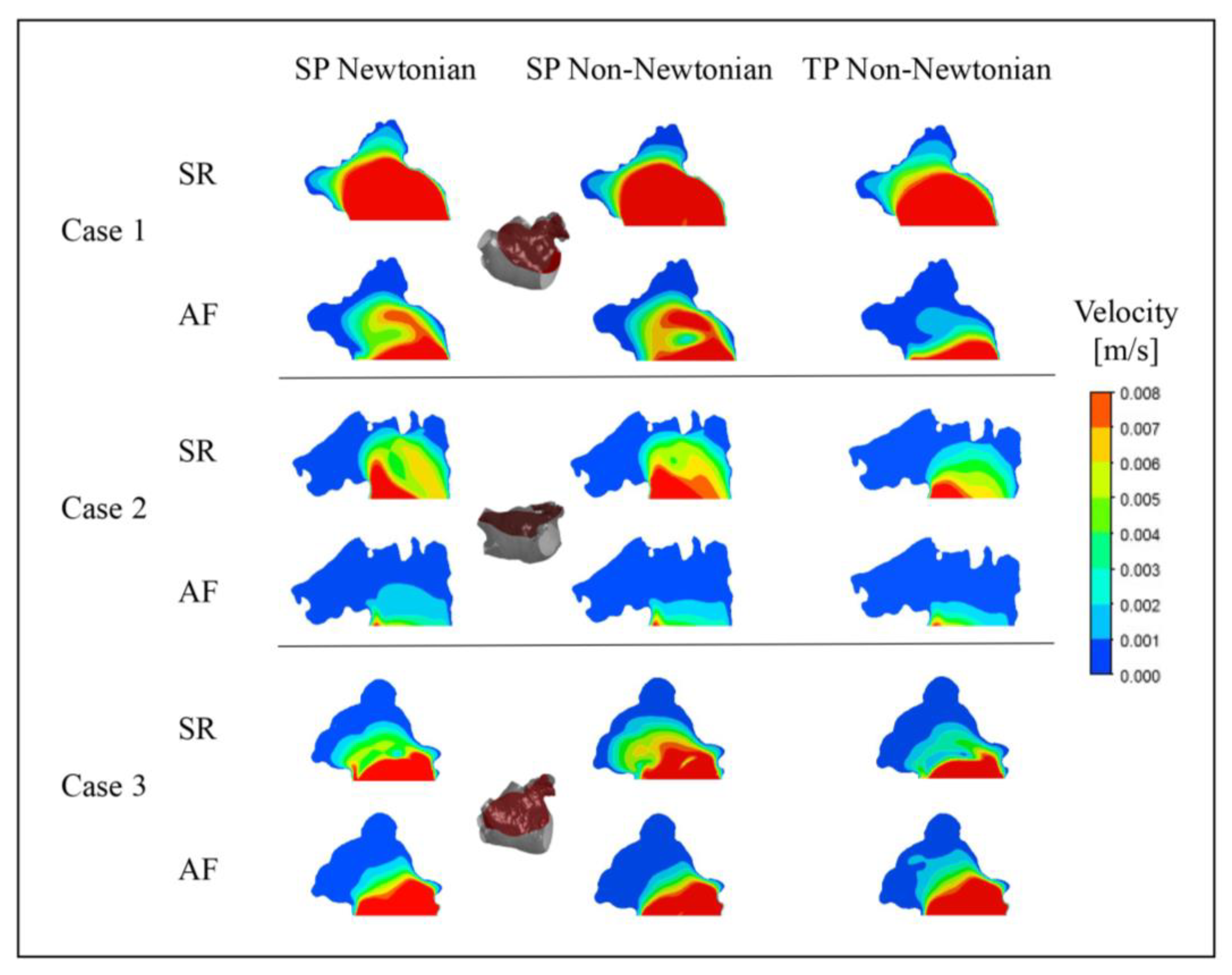
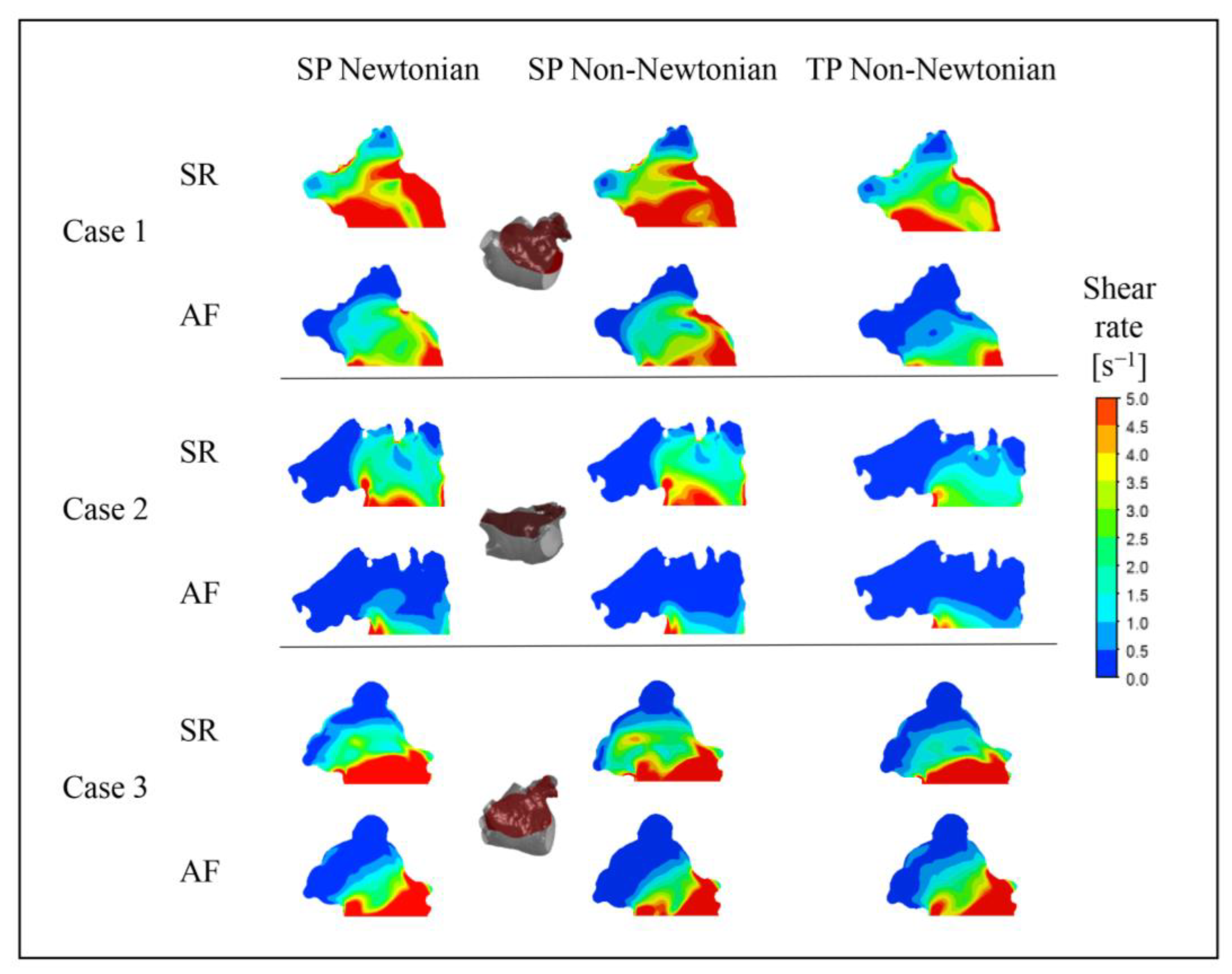
3.1.2. Effect of Blood Flow Models on Flow Field in Left Atrial Appendage
3.2. The Influence of Blood Flow Models on the Prediction of Thrombosis
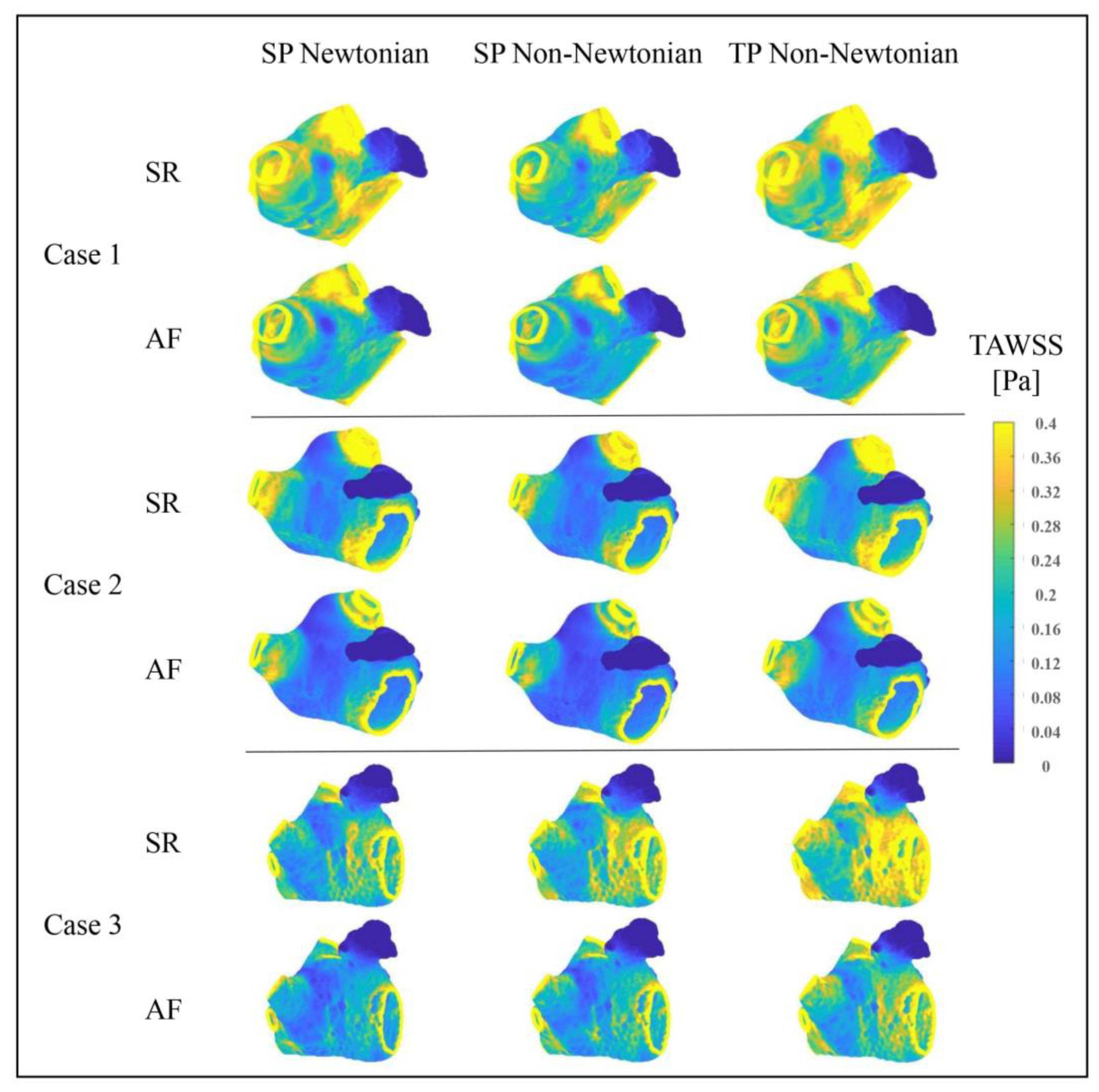
3.2.1. Effect of Blood Flow Models on TAWSS Value
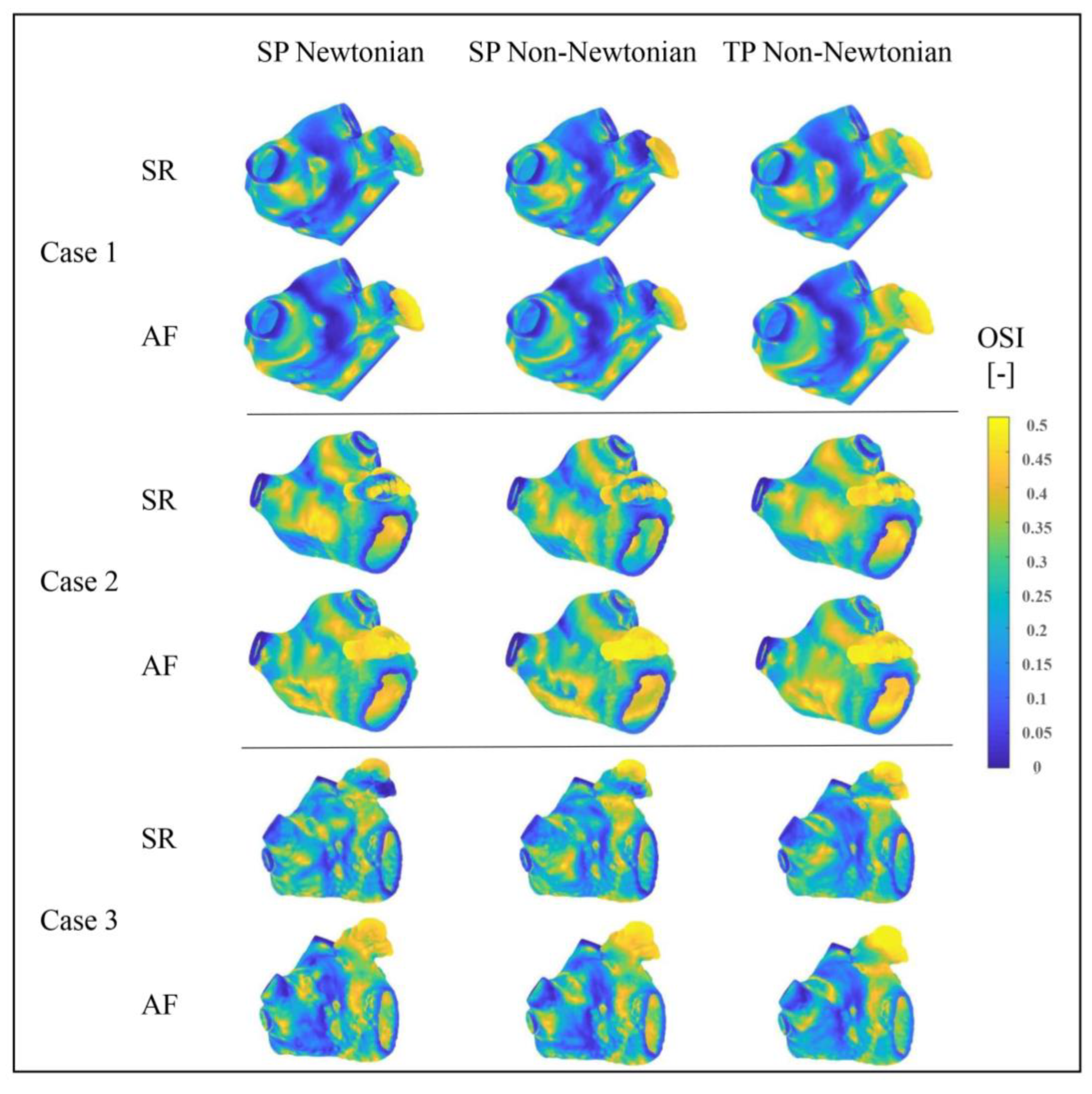
3.2.2. Effect of Blood Flow Models on OSI Value
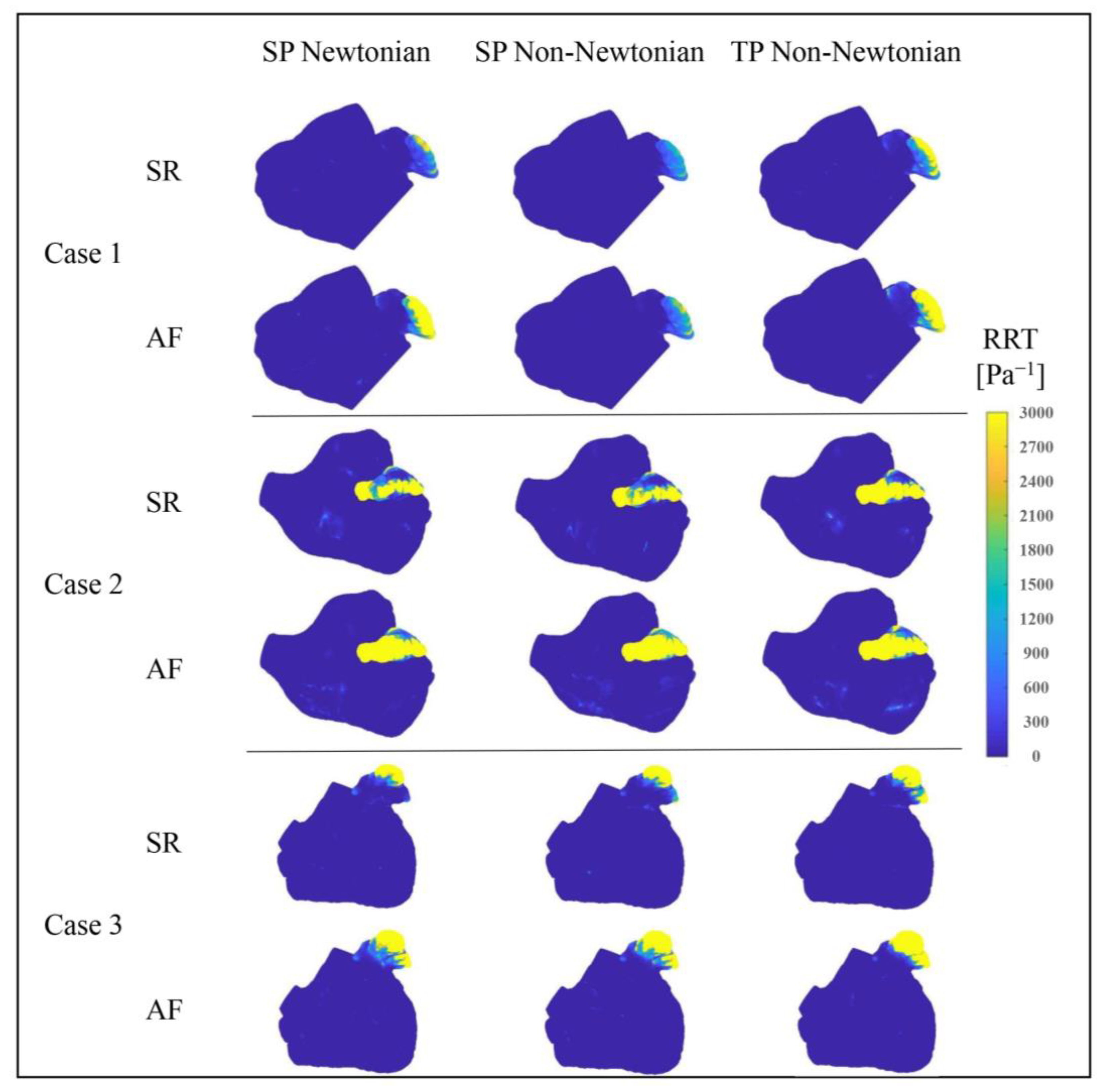
3.2.3. Effect of Blood Flow Models on RRT Value
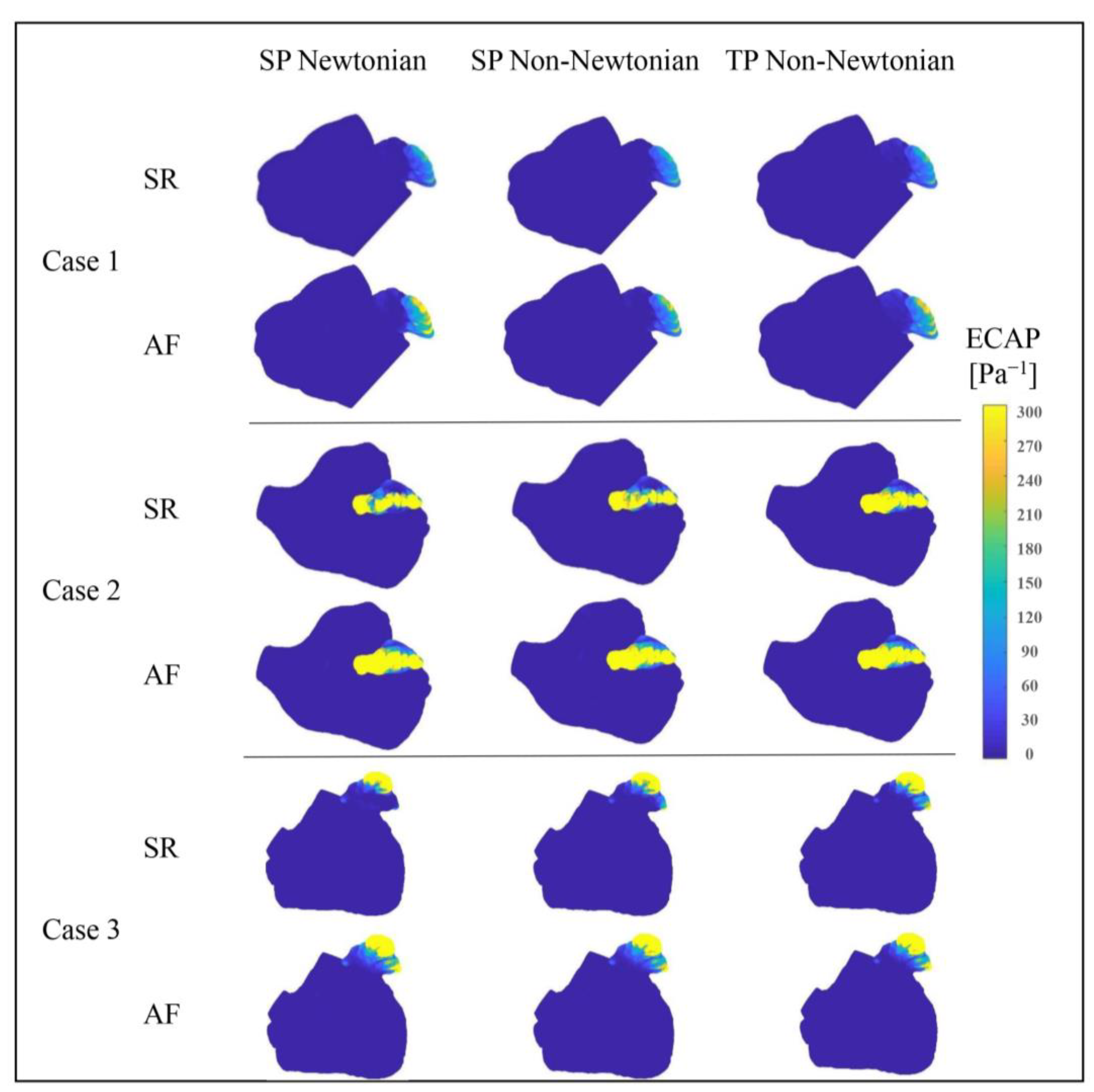
3.2.4. Effect of Blood Flow Models on ECAP Value
4. Discussion
5. Limitations
- We presumed the LA walls to be rigid. Although this assumption is feasible, particularly in the AF state where the LA wall barely contracts, it differs from the actual scenario. The interaction between the flexible LA wall and blood, along with the heart’s active contraction, can significantly affect the flow pattern. However, due to motion artifacts, dynamic cardiac CT/Magnetic Resonance Imaging (MRI) is not extensively performed on patients [36,37], thus creating a shortage of transient hemodynamic monitoring data and thereby complicating transient CFD simulations. In future research, the interaction between the flexible LA wall and blood will be considered. Currently, we are recruiting volunteers with AF for dynamic cardiac CT data collection.
- Given the limited conditions, we selected the MV outlet velocity waveform based on international norms to set the MV outlet velocity. Moving forward, the actual MV flow velocity of patients could be acquired as the boundary condition for simulation to procure more precise and individualized numerical simulation results.
- We simulated only three patients’ cases. It will be crucial to study a larger set of cases in the future to render the conclusions more accurate and reliable.
6. Conclusions
- Blood flow in the LA was roughly the same under both SR and AF when using the three different blood flow models. However, the flow-field details in some parts of LA, such as the “corner” of the LAA, are quite different. Moreover, the RT of blood in the LA under the single-phase non-Newtonian blood flow model is the shortest, especially in the SR state, while the RT of blood under the two-phase non-Newtonian blood flow is the longest.
- The OSI, RRT, and ECAP values of the LAA (with high risk of thrombosis) are all relatively lower when using the single-phase non-Newtonian blood flow model, indicating that the risk of thrombosis is lower. On the contrary, when using the two-phase non-Newtonian blood flow model, the RRT value in the LAA is relatively higher, causing the predicted risk of thrombosis to be higher.
- There are some differences in the values of the thrombosis risk calculated by different evaluation indicators in the simulation results obtained by using different blood flow models.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Singh, I.M.; Holmes, D.R. Left Atrial Appendage Closure. Curr. Cardiol. Rep. 2010, 12, 413–421. [Google Scholar] [CrossRef]
- Markl, M.; Lee, D.C.; Furiasse, N.; Carr, M.; Foucar, C.; Ng, J.; Carr, J.; Goldberger, J.J. Left Atrial and Left Atrial Appendage 4D Blood Flow Dynamics in Atrial Fibrillation. Circ. Cardiovasc. Imaging 2016, 9, e004984. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qureshi, A.; Darwish, O.I.; Dillon-Murphy, D.; Chubb, H.; Vecchi, A.D. Modelling Left Atrial Flow and Blood Coagulation for Risk of Thrombus Formation in Atrial Fibrillation. In Proceedings of the Computing in Cardiology 2020, Rimini, Italy, 13–16 September 2020. [Google Scholar] [CrossRef]
- Zhang, L.T.; Gay, M. Characterizing left atrial appendage functions in sinus rhythm and atrial fibrillation using computational models. J. Biomech. 2008, 41, 2515–2523. [Google Scholar] [CrossRef] [PubMed]
- Aguado, A.M.; Olivares, A.L.; Yagüe, C.; Silva, E.; Nuñez-García, M.; Fernandez-Quilez, Á.; Mill, J.; Genua, I.; Arzamendi, D.; De Potter, T.; et al. In silico Optimization of Left Atrial Appendage Occluder Implantation Using Interactive and Modeling Tools. Front. Physiol. 2019, 10, 237. [Google Scholar] [CrossRef] [Green Version]
- Olivares, A.L.; Silva, E.; Nuñez-Garcia, M.; Butakoff, C.; Sánchez-Quintana, D.; Freixa, X.; Noailly, J.; de Potter, T.; Camara, O. In Silico Analysis of Haemodynamics in Patient-Specific Left Atria with Different Appendage Morphologies. In Proceedings of the Functional Imaging and Modelling of the Heart, Toronto, ON, Canada, 11–13 June 2017; pp. 412–420. [Google Scholar] [CrossRef]
- Bosi, G.M.; Cook, A.; Rai, R.; Menezes, L.; Schievano, S.; Torii, R.; Burriesci, G.B. Computational Fluid Dynamic Analysis of the Left Atrial Appendage to Predict Thrombosis Risk. Front. Cardiovasc. Med. 2018, 5, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polanczyk, A.; Podyma, M.; Stefanczyk, L.; Szubert, W.; Zbicinski, I. A 3D model of thrombus formation in a stent-graft after implantation in the abdominal aorta. J. Biomech. 2015, 48, 425–431. [Google Scholar] [CrossRef] [PubMed]
- Qi, Y.; Lu, K.; Fa, J.; Ma, L.; Zhu, T. Numerical simulation of two-phase blood flow after thoracic endovascular aortic repair with in situ fenestration. J. Univ. Chin. Acad. Sci. 2020, 37, 192–197. [Google Scholar] [CrossRef]
- Zhang, Y.; Xie, H.W. Effects from non-inertial lift of red blood cells on blood flow. J. Med. Biomech. 2015, 30, 558–563. [Google Scholar]
- Johnston, B.M.; Johnston, P.R.; Corney, S.; Kilpatrick, D. Non-Newtonian blood flow in human right coronary arteries: Transient simulations. J. Biomech. 2006, 39, 1116–1128. [Google Scholar] [CrossRef] [Green Version]
- Jung, J.; Hassanein, A. Three-phase CFD analytical modeling of blood flow. Med. Eng. Phys. 2008, 30, 91–103. [Google Scholar] [CrossRef]
- Arzani, A. Accounting for residence-time in blood rheology models: Do we really need non-Newtonian blood flow modelling in large arteries? J. R. Soc. Interface 2018, 15, 20180486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonzalo, A.; García-Villalba, M.; Rossini, L.; Durán, E.; Vigneault, D.; Martínez-Legazpi, P.; Flores, O.; Bermejo, J.; McVeigh, E.; Kahn, A.M.; et al. Non-Newtonian blood rheology impacts left atrial stasis in patient-specific simulations. Int. J. Numer. Methods Biomed. Eng. 2022, 38, e3597. [Google Scholar] [CrossRef]
- Liu, H.; Lan, L.; Abrigo, J.; Ip, H.L.; Soo, Y.; Zheng, D.; Wong, K.S.; Wang, D.; Shi, L.; Leung, T.W.; et al. Comparison of Newtonian and Non-newtonian Fluid Models in Blood Flow Simulation in Patients with Intracranial Arterial Stenosis. Front. Physiol. 2021, 12, 718540. [Google Scholar] [CrossRef]
- Liu, H.; Gong, Y.; Leng, X.; Xia, L.; Wong, K.S.; Ou, S.; Leung, T.W.; Wang, D.; Shi, L. Estimating current and long-term risks of coronary artery in silico by fractional flow reserve, wall shear stress and low-density lipoprotein filtration rate. Biomed. Phys. Eng. Express 2018, 4, 025006. [Google Scholar] [CrossRef]
- Tsao, H.-M.; Wu, M.-H.; Yu, W.-C.; Tai, C.-T.; Lin, Y.-K.; Hsieh, M.-H.; Ding, Y.-A.; Chang, M.-S.; Chen, S.-A. Role of Right Middle Pulmonary Vein in Patients with Paroxysmal Atrial Fibrillation. J. Cardiovasc. Electrophysiol. 2001, 12, 1353–1357. [Google Scholar] [CrossRef]
- Cheng, Z.; Wood, N.B.; Gibbs, R.G.J.; Xu, X.Y. Geometric and flow features of type B aortic dissection: Initial findings and comparison of medically treated and stented cases. Ann. Biomed. Eng. 2014, 43, 177–189. [Google Scholar] [CrossRef]
- Yang, J.; Song, C.; Ding, H.; Chen, M.; Sun, J.; Liu, X. Numerical study of the risk of thrombosis in the left atrial appendage of chicken wing shape in atrial fibrillation. Front. Cardiovasc. Med. 2022, 9, 985674. [Google Scholar] [CrossRef] [PubMed]
- Soulis, J.V.; Lampri, O.P.; Fytanidis, D.K.; Giannoglou, G.D. Relative residence time and oscillatory shear index of non-Newtonian flow models in aorta. In Proceedings of the 2011 10th International Workshop on Biomedical Engineering, Kos, Greece, 5–7 October 2011; pp. 1–4. [Google Scholar] [CrossRef]
- García-Isla, G.; Olivares, A.L.; Silva, E.; Nuñez-Garcia, M.; Butakoff, C.; Sanchez-Quintana, D.; Morales, H.G.; Freixa, X.; Noailly, J.; De Potter, T.; et al. Sensitivity analysis of geometrical parameters to study haemodynamics and thrombus formation in the left atrial appendage. Int. J. Numer. Methods Biomed. Eng. 2018, 34, e3100. [Google Scholar] [CrossRef] [PubMed]
- Mill, J.; Agudelo, V.; Olivares, A.L.; Pons, M.I.; Silva, E.; Nuñez-Garcia, M.; Morales, X.; Arzamendi, D.; Freixa, X.; Noailly, J.; et al. Sensitivity Analysis of In Silico Fluid Simulations to Predict Thrombus Formation after Left Atrial Appendage Occlusion. Mathematics 2021, 9, 2304. [Google Scholar] [CrossRef]
- Di Achille, P.; Tellides, G.; Figueroa, C.A.; Humphrey, J.D. A haemodynamic predictor of intraluminal thrombus formation in abdominal aortic aneurysms. Proc. R. Soc. A Math. Phys. Eng. Sci. 2014, 470, 20140163. [Google Scholar] [CrossRef]
- Liu, B. The influences of stenosis on the downstream flow pattern in curved arteries. Med. Eng. Phys. 2007, 29, 868–876. [Google Scholar] [CrossRef]
- Moore, S.; David, T.; Chase, J.G.; Arnold, J.; Fink, J. 3D models of blood flow in the cerebral vasculature. J. Biomech. 2006, 39, 1454–1463. [Google Scholar] [CrossRef] [Green Version]
- Quemada, D. A rheological model for studying the hematocrit dependence of red cell-red cell and red cell-protein inter-actions in blood. Biorheology 1981, 18, 501–516. [Google Scholar] [CrossRef]
- Jung, J.; Lyczkowski, R.W.; Panchal, C.B.; Hassanein, A. Multiphase hemodynamic simulation of pulsatile flow in a coronary artery. J. Biomech. 2006, 39, 2064–2073. [Google Scholar] [CrossRef] [PubMed]
- Kowal, P.; Marcinkowska-Gapińska, A. Hemorheological changes dependent on the time from the onset of ischemic stroke. J. Neurol. Sci. 2007, 258, 132–136. [Google Scholar] [CrossRef]
- Institution, B.S. BS EN ISO 5840-1; Cardiovascular Implants—Cardiac Valve Prostheses—Part 1: General Requirements. ISO: Geneva, Switzerland, 2015.
- Gautam, S.; John, R.M. Interatrial electrical dissociation after catheter-based ablation for atrial fibrillation and flutter. Circ. Arrhythmia Electrophysiol. 2011, 4, 26–28. [Google Scholar] [CrossRef] [Green Version]
- Jhunjhunwala, P.; Padole, P.; Thombre, S. CFD Analysis of Pulsatile Flow and Non-Newtonian Behavior of Blood in Arteries. MCB Mol. Cell. Biomech. 2015, 12, 37–47. [Google Scholar]
- Dahl, S.K.; Thomassen, E.; Hellevik, L.R.; Skallerud, B. Impact of Pulmonary Venous Locations on the Intra-Atrial Flow and the Mitral Valve Plane Velocity Profile. Cardiovasc. Eng. Technol. 2012, 3, 269–281. [Google Scholar] [CrossRef] [Green Version]
- Menichini, C.; Xu, X.Y. Mathematical modeling of thrombus formation in idealized models of aortic dissection: Initial findings and potential applications. J. Math. Biol. 2016, 73, 1205–1226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karino, T.; Goldsmith, H.L. Flow behaviour of blood cells and rigid spheres in an annular vortex. Philos. Trans. R. Soc. Lond. B Biol. Sci. 1977, 279, 413–445. [Google Scholar] [CrossRef]
- Malvè, M.; García, A.; Ohayon, J.; Martínez, M.A. Unsteady blood flow and mass transfer of a human left coronary artery bifurcation: FSI vs. CFD. Int. Commun. Heat Mass Transf. 2012, 39, 745–751. [Google Scholar] [CrossRef]
- Liu, H.; Wingert, A.; Wang, J.A.; Zhang, J.; Wang, X.; Sun, J.; Chen, F.; Khalid, S.G.; Jiang, J.; Zheng, D. Extraction of Coronary Atherosclerotic Plaques from Computed Tomography Imaging: A Review of Recent Methods. Front. Cardiovasc. Med. 2021, 8, 597568. [Google Scholar] [CrossRef] [PubMed]
- Nieman, K.; Balla, S. Dynamic CT myocardial perfusion imaging. J. Cardiovasc. Comput. Tomogr. 2019, 14, 303–306. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, D.; Jani, N.D.; Selvaganesan, K.; Weng, C.L.; Shadden, S.C. Computational Assessment of the Relation between Embolism Source and Embolus Distribution to the Circle of Willis for Improved Understanding of Stroke Etiology. J. Biomech. Eng. 2016, 138, 081008. [Google Scholar] [CrossRef]
- Liu, H.; Pan, F.; Lei, X.; Hui, J.; Gong, R.; Feng, J.; Zheng, D. Effect of intracranial pressure on photoplethysmographic waveform in different cerebral perfusion territories: A computational study. Front. Physiol. 2023, 14, 1085871. [Google Scholar] [CrossRef]


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | LA Volume (mL) | LAA Volume (mL) | Mitral Orifice Area (cm2) | Number of Pulmonary Veins (PVs) |
|---|---|---|---|---|
| 1 | 136.08 | 19.33 | 9.57 | 4 |
| 2 | 213.40 | 20.98 | 9.69 | 4 |
| 3 | 122.69 | 19.48 | 8.70 | 5 |
| State | Case | Flow Model | Ave. TAWSS in LA (Pa−1) | Ave. TAWSS in LAA (Pa−1) |
|---|---|---|---|---|
| SR | Case 1 | SP Newtonian | 0.3588 | 0.0282 |
| SP non-Newtonian | 0.2893 | 0.0278 | ||
| TP non-Newtonian | 0.3613 | 0.0290 | ||
| Case 2 | SP Newtonian | 0.3185 | 0.0192 | |
| SP non-Newtonian | 0.2566 | 0.0185 | ||
| TP non-Newtonian | 0.3193 | 0.0208 | ||
| Case 3 | SP Newtonian | 0.4044 | 0.0331 | |
| SP non-Newtonian | 0.3262 | 0.0337 | ||
| TP non-Newtonian | 0.4037 | 0.0386 | ||
| AF | Case 1 | SP Newtonian | 0.2803 | 0.0179 |
| SP non-Newtonian | 0.2324 | 0.0197 | ||
| TP non-Newtonian | 0.2889 | 0.0206 | ||
| Case 2 | SP Newtonian | 0.2383 | 0.0120 | |
| SP non-Newtonian | 0.1942 | 0.0112 | ||
| TP non-Newtonian | 0.2421 | 0.0158 | ||
| Case 3 | SP Newtonian | 0.3089 | 0.0230 | |
| SP non-Newtonian | 0.2534 | 0.0209 | ||
| TP non-Newtonian | 0.3109 | 0.0289 |
| State | Case | Flow Model | Ave. RRT Value of LA (Pa−1) | Ave. RRT Value of LAA (Pa−1) |
|---|---|---|---|---|
| SR | Case 1 | SP Newtonian | 10.69 | 414.00 |
| SP non-Newtonian | 12.36 | 1257.73 | ||
| TP non-Newtonian | 9.70 | 1167.37 | ||
| Case 2 | SP Newtonian | 18.25 | 30,534.14 | |
| SP non-Newtonian | 21.82 | 17,758.14 | ||
| TP non-Newtonian | 17.32 | 35,697.30 | ||
| Case 3 | SP Newtonian | 11.01 | 41,553.43 | |
| SP non-Newtonian | 12.59 | 4829.39 | ||
| TP non-Newtonian | 9.48 | 11,569.01 | ||
| AF | Case 1 | SP Newtonian | 16.34 | 4212.30 |
| SP non-Newtonian | 16.68 | 846.95 | ||
| TP non-Newtonian | 13.48 | 4272.21 | ||
| SP Newtonian | 27.54 | 118,042.04 | ||
| Case 2 | SP non-Newtonian | 34.37 | 131,275.75 | |
| TP non-Newtonian | 30.95 | 153,265.30 | ||
| Case 3 | SP Newtonian | 13.19 | 31,588.81 | |
| SP non-Newtonian | 16.08 | 6819.30 | ||
| TP non-Newtonian | 12.26 | 21,834.54 |
| State | Case | Flow Model | Ave. ECAP Value of LA (Pa−1) | Ave. ECAP Value of LAA (Pa−1) |
|---|---|---|---|---|
| SR | Case 1 | SP Newtonian | 0.93 | 37.24 |
| SP non-Newtonian | 1.12 | 41.05 | ||
| TP non-Newtonian | 0.89 | 42.72 | ||
| Case 2 | SP Newtonian | 1.51 | 706.80 | |
| SP non-Newtonian | 1.80 | 480.37 | ||
| TP non-Newtonian | 1.38 | 665.78 | ||
| Case 3 | SP Newtonian | 0.96 | 138.88 | |
| SP non-Newtonian | 1.09 | 81.21 | ||
| TP non-Newtonian | 0.86 | 105.32 | ||
| AF | Case 1 | SP Newtonian | 1.34 | 77.77 |
| SP non-Newtonian | 1.51 | 49.78 | ||
| TP non-Newtonian | 1.19 | 69.22 | ||
| Case 2 | SP Newtonian | 2.22 | 1119.29 | |
| SP non-Newtonian | 2.59 | 794.72 | ||
| TP non-Newtonian | 2.04 | 938.10 | ||
| Case 3 | SP Newtonian | 1.14 | 197.79 | |
| SP non-Newtonian | 1.35 | 137.74 | ||
| TP non-Newtonian | 1.02 | 157.88 |
| Indicators | Flow Model | Predicted Thrombosis Risk |
|---|---|---|
| RRT | SP Newtonian | Medium |
| SP non-Newtonian | Lower | |
| TP non-Newtonian | Higher | |
| ECAP | SP Newtonian | Higher |
| SP non-Newtonian | Lower | |
| TP non-Newtonian | Medium |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, J.; Bai, Z.; Song, C.; Ding, H.; Chen, M.; Sun, J.; Liu, X. Research on the Internal Flow Field of Left Atrial Appendage and Stroke Risk Assessment with Different Blood Models. Bioengineering 2023, 10, 944. https://doi.org/10.3390/bioengineering10080944
Yang J, Bai Z, Song C, Ding H, Chen M, Sun J, Liu X. Research on the Internal Flow Field of Left Atrial Appendage and Stroke Risk Assessment with Different Blood Models. Bioengineering. 2023; 10(8):944. https://doi.org/10.3390/bioengineering10080944
Chicago/Turabian StyleYang, Jun, Zitao Bai, Chentao Song, Huirong Ding, Mu Chen, Jian Sun, and Xiaohua Liu. 2023. "Research on the Internal Flow Field of Left Atrial Appendage and Stroke Risk Assessment with Different Blood Models" Bioengineering 10, no. 8: 944. https://doi.org/10.3390/bioengineering10080944