
Long-Term Culture Performance of a Polyelectrolyte Complex Microcapsule Platform for Hyaline Cartilage Repair

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
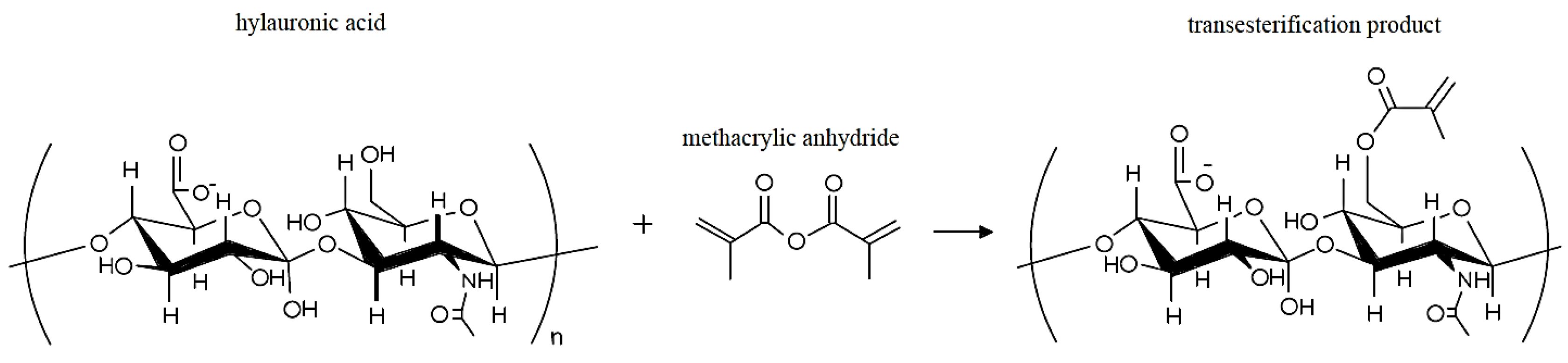
2.1. Modification of Hyaluronic Acid with Methacrylic Anhydride
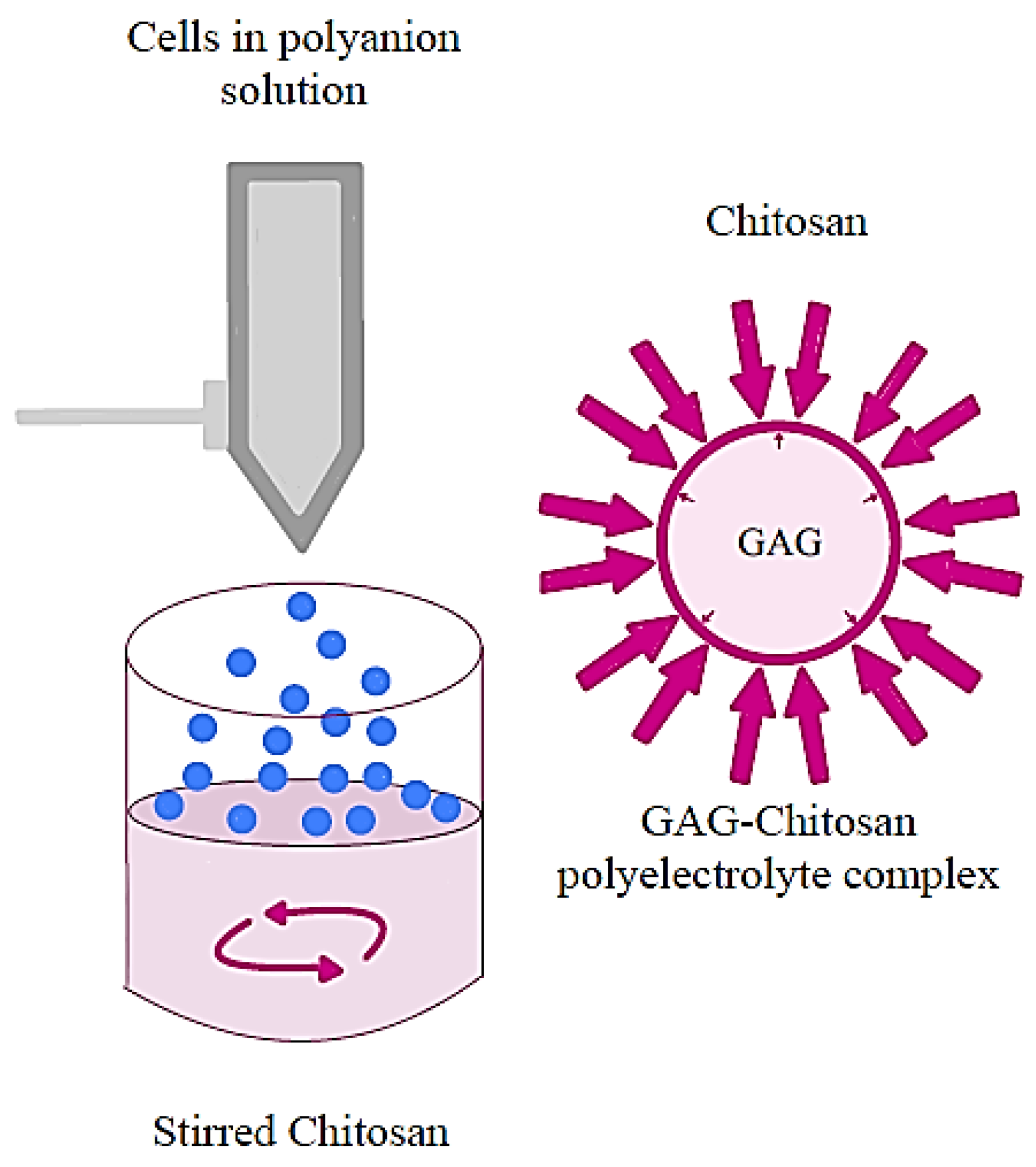
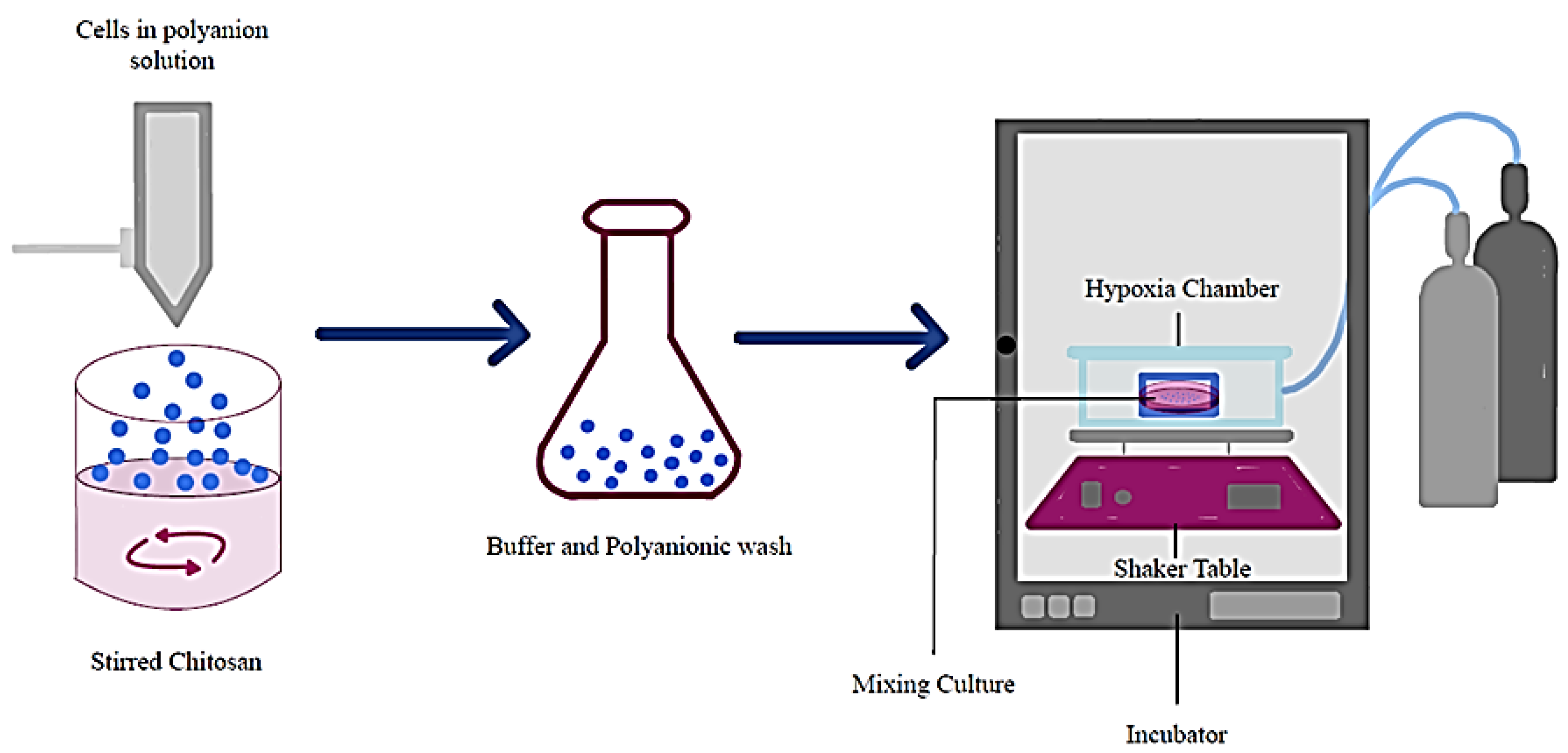
2.2. Formation of Polyelectrolyte Complex Microcapsules
2.3. Assessing Mass Transport in Polyelectrolyte Complex Microcapsules
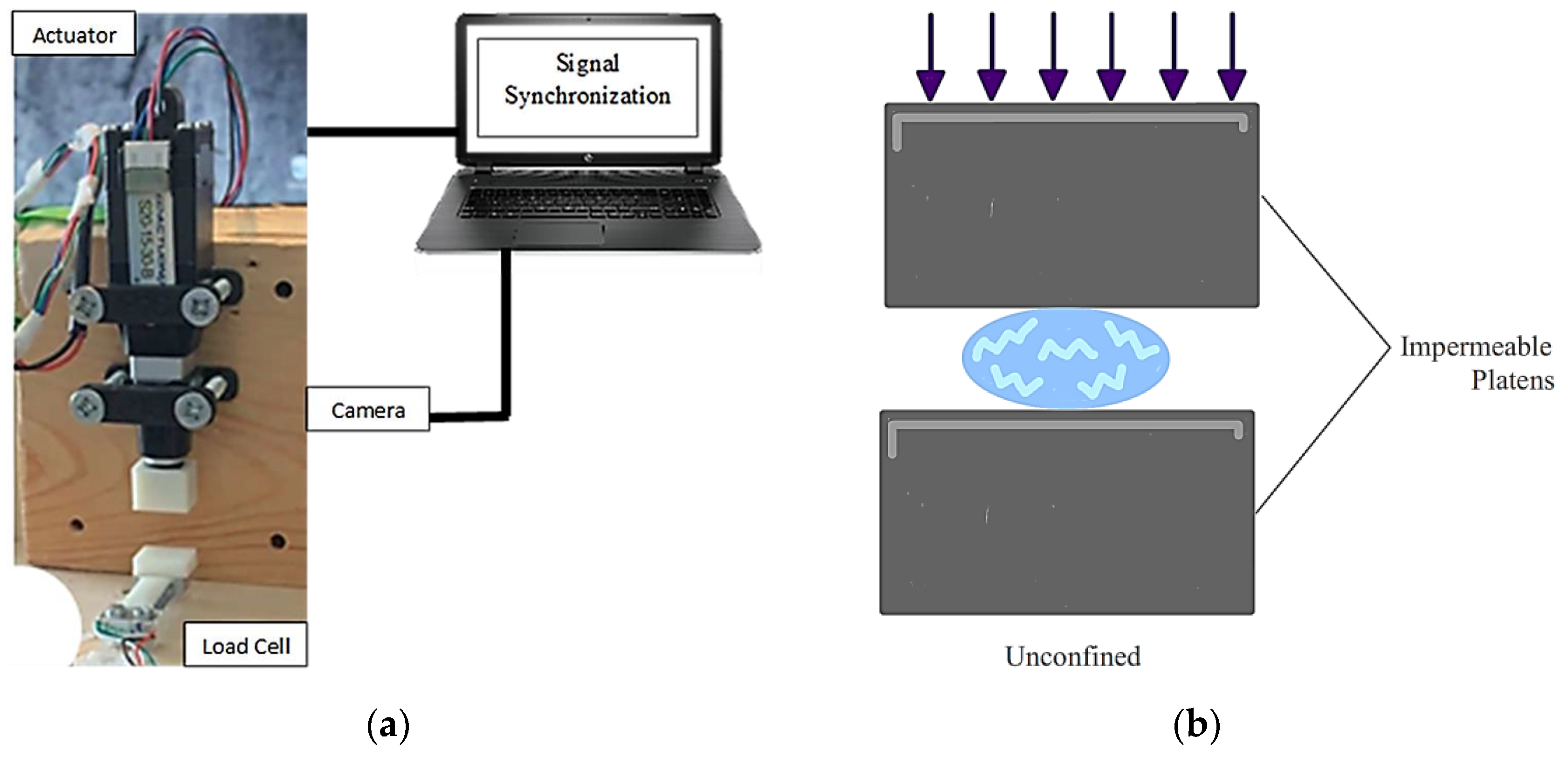
2.4. Assessing Capsule Rupture Strength
2.5. Isolation and Culture of Chondrocytes and bMSCs
2.6. 28-Day Encapsulated Culture of Chondrocytes and bMSC
2.7. Assessing the Effect of the PECM Culture on Chondrocytes and bMSCs
2.8. 90-Day Encapsulated Cell Cultures
2.9. Assessing the 90-Day 3-Cell Condition Encapsulation Culture
3. Results
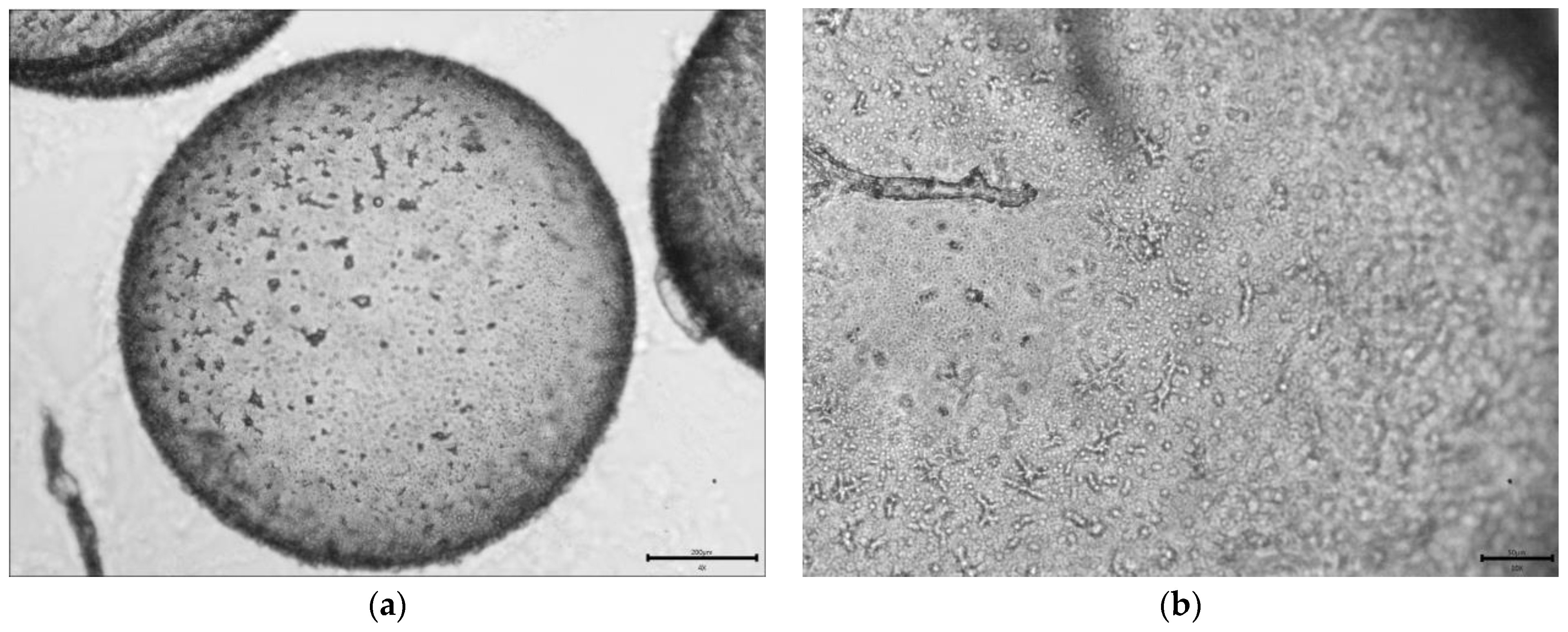
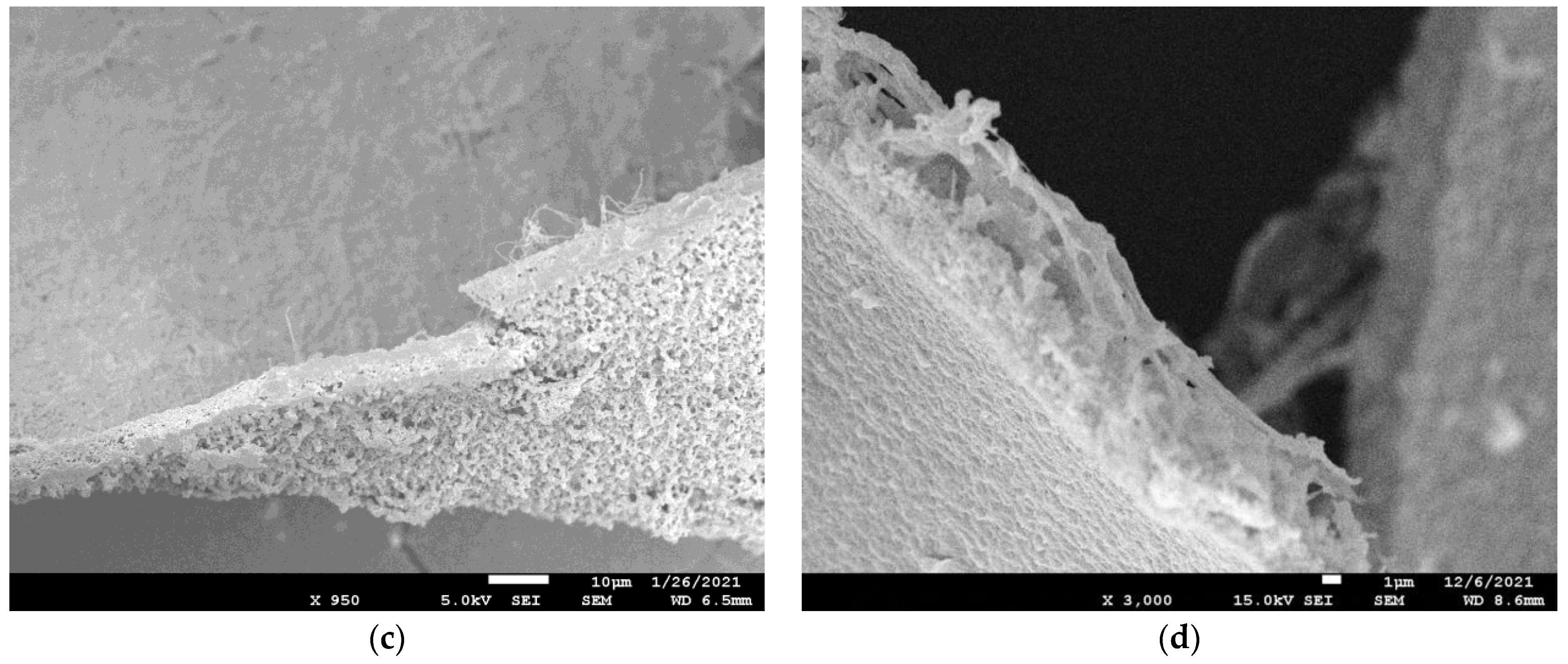
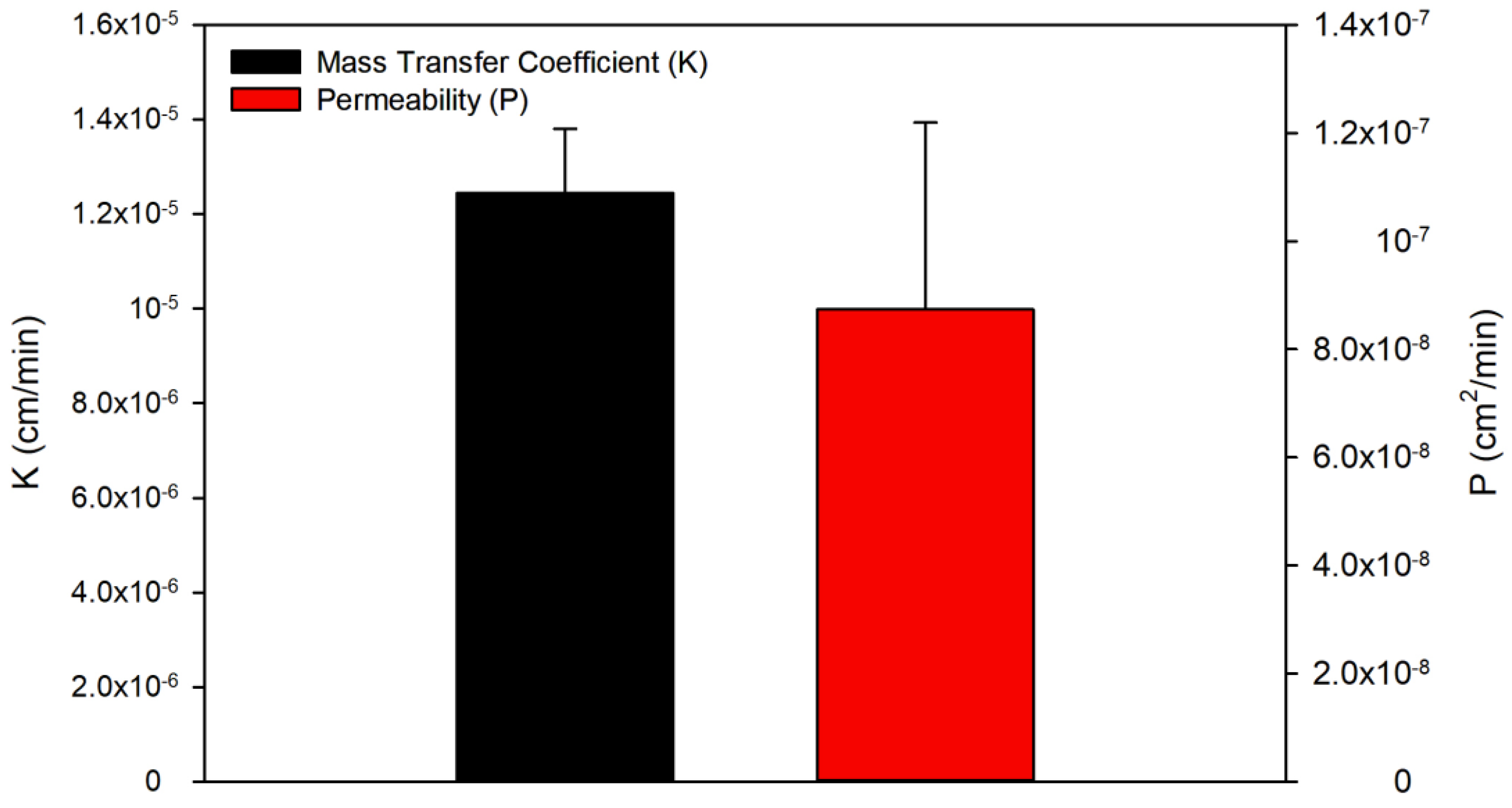
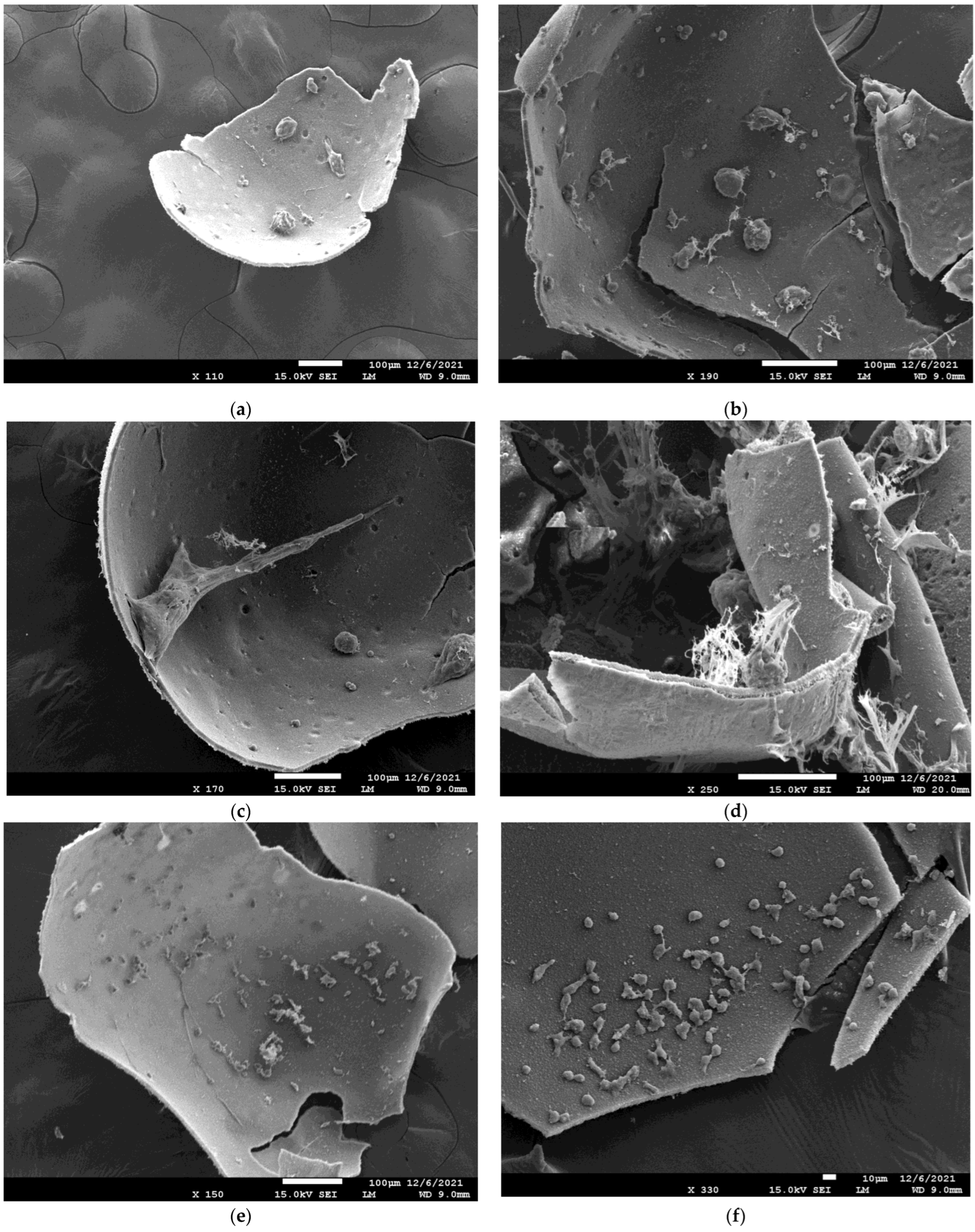
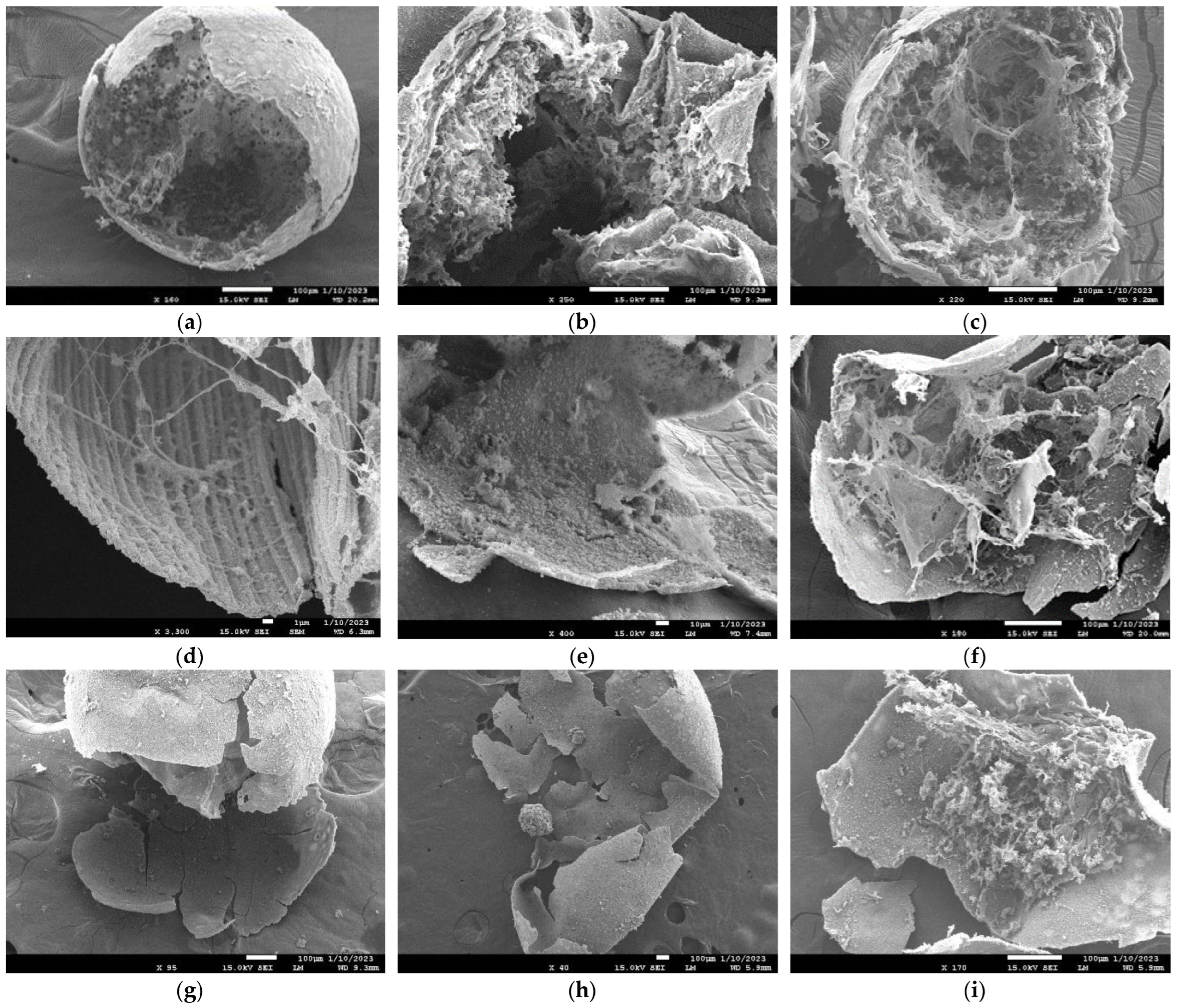
3.1. Material Characteristics of the Polyelectrolyte Complex Microcapsule
Polyelectrolyte Complex Microcapsule Morphology and Permeability
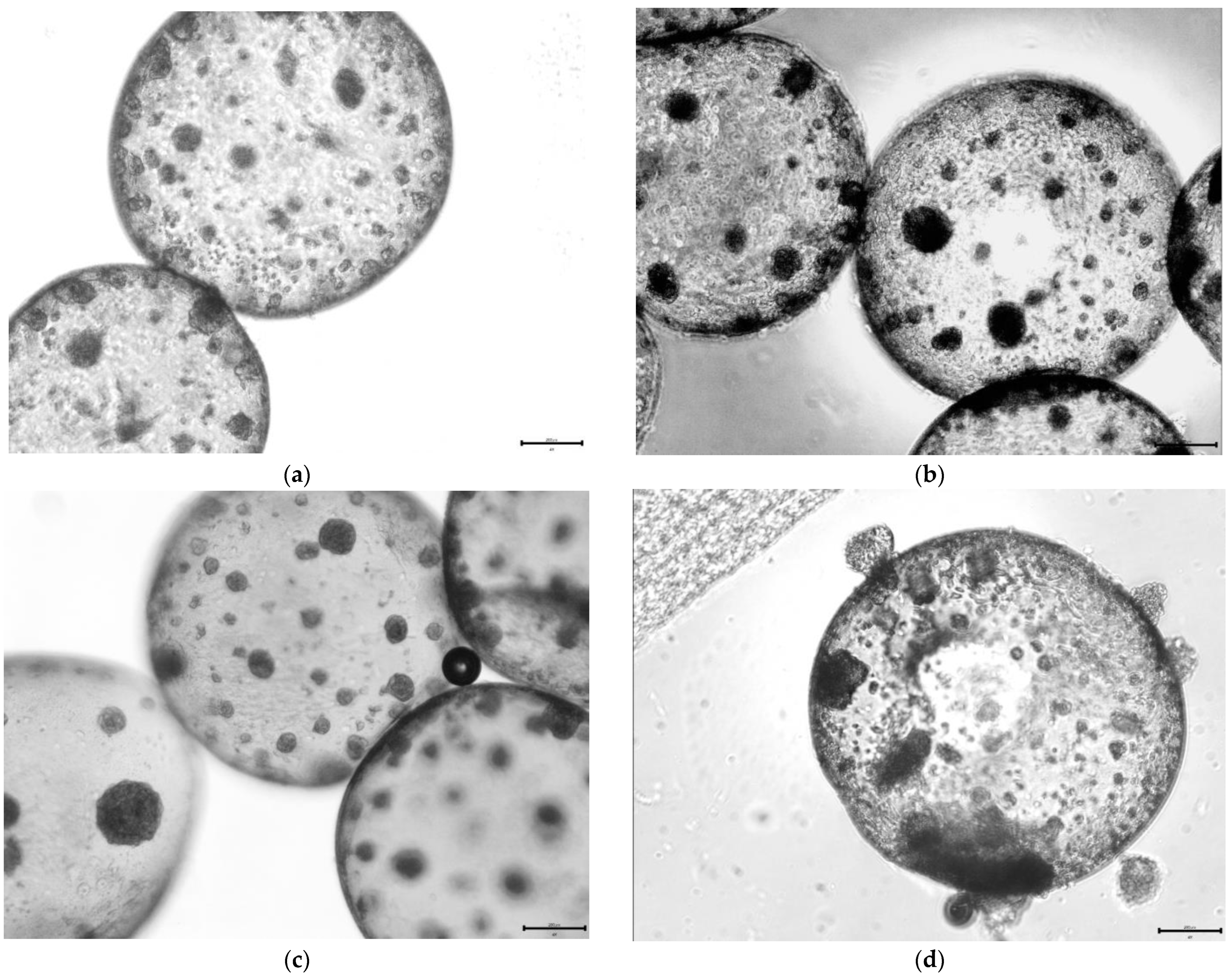
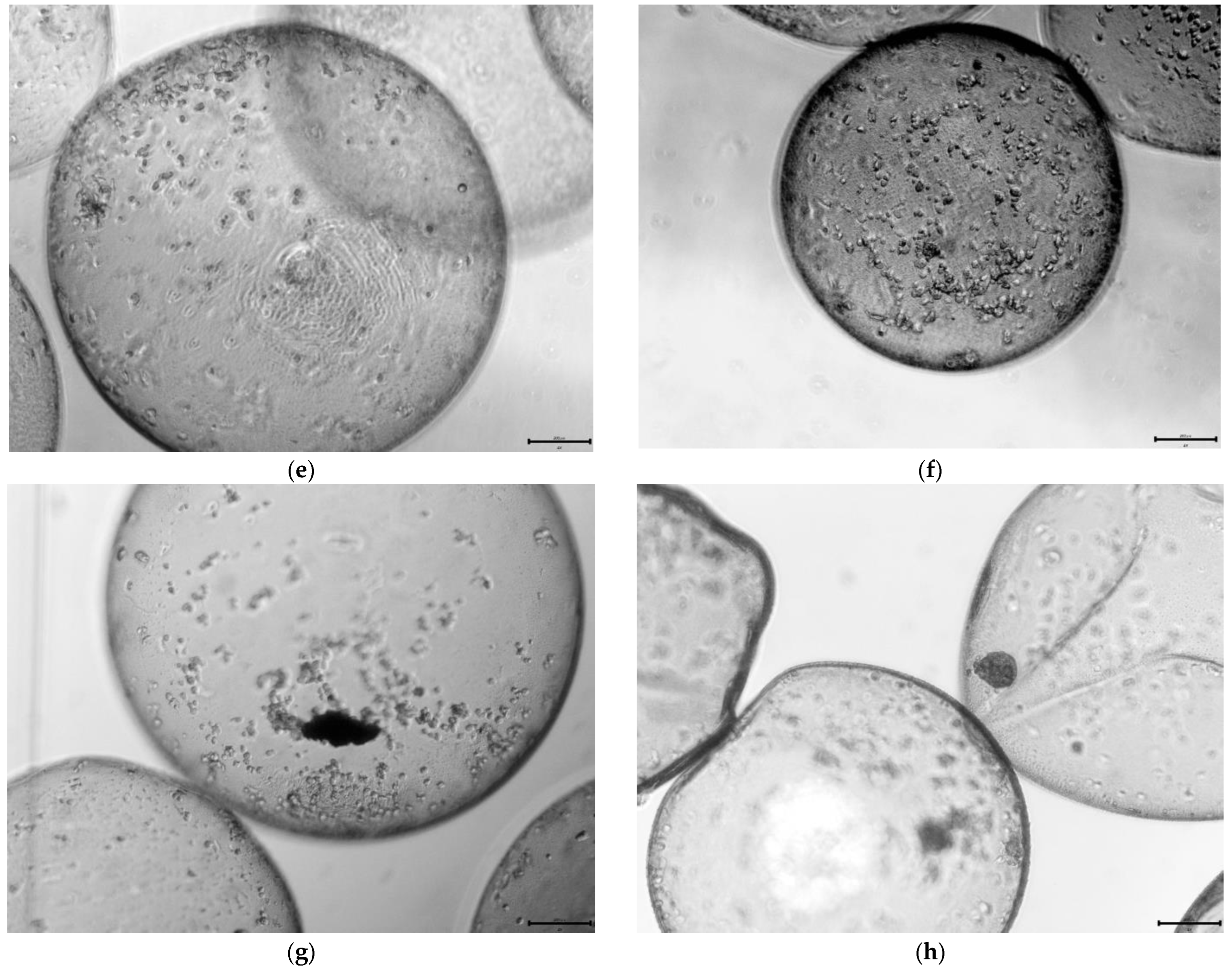
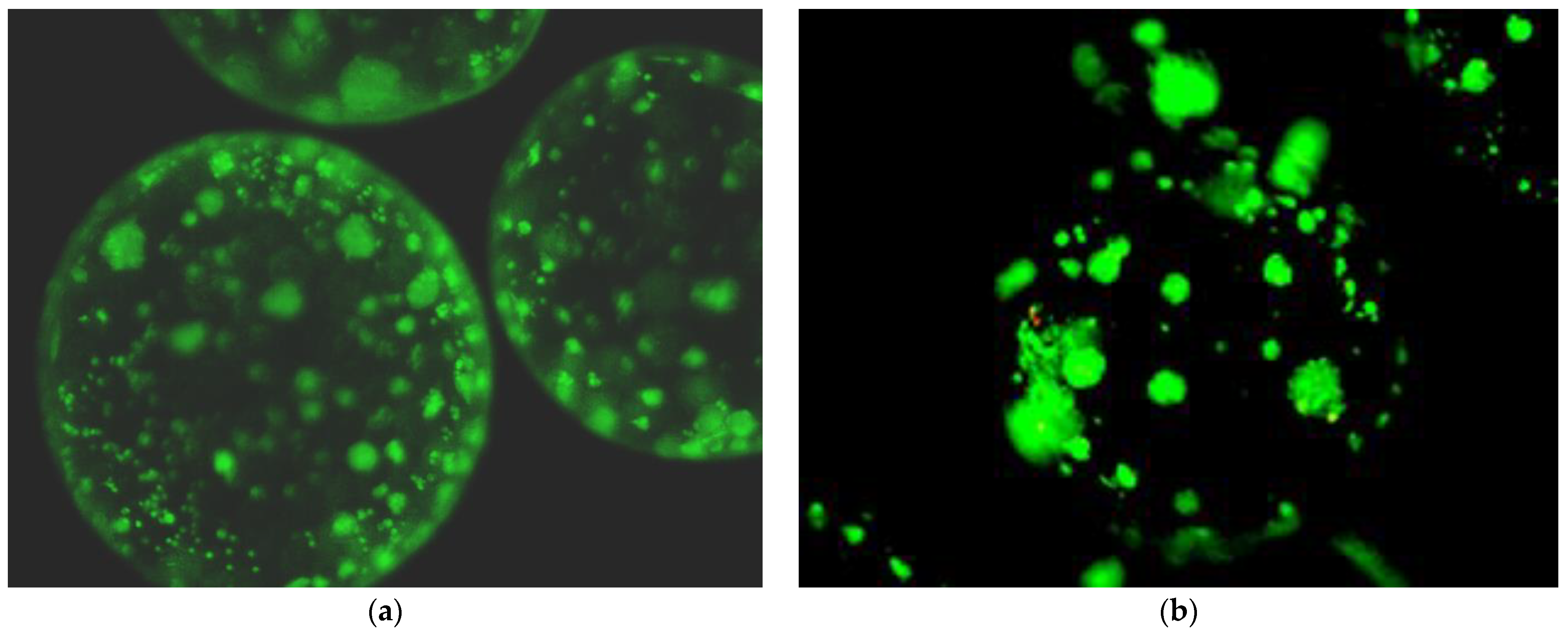
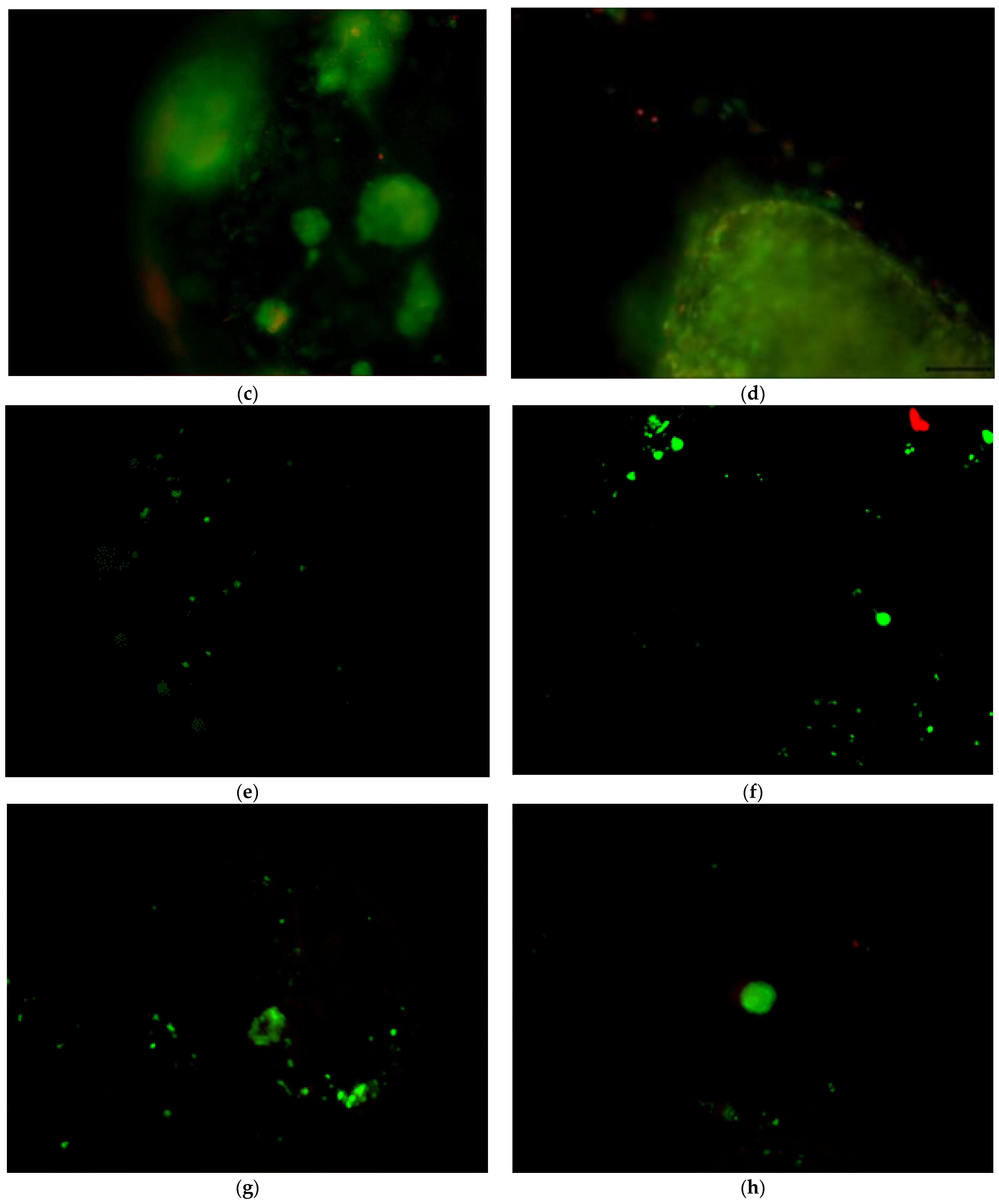
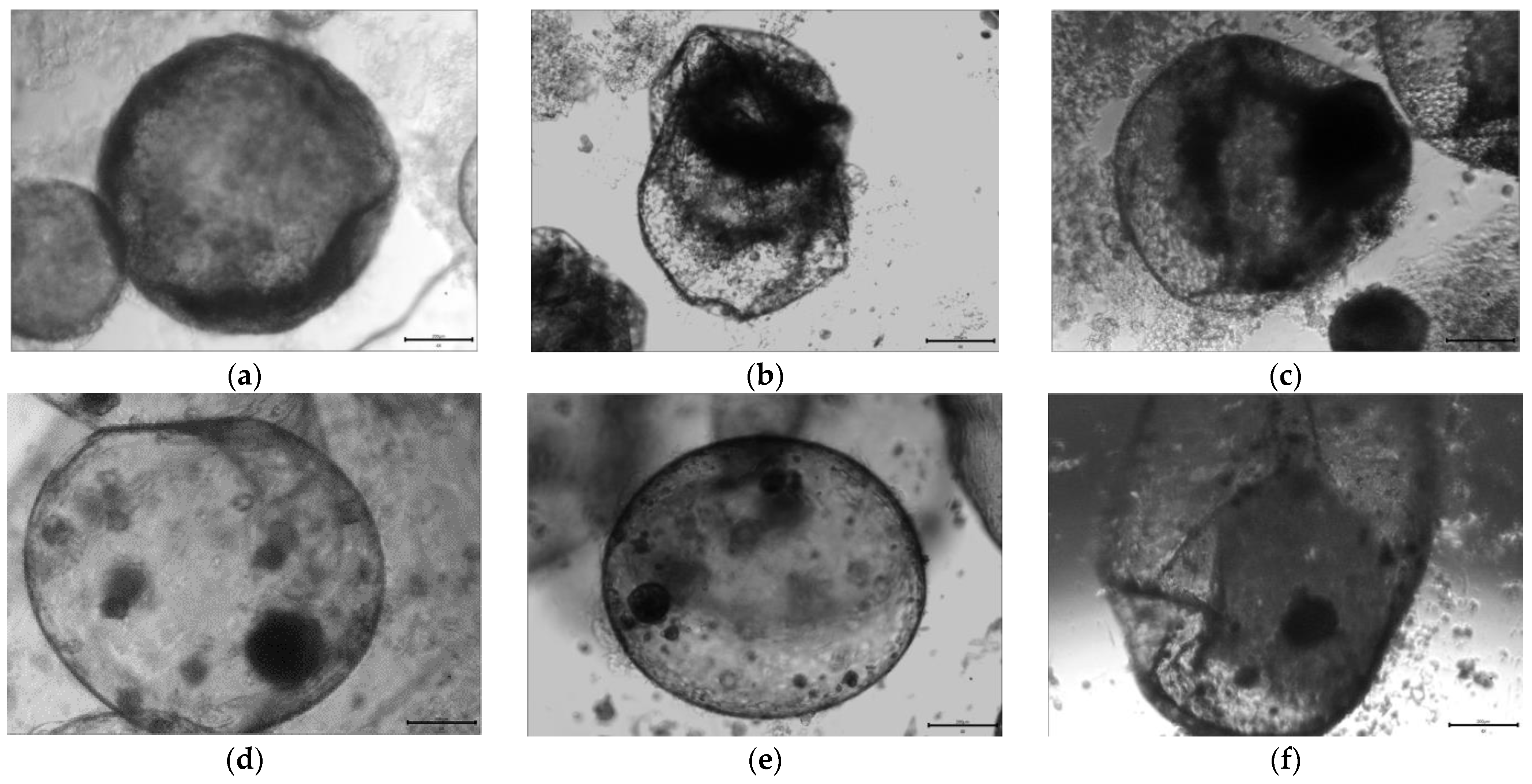
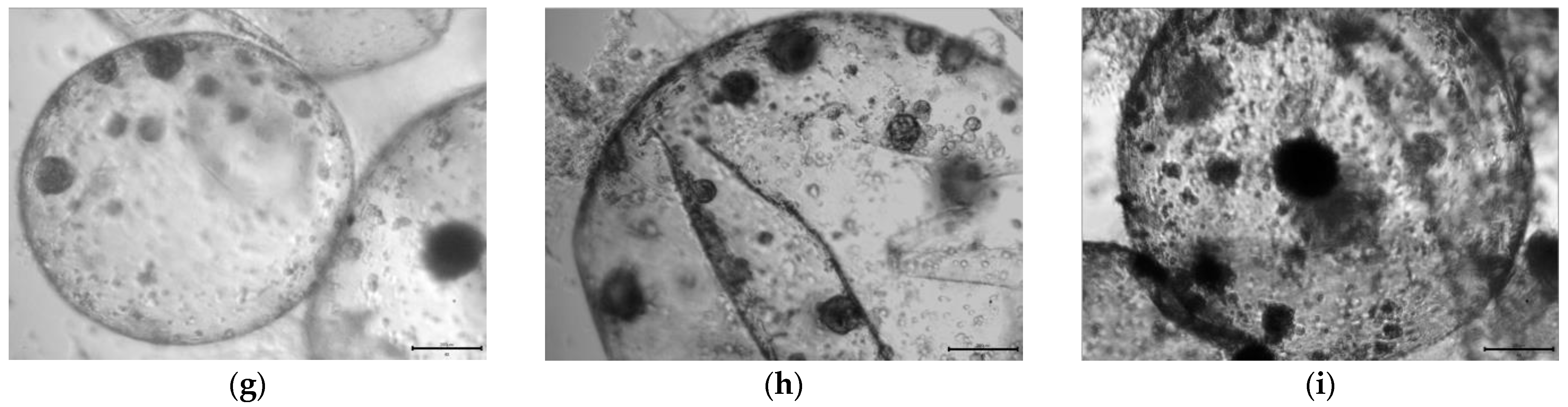
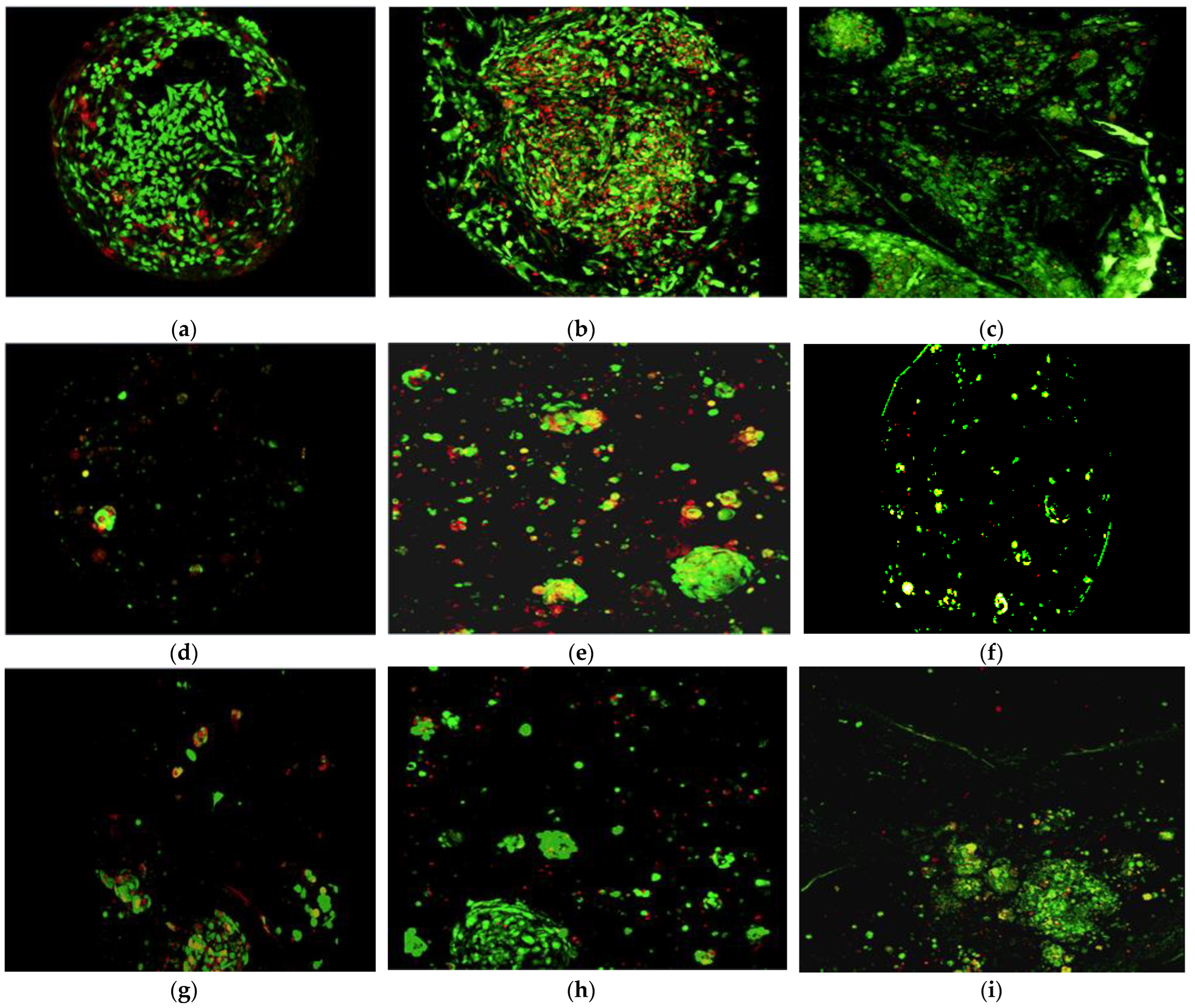
3.2. Morphology of Chondrocytes and bMSCs over 28-Day Encapsulated Culture
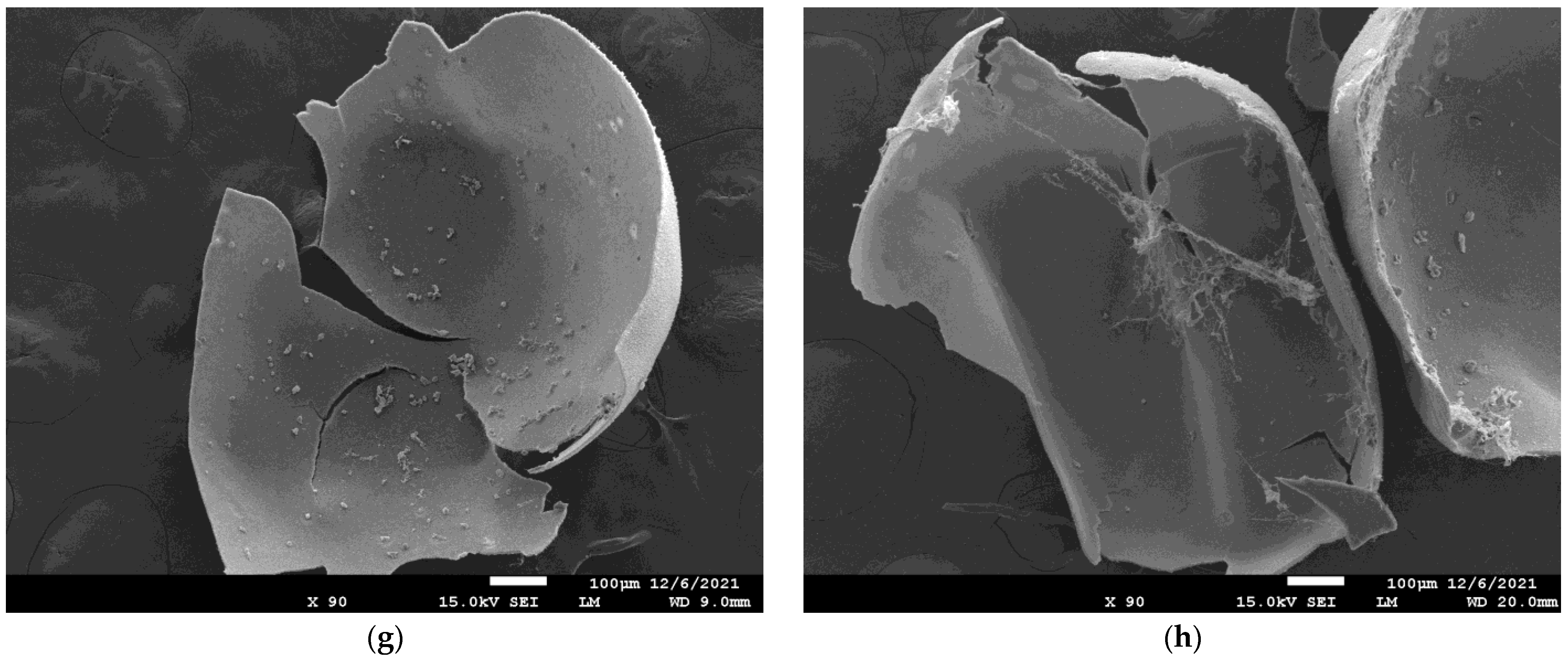
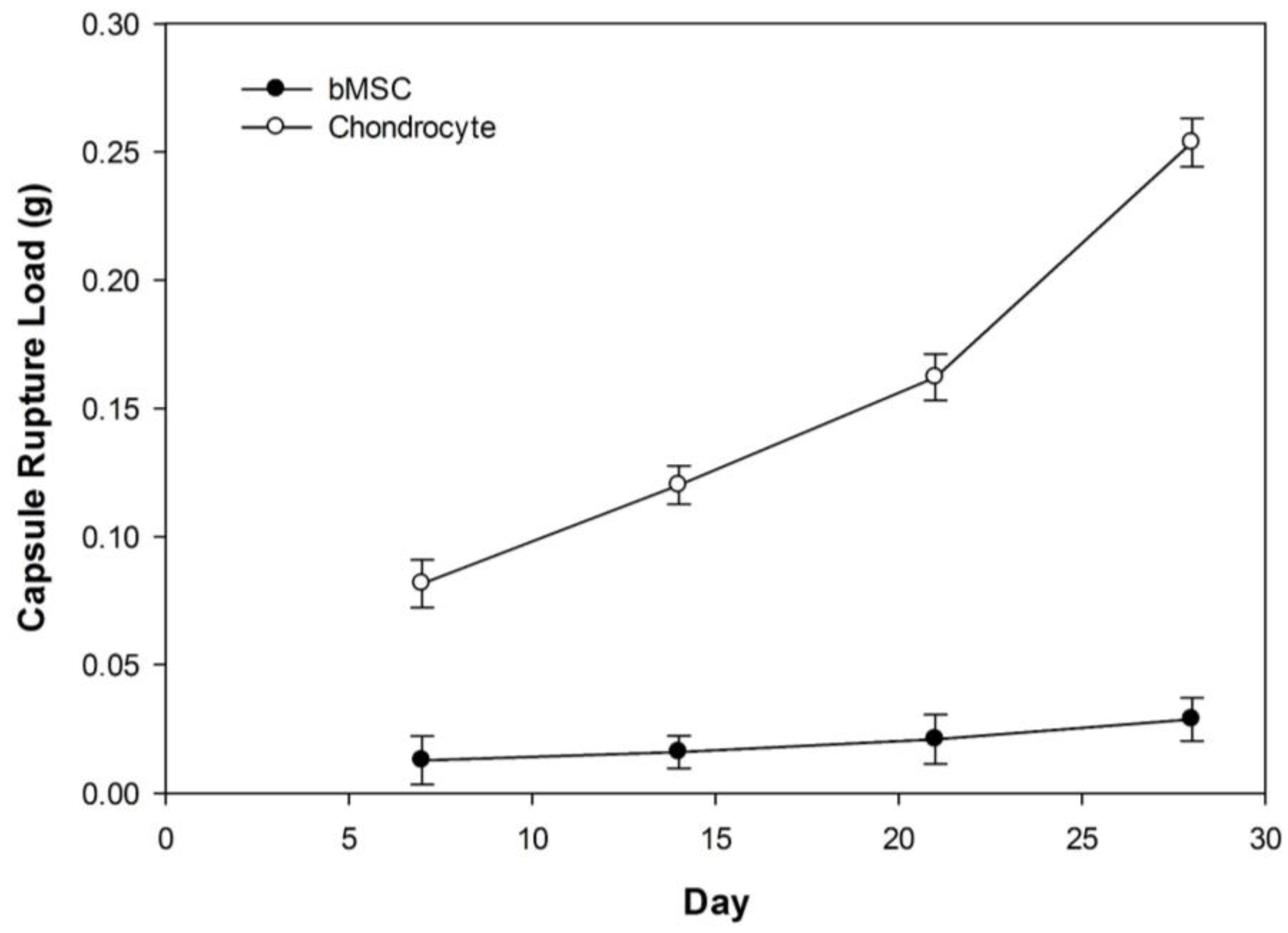
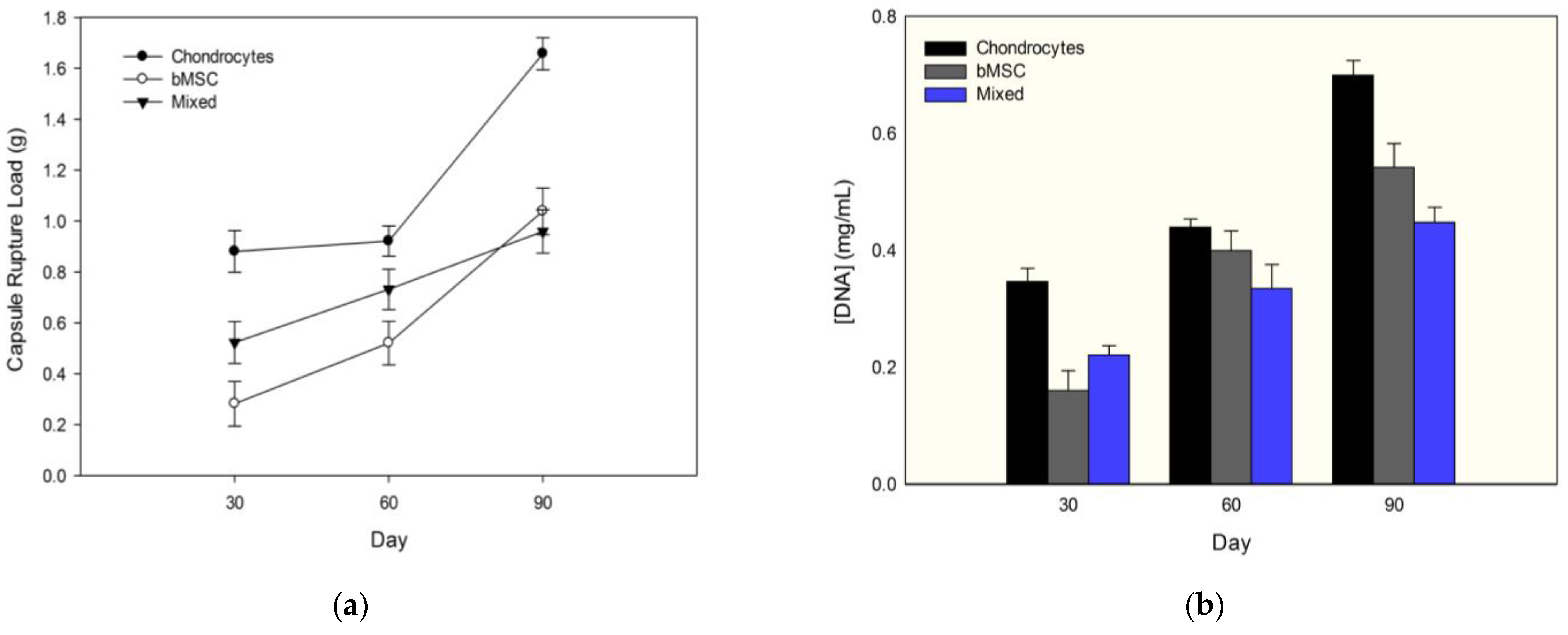
3.3. Changes in PECM Rupture Strength during Culture
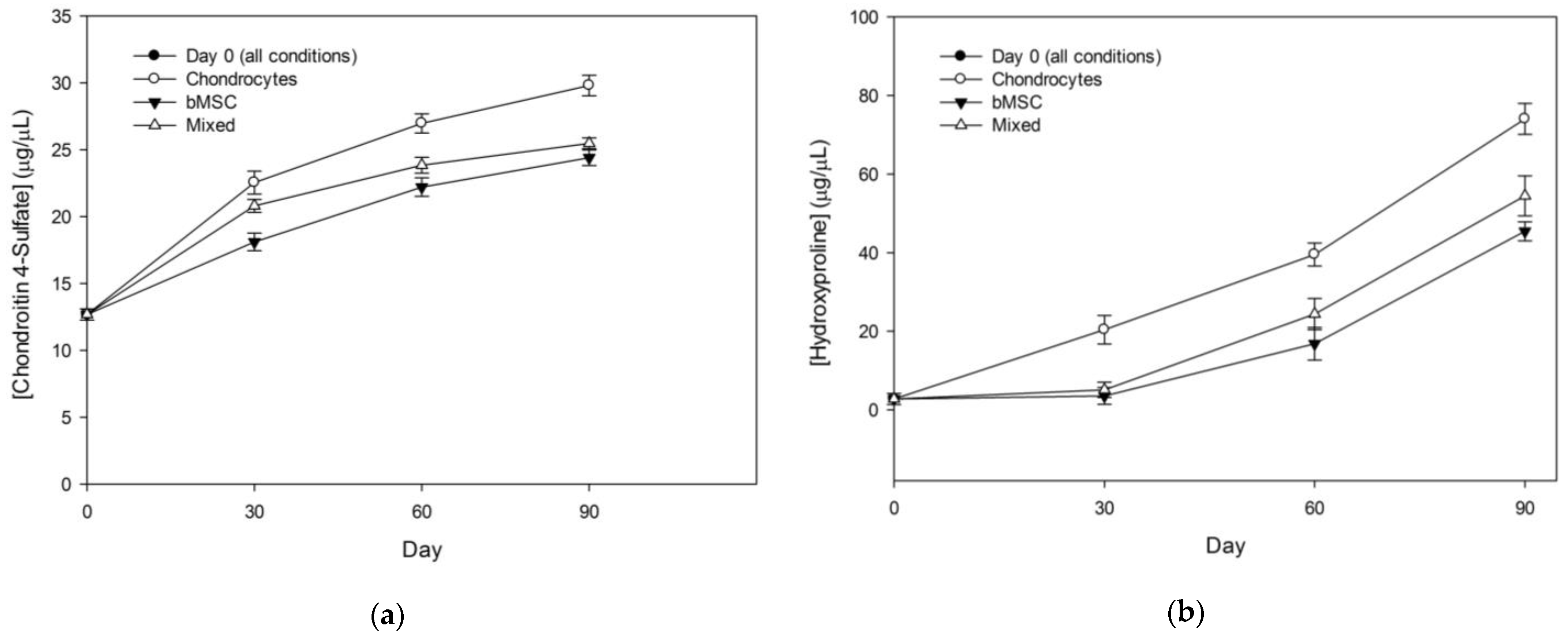
3.4. 90-Day Encapsulation Cultures
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Glyn-Jones, S.; Palmer, A.J.R.; Agricola, R.; Price, A.J.; Vincent, T.L.; Weinans, H.; Carr, A.J. Osteoarthritis. Lancet 2015, 386, 376–387. [Google Scholar] [CrossRef] [PubMed]
- Kan, H.S.; Chan, P.K.; Chiu, K.Y.; Yan, C.H.; Yeung, S.S.; Ng, Y.L.; Shiu, K.W.; Ho, T. Non-surgical treatment of knee osteoarthritis. Hong Kong Med. J. 2019, 25, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, M.T.; Gomes, M.E.; Reis, R.L. Current strategies for osteochondral regeneration: From stem cells to pre-clinical approaches. Curr. Opin. Biotechnol. 2011, 22, 726–733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borrelli, J.; Olson, S.A.; Godbout, C.; Schemitsch, E.H.; Stannard, J.P.; Giannoudis, P.V. Understanding Articular Cartilage Injury and Potential Treatments. J. Orthop. Trauma 2019, 33, S6–S12. [Google Scholar] [CrossRef] [PubMed]
- Bortoluzzi, A.; Furini, F.; Scirè, C.A. Osteoarthritis and its management—Epidemiology, nutritional aspects and environmental factors. Autoimmun. Rev. 2018, 17, 1097–1104. [Google Scholar] [CrossRef]
- Hawker, G.A. Osteoarthritis is a serious disease. Clin. Exp. Rheumatol. 2019, 37, 3–6. [Google Scholar]
- Neogi, T.; Zhang, Y. Epidemiology of Osteoarthritis. Rheum. Dis. Clin. N. Am. 2013, 39, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Grayson, W.L.; Chao, P.H.G.; Marolt, D.; Kaplan, D.L.; Vunjak-Novakovic, G. Engineering custom-designed osteochondral tissue grafts. Trends Biotechnol. 2008, 26, 181–189. [Google Scholar] [CrossRef] [Green Version]
- Tan, A.R.; Hung, C.T. Concise review: Mesenchymal stem cells for functional cartilage tissue engineering: Taking cues from chondrocyte-based constructs. Stem Cells Transl. Med. 2017, 6, 1295–1303. [Google Scholar] [CrossRef]
- Goldring, M.B. Chondrogenesis, chondrocyte differentiation, and articular cartilage metabolism in health and osteoarthritis. Ther. Adv. Musculoskelet. Dis. 2012, 4, 269–285. [Google Scholar] [CrossRef]
- Jiang, S.; Guo, W.; Tian, G.; Luo, X.; Peng, L.; Liu, S.; Sui, X.; Guo, Q.; Li, X. Clinical Application Status of Articular Cartilage Regeneration Techniques: Tissue-Engineered Cartilage Brings New Hope. Stem Cells Int. 2020, 2020, 5690252. [Google Scholar] [CrossRef]
- Moyad, T.F. Cartilage injuries in the adult knee: Evaluation and management. Cartilage 2011, 2, 226–236. [Google Scholar] [CrossRef] [Green Version]
- Gomoll, A.H.; Filardo, G.; Almqvist, F.K.; Bugbee, W.D.; Jelic, M.; Monllau, J.C.; Puddu, G.; Rodkey, W.G.; Verdonk, P.; Verdonk, R.; et al. Surgical treatment for early osteoarthritis. Part II: Allografts and concurrent procedures. Knee Surg. Sport. Traumatol. Arthrosc. 2012, 20, 468–486. [Google Scholar] [CrossRef]
- de l’Escalopier, N.; Anract, P.; Biau, D. Surgical treatments for osteoarthritis. Ann. Phys. Rehabil. Med. 2016, 59, 227–233. [Google Scholar] [CrossRef]
- Gomoll, A.H.; Filardo, G.; de Girolamo, L.; Esprequeira-Mendes, J.; Marcacci, M.; Rodkey, W.G.; Steadman, R.J.; Zaffagnini, S.; Kon, E. Surgical treatment for early osteoarthritis. Part I: Cartilage repair procedures. Knee Surg. Sport. Traumatol. Arthrosc. 2012, 20, 450–466. [Google Scholar] [CrossRef]
- Negoro, T.; Takagaki, Y.; Okura, H.; Matsuyama, A. Trends in clinical trials for articular cartilage repair by cell therapy. npj Regen. Med. 2018, 3, 17. [Google Scholar] [CrossRef] [Green Version]
- Sophia Fox, A.J.; Bedi, A.; Rodeo, S.A. The basic science of articular cartilage: Structure, composition, and function. Sport. Health 2009, 1, 461–468. [Google Scholar] [CrossRef] [Green Version]
- Dhollander, A.A.M.; Liekens, K.; Almqvist, K.F.; Verdonk, R.; Lambrecht, S.; Elewaut, D.; Verbruggen, G.; Verdonk, P.C.M. A pilot study of the use of an osteochondral scaffold plug for cartilage repair in the knee and how to deal with early clinical failures. Arthrosc.—J. Arthrosc. Relat. Surg. 2012, 28, 225–233. [Google Scholar] [CrossRef]
- Runhaar, J.; Zhang, Y. Can we prevent OA? Epidemiology and public health insights and implications. Rheumatology 2018, 57, iv3–iv9. [Google Scholar] [CrossRef] [Green Version]
- Fosang, A.J.; Beier, F. Emerging Frontiers in cartilage and chondrocyte biology. Best Pract. Res. Clin. Rheumatol. 2011, 25, 751–766. [Google Scholar] [CrossRef]
- Huang, B.J.; Hu, J.C.; Athanasiou, K.A. Cell-based tissue engineering strategies used in the clinical repair of articular cartilage. Biomaterials 2016, 98, 1–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miles, K.B.; Maerz, T.; Matthew, H.W.T. Scalable MSC-derived bone tissue modules: In vitro assessment of differentiation, matrix deposition, and compressive load bearing. Acta Biomater. 2019, 95, 395–407. [Google Scholar] [CrossRef] [PubMed]
- Vunjak-Novakovic, G.; Meinel, L.; Altman, G.; Kaplan, D. Bioreactor cultivation of osteochondral grafts. Orthod. Craniofacial Res. 2005, 8, 209–218. [Google Scholar] [CrossRef] [PubMed]
- Roseti, L.; Cavallo, C.; Desando, G.; Parisi, V.; Petretta, M.; Bartolotti, I.; Grigolo, B. Three-dimensional bioprinting of cartilage by the use of stem cells: A strategy to improve regeneration. Materials 2018, 11, 1749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thorp, H.; Kim, K.; Kondo, M.; Grainger, D.W.; Okano, T. Fabrication of hyaline-like cartilage constructs using mesenchymal stem cell sheets. Sci. Rep. 2020, 10, 20869. [Google Scholar] [CrossRef]
- Bi, L.; Li, D.; Liu, J.; Hu, Y.; Yang, P.; Yang, B.; Yuan, Z. Fabrication and characterization of a biphasic scaffold for osteochondral tissue engineering. Mater. Lett. 2011, 65, 2079–2082. [Google Scholar] [CrossRef]
- Huang, A.H.; Yeger-McKeever, M.; Stein, A.; Mauck, R.L. Tensile properties of engineered cartilage formed from chondrocyte- and MSC-laden hydrogels. Osteoarthr. Cartil. 2008, 16, 1074–1082. [Google Scholar] [CrossRef] [Green Version]
- Tiruvannamalai-Annamalai, R.; Armant, D.R.; Matthew, H.W.T. A glycosaminoglycan based, modular tissue scaffold system for rapid assembly of perfusable, high cell density, engineered tissues. PLoS ONE 2014, 9, e84287. [Google Scholar] [CrossRef] [Green Version]
- Miles, K.B.; Ball, R.L.; Matthew, H.W.T. Chitosan films with improved tensile strength and toughness from N-acetyl-cysteine mediated disulfide bonds. Carbohydr. Polym. 2016, 139, 1–9. [Google Scholar] [CrossRef]
- Vossoughi, A.; Matthew, H.W.T. Encapsulation of mesenchymal stem cells in glycosaminoglycans-chitosan polyelectrolyte microcapsules using electrospraying technique: Investigating capsule morphology and cell viability. Bioeng. Transl. Med. 2018, 3, 265–274. [Google Scholar] [CrossRef] [Green Version]
- Sechriest, V.F.; Miao, Y.J.; Niyibizi, C.; Westerhausen-Larson, A.; Matthew, H.W.; Evans, C.H.; Fu, F.H.; Suh, J.K. GAG-augmented polysaccharide hydrogel: A novel biocompatible and biodegradable material to support chondrogenesis. J. Biomed. Mater. Res. 2000, 49, 534–541. [Google Scholar] [CrossRef]
- Poldervaart, M.T.; Goversen, B.; De Ruijter, M.; Abbadessa, A.; Melchels, F.P.W.; Öner, F.C.; Dhert, W.J.A.; Vermonden, T.; Alblas, J. 3D bioprinting of methacrylated hyaluronic acid (MeHA) hydrogel with intrinsic osteogenicity. PLoS ONE 2017, 12, e0177628. [Google Scholar] [CrossRef] [Green Version]
- Matthew, H.W.; Salley, S.O.; Peterson, W.D.; Klein, M.D. Complex Coacervate Microcapsules for Mammalian Cell Culture and Artificial Organ Development. Biotechnol. Prog. 1993, 9, 510–519. [Google Scholar] [CrossRef]
- Lan, X.; Liang, Y.; Erkut, E.J.N.; Kunze, M.; Mulet-Sierra, A.; Gong, T.; Osswald, M.; Ansari, K.; Seikaly, H.; Boluk, Y.; et al. Bioprinting of human nasoseptal chondrocytes-laden collagen hydrogel for cartilage tissue engineering. FASEB J. 2021, 35, e21191. [Google Scholar] [CrossRef]
- Karaoz, E.; Aksoy, A.; Ayhan, S.; Sariboyaci, A.E.; Kaymaz, F.; Kasap, M. Characterization of mesenchymal stem cells from rat bone marrow: Ultrastructural properties, differentiation potential and immunophenotypic markers. Histochem. Cell Biol. 2009, 132, 533–546. [Google Scholar] [CrossRef]
- Karcz, J. Scanning Electron Microscopy Technique: Standard Preparation of Biological Material for SEM Analysis. Univ Silesia SEM-Lab, 2008, pp. 1–2. Available online: https://www.researchgate.net/file.PostFileLoader.html?id=53819addd5a3f294718b463e&assetKey=AS%3A272444059783194%401441967137890 (accessed on 5 April 2023).
- Cissell, D.D.; Link, J.M.; Hu, J.C.; Athanasiou, K.A. A Modified Hydroxyproline Assay Based on Hydrochloric Acid in Ehrlich’s Solution Accurately Measures Tissue Collagen Content. Tissue Eng. Part C Methods 2017, 23, 243–250. [Google Scholar] [CrossRef] [Green Version]
- Middendorf, J.M.; Griffin, D.J.; Shortkroff, S.; Dugopolski, C.; Kennedy, S.; Siemiatkoski, J.; Cohen, I.; Bonassar, L.J. Mechanical properties and structure-function relationships of human chondrocyte-seeded cartilage constructs after in vitro culture. J. Orthop. Res. 2017, 35, 2298–2306. [Google Scholar] [CrossRef] [Green Version]
- Gaigalas, A.K.; Hubbard, J.B.; McCurley, M.; Woo, S. Diffusion of bovine serum albumin in aqueous solutions. J. Phys. Chem. 1992, 96, 2355–2359. [Google Scholar] [CrossRef]
- Annamalai, R.T.; Matthew, H.W.T. Transport analysis of engineered liver tissue fabricated using a capsule-based, modular approach. Ann. Biomed. Eng. 2019, 47, 1223–1236. [Google Scholar] [CrossRef]




















Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arhebamen, E.P.; Teodoro, M.T.; Blonka, A.B.; Matthew, H.W.T. Long-Term Culture Performance of a Polyelectrolyte Complex Microcapsule Platform for Hyaline Cartilage Repair. Bioengineering 2023, 10, 467. https://doi.org/10.3390/bioengineering10040467
Arhebamen EP, Teodoro MT, Blonka AB, Matthew HWT. Long-Term Culture Performance of a Polyelectrolyte Complex Microcapsule Platform for Hyaline Cartilage Repair. Bioengineering. 2023; 10(4):467. https://doi.org/10.3390/bioengineering10040467
Chicago/Turabian StyleArhebamen, Ehinor P., Maria T. Teodoro, Amelia B. Blonka, and Howard W. T. Matthew. 2023. "Long-Term Culture Performance of a Polyelectrolyte Complex Microcapsule Platform for Hyaline Cartilage Repair" Bioengineering 10, no. 4: 467. https://doi.org/10.3390/bioengineering10040467