
Isochoric Supercooling Organ Preservation System
 , , and
, , and
Abstract
:
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
- Heart: The heart can typically be stored for about 4 to 6 h using cold storage.
- Liver: The liver can be stored using cold storage for approximately 8 to 12 h.
- Kidneys: Kidneys are relatively robust organs and can be stored using cold storage for a longer period compared to other organs. Typically, kidneys can be preserved for around 24 to 36 h using cold storage.
- Pancreas: The pancreas can be stored for approximately 12 to 18 h using cold storage.
2. Materials and Methods
2.1. Principles of Design
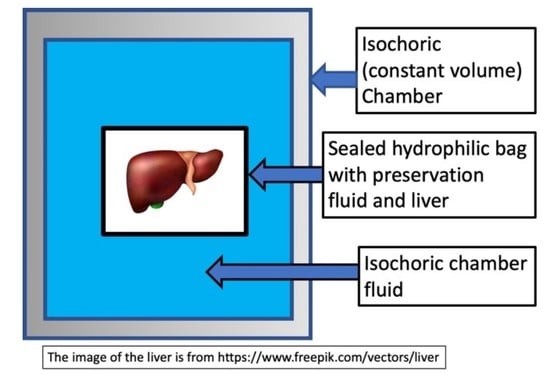
2.2. Isochoric Supercooling Preservation Chamber
2.3. Refrigeration System
2.4. Control Hardware and Software
2.5. Experimental Protocol
3. Results and Discussion
3.1. Control System in Response to Ice Nucleation
3.2. Experiments on Ice Nucleation in a Sham Study with a Non-Viable Pig Liver in a Cold Storage Solution in a Polymer Bag
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Taylor, M.J.; Weegman, B.P.; Baicu, S.C.; Giwa, S.E. New Approaches to Cryopreservation of Cells, Tissues, and Organs. Transfus. Med. Hemother. 2019, 46, 197–215. [Google Scholar] [CrossRef] [PubMed]
- Lewis, J.K.; Bischof, J.C.; Braslavsky, I.; Brockbank, K.G.M.; Fahy, G.M.; Fuller, B.J.; Rabin, Y.; Tocchio, A.; Woods, E.J.; Wowk, B.G.; et al. The Grand Challenges of Organ Banking: Proceedings from the First Global Summit on Complex Tissue Cryopreservation. Cryobiology 2016, 72, 169–182. [Google Scholar] [CrossRef] [PubMed]
- Giwa, S.; Lewis, J.K.; Alvarez, L.; Langer, R.; Roth, A.E.; Church, G.M.; Markmann, J.F.; Sachs, D.H.; Chandraker, A.; Wertheim, J.A.; et al. The Promise of Organ and Tissue Preservation to Transform Medicine. Nat. Biotechnol. 2017, 35, 530–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clavien, P.-A.; Dutkowski, P.; Mueller, M.; Eshmuminov, D.; Burg, B.R.; von Rohr, P.R.; Schuler, M.J.; Becker, D.; Hefti, M.; Tibbit, M.W. Transplantation of a Human Liver Following 3 Days of Ex Situ Normothermic Preservation. Nat. Biotechnol. 2022, 40, 1610–1616. [Google Scholar] [CrossRef]
- Jing, L.; Yao, L.; Zhao, M.; Peng, L.; Liu, M. Organ Preservation: From the Past to the Future. Acta Pharmacol. Sin. 2018, 39, 845–857. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collins, G.M.; Bravo-Shugarman, M.; Terasaki, P. Kidney Preservation for Transportation: Initial Perfusion and 30 Hours’ Ice Storage. Lancet 1969, 294, 1219–1222. [Google Scholar] [CrossRef] [PubMed]
- Belzer, F.O.; Southard, J.H. Principles of Solid Organ Preservation by Cold Storage. Transplantation 1988, 45, 673–676. [Google Scholar] [CrossRef]
- Southard, J.H.; Belzer, F.O. Organ Preservation. Annu. Rev. Med. 1995, 46, 235–247. [Google Scholar] [CrossRef]
- Dalessandro, A.M.; Southard, J.H.; Love, R.B.; Belzer, F.O. Organ Preservation. Surg. Clin. N. Am. 1994, 74, 1083–1095. [Google Scholar] [CrossRef] [PubMed]
- Mazur, P. Cryobiology: The Freezing of Biological Systems. Science 1970, 168, 939–949. [Google Scholar] [CrossRef]
- Mazur, P. Freezing of Living Cells-Mechanisms and Implications. Am. J. Physiol. 1984, 247, C125–C142. [Google Scholar] [CrossRef] [PubMed]
- Leibo, S.P.; Pool, T.B. The Principal Variables of Cryopreservation: Solutions, Temperatures, and Rate Changes. Fertil. Steril. 2011, 96, 269–276. [Google Scholar] [CrossRef] [PubMed]
- Pegg, D.E. Principles of Cryopreservation. In Cryopreservation and Freeze-Drying Protocols; Wolkers, W., Oldenhof, H., Eds.; Humana Press Inc.: Totowa, NJ, USA, 2015; Volume 1257, pp. 3–19. ISBN 978-1-59745-362-2. [Google Scholar]
- Smith, A.U.; Polge, C. Survival of Spermatozoa at Low Temperatures. Nature 1950, 166, 668–669. [Google Scholar] [CrossRef] [PubMed]
- Polge, C.; Smith, A.U.; Parkes, A.S. Revival of Spermatozoa after Vitrification and Dehydration at Low Temperatures. Nature 1949, 164, 666. [Google Scholar] [CrossRef]
- Trounson, A.; Mohr, L. Human Pregnancy Following Cryopreservation, Thawing and Transfer of an Eight-Cell Embryo. Nature 1983, 305, 707–709. [Google Scholar] [CrossRef]
- Chen, C. Pregnancy after Human Oocytes Cryopreservation. Lancet 1986, 327, 884–886. [Google Scholar] [CrossRef] [PubMed]
- Kojayan, G.G.; Alexander, M.; Imagawa, D.K.; Lakey, J.R.T. Systematic Review of Islet Cryopreservation. Islets 2018, 10, 40–49. [Google Scholar] [CrossRef] [PubMed]
- Jacobsen, I.A.; Pegg, D.E. Cryopreservation of Organs—A Review. Cryobiology 1983, 20, 698. [Google Scholar] [CrossRef]
- Luyet, B. On the Supercooling of Water. Phys. Rev. 1952, 85, 746. [Google Scholar]
- Huang, H.; Yarmush, M.L.; Usta, O.B. Long-Term Deep-Supercooling of Large-Volume Water and Red Cell Suspensions via Surface Sealing with Immiscible Liquids. Nat. Commun. 2018, 9, 3201. [Google Scholar] [CrossRef] [Green Version]
- Bruinsma, B.G.; Berendsen, T.A.; Izamis, M.L.; Yeh, H.; Yarmush, M.L.; Uygun, K. Supercooling Preservation and Transplantation of the Rat Liver. Nat. Protoc. 2015, 10, 484–494. [Google Scholar] [CrossRef]
- Puts, C.F.; Berendsen, T.A.; Bruinsma, B.G.; Ozer, S.; Luitje, M.; Usta, O.B.; Yarmush, M.L.; Uygun, K. Polyethylene Glycol Protects Primary Hepatocytes during Supercooling Preservation. Cryobiology 2015, 71, 125–129. [Google Scholar] [CrossRef] [Green Version]
- Usta, O.B.; Kim, Y.; Ozer, S.; Bruinsma, B.B.; Lee, J.; Demir, E.; Berendsenm, T.A.; Puts, C.F.; Izamis, M.-L.; Uygun, K.; et al. Supercooling as a Viable Non-Freezing Cell Preservaion Method of Rat Hepatocytes. PLoS ONE 2013, 8, e69334. [Google Scholar] [CrossRef] [Green Version]
- Berendsen, T.A.; Bruinsma, B.G.; Puts, C.F.; Saeidi, N.; Usta, O.B.; Uygun, B.E.; Izamis, M.L.; Toner, M.; Yarmush, M.L.; Uygun, K. Supercooling Enables Long-Term Transplantation Survival Following 4 Days of Liver Preservation. Nat. Med. 2014, 20, 790–793. [Google Scholar] [CrossRef] [PubMed]
- de Vries, R.J.; Tessier, S.N.; Banik, P.D.; Nagpal, S.; Cronin, S.E.J.; Ozer, S.; Hafiz, E.O.A.; van Gulik, T.M.; Yarmush, M.L.; Markmann, J.F.; et al. Subzero Non-Frozen Preservation of Human Livers in the Supercooled State. Nat. Protoc. 2020, 15, 2024–2040. [Google Scholar] [CrossRef]
- de Vries, R.J.; Tessier, S.N.; Banik, P.D.; Nagpal, S.; Cronin, S.E.J.; Ozer, S.; Hafiz, E.O.A.; van Gulik, T.M.; Yarmush, M.L.; Markmann, J.F.; et al. Supercooling Extends Preservation Time of Human Livers. Nat. Biotechnol. 2019, 37, 1131–1136. [Google Scholar] [CrossRef] [PubMed]
- Tessier, S.N.; de Vries, R.J.; Pendexter, C.A.; Cronin, S.E.; Ozer, S.; Hafiz, E.O.; Raigani, S.; Oliveira-Costa, J.P.; Wilks, B.T.; Lopera Higuita, M.; et al. Partial Freezing of Rat Livers Extends Preservation Time by 5-Fold. Nat. Commun. 2022, 13, 4008. [Google Scholar] [CrossRef]
- de Vries, R.; Tessier, S.N.; Banik, P.D.; Ozer, S.; Crorin, S.E.J.; Nagpal, S.; Yeh, H.; Uygun, K. Extending the Human Liver Preservation Time for Transplantation by Supercooling. Transplantation 2018, 102, S396. [Google Scholar] [CrossRef]
- Ueno, T.; Omura, T.; Takahashi, T.; Matsumoto, H.; Takahashi, Y.; Kakita, A.; Yamashina, S. Liver Transplantation Using Liver Grafts Preserved under High Pressure. Artif. Organs 2005, 29, 849–855. [Google Scholar] [CrossRef]
- Takahashi, T.; Kakita, A.; Takashi, Y.; Yokoyama, K.; Sakamoto, I.; Yamashina, S.; Takahashi, Y.; Yokoyama, K.; Sakamoto, I.; Yamashina, S. Preservation of Rat Livers by Supercooling under High Pressure. Transplant. Proc. 2001, 33, 916–919. [Google Scholar] [CrossRef]
- Takahashi, T.; Kakita, A.; Takahashi, Y.; Sakamoto, I.; Yokoyama, K.; Fujiu, T.; Yamashina, S.; Tamaki, T.; Takazawa, Y.; Muratsubaki, R. Functional Integrity of the Rat Liver after Subzero Preservation under High Pressure. Transplant. Proc. 2000, 32, 1634–1636. [Google Scholar] [CrossRef] [PubMed]
- Monzen, K.; Hosoda, T.; Hayashi, D.; Imai, Y.; Okawa, Y.; Kohro, T.; Uozaki, H.; Nishiyama, T.; Fukayama, M.; Nagai, R.; et al. The Use of a Supercooling Refrigerator Improves the Preservation of Organ Grafts. Biochem. Biophys. Res. Commun. 2005, 337, 534–539. [Google Scholar] [CrossRef] [PubMed]
- Rubinsky, B.; Perez, P.A.; Carlson, E.M. The Thermodynamic Principles of Isochoric Cryopreservation. Cryobiology 2005, 50, 121–138. [Google Scholar] [CrossRef] [PubMed]
- Powell-Palm, M.J. Calculations of a Temperature-Volume Phase Diagram of Water to Inform the Study of Isochoric Freezing down to Cryogenic Temperaturess. RSC Adv. 2022, 12, 20603–20609. [Google Scholar] [CrossRef]
- McHugh, T.; Bilbao-Sainz, C. Isochoric Freezing: A New Technology for Food Preservation. Food Technol. 2019, 73, 66–68. [Google Scholar]
- Nida, S.; Moses, J.A.; Anandharamakrishnan, C. Isochoric Freezing and Its Emerging Applications in Food Preservation. Food Eng. Rev. 2021, 13, 812–821. [Google Scholar] [CrossRef]
- Chavez-Quesada, J.; Acosta-Montoya, O. Isochoric Freezing: Advantages and Research Opportunities in the Food Industry. Agon. Mesoam. 2023, 34, 52879. [Google Scholar] [CrossRef]
- Powell-Palm, M.J.; Koh-Bell, A.; Rubinsky, B. Isochoric Conditions Enhance Stability of Metastable Supercooled Water. Appl. Phys. Lett. 2020, 116, 123702. [Google Scholar] [CrossRef]
- Powell-Palm, M.J.; Charwat, V.; Charrez, B.; Siemons, B.; Healy, K.E.; Rubinsky, B. Isochoric Supercooled Preservation and Revival of Human Cardiac Microtissues. Commun. Biol. 2021, 4, 1118. [Google Scholar] [CrossRef]
- Vasileiou, T.; Schutzius, T.M.; Poulikakos, D. Imparting Icephobicity with Substrate Flexibility. Langmuir 2017, 33, 6708–6718. [Google Scholar] [CrossRef] [Green Version]
- Szobota, S.A.; Rubinsky, B. Analysis of Isochoric Subcooling. Cryobiology 2006, 53, 139–142. [Google Scholar] [CrossRef] [PubMed]
- Perez; Pedro, A. Thermodynamic and Heat Transfer Analysis for Isochoric Cryopreservation. Ph.D. Thesis, Department of Mechanical Engineering, University of California Berkeley, Berkeley, CA, USA, 2006. (OCoLC)945, OCLC Number: 892833675. [Google Scholar]













Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Năstase, G.; Botea, F.; Beșchea, G.-A.; Câmpean, Ș.-I.; Barcu, A.; Neacșu, I.; Herlea, V.; Popescu, I.; Chang, T.T.; Rubinsky, B.; et al. Isochoric Supercooling Organ Preservation System. Bioengineering 2023, 10, 934. https://doi.org/10.3390/bioengineering10080934
Năstase G, Botea F, Beșchea G-A, Câmpean Ș-I, Barcu A, Neacșu I, Herlea V, Popescu I, Chang TT, Rubinsky B, et al. Isochoric Supercooling Organ Preservation System. Bioengineering. 2023; 10(8):934. https://doi.org/10.3390/bioengineering10080934
Chicago/Turabian StyleNăstase, Gabriel, Florin Botea, George-Andrei Beșchea, Ștefan-Ioan Câmpean, Alexandru Barcu, Ion Neacșu, Vlad Herlea, Irinel Popescu, Tammy T. Chang, Boris Rubinsky, and et al. 2023. "Isochoric Supercooling Organ Preservation System" Bioengineering 10, no. 8: 934. https://doi.org/10.3390/bioengineering10080934