

SeizFt: Interpretable Machine Learning for Seizure Detection Using Wearables

Abstract
:1. Introduction
- First, we propose a deep learning model that combines CNN, Long Short-Term Memory (LSTM), and multi-headed attention elements outperforming traditional deep learning methods.
- We propose SeizFt, a robust and explainable seizure detection method for wearable EEG devices. This framework merges several computational strategies, including feature extraction, data augmentation via Fourier Transform (FT) Surrogates, class balancing, and a CatBoost-driven ensemble of decision trees.
- By means of comprehensive experimental analysis, we validate the superior performance of SeizFt. We show that our model excels in terms of sensitivity and false alarm rates, consistently outperforming other established state-of-the-art methods.
- Importantly, we highlight the vital, clinically interpretable features that SeizFt employs to characterize seizures as captured by EEG. These critical features underline the interpretability of our model, enhancing trust in its predictive ability and marking a significant advance in the integration of machine learning within a clinical context.
- Finally, we consider the practical implications and future potential of SeizFt, asserting that it establishes a new benchmark for seizure detection using wearable EEG and suggest possible directions for future research and application. This, we believe, will inspire advancements that could profoundly impact patient care.
2. The 2023 ICASSP Seizure Detection Grand Challenge
2.1. Tasks
2.2. Data Sources
2.2.1. SeizeIt1 Dataset—Training Set
2.2.2. SeizeIT2 Dataset—Validation and Test Set
2.3. Performance Metrics
3. Methods
3.1. SeizFt Model Framework
3.1.1. Data Augmentation and Class Balancing
3.1.2. Feature Extraction
3.1.3. Model Training
3.2. Experimental Setup
3.3. Baselines
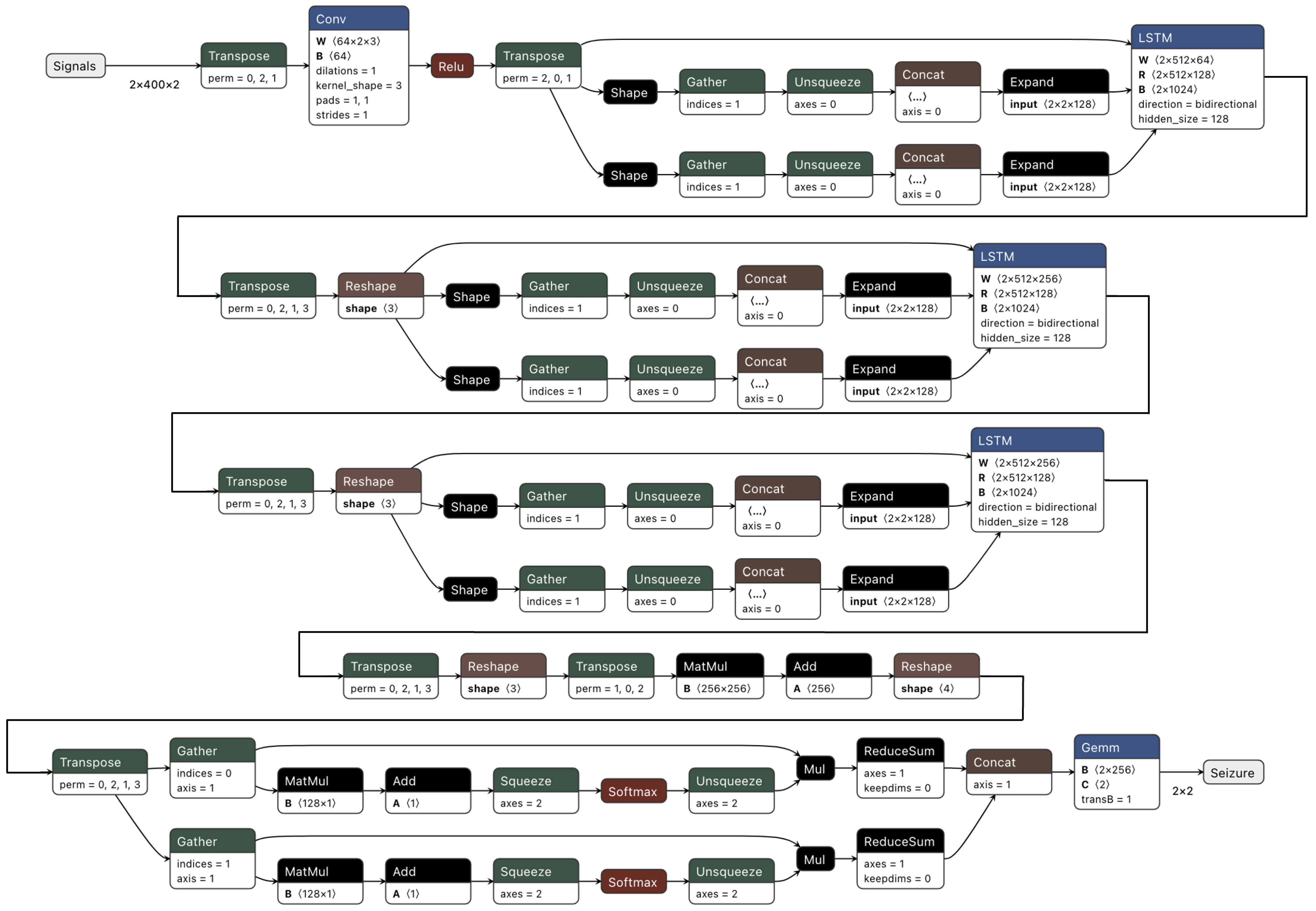
- AttentionNet: The architecture, as depicted in Figure 2, integrates a neural network comprised of CNN layers followed by LSTM layers. It is augmented with a multi-headed attention mechanism.
- ChronoNet [45]: This approach utilized a novel Recurrent Neural Network (RNN) architecture, dubbed ChronoNet, which was inspired by recent advancements in image classification. The authors adapted the methodology to EEG data interpretation to improve the efficiency and accuracy in distinguishing between normal and abnormal brain activity. ChronoNet incorporates multiple 1D convolution layers followed by deep Gated Recurrent Unit (GRU) layers, taking raw time-series EEG data and learning to identify patterns in brain activity.
- Transformer and CNN [60]: Recognizing the limitation of conventional EEG systems and the need for timely and accurate diagnosis, the authors adopted a transformer-based deep neural network approach. This model incorporated a mixed Transformer and CNN architecture, which was trained and pre-trained on several datasets, including the Temple University Hospital Seizure Corpus [61]. To improve the model’s robustness and mitigate overfitting, dropout, and early stopping techniques were employed. For the second task, the authors enhanced the ChronoNet architecture for abnormal EEG detection by boosting the signal-to-noise ratio in EEG data and optimizing various training parameters.
- Spectral Power and Random Forest [62]: This approach to epilepsy monitoring used lightweight machine-learning models specifically tailored for resource-constrained wearable devices. The framework uses the Random Forest (RF) algorithm in conjunction with power features extracted from specific EEG frequency bands for seizure detection. The power features were derived from different frequency ranges and are calculated through a combination of time-domain band-pass filtering and the application of Parseval’s theorem to the filtered signal. For the RF algorithm, an ensemble of relatively shallow decision trees is employed. The final prediction was obtained by voting on the outcomes of all the trees, which reduces computational complexity for real-time inference on wearable devices. In the second task, the data-centric ChronoNet architecture was utilized to optimize certain hyperparameters to balance seizure detection sensitivity and false alarm rates.
- Deep Convolutional Neural Network [63]: EEG data were preprocessed, standardized, and segmented into 2-second intervals before model training. Experiments were performed with several deep CNN architectures and a range of input types, such as raw EEG signals, Short-time Fourier Transform (STFT) transformed signals, wavelets, and mel scale spectral transformations. Over 100 different DCNN models were trained. The optimal models were chosen based on the mean of lower boundaries of 95% confidence intervals for cross-validation and hold-out scores. Additionally, data augmentation techniques were implemented in the second task to improve the performance of the ChronoNet architecture.
4. Results
4.1. Comparative Analysis

{kind=link}
{kind=link}
{kind=link}
| Sensitivity (OVLP [49]) | False Alarms per Hour (EPOCH [49]) | Total Score | |
|---|---|---|---|
| ChronoNet [45] | 58.22 | 117.12 | 11.37 |
| AttentionNet (Figure 2) | 53.57 | 30.85 | 41.23 |
| SeizFt (Task 1) | 62.86 | 14.93 | 56.88 |
| ChronoNet (Task 2) | 22.22 | 9.82 | 18.30 |
| Score Task 1 | Score Task 2 | Total Score | |
|---|---|---|---|
| Benchmark | 45.10 | 10.42 | 31.03 |
| Pathology Dynamics (SeizFt) | 47.57 | 29.01 | 40.15 |
| UCLA CDx [60] | 26.92 | 29.32 | 27.88 |
| Neural Engineering Lab [62] | 36.98 | 4.06 | 23.81 |
| Brainify.ai [63] | 6.54 | 25.21 | 14.00 |
4.2. Model Interpretation
4.3. Model Robustness and Generalizability
5. Discussion
- We propose a deep neural network that incorporates CNN, LSTM, and multi-headed attention elements, which outperforms other deep learning techniques.
- We introduce SeizFt, a robust and interpretable framework for seizure detection in wearable EEGs, which amalgamates feature extraction, data augmentation via Fourier Transform (FT) Surrogates, class balancing, and a CatBoost-driven ensemble of decision trees.
- Through experimental evaluation, we illustrate the superior performance of our SeizFt framework in terms of sensitivity and false alarm rates relative to existing state-of-the-art methods.
- We elucidate the crucial, clinically interpretable features employed by the SeizFt framework that characterize seizures as measured via EEG. The SeizFt features enhance trust in the model’s predictive capability.
5.1. Interpretable Models Can Compete with Black-Box Models
5.2. Evaluation of Design Choices That Made SeizFt a Success
5.3. Potential for Clinical Impact
5.4. Limitations and Future Directions
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Paz, J.T.; Huguenard, J.R. Microcircuits and their interactions in epilepsy: Is the focus out of focus? Nat. Neurosci. 2015, 18, 351–359. [Google Scholar] [CrossRef] [Green Version]
- Staley, K. Molecular mechanisms of epilepsy. Nat. Neurosci. 2015, 18, 367–372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jirsa, V.K.; Stacey, W.C.; Quilichini, P.P.; Ivanov, A.I.; Bernard, C. On the nature of seizure dynamics. Brain 2014, 137, 2210–2230. [Google Scholar] [CrossRef] [Green Version]
- Hauser, W.A. Seizure disorders: The changes with age. Epilepsia 1992, 33, 6–14. [Google Scholar] [CrossRef] [PubMed]
- Jory, C.; Shankar, R.; Coker, D.; McLean, B.; Hanna, J.; Newman, C. Safe and sound? A systematic literature review of seizure detection methods for personal use. Seizure 2016, 36, 4–15. [Google Scholar] [CrossRef] [Green Version]
- Gómez, C.; Arbeláez, P.; Navarrete, M.; Alvarado-Rojas, C.; Le Van Quyen, M.; Valderrama, M. Automatic seizure detection based on imaged-EEG signals through fully convolutional networks. Sci. Rep. 2020, 10, 21833. [Google Scholar] [CrossRef]
- Wang, Z.; Mengoni, P. Seizure classification with selected frequency bands and EEG montages: A Natural Language Processing approach. Brain Inform. 2022, 9, 11. [Google Scholar] [CrossRef] [PubMed]
- Yan, X.; Yang, D.; Lin, Z.; Vucetic, B. Significant low-dimensional spectral-temporal features for seizure detection. IEEE Trans. Neural Syst. Rehabil. Eng. 2022, 30, 668–677. [Google Scholar] [CrossRef] [PubMed]
- Thompson, M.E.; Langer, J.; Kinfe, M. Seizure detection watch improves quality of life for adolescents and their families. Epilepsy Behav. 2019, 98, 188–194. [Google Scholar] [CrossRef]
- Chiang, S.; Moss, R.; Patel, A.D.; Rao, V.R. Seizure detection devices and health-related quality of life: A patient-and caregiver-centered evaluation. Epilepsy Behav. 2020, 105, 106963. [Google Scholar] [CrossRef]
- Zhao, X.; Lhatoo, S.D. Seizure detection: Do current devices work? And when can they be useful? Curr. Neurol. Neurosci. Rep. 2018, 18, 1–19. [Google Scholar] [CrossRef]
- Pohlmann-Eden, B.; Newton, M. First seizure: EEG and neuroimaging following an epileptic seizure. Epilepsia 2008, 49, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Shellhaas, R.A. Continuous long-term electroencephalography: The gold standard for neonatal seizure diagnosis. In Seminars in Fetal and Neonatal Medicine; Elsevier: Piscataway, NJ, USA, 2015; Volume 20, pp. 149–153. [Google Scholar]
- Haider, H.A.; Esteller, R.; Hahn, C.D.; Westover, M.B.; Halford, J.J.; Lee, J.W.; Shafi, M.M.; Gaspard, N.; Herman, S.T.; Gerard, E.E.; et al. Sensitivity of quantitative EEG for seizure identification in the intensive care unit. Neurology 2016, 87, 935–944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shoeb, A.H.; Guttag, J.V. Application of machine learning to epileptic seizure detection. In Proceedings of the 27th International Conference on Machine Learning (ICML-10), Haifa, Israel, 21–24 June 2010; pp. 975–982. [Google Scholar]
- Shoeb, A.H. Application of Machine Learning to Epileptic Seizure Onset Detection and Treatment. Ph.D. Thesis, Massachusetts Institute of Technology, Cambridge, MA, USA, 2009. [Google Scholar]
- Athena, F.F.; West, M.P.; Hah, J.; Hanus, R.; Graham, S.; Vogel, E.M. Towards a better understanding of the forming and resistive switching behavior of Ti-doped HfOx RRAM. J. Mater. Chem. C 2022, 10, 5896–5904. [Google Scholar] [CrossRef]
- Gong, N.; Rasch, M.; Seo, S.C.; Gasasira, A.; Solomon, P.; Bragaglia, V.; Consiglio, S.; Higuchi, H.; Park, C.; Brew, K.; et al. Deep learning acceleration in 14 nm CMOS compatible ReRAM array: Device, material and algorithm co-optimization. In Proceedings of the IEEE International Electron Devices Meeting, San Francisco, CA, USA, 3–7 December 2022. [Google Scholar]
- Basnet, P.; Anderson, E.C.; Athena, F.F.; Chakrabarti, B.; West, M.P.; Vogel, E.M. Asymmetric Resistive Switching of Bilayer HfOx/AlOy and AlOy/HfOx Memristors: The Oxide Layer Characteristics and Performance Optimization for Digital Set and Analog Reset Switching. ACS Appl. Electron. Mater. 2023, 5, 1859–1865. [Google Scholar] [CrossRef]
- Hah, J.; West, M.P.; Athena, F.F.; Hanus, R.; Vogel, E.M.; Graham, S. Impact of oxygen concentration at the HfOx/Ti interface on the behavior of HfOx filamentary memristors. J. Mater. Sci. 2022, 57, 9299–9311. [Google Scholar] [CrossRef]
- Athena, F.F.; West, M.P.; Hah, J.; Graham, S.; Vogel, E.M. Trade-Off between Gradual Set and On/Off Ratio in HfOx-Based Analog Memory with a Thin SiOx Barrier Layer. ACS Appl. Electron. Mater. 2023, 5, 3048–3058. [Google Scholar] [CrossRef]
- Zhang, J.; Chatzichristos, C.; Vandecasteele, K.; Swinnen, L.; Broux, V.; Cleeren, E.; Van Paesschen, W.; De Vos, M. Automatic annotation correction for wearable EEG based epileptic seizure detection. J. Neural Eng. 2022, 19, 016038. [Google Scholar] [CrossRef]
- Brinkmann, B.H.; Karoly, P.J.; Nurse, E.S.; Dumanis, S.B.; Nasseri, M.; Viana, P.F.; Schulze-Bonhage, A.; Freestone, D.R.; Worrell, G.; Richardson, M.P.; et al. Seizure diaries and forecasting with wearables: Epilepsy monitoring outside the clinic. Front. Neurol. 2021, 12, 690404. [Google Scholar] [CrossRef]
- Gu, Y.; Cleeren, E.; Dan, J.; Claes, K.; Van Paesschen, W.; Van Huffel, S.; Hunyadi, B. Comparison between scalp EEG and behind-the-ear EEG for development of a wearable seizure detection system for patients with focal epilepsy. Sensors 2017, 18, 29. [Google Scholar] [CrossRef] [Green Version]
- Olokodana, I.L.; Mohanty, S.P.; Kougianos, E.; Sherratt, R.S. EZcap: A novel wearable for real-time automated seizure detection from EEG signals. IEEE Trans. Consum. Electron. 2021, 67, 166–175. [Google Scholar] [CrossRef]
- Thodoroff, P.; Pineau, J.; Lim, A. Learning robust features using deep learning for automatic seizure detection. In Proceedings of the 1st Machine Learning for Healthcare Conference, PMLR, Los Angeles, CA, USA, 19–20 August 2016; pp. 178–190. [Google Scholar]
- Yuan, Y.; Xun, G.; Jia, K.; Zhang, A. A multi-view deep learning framework for EEG seizure detection. IEEE J. Biomed. Health Inform. 2018, 23, 83–94. [Google Scholar] [CrossRef] [PubMed]
- Hossain, M.S.; Amin, S.U.; Alsulaiman, M.; Muhammad, G. Applying deep learning for epilepsy seizure detection and brain mapping visualization. ACM Trans. Multimed. Comput. Commun. Appl. (TOMM) 2019, 15, 1–17. [Google Scholar] [CrossRef]
- Gramacki, A.; Gramacki, J. A deep learning framework for epileptic seizure detection based on neonatal EEG signals. Sci. Rep. 2022, 12, 13010. [Google Scholar] [CrossRef] [PubMed]
- Cherian, R.; Kanaga, E.G. Theoretical and methodological analysis of EEG based seizure detection and prediction: An exhaustive review. J. Neurosci. Methods 2022, 369, 109483. [Google Scholar] [CrossRef]
- Al-Hussaini, I.; Xiao, C.; Westover, M.B.; Sun, J. SLEEPER: Interpretable Sleep staging via Prototypes from Expert Rules. In Proceedings of the Machine Learning for Healthcare Conference, PMLR, Ann Arbor, MI, USA, 9–10 August 2019; pp. 721–739. [Google Scholar]
- Kaushik, G.; Gaur, P.; Sharma, R.R.; Pachori, R.B. EEG signal based seizure detection focused on Hjorth parameters from tunable-Q wavelet sub-bands. Biomed. Signal Process. Control 2022, 76, 103645. [Google Scholar] [CrossRef]
- Shen, M.; Wen, P.; Song, B.; Li, Y. An EEG based real-time epilepsy seizure detection approach using discrete wavelet transform and machine learning methods. Biomed. Signal Process. Control 2022, 77, 103820. [Google Scholar] [CrossRef]
- Zhang, Y.; Yao, S.; Yang, R.; Liu, X.; Qiu, W.; Han, L.; Zhou, W.; Shang, W. Epileptic seizure detection based on bidirectional gated recurrent unit network. IEEE Trans. Neural Syst. Rehabil. Eng. 2022, 30, 135–145. [Google Scholar] [CrossRef]
- Doshi-Velez, F.; Kim, B. Considerations for evaluation and generalization in interpretable machine learning. In Explainable and Interpretable Models in Computer Vision and Machine Learning; Springer: Berlin/Heidelberg, Germany, 2018; pp. 3–17. [Google Scholar]
- Al-Hussaini, I.; Mitchell, C.S. SERF: Interpretable Sleep Staging using Embeddings, Rules, and Features. In Proceedings of the 31st ACM International Conference on Information & Knowledge Management, Atlanta, GA, USA, 17–21 October 2022; pp. 3791–3795. [Google Scholar]
- Hooker, S.; Erhan, D.; Kindermans, P.J.; Kim, B. A benchmark for interpretability methods in deep neural networks. Adv. Neural Inf. Process. Syst. 2019, 32, 9737–9748. [Google Scholar]
- Lipton, Z.C. The mythos of model interpretability: In machine learning, the concept of interpretability is both important and slippery. Queue 2018, 16, 31–57. [Google Scholar] [CrossRef]
- Al-Hussaini, I.; Mitchell, C.S. Performance and utility trade-off in interpretable sleep staging. In Proceedings of the NeurIPS 2022 Workshop on Learning from Time Series for Health, New Orleans, LA, USA, 2 December 2022. [Google Scholar]
- Van Der Donckt, J.; Van Der Donckt, J.; Deprost, E.; Vandenbussche, N.; Rademaker, M.; Vandewiele, G.; Van Hoecke, S. Do not sleep on traditional machine learning: Simple and interpretable techniques are competitive to deep learning for sleep scoring. Biomed. Signal Process. Control 2023, 81, 104429. [Google Scholar] [CrossRef]
- Schwabedal, J.T.; Snyder, J.C.; Cakmak, A.; Nemati, S.; Clifford, G.D. Addressing class imbalance in classification problems of noisy signals by using fourier transform surrogates. arXiv 2018, arXiv:1806.08675. [Google Scholar]
- Schirrmeister, R.T.; Springenberg, J.T.; Fiederer, L.D.J.; Glasstetter, M.; Eggensperger, K.; Tangermann, M.; Hutter, F.; Burgard, W.; Ball, T. Deep learning with convolutional neural networks for EEG decoding and visualization. Hum. Brain Mapp. 2017, 38, 5391–5420. [Google Scholar] [CrossRef] [Green Version]
- Dorogush, A.V.; Ershov, V.; Gulin, A. CatBoost: Gradient boosting with categorical features support. arXiv 2018, arXiv:1810.11363. [Google Scholar]
- Prokhorenkova, L.; Gusev, G.; Vorobev, A.; Dorogush, A.V.; Gulin, A. CatBoost: Unbiased boosting with categorical features. Adv. Neural Inf. Process. Syst. 2018, 31, 6639–6649. [Google Scholar]
- Roy, S.; Kiral-Kornek, I.; Harrer, S. ChronoNet: A deep recurrent neural network for abnormal EEG identification. In Artificial Intelligence in Medicine, Proceedings of the 17th Conference on Artificial Intelligence in Medicine, AIME 2019, Proceedings 17, Poznan, Poland, 26–29 June 2019; Springer: Berlin/Heidelberg, Germany, 2019; pp. 47–56. [Google Scholar]
- Al-Hussaini, I.; Mitchell, C.S. Towards Interpretable Seizure Detection Using Wearables. In Proceedings of the ICASSP 2023—2023 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP), Rhodes Island, Greece, 4–10 June 2023. [Google Scholar] [CrossRef]
- Chatzichristos, C.; Swinnen, L.; Macea, J.; Bhagubai, M.; Van Paesschen, W.; De Vos, M. Multimodal detection of typical absence seizures in home environment with wearable electrodes. Front. Signal Process. 2022, 2, 1014700. [Google Scholar] [CrossRef]
- Chatzichristos, C.; Claro Bhagubai, M.; Van Paesschen, W.; De Vos, M. SeizeIT1; KU Leuven RDR: Leuven, Belgium, 2023. [Google Scholar]
- Shah, V.; Golmohammadi, M.; Obeid, I.; Picone, J. Objective evaluation metrics for automatic classification of EEG events. In Biomedical Signal Processing: Innovation and Applications; Springer: Cham, Switzerland, 2021; pp. 223–255. [Google Scholar]
- Zhong, Z.; Zheng, L.; Kang, G.; Li, S.; Yang, Y. Random erasing data augmentation. In Proceedings of the AAAI Conference on Artificial Intelligence, New York, NY, USA, 7–12 February 2020; Volume 34, pp. 13001–13008. [Google Scholar]
- Xie, Q.; Dai, Z.; Hovy, E.; Luong, T.; Le, Q. Unsupervised data augmentation for consistency training. Adv. Neural Inf. Process. Syst. 2020, 33, 6256–6268. [Google Scholar]
- Cubuk, E.D.; Zoph, B.; Shlens, J.; Le, Q.V. Randaugment: Practical automated data augmentation with a reduced search space. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition Workshops, Seattle, WA, USA, 14–19 June 2020; pp. 702–703. [Google Scholar]
- Ross, C.L. Energy medicine: Current status and future perspectives. Glob. Adv. Health Med. 2019, 8, 2164956119831221. [Google Scholar] [CrossRef] [Green Version]
- Gramfort, A.; Luessi, M.; Larson, E.; Engemann, D.; Strohmeier, D.; Brodbeck, C.; Goj, R.; Jas, M.; Brooks, T.; Parkkonen, L.; et al. MEG and EEG data analysis with MNE-Python. Front. Neurosci. 2013, 7, 267. [Google Scholar] [CrossRef] [Green Version]
- Van Der Donckt, J.; Van Der Donckt, J.; Deprost, E.; Van Hoecke, S. tsflex: Flexible time series processing & feature extraction. SoftwareX 2021, 17, 100971. [Google Scholar]
- Virtanen, P.; Gommers, R.; Oliphant, T.E.; Haberland, M.; Reddy, T.; Cournapeau, D.; Burovski, E.; Peterson, P.; Weckesser, W.; Bright, J.; et al. SciPy 1.0: Fundamental Algorithms for Scientific Computing in Python. Nat. Methods 2020, 17, 261–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V.; et al. Scikit-learn: Machine Learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
- Paszke, A.; Gross, S.; Massa, F.; Lerer, A.; Bradbury, J.; Chanan, G.; Killeen, T.; Lin, Z.; Gimelshein, N.; Antiga, L.; et al. Pytorch: An imperative style, high-performance deep learning library. Adv. Neural Inf. Process. Syst. 2019, 32, 8026–8037. [Google Scholar]
- Abadi, M.; Agarwal, A.; Barham, P.; Brevdo, E.; Chen, Z.; Citro, C.; Corrado, G.S.; Davis, A.; Dean, J.; Devin, M.; et al. TensorFlow: Large-Scale Machine Learning on Heterogeneous Systems. 2015. Available online: www.tensorflow.org (accessed on 30 July 2023).
- Panchavati, S.; Dussen, S.V.; Semwal, H.; Ali, A.; Chen, J.; Li, H.; Arnold, C.; Speier, W. Pretrained Transformers for Seizure Detection. In Proceedings of the ICASSP 2023—2023 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP), Rhodes Island, Greece, 4–10 June 2023. [Google Scholar] [CrossRef]
- Shah, V.; Von Weltin, E.; Lopez, S.; McHugh, J.R.; Veloso, L.; Golmohammadi, M.; Obeid, I.; Picone, J. The temple university hospital seizure detection corpus. Front. Neuroinform. 2018, 12, 83. [Google Scholar] [CrossRef] [PubMed]
- Huang, B.; Abtahi, A.; Aminifar, A. Lightweight Machine Learning for Seizure Detection on Wearable Devices. In Proceedings of the ICASSP 2023—2023 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP), Rhodes Island, Greece, 4–10 June 2023. [Google Scholar] [CrossRef]
- Shovkun, A.; Kiryasov, A.; Zakharov, I.; Khayretdinova, M. Optimization of the Deep Neural Networks for Seizure Detection. In Proceedings of the ICASSP 2023—2023 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP), Rhodes Island, Greece, 4–10 June 2023. [Google Scholar] [CrossRef]
- Lundberg, S.M.; Lee, S.I. A unified approach to interpreting model predictions. Adv. Neural Inf. Process. Syst. 2017, 30, 4768–4777. [Google Scholar]
- Marchal, R.; Rheims, S. Assessing epilepsy-related autonomic manifestations: Beyond cardiac and respiratory investigations. Neurophysiol. Clin. 2023, 53, 102850. [Google Scholar] [CrossRef]
- Bedeeuzzaman, M.; Farooq, O.; Khan, Y.U. Automatic seizure detection using inter quartile range. Int. J. Comput. Appl. 2012, 44, 1–5. [Google Scholar] [CrossRef]
- Greene, B.R.; Faul, S.; Marnane, W.; Lightbody, G.; Korotchikova, I.; Boylan, G.B. A comparison of quantitative EEG features for neonatal seizure detection. Clin. Neurophysiol. 2008, 119, 1248–1261. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Hussaini, I.; Mitchell, C.S. SeizFt: Interpretable Machine Learning for Seizure Detection Using Wearables. Bioengineering 2023, 10, 918. https://doi.org/10.3390/bioengineering10080918
Al-Hussaini I, Mitchell CS. SeizFt: Interpretable Machine Learning for Seizure Detection Using Wearables. Bioengineering. 2023; 10(8):918. https://doi.org/10.3390/bioengineering10080918
Chicago/Turabian StyleAl-Hussaini, Irfan, and Cassie S. Mitchell. 2023. "SeizFt: Interpretable Machine Learning for Seizure Detection Using Wearables" Bioengineering 10, no. 8: 918. https://doi.org/10.3390/bioengineering10080918