
COVID-19 Detection by Means of ECG, Voice, and X-ray Computerized Systems: A Review


Abstract
:1. Introduction
1.1. Mechanism
1.2. Symptoms
1.3. Laboratory Diagnostic
1.4. Rational for the Review
1.5. Objectives/Questions for the Review to Address
2. Methods
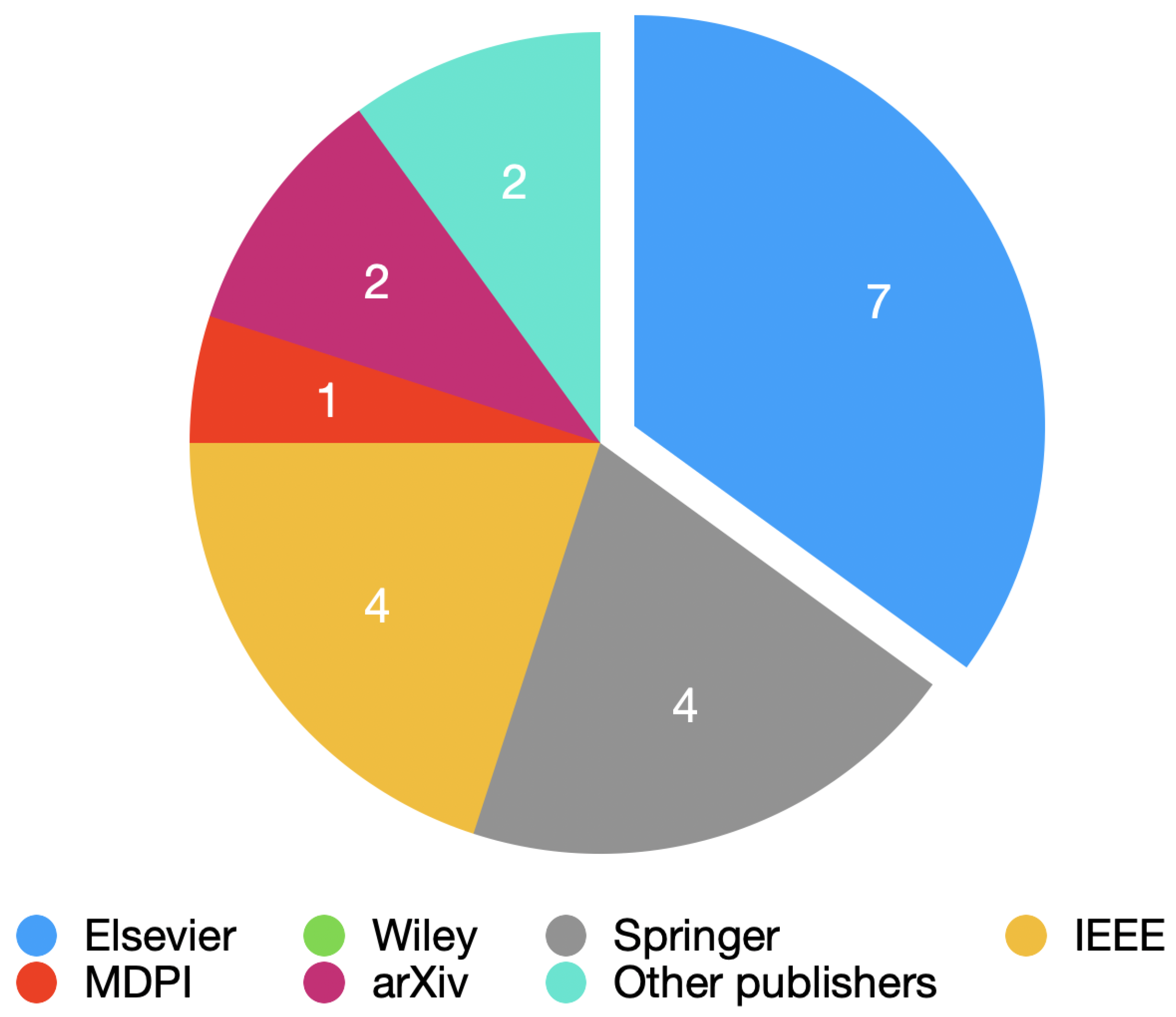
2.1. Document Search
2.2. Search Strategy
2.3. Limitations
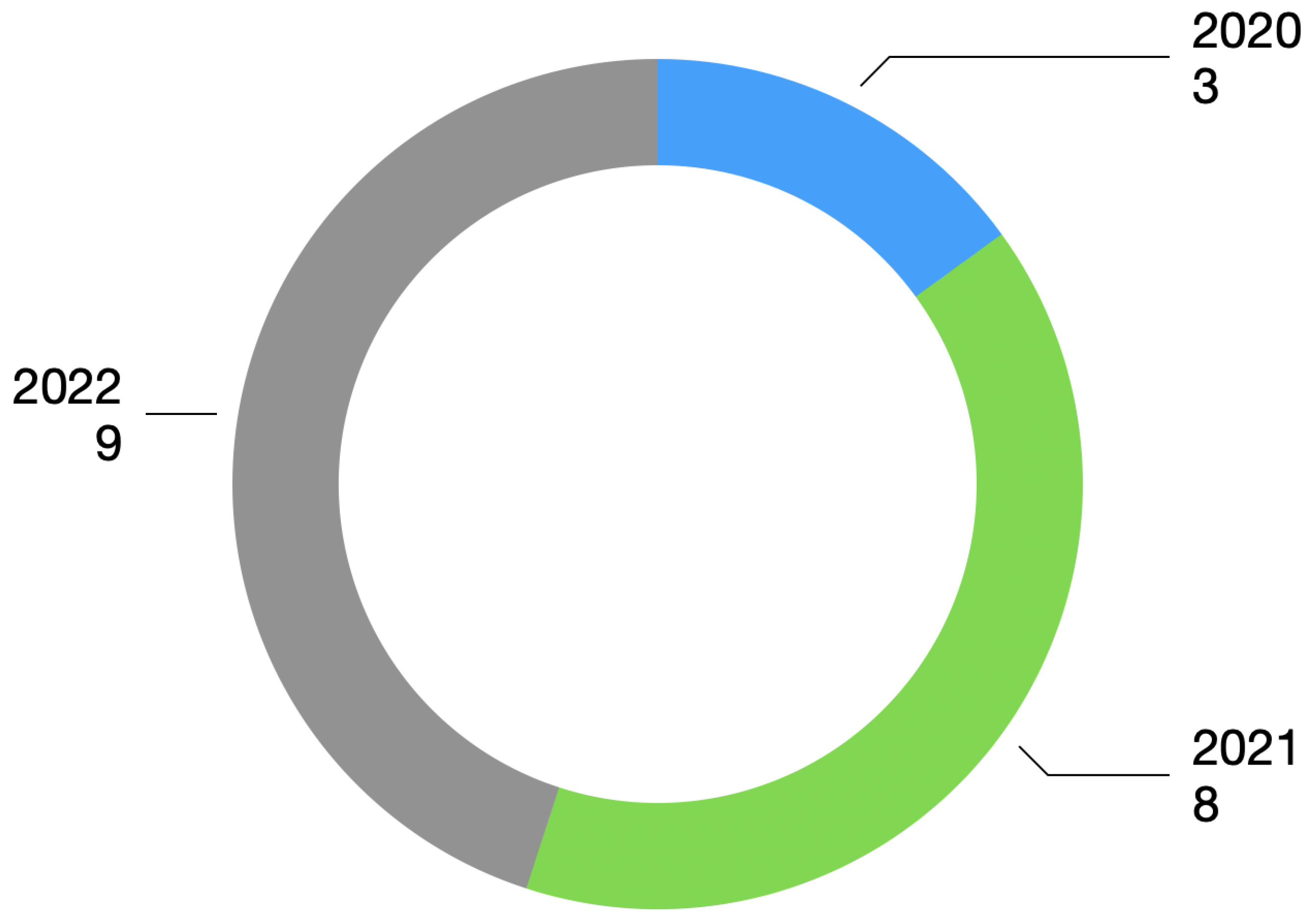
2.4. Year of Publication Present in the Review
3. Results
3.1. COVID-19 Detection Based on ECG Processing
3.2. COVID-19 Detection Based on Voice Processing
3.3. COVID-19 Detection Based on Image Processing
4. Discussion
4.1. ECG Processing
4.2. Voice Processing
4.3. X-ray Processing
4.4. Critical Analysis for the Selected Papers
5. Conclusions
Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 22 August 2022).
- Mehraeen, E.; Alinaghi, S.; Nowroozi, A.; Dadras, O.; Alilou, S.; Shobeiri, P.; Behnezhad, F.; Karimi, A. A systematic review of ECG findings in patients with COVID-19. Indian Heart J. 2020, 72, 500–507. [Google Scholar] [CrossRef]
- Yesudhas, D.; Srivastava, A.; Gromiha, M. COVID-19 outbreak: History, mechanism, transmission, structural studies and therapeutics. Infection 2020, 49, 199–213. [Google Scholar] [CrossRef] [PubMed]
- Hosseini, E.; Kashani, N.; Nikzad, H.; Azadbakht, J.; Bafrani, H.; Kashani, H. The novel coronavirus Disease-2019 (COVID-19): Mechanism of action, detection and recent therapeutic strategies. Virology 2020, 551, 1–9. [Google Scholar] [CrossRef]
- Ciotti, M.; Ciccozzi, M.; Terrinoni, A.; Jiang, W.; Wang, C.; Bernardini, S. The COVID-19 pandemic. Crit. Rev. Clin. Lab. Sci. 2020, 57, 365–388. [Google Scholar] [CrossRef] [PubMed]
- Chinitz, J.; Goyal, R.; Harding, M.; Veseli, G.; Gruberg, L.; Jadonath, R.; Maccaro, P.; Gandotra, P.; Ong, L.; Epstein, L. Bradyarrhythmias in patients with COVID-19: Marker of poor prognosis? Pacing Clin. Electrophysiol. 2020, 43, 1199–1204. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.; Lam, W. Laboratory testing for the diagnosis of COVID-19. Biochem. Biophys. Res. Commun. 2021, 538, 226–230. [Google Scholar] [CrossRef]
- Long, B.; Brady, W.; Bridwell, R.; Ramzy, M.; Montrief, T.; Singh, M.; Gottlieb, M. Electrocardiographic manifestations of COVID-19. Am. J. Emerg. Med. 2021, 538, 96–103. [Google Scholar] [CrossRef]
- COVID-19: Cardiac Manifestations in Adults. Available online: https://www.uptodate.com/contents/covid-19-cardiac-manifestations-in-adults (accessed on 31 October 2022).
- Bergamaschi, L.; D’Angelo, E.; Paolisso, P.; Toniolo, S.; Fabrizio, M.; Angeli, F.; Donati, F.; Magnani, I.; Rinaldi, A.; Bartoli, L.; et al. The value of ECG changes in risk stratification of COVID-19 patients. Ann. Noninvasive Electrocardiol. 2021, 26, e12815. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Chen, L.; Wang, J.; He, X.; Huang, F.; Chen, J.; Yang, X. Electrocardiogram analysis of patients with different types of COVID-19. Ann. Noninvasive Electrocardiol. 2020, 25, e12806. [Google Scholar] [CrossRef]
- Chorin, E.; Dai, M.; Kogan, E.; Wadhwani, L.; Shulman, E.; Nadeau-Routhier, C.; Knotts, R.; Bar-Cohen, R.; Barbhaiya, C.; Aizer, A.; et al. Electrocardiographic risk stratification in COVID-19 patients. Front. Cardiovasc. Med. 2021, 8, 636073. [Google Scholar] [CrossRef]
- Yang, D.; Li, J.; Gao, P.; Chen, T.; Cheng, Z.; Cheng, K.; Deng, H.; Fang, Q.; Yi, C.; Fan, H.; et al. The prognostic significance of electrocardiography findings in patients with coronavirus disease 2019: A retrospective study. Clin. Cardiol. 2021, 44, 963–970. [Google Scholar] [CrossRef]
- Aghajani, M.; Toloui, A.; Aghamohammadi, M.; Pourhoseingholi, A.; Taherpour, N.; Sistanizad, M.; Neishaboori, A.; Asadpoordezaki, Z.; Miri, R. Electrocardiographic findings and in-hospital mortality of COVID-19 patients; a retrospective cohort study. Arch. Acad. Emerg. Med. 2021, 9, e45. [Google Scholar]
- Kaliyaperumal, D.; Bhargavi, K.; Ramaraju, K.; Nair, K.; Ramalingam, S.; Alagesan, M. Electrocardiographic Changes in COVID-19 Patients: A Hospital-based Descriptive Study. Indian J. Crit. Care Med. 2022, 26, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Angeli, F.; Spanevello, A.; Ponti, R.; Visca, D.; Marazzato, J.; Palmiotto, G.; Feci, D.; Reboldi, G.; Fabbri, L.; Verdecchia, P. Electrocardiographic features of patients with COVID-19 pneumonia. Eur. J. Intern. Med. 2020, 78, 101–106. [Google Scholar] [CrossRef]
- Bassiouni, M.; Hegazy, I.; Rizk, N.; El-Dahshan, E.; Salem, A. Automated Detection of COVID-19 Using Deep Learning Approaches with Paper-Based ECG Reports. Circuits Syst. Signal Process. 2022, 41, 5535–5577. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.; Pham, H.; Le, H.; Nguyen, A.; Thanh, N.; Do, C. Detecting COVID-19 from digitized ECG printouts using 1D convolutional neural networks. PLoS ONE 2022, 17, e0277081. [Google Scholar] [CrossRef]
- Shahin, I.; Nassif, A.; Alsabek, M. COVID-19 Electrocardiograms Classification using CNN Models. In Proceedings of the 2021 14th International Conference on Developments in eSystems Engineering (DeSE), Sharjah, United Arab Emirates, 7–10 December 2021. [Google Scholar]
- Attallah, O. ECG-BiCoNet: An ECG-based pipeline for COVID-19 diagnosis using Bi-Layers of deep features integration. Comput. Biol. Med. 2022, 142, 105210. [Google Scholar] [CrossRef]
- Sobahi, N. Attention-based 3D CNN with residual connections for efficient ECG-based COVID-19 detection. Comput. Biol. Med. 2022, 143, 105335. [Google Scholar] [CrossRef]
- Rahman, T. COV-ECGNET: COVID-19 detection using ECG trace images with deep convolutional neural network. Health Inf. Sci. Syst. 2022, 10, 1. [Google Scholar] [CrossRef]
- Heart Problems after COVID-19. Available online: https://www.hopkinsmedicine.org/health/conditions-and-diseases/coronavirus/heart-problems-after-covid19 (accessed on 25 October 2022).
- Heart Rate Variability Disturbances and Biofeedback Treatment in COVID-19 Survivors. Available online: https://www.escardio.org/Journals/E-Journal-of-Cardiology-Practice/Volume-21/heart-rate-variability-disturbances-and-biofeedback-treatment-in-covid-19-surviv (accessed on 25 October 2022).
- Mishra, T.; Wang, M.; Metwally, A.; Bogu, G.; Brooks, A.; Bahmani, A.; Alavi, A.; Celli, A.; Higgs, E.; Dagan-Rosenfeld, O.; et al. Early detection of COVID-19 using a smartwatch. medRxiv 2020, in press. [Google Scholar]
- Ponomarev, A.; Tyapochkin, K.; Surkova, E.; Smorodnikova, E.; Pravdin, P. Heart Rate Variability as a Prospective Predictor of Early COVID-19 Symptoms. medRxiv 2021, in press. [Google Scholar]
- Hasty, F.; Garcia, G.; Dávila, H.; Wittels, S.; Hendricks, S.; Chong, S. Heart Rate Variability as a Possible Predictive Marker for Acute Inflammatory Response in COVID-19 Patients. Mil. Med. 2021, 186, e34–e38. [Google Scholar] [CrossRef] [PubMed]
- Smilowitz, N.; Kunichoff, D.; Garshick, M.; Shah, B.; Pillinger, M.; Hochman, J.; Berger, J. C-reactive protein and clinical outcomes in patients with COVID-19. Eur. Heart J. 2021, 42, 2270–2279. [Google Scholar] [CrossRef]
- Hassan, A.; Shahin, I.; Alsabek, M. COVID-19 Detection System using Recurrent Neural Networks. In Proceedings of the 2020 International Conference on Communications, Computing, Cybersecurity, and Informatics (CCCI), Sharjah, United Arab Emirates, 3–5 November 2020; pp. 1–5. [Google Scholar]
- Diagnosing Disease by Voice. Available online: https://www.pfizer.com/news/articles/diagnosing_disease_by_voice (accessed on 24 October 2022).
- COVID-19 Lung Damage. Available online: https://www.hopkinsmedicine.org/health/conditions-and-diseases/coronavirus/what-coronavirus-does-to-the-lungs (accessed on 24 October 2022).
- Deshpande, G.; Schuller, B. An overview on audio, signal, speech, & language processing for COVID-19. arXiv 2020, arXiv:2005.08579. [Google Scholar]
- Feng, K.; He, F.; Steinmann, J.; Demirkiran, I. Deep-learning Based Approach to Identify COVID-19. In Proceedings of the SoutheastCon 2021, Atlanta, GA, USA, 10–13 March 2021; pp. 1–4. [Google Scholar]
- Despotovic, V. Detection of COVID-19 from voice, cough and breathing patterns: Dataset and preliminary results. Comput. Biol. Med. 2021, 138, 104944. [Google Scholar] [CrossRef]
- Tena, A.; Clarià, F.; Solsona, F. Automated detection of COVID-19 cough. Biomed. Signal Process. Control 2022, 71, 103175. [Google Scholar] [CrossRef]
- Mouawad, P.; Dubnov, T.; Dubnov, S. Robust detection of COVID-19 in cough sounds. SN Comput. Sci. 2021, 2, 34. [Google Scholar] [CrossRef] [PubMed]
- Dash, T.; Mishra, S.; Panda, G.; Satapathy, S. Detection of COVID-19 from speech signal using bio-inspired based cepstral features. Pattern Recognit. 2021, 117, 107999. [Google Scholar] [CrossRef]
- Atmaja, B.; Zanjabila, S.; Sasou, A. Cross-dataset COVID-19 Transfer Learning with Cough Detection, Cough Segmentation, and Data Augmentation. arXiv 2022, arXiv:2210.05843. [Google Scholar]
- Imran, A.; Posokhova, I.; Qureshi, H.; Masood, U.; Riaz, M.; Ali, K.; John, C.; Hussain, M.; Nabeel, M. AI4COVID-19: AI enabled preliminary diagnosis for COVID-19 from cough samples via an app. Inform. Med. Unlocked 2020, 20, 100378. [Google Scholar] [CrossRef]
- Verde, L.; Pietro, G.; Ghoneim, A.; Alrashoud, M.; Al-Mutib, K.; Sannino, G. Exploring the Use of Artificial Intelligence Techniques to Detect the Presence of Coronavirus COVID-19 Through Speech and Voice Analysis. IEEE Access 2021, 9, 65750–65757. [Google Scholar] [CrossRef]
- Silva, G.; Batista, P.; Rodrigues, P.M. COVID-19 activity screening by a smart-data-driven multi-band voice analysis. J. Voice 2022, in press. [Google Scholar] [CrossRef]
- Abdallah, Y.; Alqahtani, T. Research in Medical Imaging Using Image Processing Techniques. In Medical Imaging—Principles and Applications; IntechOpen: London, UK, 2019. [Google Scholar]
- Tello-Mijares, S.; Woo, L. Computed Tomography Image Processing Analysis in COVID-19 Patient Follow-Up Assessment. J. Healthc. Eng. 2021, 2021, 8869372. [Google Scholar] [CrossRef] [PubMed]
- Salman, F.; Abu-Naser, S.; Alajrami, E.; Abu-Nasser, B.; Alashqar, B. COVID-19 detection using artificial intelligence. Int. J. Acad. Eng. Res. 2020, 4, 18–25. [Google Scholar]
- DeGrave, A.; Janizek, J.; Lee, S. AI for radiographic COVID-19 detection selects shortcuts over signal. Nat. Mach. Intell. 2021, 3, 610–619. [Google Scholar] [CrossRef]
- Öztaş, A.; Boncukcu, D.; Ozteke, E.; Demir, M.; Mirici, A.; Mutlu, P. Covid19 Diagnosis: Comparative Approach Between Chest X-ray and Blood Test Data. In Proceedings of the 2021 6th International Conference on Computer Science and Engineering (UBMK), Ankara, Turkey, 15–17 September 2021; Volume 6, pp. 472–477. [Google Scholar]
- Wu, C.; Khishe, M.; Mohammadi, M.; Karim, S.; Rashid, T. Evolving deep convolutional neutral network by hybrid sine–cosine and extreme learning machine for real-time COVID19 diagnosis from X-ray images. Soft Comput 2021, 25, 1–20. [Google Scholar] [CrossRef]
- Al-Falluji, R.; Katheeth, Z.; Alathari, B. Automatic detection of COVID-19 using chest X-ray images and modified ResNet18-based convolutional neural networks. Comput. Mater. Contin. 2021, 66, 1301–1313. [Google Scholar]
- Sethy, P.; Behera, S. Detection of coronavirus disease (COVID-19) based on deep features. IJMEMS 2020, 5, 643–651. [Google Scholar]
- Fang, Z.; Ren, J.; MacLellan, C.; Li, H.; Zhao, H.; Hussain, A.; Fortino, G. A Novel Multi-Stage Residual Feature Fusion Network for Detection of COVID-19 in Chest X-ray Images. IEEE Trans. Mol. Biol. Multi-Scale Commun. 2022, 8, 17–27. [Google Scholar] [CrossRef]
- Yousri, D.; Elaziz, M.; Abualigah, L.; Oliva, D.; Al-qaness, M.; Ewees, A. COVID-19 X-ray images classification based on enhanced fractional-order cuckoo search optimizer using heavy-tailed distributions. Appl. Soft Comput. 2020, 101, 107052. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Ref. | Dataset | Data Augmentation | Source | Features | Machine Learning Classifier | Cross-Validation |
|---|---|---|---|---|---|---|
| [17] | ECG images dataset of cardiac and COVID-19 patients (1937 records) | Yes | ECG | Feature extraction from ECGConvnet (transfer learning) | ECGConvnet | Yes |
| [18] | ECG images dataset of cardiac and COVID-19 patients (1937 records) | No | ECG | Feature extraction from SEResNet18 (transfer learning) | SEResNet18 | Yes |
| [19] | ECG images dataset of cardiac and COVID-19 patients (1937 records) | Yes | ECG | Feature extraction with VGG16 pre-trained (transfer learning) | CNN VGG16 | Yes |
| [20] | ECG images dataset of cardiac and COVID-19 patients (1937 records) | Yes | ECG | ResNet-50, Inception V3, Xception, InceptionResNet and DenseNet-201 pre-tained feature extraction (transfer learning) | ECG-BiCoNet (CNN) | Yes |
| [21] | ECG images dataset of cardiac and COVID-19 patients (1937 records) | Yes | ECG | Feature extraction from 3D CNN (transfer learning) | 3D CNN | Yes |
| [22] | ECG images dataset of cardiac and COVID-19 patients (1937 records) | Yes | ECG | Feature extraction from InceptionV3 pre-trained (transfer learning) | CNN | Yes |
| [35] | UdL+UC+Coswara+Virufy+Pertussis (813 samples) | Yes | Voice | Energy, instantaneous frequency, instantaneous frequency peak, Shannon entropy, instantaneous entropy, spectral information entropy, spectral information, and kurtosis | Random Forest | Yes |
| [36] | Corona Voice Detect project with Voca.ai (3415 samples) | Yes | Voice | Mel frequency cepstral coefficients | XGBoost | Yes |
| [37] | Crowd-sourced Respiratory Sound Data | Yes | Voice | C-19CC | SVM | Yes |
| [38] | Coswara + COUGHVID + ComPare-CCS (2026 samples) | Yes | Voice | Log Mel Spectrogram | CNN14 | No |
| [39] | ESC-50 (5435 samples) | No | Voice | Mel frequency cepstral coefficients | Deep Transfer Learning-based Multi Class classifier | Yes |
| [40] | Coswara database (1027 samples) | No | Voice | Fundamental frequency, jitter and shimmer, harmonic to noise ratio, mel-frequency cepstral coefficients, first and second derivatives of cepstral coefficient, spectral centroid and spectral Roll-off | SVM | No |
| [41] | Coswara database (909 samples) | No | Voice | Energy, entropies, correlation dimension, detrended fluctuation analysis, Lyapunov Exponent and fractal dimensions | XGBoost | Yes |
| [46] | Covid chestxray dataset + Chex Pert dataset (5370 samples) | No | X-ray | Feature extraction from Resnet18 pre-trained (transfer learning) | Resnet18 | Yes |
| [47] | Covid chestxray dataset + Chex Pert dataset (5184 samples) | Yes | X-ray | Feature extraction from LetNet-5 (transfer learning) | Extreme Learning Machine | No |
| [44] | Covid chestxray dataset + Kaggle repository + Open-i repository (160 samples) | Yes | X-ray | Deep feature extraction based on VGG16, ResNet50 and InceptionV3 (transfer learning) | CNN Inceptionv3 | No |
| [48] | Covid chestxray dataset + Labeled Optical Coherence Tomography + Chest X-ray Images for Classification | Yes | X-ray | Feature extraction from CNN (transfer learning) | Modified ResNet-18 | No |
| [49] | Covid chestxray dataset + Kaggle repository (50 samples) | Yes | X-ray | Feature extracted by CNN ResNet50 (transfer learning) | SVM | No |
| [50] | Covidx Dataset (14,003 samples) | Yes | X-ray | Feature extracted by ResNet-18 (transfer learning) | MSRCovXNet (multi-stage residual network) | Yes |
| [51] | COVID-19 CHEST X-RAY DATABASE+ COVID-19 Database + COVID-Chestxray Database + ChestX-ray8 + chest-xray-pneumonia (1560 samples) | No | X-ray | Contrast, correlation, energy, entropy, homogeneity, Mittag-Leffler distribution, Pareto distribution, and Cauchy distribution | KNN | No |
| Ref. | Accuracy | F1-Score | Sensitivity | Specificity |
|---|---|---|---|---|
| [17] | 99.74% | 99.70% | 99.70% | ≈100% |
| [18] | 83.17% | 85.38% | 84.81% | 86.28% |
| [19] | 81.39% | N/A | N/A | N/A |
| [20] | 91.73% | 91.80% | 91.70% | 95.90% |
| [21] | 92.00% | 92.03% | 95.99% | 92.00% |
| [22] | 97.83% | 97.82% | 97.83% | 98.86% |
| [35] | 85.53% | 85.58% | 85.96% | 85.09% |
| [36] | 99.00% | 69.00% | 70.00% | N/A |
| [37] | 85.70% | N/A | N/A | N/A |
| [38] | 88.19% | N/A | N/A | N/A |
| [39] | 92.64% | 92.66% | 92.64% | 97.55% |
| [40] | 97.07% | 82.35% | 93.33% | 97.37% |
| [41] | 98.46% | N/A | N/A | N/A |
| [46] | ≈98% | N/A | N/A | N/A |
| [47] | 98.83% | N/A | N/A | N/A |
| [44] | 100% | 100% | 100% | 100% |
| [48] | 96.73% | N/A | N/A | N/A |
| [49] | 95.38% | 95.52% | 97.29% | 93.47% |
| [50] | 82.20% | N/A | N/A | N/A |
| [51] | 100% | N/A | N/A | N/A |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ribeiro, P.; Marques, J.A.L.; Rodrigues, P.M. COVID-19 Detection by Means of ECG, Voice, and X-ray Computerized Systems: A Review. Bioengineering 2023, 10, 198. https://doi.org/10.3390/bioengineering10020198
Ribeiro P, Marques JAL, Rodrigues PM. COVID-19 Detection by Means of ECG, Voice, and X-ray Computerized Systems: A Review. Bioengineering. 2023; 10(2):198. https://doi.org/10.3390/bioengineering10020198
Chicago/Turabian StyleRibeiro, Pedro, João Alexandre Lobo Marques, and Pedro Miguel Rodrigues. 2023. "COVID-19 Detection by Means of ECG, Voice, and X-ray Computerized Systems: A Review" Bioengineering 10, no. 2: 198. https://doi.org/10.3390/bioengineering10020198