
A Proposal for the Classification of Temporomandibular Joint Disc Deformity in Hemifacial Microsomia
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. CT, 3D Reconstruction, and MRI
2.3. Statistical Analysis
3. Results
3.1. Classification of the OMENS+C
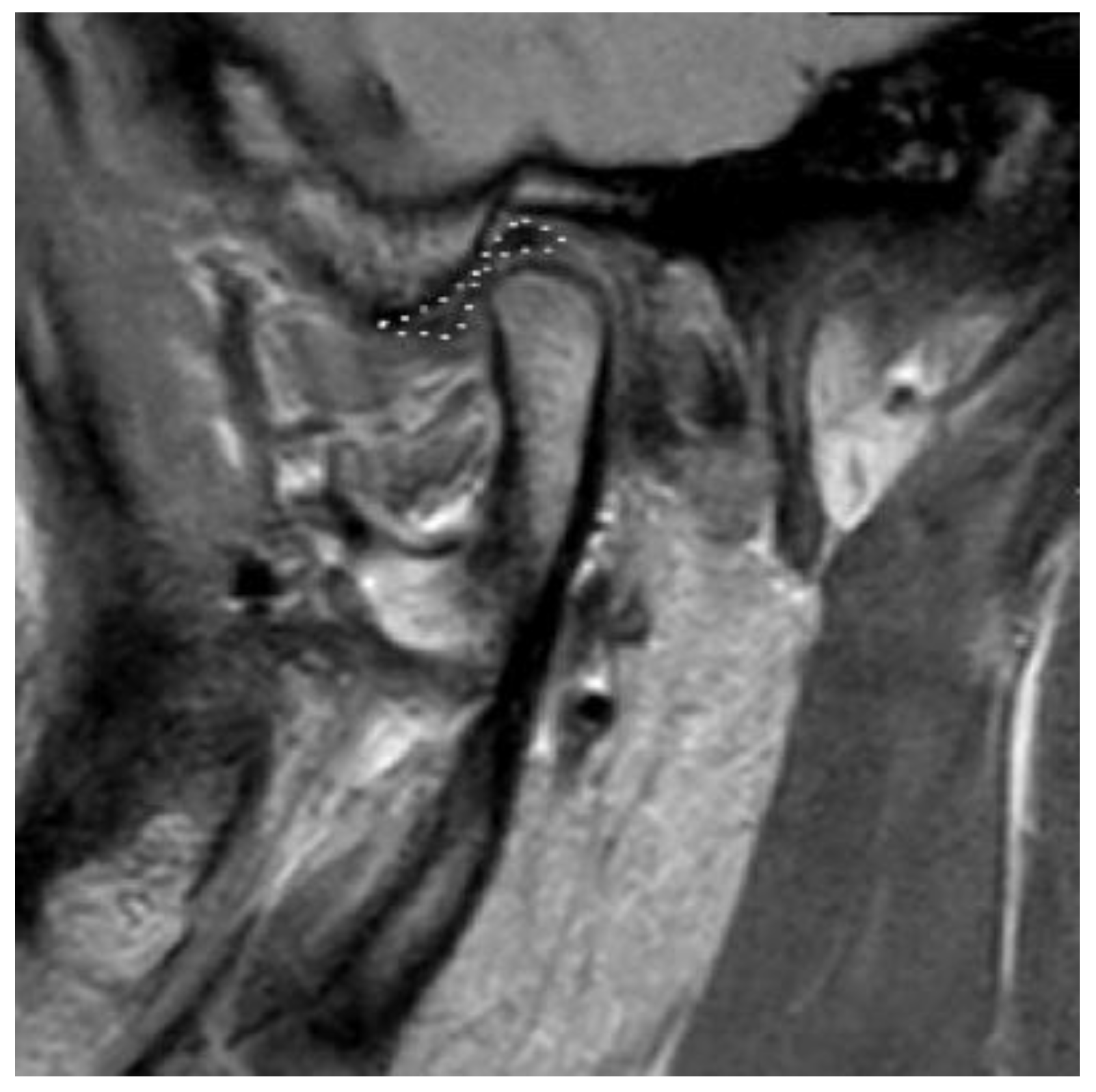
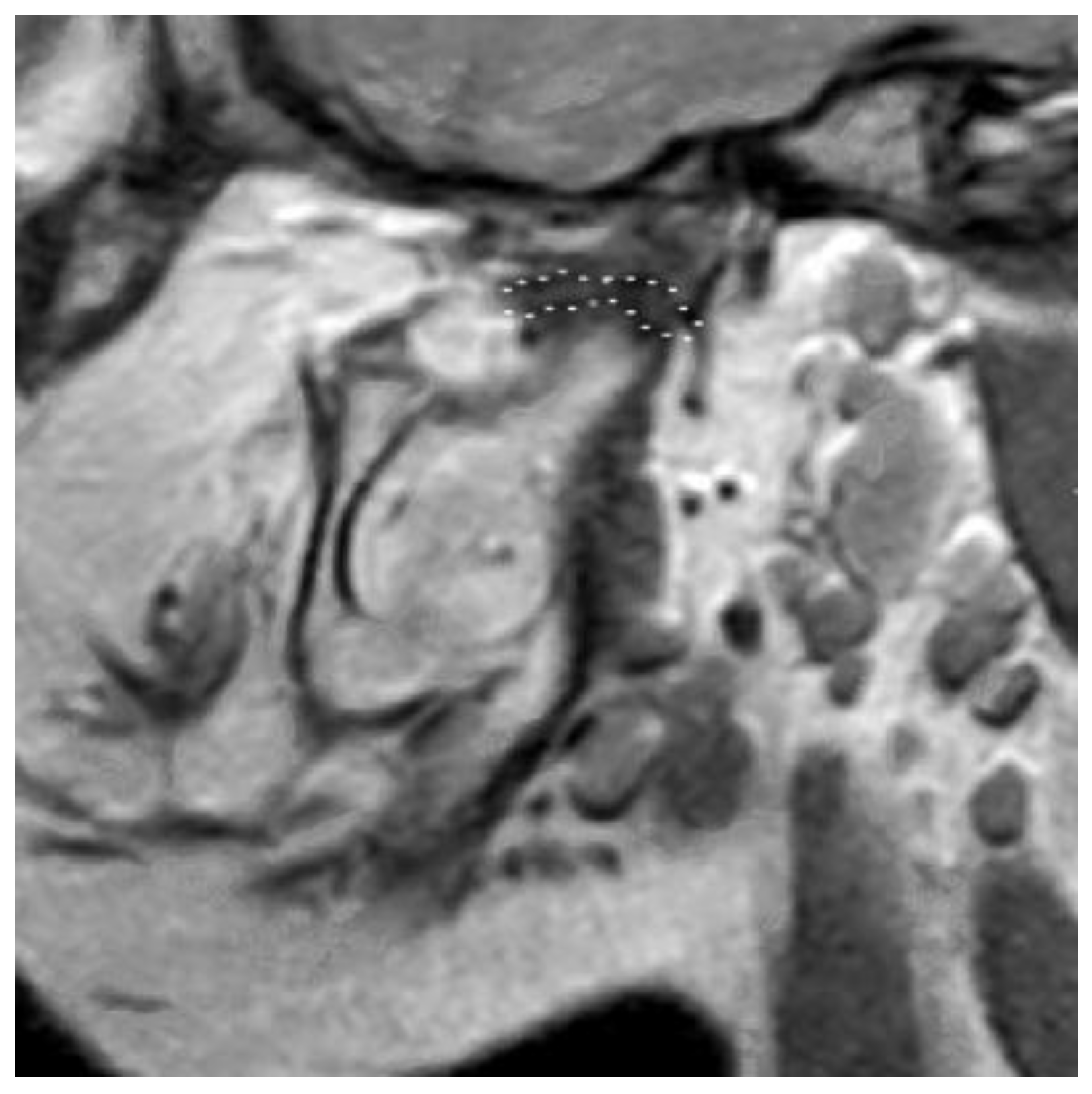
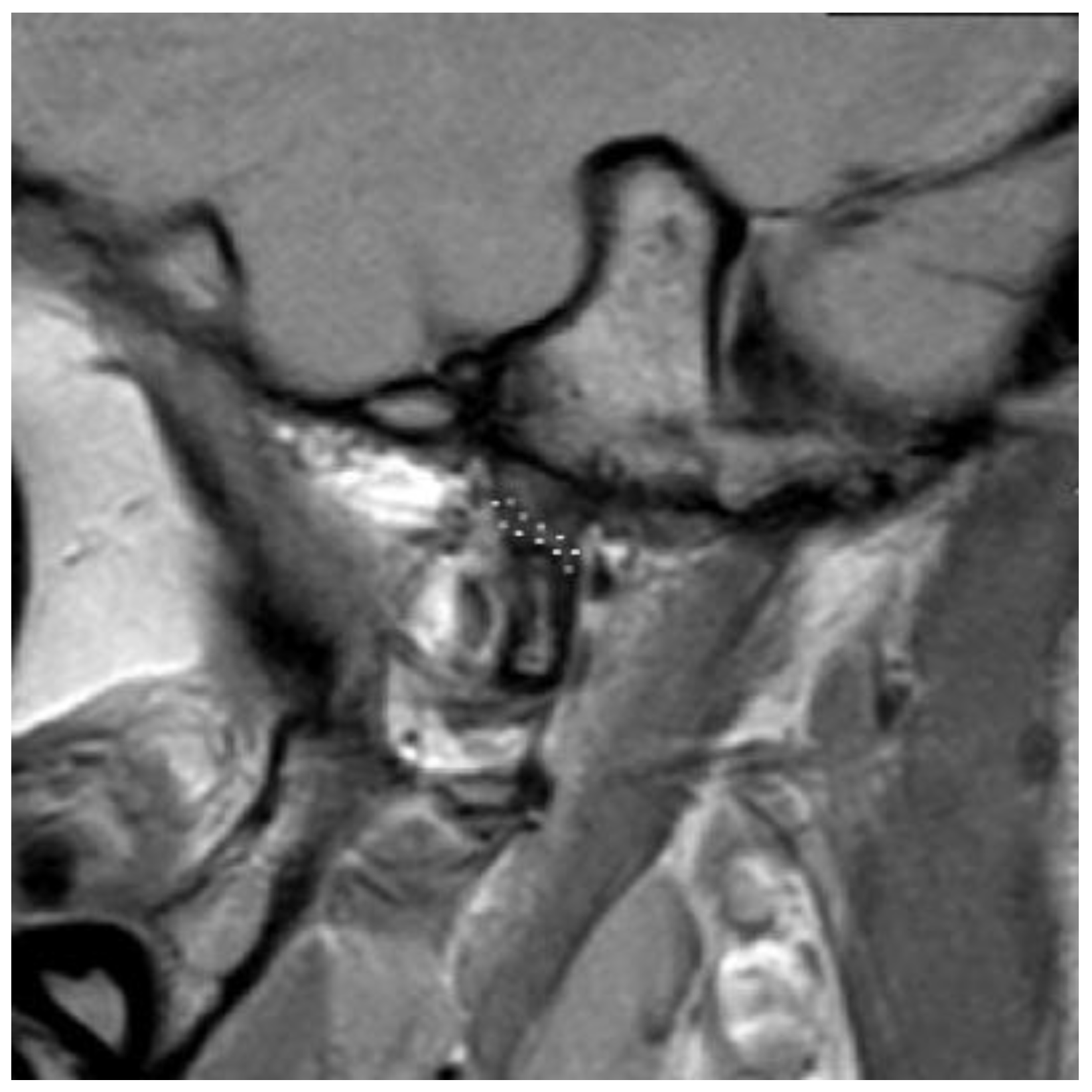
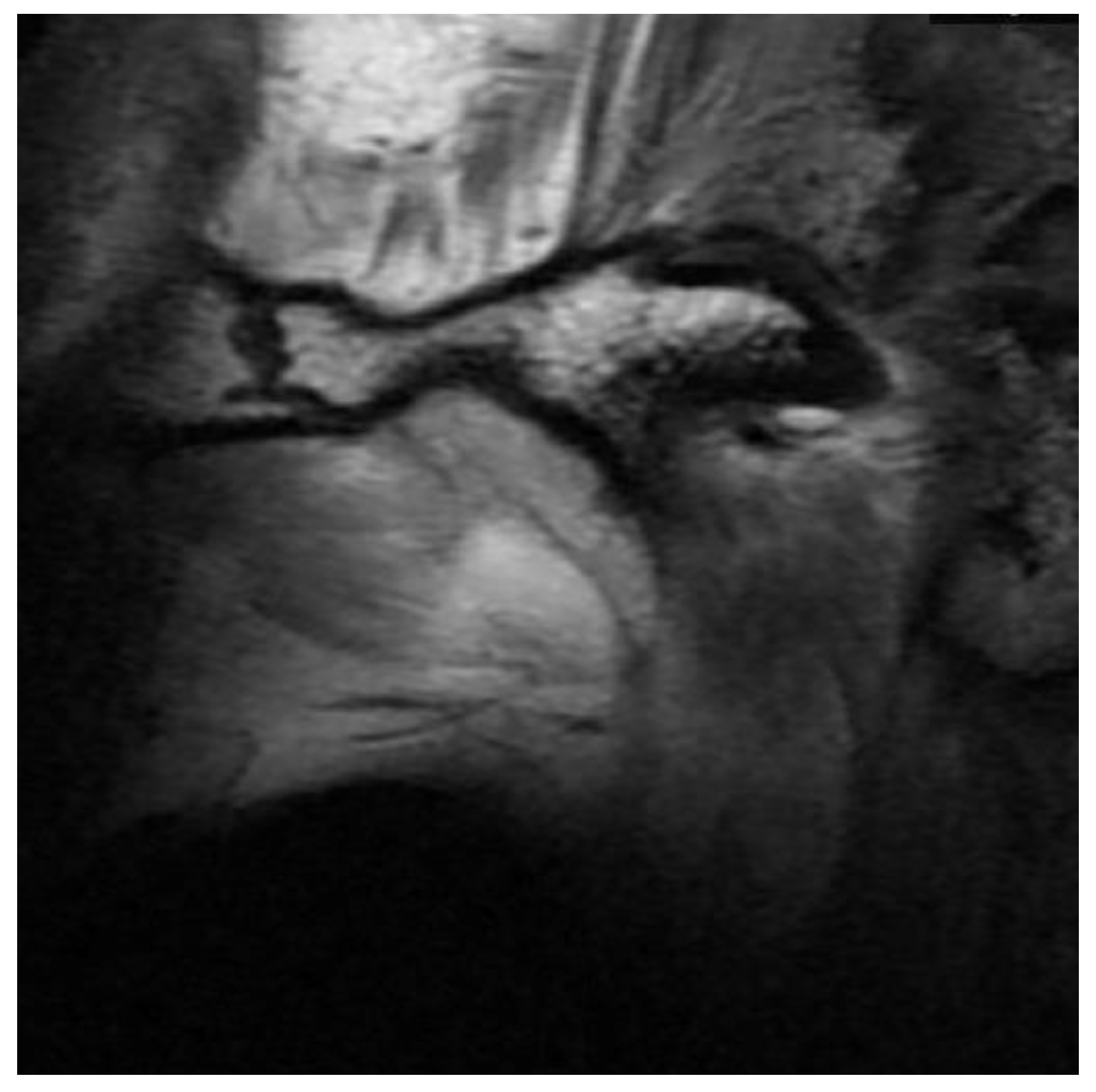
3.2. Definition of Disc Classification
3.3. Sample Distribution
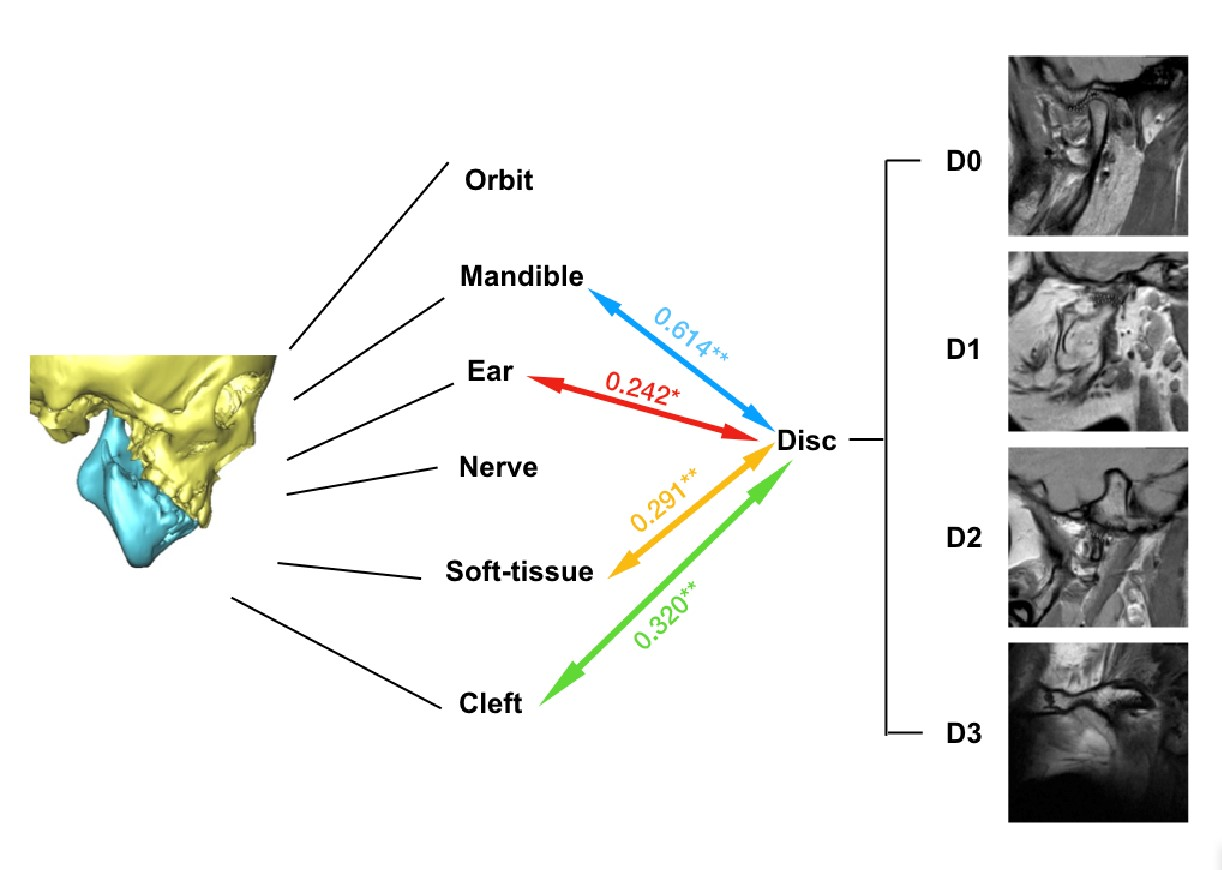
3.4. Correlation between OMENS+C and Disc Classifications
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gougoutas, A.J.; Singh, D.J.; Low, D.W.; Bartlett, S.P. Hemifacial Microsomia: Clinical Features and Pictographic Representations of the OMENS Classification System. Plast. Reconstr. Surg. 2007, 120, 112e–120e. [Google Scholar] [CrossRef] [PubMed]
- Hartsfield, J.K. Review of the etiologic heterogeneity of the oculo-auriculo-vertebral spectrum (Hemifacial Microsomia). Orthod. Craniofac. Res. 2007, 10, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Tuin, A.J.; Tahiri, Y.; Paine, K.M.; Paliga, J.T.; Taylor, J.A.; Bartlett, S.P. Clarifying the Relationships among the Different Features of the OMENS+ Classification in Craniofacial Microsomia. Plast. Reconstr. Surg. 2015, 135, 149e–156e. [Google Scholar] [CrossRef] [PubMed]
- Bogusiak, K.; Puch, A.; Arkuszewski, P. Goldenhar syndrome: Current perspectives. World J. Pediatr. 2017, 13, 405–415. [Google Scholar] [CrossRef]
- Horgan, J.E.; Padwa, B.L.; Labrie, R.A.; Mulliken, J.B. OMENS-Plus: Analysis of Craniofacial and Extracraniofacial Anomalies in Hemifacial Microsomia. Cleft Palate-Craniofac. J. 1995, 32, 405–412. [Google Scholar] [CrossRef]
- Pierpont, M.E.M.; Moller, J.H.; Gorlin, R.J.; Edwards, J.E. Congenital cardiac, pulmonary, and vascular malformations in oculoauriculovertebral dysplasia. Pediatr. Cardiol. 1982, 2, 297–302. [Google Scholar] [CrossRef]
- David, D.J.; Mahatumarat, C.; Cooter, R.D. Hemifacial microsomia—A multisystem classification. Plast. Reconstr. Surg. 1987, 80, 525–535. [Google Scholar] [CrossRef]
- Rollnick, B.R.; Kaye, C.I.; Nagatoshi, K.; Hauck, W.; Martin, A.O.; Reynolds, J.F. Oculoauriculovertebral dysplasia and variants: Phenotypic characteristics of 294 patients. Am. J. Med Genet. 1987, 26, 361–375. [Google Scholar] [CrossRef]
- Birgfeld, C.; Heike, C. Craniofacial Microsomia. Clin. Plast. Surg. 2019, 46, 207–221. [Google Scholar] [CrossRef]
- Pruzansky, S. Not all dwarfed mandibles are alike. Birth Defects 1969, 1, 120–129. [Google Scholar]
- Kaban, L.B.; Moses, M.H.; Mulliken, J.B. Surgical correction of hemifacial microsomia in the growing child. Plast. Reconstr. Surg. 1988, 82, 9–19. [Google Scholar] [CrossRef]
- Lauritzen, C.; Munro, I.R.; Ross, R.B. Classification and treatment of hemifacial microsomia. Scand. J. Plast. Reconstr. Surg. 1985, 19, 33–39. [Google Scholar] [CrossRef]
- Meurman, Y. Congenital Microtia and Meatal Atresia: Observations and Aspects of Treatment. AMA Arch. Otolaryngol. Neck Surg. 1957, 66, 443–463. [Google Scholar] [CrossRef]
- Murray, J.E.; Kaban, L.B.; Mulliken, J.B. Analysis and Treatment of Hemifacial Microsomia. Plast. Reconstr. Surg. 1984, 74, 186–199. [Google Scholar] [CrossRef]
- Vento, A.R.; LaBrie, R.A.; Mulliken, J.B. The O.M.E.N.S. classification of hemifacial microsomia. Cleft Palate Craniofac. J. 1991, 28, 68–76. [Google Scholar] [CrossRef]
- Birgfeld, C.B.; Heike, C. Craniofacial microsomia. Semin. Plast. Surg. 2012, 26, 91–104. [Google Scholar] [CrossRef]
- Brandstetter, K.A.; Patel, K.G. Craniofacial Microsomia. Facial. Plast. Surg. Clin. N. Am. 2016, 24, 495–515. [Google Scholar] [CrossRef]
- Nebbe, B.; Major, P.W.; Prasad, N.G.N.; Hatcher, D. Quantitative assessment of temporomandibular joint disk status. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1998, 85, 598–607. [Google Scholar] [CrossRef]
- Xie, Q.; Yang, C.; He, D.; Cai, X.; Ma, Z. Is mandibular asymmetry more frequent and severe with unilateral disc displacement? J. Craniomaxillofac. Surg. 2015, 43, 81–86. [Google Scholar] [CrossRef]
- Sun, H.; Zhang, J.; Li, B.; Liu, Z.; Shen, S.; Wang, X. Accuracy of a new custom-made bone-supported osteotomy and repositioning guide system for reconstruction of the mandibular ramus using costochondral grafts: A preliminary study. Br. J. Oral Maxillofac. Surg. 2020, 58, 51–56. [Google Scholar] [CrossRef]
- Li, B.; Sun, H.; Zeng, F.; Zhang, T.; Wang, X. Accuracy of a CAD/CAM surgical template for mandibular distraction: A preliminary study. Br. J. Oral Maxillofac. Surg. 2018, 56, 814–819. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.K.; Yang, C.; Xie, Q.Y. Changes in disc status in the reducing and nonreducing anterior disc displacement of temporomandibular joint: A longitudinal retrospective study. Sci. Rep. 2016, 6, 34253. [Google Scholar] [CrossRef] [PubMed]
- Kitai, N.; Murakami, S.; Takashima, M.; Furukawa, S.; Kreiborg, S.; Takada, K. Evaluation of Temporomandibular Joint in Patients With Hemifacial Microsomia. Cleft Palate Craniofac. J. 2004, 41, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Al-Moraissi, E.A.; Wolford, L.M. Does Temporomandibular Joint Pathology with or without Surgical Management Affect the Stability of Counterclockwise Rotation of the Maxillomandibular Complex in Orthognathic Surgery? A Systematic Review and Meta-Analysis. J. Oral Maxillofac. Surg. 2017, 75, 805–821. [Google Scholar] [CrossRef]
- Goncalves, J.R.; Cassano, D.S.; Wolford, L.M.; Santos-Pinto, A.; Marquez, I.M. Postsurgical stability of counterclockwise maxillomandibular advancement surgery: Affect of articular disc repositioning. J. Oral Maxillofac. Surg. 2008, 66, 724–738. [Google Scholar] [CrossRef]
- Wan, J.; Meara, J.G.; Kovanlikaya, A.; Nelson, M.D.; Don, D. Clinical, Radiological, and Audiological Relationships in Hemifacial Microsomia. Ann. Plast. Surg. 2003, 51, 161–166. [Google Scholar] [CrossRef]
- Park, J.U.; Do, T.H.; Kwon, G.Y.; Choi, T.H.; Kim, S. Statistical analysis using the OMENS classification in Oriental patients with hemifacial microsomia: A comparative analysis with Western centers. Ann. Plast. Surg. 2014, 72, 50–55. [Google Scholar] [CrossRef]
- Gillies, H.D. Plastic surgery of the face. Lancet 1920, 196, 177–192. [Google Scholar] [CrossRef]
- Klein, C.; Howaldt, H.-P. Correction of Mandibular Hypoplasia by Means of Bidirectional Callus Distraction. J. Craniofac. Surg. 1996, 7, 258–266. [Google Scholar] [CrossRef]
- McCarthy, J.G.; Stelnicki, E.J.; Mehrara, B.J.; Longaker, M.T. Distraction Osteogenesis of the Craniofacial Skeleton. Plast. Reconstr. Surg. 2001, 107, 1812–1824. [Google Scholar] [CrossRef]
- Mommaerts, M.Y.; Nagy, K. Is early osteodistraction a solution for the ascending ramus compartment in hemifacial microsomia? A literature study. J. Cranio-Maxillofac. Surg. 2002, 30, 201–207. [Google Scholar] [CrossRef]
- Wang, P.; Wang, Y.; Zhang, Z.; Li, X.; Ye, B.; Li, J. Comprehensive consideration and design with the virtual surgical planning-assisted treatment for hemifacial microsomia in adult patients. J. Cranio-Maxillofacial Surg. 2018, 46, 1268–1274. [Google Scholar] [CrossRef]
- Chen, Q.; Zhao, Y.; Shen, G.; Dai, J. Etiology and Pathogenesis of Hemifacial Microsomia. J. Dent. Res. 2018, 97, 1297–1305. [Google Scholar] [CrossRef]
- Zielinski, D.; Markus, B.; Sheikh, M.; Gymrek, M.; Chu, C.; Zaks, M.; Srinivasan, B.; Hoffman, J.D.; Aizenbud, D.; Erlich, Y. OTX2 Duplication Is Implicated in Hemifacial Microsomia. PLoS ONE 2014, 9, e96788. [Google Scholar] [CrossRef]
- Digilio, M.C.; McDonald-McGinn, D.M.; Heike, C.; Catania, C.; Dallapiccola, B.; Marino, B.; Zackai, E.H. Three patients with oculo-auriculo-vertebral spectrum and microdeletion 22q11.2. Am. J. Med Genet. Part A 2009, 149A, 2860–2864. [Google Scholar] [CrossRef]
- Xu, J.; Fan, Y.S.; Siu, V.M. A child with features of Goldenhar syndrome and a novel 1.12 Mb deletion in 22q11.2 by cytogenetics and oligonucleotide array CGH: Is this a candidate region for the syndrome? Am. J. Med. Genet. A 2008, 146A, 1886–1889. [Google Scholar] [CrossRef]
- Tan, T.Y.; Collins, A.; James, P.; McGillivray, G.; Stark, Z.; Gordon, C.T.; Leventer, R.J.; Pope, K.; Forbes, R.; Crolla, J.A.; et al. Phenotypic variability of distal 22q11.2 copy number abnormalities. Am. J. Med Genet. Part A 2011, 155, 1623–1633. [Google Scholar] [CrossRef]
- Timberlake, A.T.; Griffin, C.; Heike, C.L.; Hing, A.V.; Cunningham, M.L.; Chitayat, D.; Davis, M.R.; Doust, S.J.; Drake, A.F.; Duenas-Roque, M.M.; et al. Haploinsufficiency of SF3B2 causes craniofacial microsomia. Nat. Commun. 2021, 12, 4680. [Google Scholar] [CrossRef]
- Wang, Y.; Ping, L.; Luan, X.; Chen, Y.; Fan, X.; Li, L.; Liu, Y.; Wang, P.; Zhang, S.; Zhang, B.; et al. A Mutation in VWA1, Encoding von Willebrand Factor A Domain-Containing Protein 1, Is Associated with Hemifacial Microsomia. Front. Cell Dev. Biol. 2020, 8, 571004. [Google Scholar] [CrossRef]
- Su, P.-H.; Liu, Y.-F.; Yu, J.-S.; Chen, J.-Y.; Chen, S.-J.; Lai, Y.-J. Facial asymmetry and clinical manifestations in patients with novel insertion of theTCOF1gene. Clin. Genet. 2012, 82, 460–465. [Google Scholar] [CrossRef]
- Naora, H.; Kimura, M.; Otani, H.; Yokoyama, M.; Koizumi, T.; Katsuki, M.; Tanaka, O. Transgenic Mouse Model of Hemifacial Microsomia: Cloning and Characterization of Insertional Mutation Region on Chromosome 10. Genomics 1994, 23, 515–519. [Google Scholar] [CrossRef] [PubMed]
- Cousley, R.; Naora, H.; Yokoyama, M.; Kimura, M.; Otani, H. Validity of theHfmTransgenic Mouse as a Model for Hemifacial Microsomia. Cleft Palate-Craniofac. J. 2002, 39, 81–92. [Google Scholar] [CrossRef] [PubMed]
- Gendron-Maguire, M.; Mallo, M.; Zhang, M.; Gridley, T. Hoxa-2 mutant mice exhibit homeotic transformation of skeletal elements derived from cranial neural crest. Cell 1993, 75, 1317–1331. [Google Scholar] [CrossRef]
- Santagati, F.; Minoux, M.; Ren, S.-Y.; Rijli, F.M. Temporal requirement of Hoxa2 in cranial neural crest skeletal morphogenesis. Development 2005, 132, 4927–4936. [Google Scholar] [CrossRef] [PubMed]
- Quiat, D.; Timberlake, A.T.; Curran, J.J.; Cunningham, M.L.; McDonough, B.; Artunduaga, M.A.; DePalma, S.R.; Duenas-Roque, M.M.; Gorham, J.M.; Gustafson, J.A.; et al. Damaging variants in FOXI3 cause microtia and craniofacial microsomia. Genet Med. 2023, 25, 143–150. [Google Scholar] [CrossRef]
- Luquetti, D.V.; Heike, C.L.; Zarante, I.; Timms, A.E.; Gustafson, J.; Pachajoa, H.; Porras-Hurtado, G.L.; Ayala-Ramirez, P.; Duenas-Roque, M.M.; Jimenez, N.; et al. MYT1 role in the microtia-craniofacial microsomia spectrum. Mol. Genet. Genomic Med. 2020, 8, e1401. [Google Scholar] [CrossRef]
- Poswillo, D. The pathogenesis of the first and second branchial arch syndrome. Oral Surg. Oral Med. Oral Pathol. 1973, 35, 302–328. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| O (Orbit) | |
| O0 | normal orbital size and position |
| O1 | abnormal orbital size |
| O2↓ | inferior orbital displacement |
| O2↑ | superior orbital displacement |
| O3 | abnormal orbital size and position |
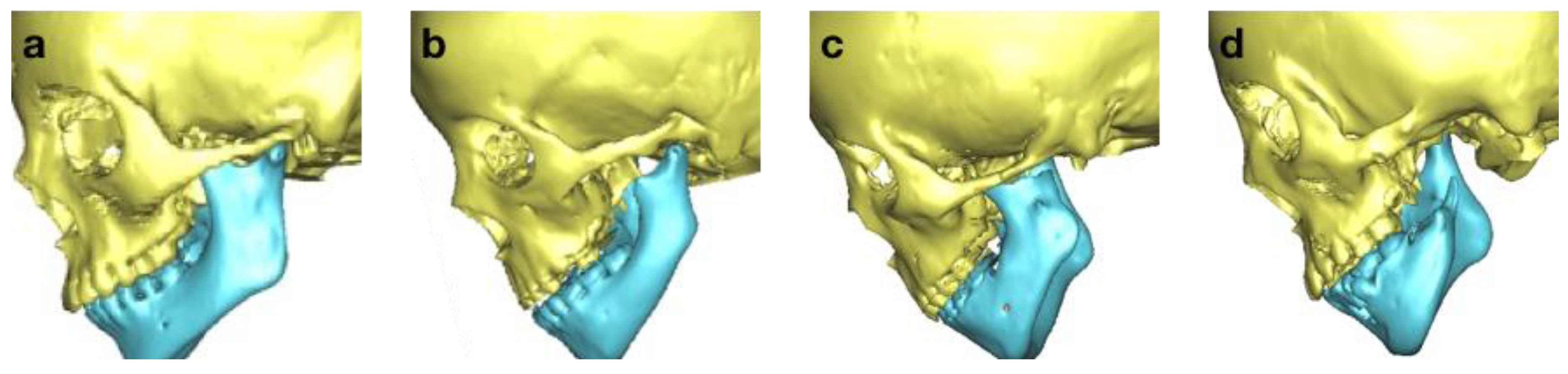
| M (Mandible) | |
| M0 | normal mandible |
| M1 | small mandible and glenoid fossa with short ramus |
| M2a | abnormally shaped and short ramus (glenoid fossa in acceptable position) |
| M2b | abnormally shaped and short ramus (glenoid fossa is inferiorly, medially, and anteriorly displaced with severe hypoplasia of condyle) |
| M3 | absence of ramus and glenoid fossa |
| E (Ear) | |
| E0 | normal auricle |
| E1 | mild hypoplasia and cupping with presence of all structures |
| E2 | absence of external canal with variable hypoplasia of concha |
| E3 | malpositioned lobule with absent auricle; lobular remnant typically inferiorly and anteriorly displaced |
| N (Nerve) | |
| N0 | no facial nerve involvement |
| N1 | temporal and/or zygomatic branch involvement |
| N2 | buccal and/or mandibular and/or cervical branch involvement |
| N3 | all branches affected |
| S (Soft tissue) | |
| S0 | no soft tissue deficiency |
| S1 | minimal soft tissue deficiency |
| S2 | moderate soft tissue deficiency (between S1 and S3) |
| S3 | severe soft tissue deficiency |
| C (Macrostomia/Cleft) | |
| C0 | no cleft |
| C1 | cleft terminates medially to anterior border of masseter |
| C2 | cleft terminates laterally to anterior border of masseter |
| Orbit | n | % |
|---|---|---|
| O0 | 35 | 32.4% |
| O1 | 24 | 22.2% |
| O2 | 33 | 30.6% |
| O3 | 16 | 14.8% |
| Total | 108 | |
| Mandible | n | % |
| M1 | 15 | 13.9% |
| M2a | 35 | 32.4% |
| M2b | 45 | 41.7% |
| M3 | 13 | 12.0% |
| Total | 108 | |
| Ear | n | % |
| E0 | 36 | 33.3% |
| E1 | 12 | 11.1% |
| E2 | 27 | 25.0% |
| E3 | 33 | 30.6% |
| Total | 108 | |
| Nerve | n | % |
| N0 | 84 | 77.8% |
| N1 | 10 | 9.3% |
| N2 | 11 | 10.2% |
| N3 | 3 | 2.8% |
| Total | 108 | |
| Soft tissue | n | % |
| S0 | 30 | 27.8% |
| S1 | 41 | 38.0% |
| S2 | 31 | 28.7% |
| S3 | 6 | 5.6% |
| Total | 108 | |
| Cleft | n | % |
| C0 | 78 | 72.2% |
| C1 | 21 | 19.4% |
| C2 | 9 | 8.3% |
| Total | 108 | |
| Disc | n | % |
| D0 | 31 | 28.7% |
| D1 | 17 | 15.7% |
| D2 | 36 | 33.3% |
| D3 | 24 | 22.2% |
| Total | 108 |
| Disc | Orbit | Mandible | Ear | Nerve | Soft Tissue | |
|---|---|---|---|---|---|---|
| Orbit | −0.016 | |||||
| Mandible | 0.614 ** | 0.099 | ||||
| Ear | 0.242 * | 0.122 | 0.137 | |||
| Nerve | −0.056 | 0.106 | −0.025 | 0.234 | ||
| Soft tissue | 0.291 ** | 0.245 * | 0.332 ** | 0.340 ** | 0.166 | |
| Cleft | 0.320 ** | −0.012 | 0.332 ** | −0.032 | 0.036 | 0.13 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xue, X.; Liu, Z.; Wei, H.; Wang, X. A Proposal for the Classification of Temporomandibular Joint Disc Deformity in Hemifacial Microsomia. Bioengineering 2023, 10, 595. https://doi.org/10.3390/bioengineering10050595
Xue X, Liu Z, Wei H, Wang X. A Proposal for the Classification of Temporomandibular Joint Disc Deformity in Hemifacial Microsomia. Bioengineering. 2023; 10(5):595. https://doi.org/10.3390/bioengineering10050595
Chicago/Turabian StyleXue, Xiaochen, Zhixu Liu, Hongpu Wei, and Xudong Wang. 2023. "A Proposal for the Classification of Temporomandibular Joint Disc Deformity in Hemifacial Microsomia" Bioengineering 10, no. 5: 595. https://doi.org/10.3390/bioengineering10050595