

Electrocardiography Assessment of Sympatico–Vagal Balance during Resting and Pain Using the Texas Instruments ADS1299
 ,
,  ,
on behalf of the P-QST Consortium
,
on behalf of the P-QST Consortium
Abstract
:1. Introduction
2. Materials and Methods
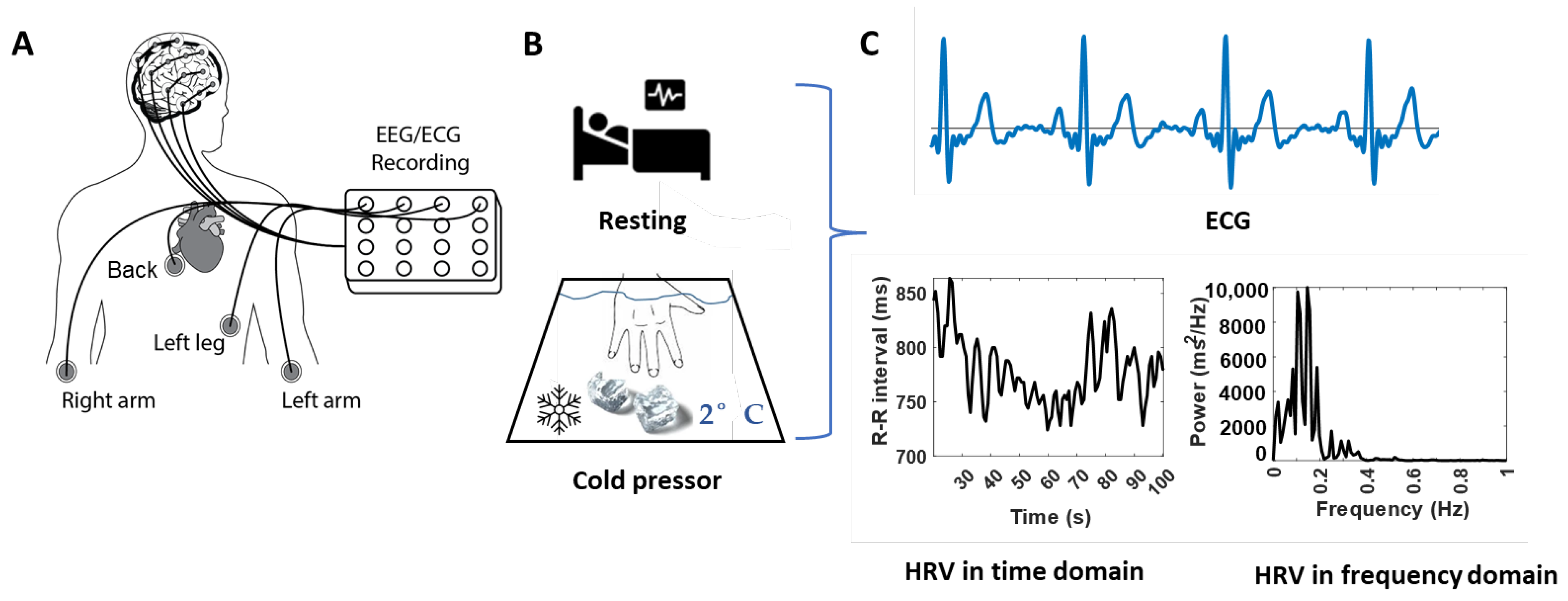
2.1. Data Recording System
2.2. Participants
2.3. Experiment Procedures
2.4. Data Processing
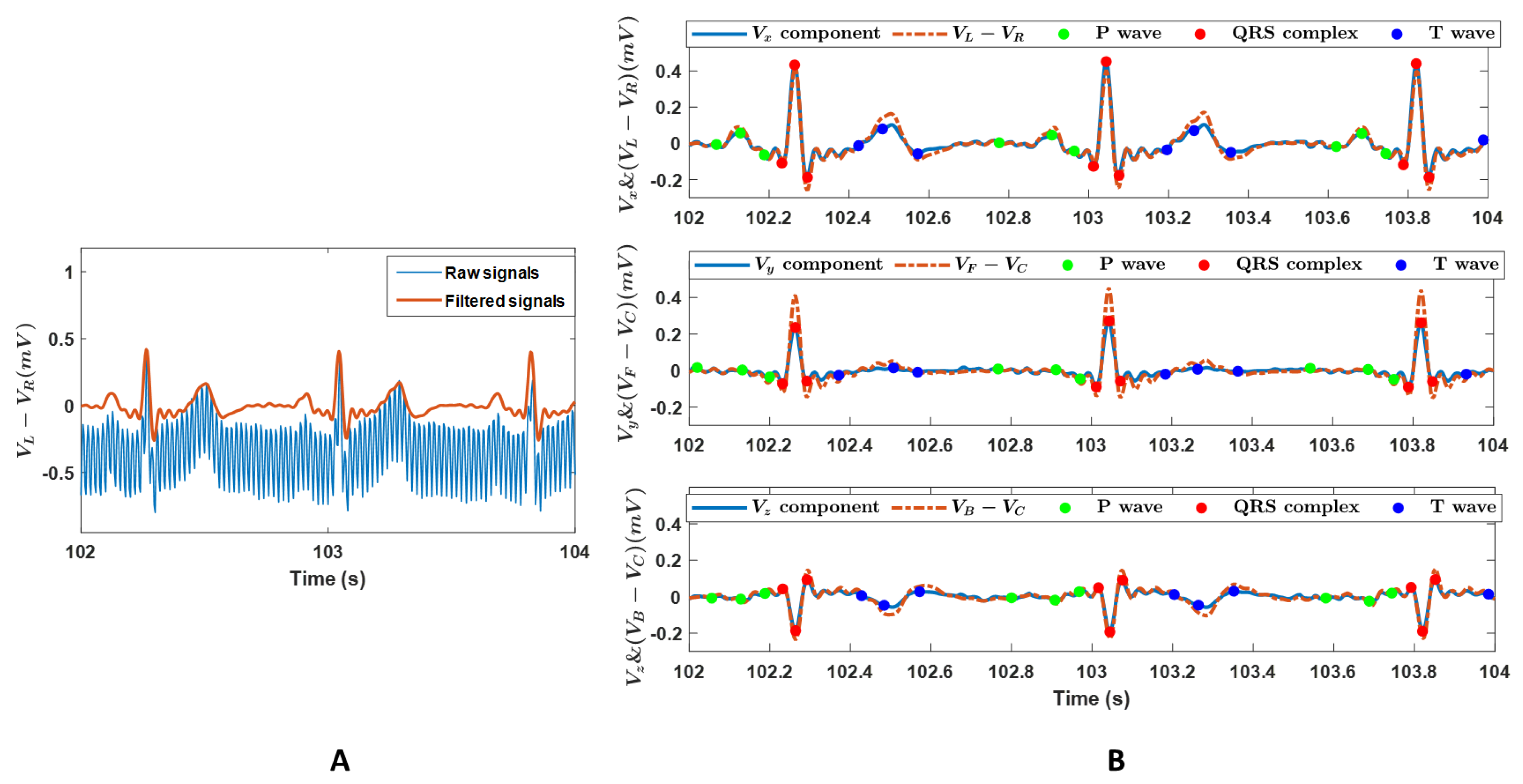
- Building zero-phase shift bandpass filter (2–26 Hz);
- Zero-phase filtering using the built band-pass filter in 1) and the scale values = 1;
- Visual inspection of data quality, the offset of the isoline of the ECG data was estimated and removed;
- Rereferencing to the common average reference.
2.4.1. Vectorcardiography Vectors
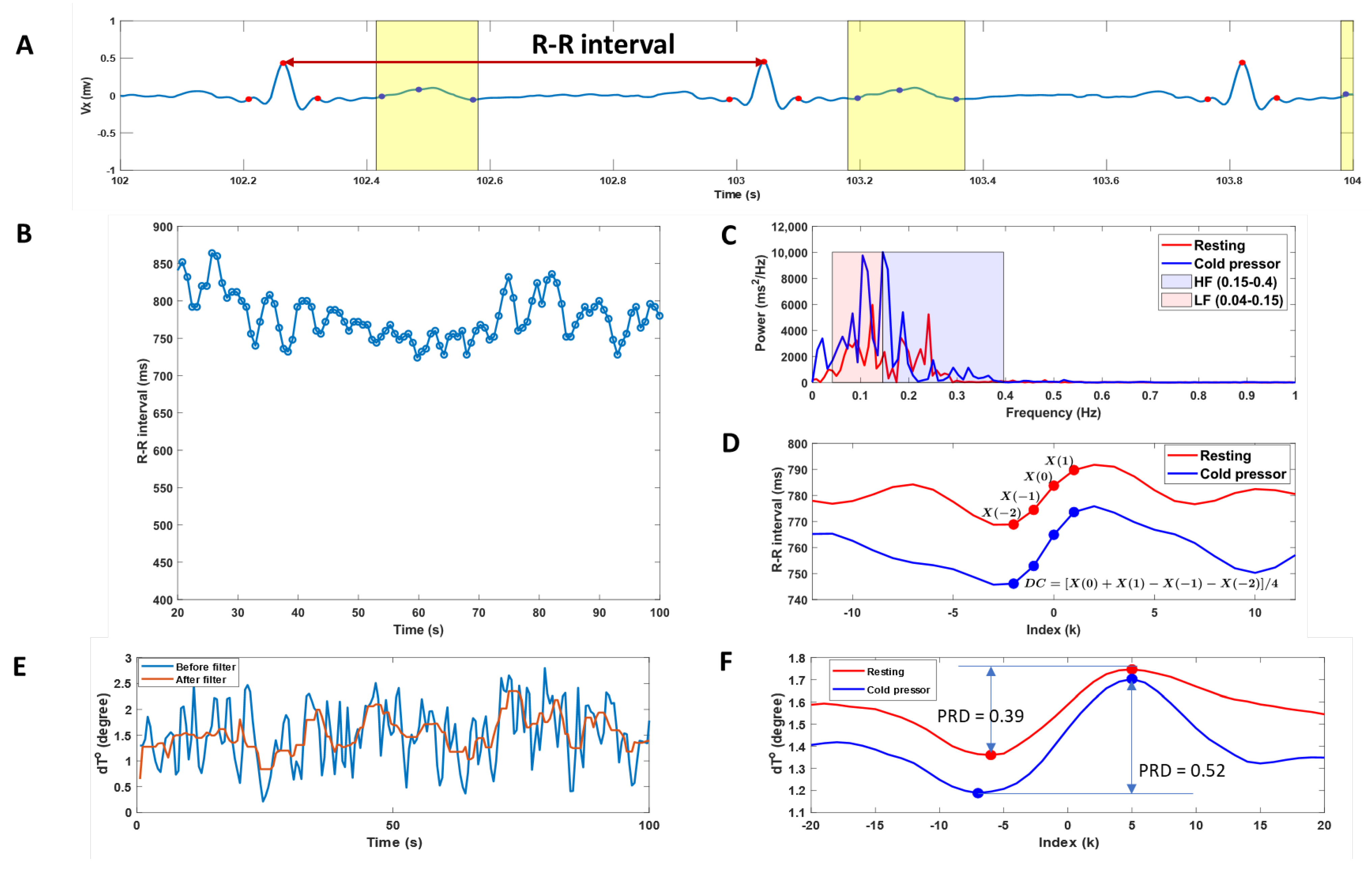
2.4.2. ECG-Based Biomarkers
- HRV parameters
- Deceleration capacity
- An anchor point, defined as the heartbeat intervals longer than the preceding interval.
- Windows of 2 L values, defined around each anchor point, where L is the point number previous and posterior to the anchor point in the RR interval curve. Anchor points in the last L samples of the RR intervals were discarded, as windows of length 2 L could not be defined around them. In this study, L = 12 was chosen because it was the minimum value to detect the low frequencies of the RR intervals series in the range of interest (0.04–0.15) Hz.
- The phase-rectified signal averaging series was obtained by averaging the RR values over all 2 L-sample windows contained in recordings during resting and cold pressor.
- A DC value was calculated from the phase-rectified signal averaging series at the anchors , the point immediately following the anchors , and the two points preceding the anchors and as:
- Periodic repolarization dynamics
- The phase-rectified signal averaging of the dT° time series was obtained using a similar procedure to the above phase-rectified signal averaging estimations in deceleration capacity calculation. The anchor points were defined by comparing averages of M = 9 values of the dT° series previous and posterior to the anchor point candidate (xi). A beat i is considered an anchor point if:
- 2.
- Windows of 2 L values were defined around each anchor point. In this study, L = 20 was chosen because it was the minimum value to detect frequencies in the range of interest (0.025–0.1) Hz, as described in Palacios [10].
- 3.
- Phase-rectified signal averaging series were obtained by averaging the dT° series overall defined windows.
- 4.
- PRD was defined as the difference between the maximum and minimum values of the phase-rectified signal averaging series.
2.5. Statistical Analysis
3. Results
3.1. ECG Signals
3.2. ECG-Based Cardiac Function Biomarkers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Florea, V.G.; Cohn, J.N. The autonomic nervous system and heart failure. Circ. Res. 2014, 114, 1815–1826. [Google Scholar] [CrossRef]
- Malik, M.; Bigger, J.T.; Camm, A.J.; Kleiger, R.E.; Malliani, A.; Moss, A.J.; Schwartz, P.J. Heart rate variability. Standards of measurement, physiological interpretation, and clinical use. Eur. Heart J. 1996, 17, 354–381. [Google Scholar] [CrossRef]
- Schüttler, D.; Hamm, W.; Bauer, A.; Brunner, S. Routine heart rate-based and novel ecg-based biomarkers of autonomic nervous system in sports medicine. Dtsch. Z. Sportmed. 2020, 71, 141–150. [Google Scholar] [CrossRef]
- Hernández-Vicente, A.; Hernando, D.; Vicente-Rodríguez, G.; Bailón, R.; Garatachea, N.; Pueyo, E. ECG Ventricular Repolarization Dynamics during Exercise: Temporal Profile, Relation to Heart Rate Variability and Effects of Age and Physical Health. Int. J. Environ. Res. Public Health 2021, 18, 9497. [Google Scholar] [CrossRef] [PubMed]
- Cui, J.; Wilson, T.E.; Crandall, C.G. Baroreflex modulation of muscle sympathetic nerve activity during cold pressor test in humans. Am. J. Physiol. Circ. Physiol. 2002, 282, H1717–H1723. [Google Scholar] [CrossRef]
- Weise, F.; Laude, D.; Girard, A.; Zitoun, P.; Siché, J.P.; Elghozi, J.L. Effects of the cold pressor test on short-term fluctuations of finger arterial blood pressure and heart rate in normal subjects. Clin. Auton. Res. 1993, 3, 303–310. [Google Scholar] [CrossRef]
- Bauer, A.; Kantelhardt, J.W.; Barthel, P.; Schneider, R.; Mäkikallio, T.; Ulm, K.; Hnatkova, K.; Schömig, A.; Huikuri, H.; Bunde, A.; et al. Deceleration capacity of heart rate as a predictor of mortality after myocardial infarction: Cohort study. Lancet 2006, 367, 1674–1681. [Google Scholar] [CrossRef]
- Rizas, K.D.; Hamm, W.; Kääb, S.; Schmidt, G.; Bauer, A. Periodic Repolarisation Dynamics: A Natural Probe of the Ventricular Response to Sympathetic Activation. Arrhythmia Electrophysiol. Rev. 2016, 5, 31–36. [Google Scholar] [CrossRef]
- Rizas, K.D.; Nieminen, T.; Barthel, P.; Zürn, C.S.; Kähönen, M.; Viik, J.; Lehtimäki, T.; Nikus, K.; Eick, C.; Greiner, T.O.; et al. Sympathetic activity-associated periodic repolarization dynamics predict mortality following myocardial infarction. J. Clin. Investig. 2014, 124, 1770–1780. [Google Scholar] [CrossRef]
- Palacios, S.; Caiani, E.G.; Landreani, F.; Martínez, J.P.; Pueyo, E. Long-Term Microgravity Exposure Increases ECG Repolarization Instability Manifested by Low-Frequency Oscillations of T-Wave Vector. Front. Physiol. 2019, 10, 1510. [Google Scholar] [CrossRef] [Green Version]
- Bauer, A.; Kantelhardt, J.W.; Bunde, A.; Barthel, P.; Schneider, R.; Malik, M.; Schmidt, G. Phase-rectified signal averaging detects quasi-periodicities in non-stationary data. Phys. A Stat. Mech. Appl. 2006, 364, 423–434. [Google Scholar] [CrossRef]
- Lear, C.A.; Westgate, J.; Kasai, M.; Beacom, M.; Maeda, Y.; Magawa, S.; Miyagi, E.; Ikeda, T.; Bennet, L.; Gunn, A. Parasympathetic activity is the key regulator of heart rate variability between decelerations during brief repeated umbilical cord occlusions in fetal sheep. Am. J. Physiol.—Regul. Integr. Comp. Physiol. 2020, 319, R541–R550. [Google Scholar] [CrossRef]
- Jauregui-Renaud, K.; Hermosillo, A.G.; Márquez, M.F.; Ramos-Aguilar, F.; Hernández-Goribar, M.; Cárdenas, M. Repeatability of heart rate variability during simple cardiovascular reflex tests on healthy subjects. Arch. Med. Res. 2001, 32, 21–26. [Google Scholar] [CrossRef]
- Hintsala, H.; Kenttä, T.V.; Tulppo, M.; Kiviniemi, A.; Huikuri, H.V.; Mäntysaari, M.; Keinänen-Kiukaannemi, S.; Bloigu, R.; Herzig, K.-H.; Antikainen, R.; et al. Cardiac Repolarization and Autonomic Regulation during Short-Term Cold Exposure in Hypertensive Men: An Experimental Study. PLoS ONE 2014, 9, e99973. [Google Scholar] [CrossRef]
- Tulppo, M.P.; Kiviniemi, A.; Hautala, A.; Kallio, M.; Seppanen, T.; Makikallio, T.H.; Huikuri, H.V. Physiological background of the loss of fractal heart rate dynamics. Circulation 2005, 112, 314–319. [Google Scholar] [CrossRef]
- Mourot, L.; Bouhaddi, M.; Regnard, J. Effects of the Cold Pressor Test on Cardiac Autonomic Control in Normal Subjects. 2009. Available online: www.biomed.cas.cz/physiolresPhysiol.Res.58:83-91,2009 (accessed on 6 October 2022).
- Rizas, K.D.; Doller, A.J.; Hamm, W.; Vdovin, N.; von Stuelpnagel, L.; Zuern, C.S.; Bauer, A. Periodic repolarization dynamics as a risk predictor after myocardial infarction: Prospective validation study. Heart Rhythm 2019, 16, 1223–1231. [Google Scholar] [CrossRef]
- Schüttler, D.; von Stülpnagel, L.; Rizas, K.D.; Bauer, A.; Brunner, S.; Hamm, W. Effect of Hyperventilation on Periodic Repolarization Dynamics. Front. Physiol. 2020, 11, 542183. [Google Scholar] [CrossRef]
- Rashid, U.; Niazi, I.K.; Signal, N.; Taylor, D. An EEG experimental study evaluating the performance of Texas instruments ADS1299. Sensors 2018, 18, 3721. [Google Scholar] [CrossRef]
- Wilson, F.N.; Johnston, F.D.; Kossmann, C.E. The substitution of a tetrahedron for the Einthoven triangle. Am. Heart J. 1947, 33, 594–603. [Google Scholar] [CrossRef]
- Frank, E. Analysis of R,L,F,B systems of spatial vectorcardiography. Am. Heart J. 1956, 51, 34–52. [Google Scholar] [CrossRef]
- Frank, E. The image surface of a homogeneous torso. Am. Heart J. 1954, 47, 757–768. [Google Scholar] [CrossRef]
- Pilia, N.; Nagel, C.; Lenis, G.; Becker, S.; Dössel, O.; Loewe, A. ECGdeli—An Open Source ECG Delineation Toolbox for MATLAB. 2020. Available online: https://github.com/KIT-IBT/ECGdeli (accessed on 2 February 2022).
- Palacios, S.; Cygankiewicz, I.; de Luna, A.B.; Pueyo, E.; Martínez, J.P. Periodic repolarization dynamics as predictor of risk for sudden cardiac death in chronic heart failure patients. Sci. Rep. 2021, 11, 20546. [Google Scholar] [CrossRef] [PubMed]
- Novak, V.; Saul, J.P.; Eckberg, D.L. Task Force Report on Heart Rate Variability. Circulation 1997, 96, 1056–1057. [Google Scholar] [PubMed]
- Shattock, M.J.; Tipton, M.J. ‘Autonomic conflict’: A different way to die during cold water immersion? J. Physiol. 2012, 590, 3219–3230. [Google Scholar] [CrossRef] [PubMed]
- Von Rosenberg, W.; Chanwimalueang, T.; Goverdovsky, V.; Looney, D.; Sharp, D.; Mandic, D.P. Smart Helmet: Wearable Multichannel ECG and EEG. IEEE J. Transl. Eng. Health Med. 2016, 4, 2700111. [Google Scholar] [CrossRef]
- Phillips, A.E.M.; Faghih, M.; Singh, V.K.M.; Olesen, S.S.M.; Kuhlmann, L.M.; Novovic, S.M.; Bick, B.; Hart, P.A.; Ramsey, M.L.; Talukdar, R.; et al. Rationale for and development of the pancreatic quantitative sensory testing consortium to study pain in chronic pancreatitis. Pancreas 2021, 50, 1298–1304. [Google Scholar] [CrossRef]
- Frank, E. A direct experimental study of three systems of spatial vectorcardiography. Circulation 1954, 10, 101–113. [Google Scholar] [CrossRef]
- Frank, E. An accurate, clinically practical system for spatial vectorcardiography. Circulation 1956, 13, 737–749. [Google Scholar] [CrossRef]
- Dower, G. Deriving the La-Lead Electrocardiogram (EASI) Electrodes. J. Electrocardiol. 1988, 21, 182–187. [Google Scholar] [CrossRef]
- Feild, D.Q.; Feldman, C.L.; Horaácçek, B.M. Improved EASI coefficients: Their derivation, values, and performance. J. Electrocardiol. 2002, 35, 23–33. [Google Scholar] [CrossRef]
- Wang, L.; Zhou, X.; Xing, Y.; Yang, M.; Zhang, C. Clustering ECG heartbeat using improved semi-supervised affinity propagation; Clustering ECG heartbeat using improved semi-supervised affinity propagation. IET Softw. 2016, 11, 207–213. [Google Scholar] [CrossRef]
- Francesco, B.; Grazia, B.M.; Emanuele, G.; Valentina, F.; Sara, C.; Chiara, F.; Riccardo, M.; Francesco, F. Linear and Nonlinear Heart Rate Variability Indexes in Clinical Practice. Comput. Math. Methods Med. 2012, 2012, 219080. [Google Scholar] [CrossRef]
- Huikuri, H.V.; Mäkikallio, T.H.; Perkiömäki, J. Measurement of heart rate variability by methods based on nonlinear dynamics. J. Electrocardiol. 2003, 36, 95–99. [Google Scholar] [CrossRef]
- Tapanainen, J.M.; Thomsen, P.E.B.; Køber, L.; Torp-Pedersen, C.; Mäkikallio, T.H.; Still, A.-M.; Lindgren, K.S.; Huikuri, H.V. Fractal analysis of heart rate variability and mortality after an acute myocardial infarction. Am. J. Cardiol. 2002, 90, 347–352. [Google Scholar] [CrossRef]
- Hussain, I.; Park, S.J. Big-ECG: Cardiographic Predictive Cyber-Physical System for Stroke Management. IEEE Access 2021, 9, 123146–123164. [Google Scholar] [CrossRef]
- Hussain, I.; Hossain, A.; Jany, R.; Bari, A.; Uddin, M.; Kamal, A.R.M.; Ku, Y.; Kim, J.-S. Quantitative Evaluation of EEG-Biomarkers for Prediction of Sleep Stages. Sensors 2022, 22, 3079. [Google Scholar] [CrossRef]
- Hussain, I.; Park, S.J. HealthSOS: Real-Time Health Monitoring System for Stroke Prognostics. IEEE Access 2020, 8, 213574–213586. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| ECG-Based Biomarkers | Resting | Cold Pressor | p-Values | |
|---|---|---|---|---|
| HRV | RR intervals (ms) | 800 ± 13 | 799 ± 14 | 0.35 |
| Heartbeat rate (bpm) | 76 ± 1.2 | 76 ± 1.4 | 0.23 | |
| LF (ms2) | 725 ± 128 | 816 ± 185 | 0.81 | |
| HF (ms2) | 712 ± 116 | 893 ± 185 | 0.37 | |
| LF/HF | 1.43 ± 0.3 | 1.04 ± 0.3 | 0.36 | |
| DC (ms) | 14.3 ± 1.3 | 16.1 ± 1.6 | 0.25 | |
| PRD (degree) | 0.38 ± 0.01 | 0.42 ± 0.02 | 0.02 * | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liao, D.; Nedergaard, R.B.; Unnisa, M.; Mahapatra, S.J.; Faghih, M.; Phillips, A.E.; Yadav, D.; Singh, V.K.; Olesen, S.S.; Talukdar, R.; et al. Electrocardiography Assessment of Sympatico–Vagal Balance during Resting and Pain Using the Texas Instruments ADS1299. Bioengineering 2023, 10, 205. https://doi.org/10.3390/bioengineering10020205
Liao D, Nedergaard RB, Unnisa M, Mahapatra SJ, Faghih M, Phillips AE, Yadav D, Singh VK, Olesen SS, Talukdar R, et al. Electrocardiography Assessment of Sympatico–Vagal Balance during Resting and Pain Using the Texas Instruments ADS1299. Bioengineering. 2023; 10(2):205. https://doi.org/10.3390/bioengineering10020205
Chicago/Turabian StyleLiao, Donghua, Rasmus B. Nedergaard, Misbah Unnisa, Soumya J. Mahapatra, Mahya Faghih, Anna E. Phillips, Dhiraj Yadav, Vikesh K. Singh, Søren S. Olesen, Rupjyoti Talukdar, and et al. 2023. "Electrocardiography Assessment of Sympatico–Vagal Balance during Resting and Pain Using the Texas Instruments ADS1299" Bioengineering 10, no. 2: 205. https://doi.org/10.3390/bioengineering10020205