


TARTESSUS: A Customized Electrospun Drug Delivery System Loaded with Irinotecan for Local and Sustained Chemotherapy Release in Pancreatic Cancer
 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials and Reagents for Membrane Fabrication
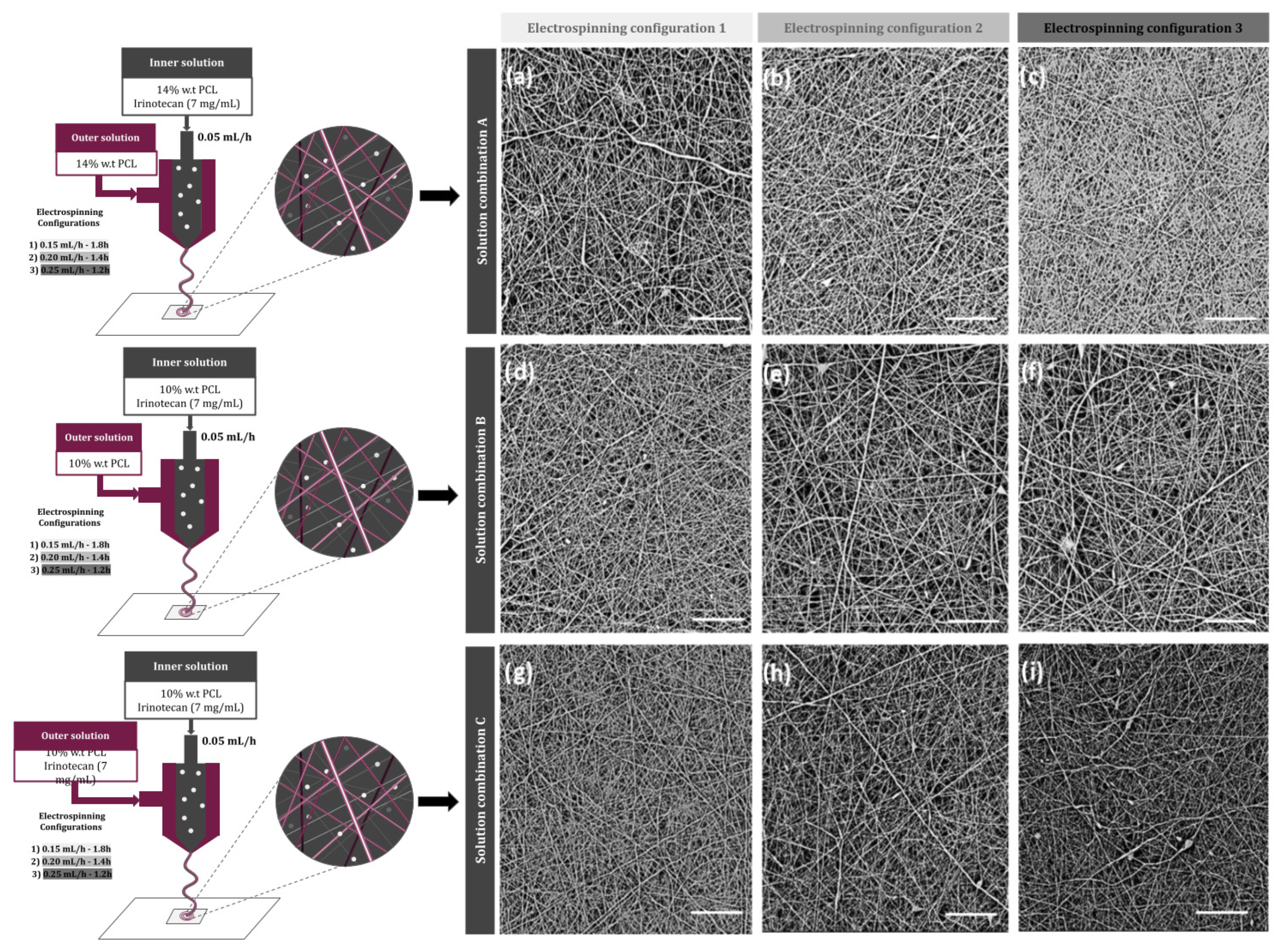
2.2. Drug-Loaded Membrane Fabrication (TARTESSUS)
2.3. Characterization of Nanofibers
2.3.1. Surface Morphology
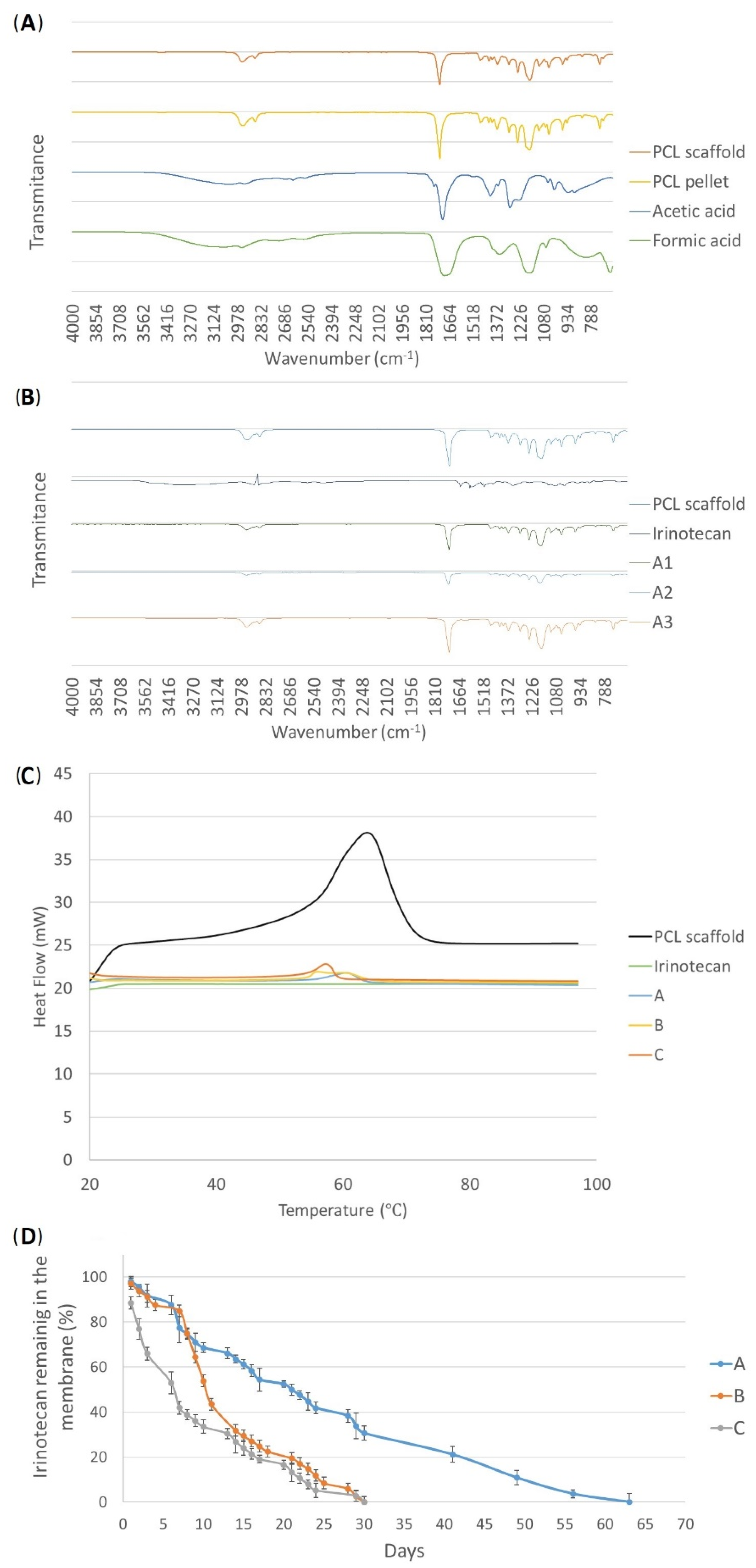
2.3.2. Solvent Remanence
2.3.3. Drug Loading and In Vitro Drug Release
2.4. Determination of Drug Dose per Membrane Surface
2.5. D Cell Culture Conditions
2.6. D Cell Culture
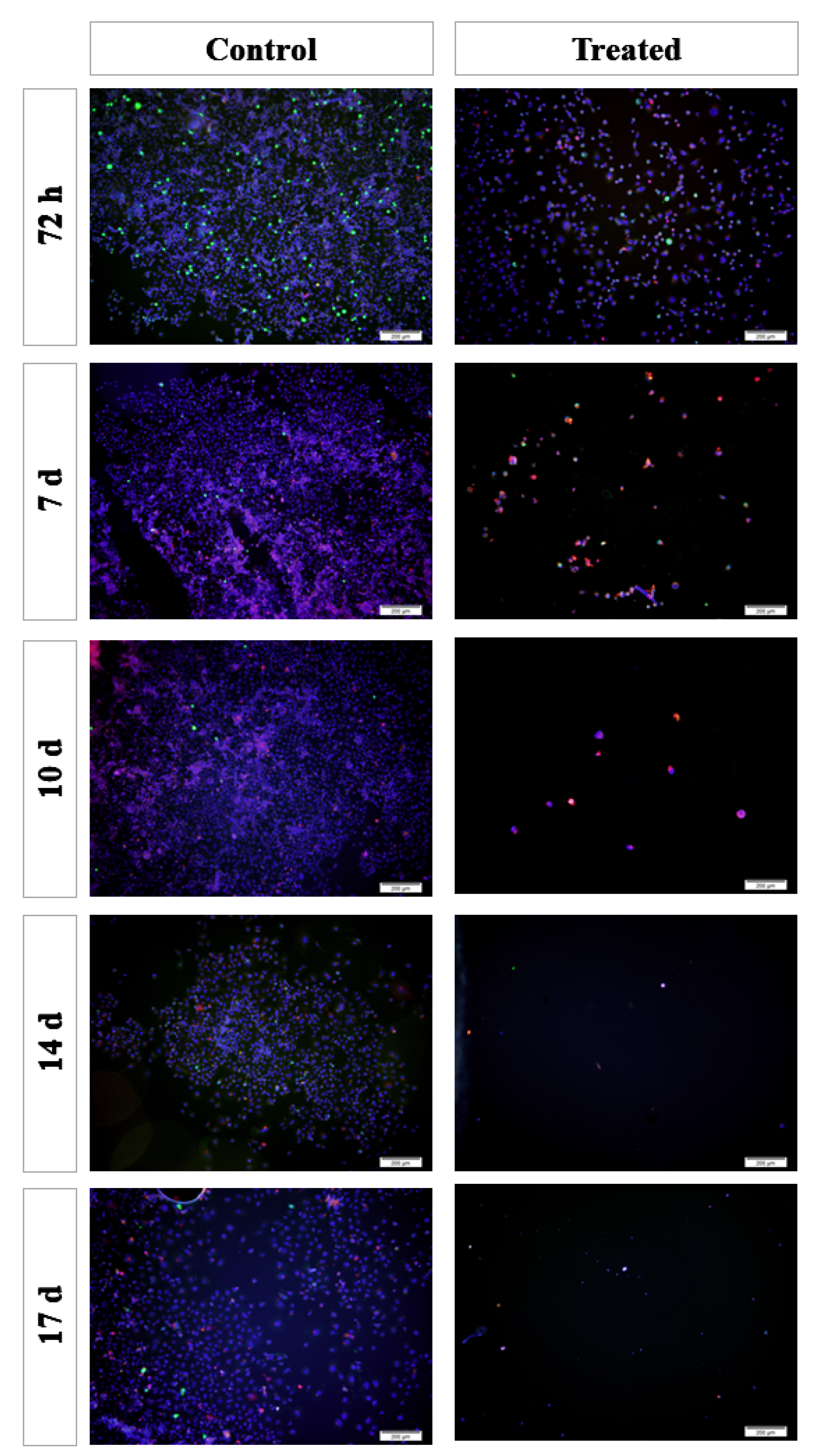
2.7. Analyses of In Vitro Proliferation and Apoptosis of Pancreatic Cancer Cells
2.8. Statistical Analysis
3. Results
3.1. Membrane Characterization
3.2. Drug Release
3.3. D Cell Cultures
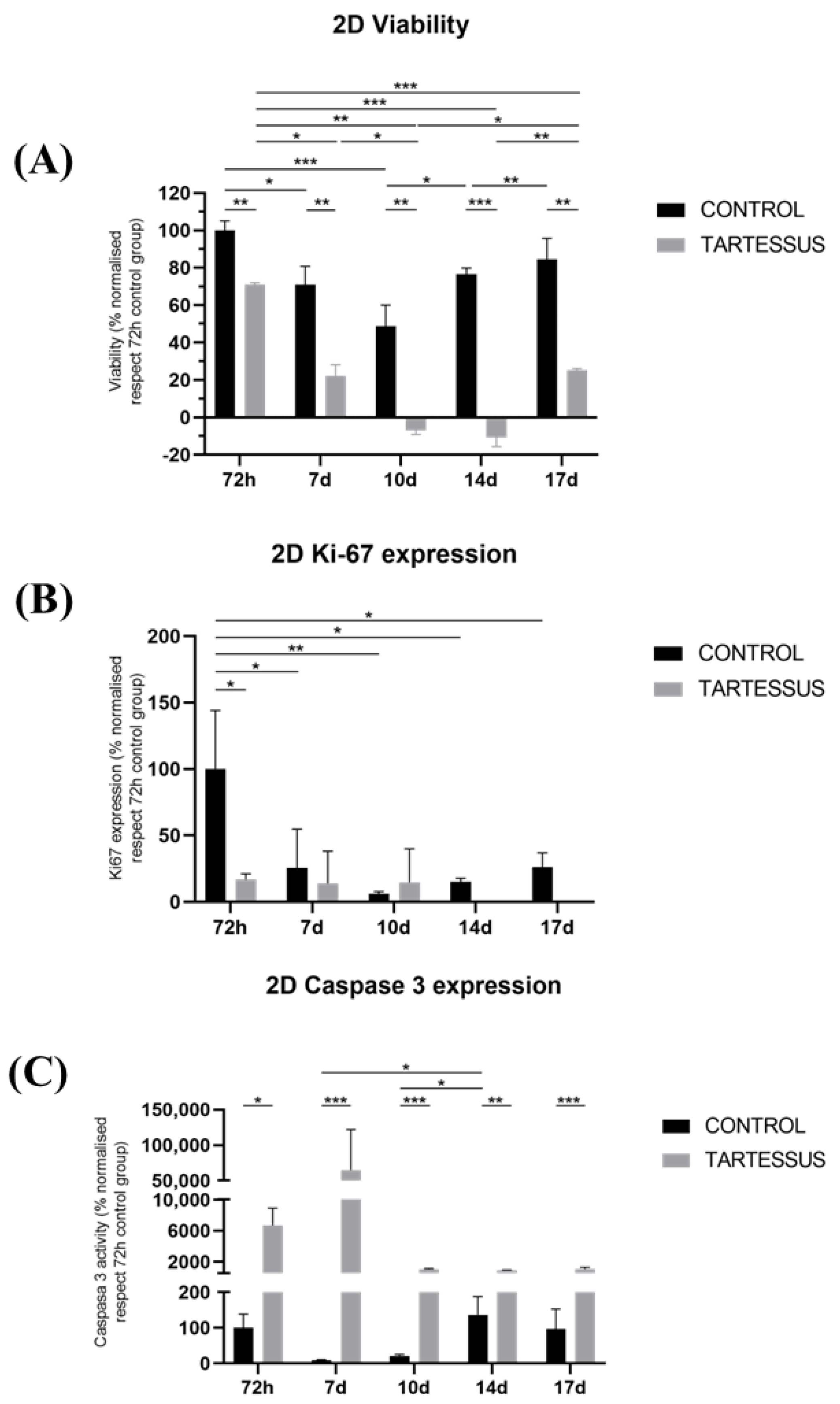
3.3.1. D Cell Viability
3.3.2. D Cell Proliferation
3.3.3. D Cell Death
3.4. D Cell Culture
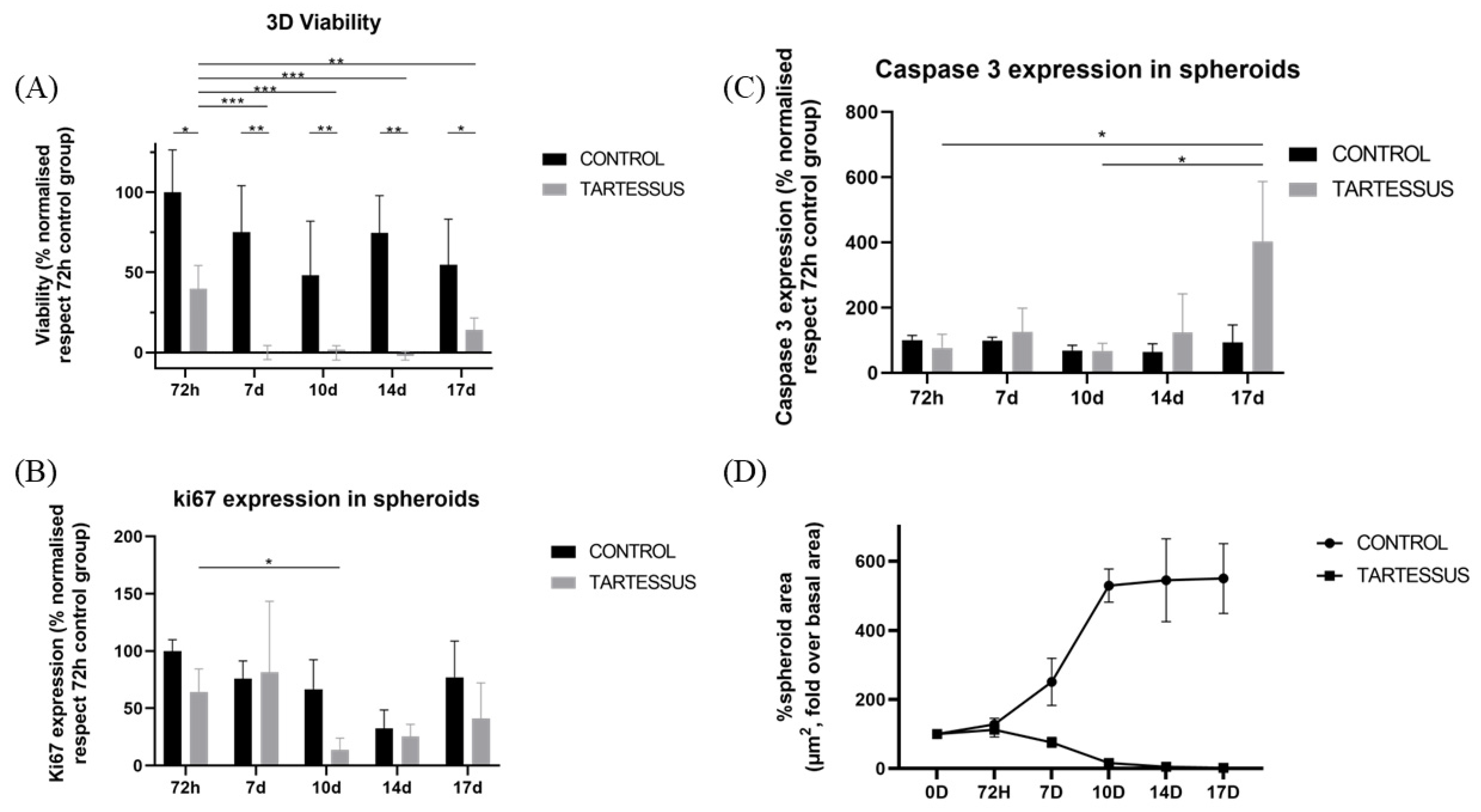
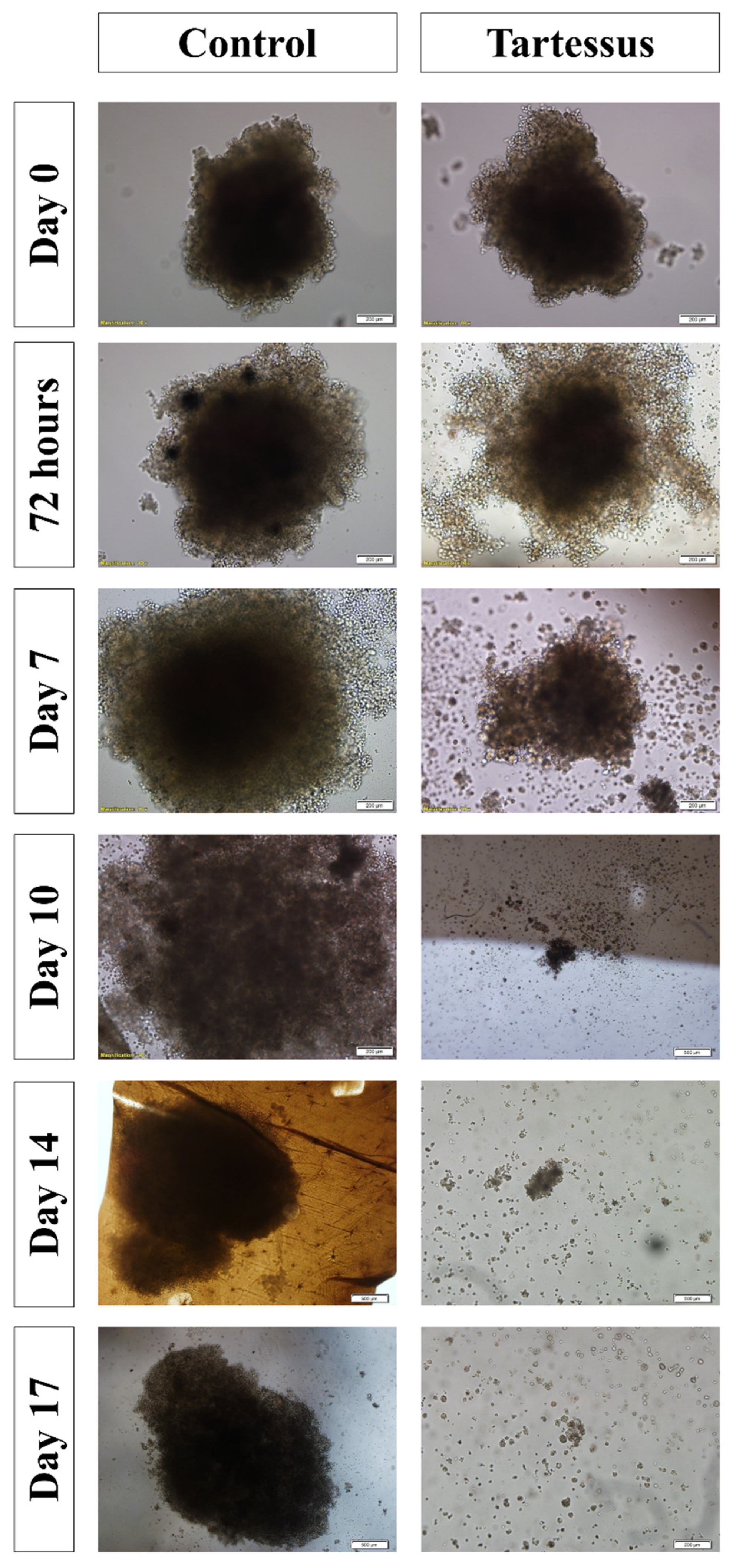
3.4.1. D Cell Viability
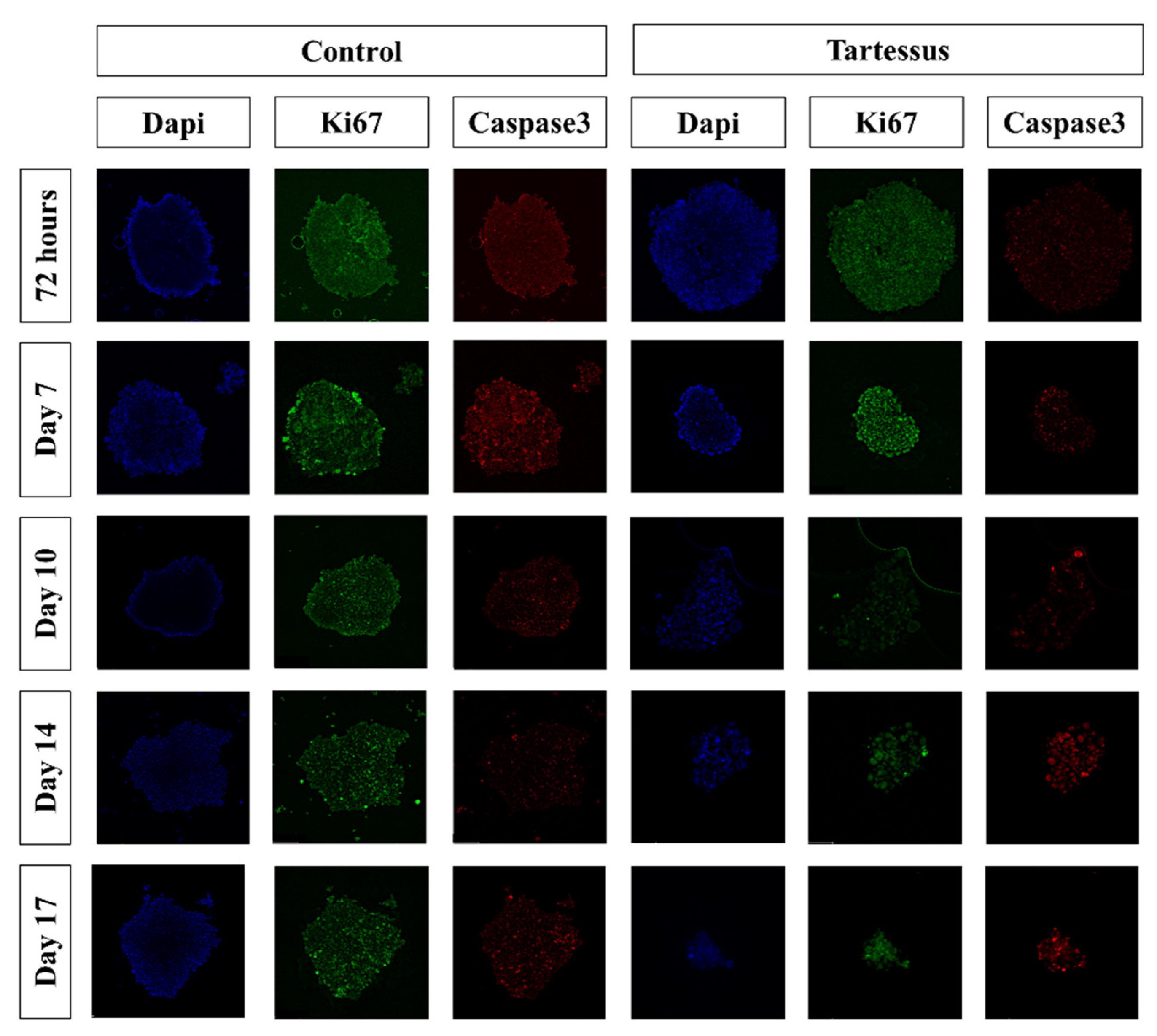
3.4.2. D Cell Proliferation
3.4.3. D Cell Death
3.4.4. Spheroid Size
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Pancreatic Cancer: Types of Treatment. Available online: https://www.cancer.net/cancer-types/pancreatic-cancer (accessed on 26 December 2022).
- Padillo-Ruiz, J.; Suarez, G.; Pereira, S.; Calero-Castro, F.J.; Tinoco, J.; Marin, L.; Bernal, C.; Cepeda-Franco, C.; Alamo, J.M.; Almoguera, F.; et al. Circulating tumor cells enumeration from the portal vein for risk stratification in early pancreatic cancer patients. Cancers 2021, 13, 6153. [Google Scholar] [CrossRef]
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Cancer statistics for the year 2020: An overview. Int. J. Cancer 2021, 149, 778–789. [Google Scholar] [CrossRef]
- Bu, L.-L.; Yan, J.; Wang, Z.; Ruan, H.; Chen, Q.; Gunadhi, V.; Bell, R.B.; Gu, Z. Advances in drug delivery for post-surgical cancer treatment. Biomaterials 2019, 219, 119182. [Google Scholar] [CrossRef] [PubMed]
- Wade, S.J.; Zuzic, A.; Foroughi, J.; Talebian, S.; Aghmesheh, M.; Moulton, S.E.; Vine, K.L. Preparation and in vitro assessment of wet-spun gemcitabine-loaded polymeric fibers: Towards localized drug delivery for the treatment of pancreatic cancer. Pancreatology 2017, 17, 795–804. [Google Scholar] [CrossRef]
- Conroy, T.; Desseigne, F.; Ychou, M.; Bouché, O.; Guimbaud, R.; Bécouarn, Y.; Adenis, A.; Raoul, J.-L.; Gourgou-Bourgade, S.; de la Fouchardière, C.; et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N. Engl. J. Med. 2011, 364, 1817–1825. [Google Scholar] [CrossRef]
- Xia, G.; Zhang, H.; Cheng, R.; Wang, H.; Song, Z.; Deng, L.; Huang, X.; Santos, H.A.; Cui, W. Localized controlled delivery of gemcitabine via microsol electrospun fibers to prevent pancreatic cancer recurrence. Adv. Healthc. Mater. 2018, 7, 1800593. [Google Scholar] [CrossRef]
- Zhan, Q.; Shen, B.; Deng, X.; Chen, H.; Jin, J.; Zhang, X.; Peng, C.; Li, H. Drug-eluting scaffold to deliver chemotherapeutic medication for management of pancreatic cancer after surgery. Int. J. Nanomed. 2013, 8, 2465–2472. [Google Scholar] [CrossRef]
- Kumar, S.; Rastogi, A.; Rai, A.K.; Singh, S. Novel drug delivery system for anticancer drug: A review. Int. J. Pharmtech. Res. 2012, 4, 542–553. [Google Scholar]
- Tiwari, G.; Tiwari, R.; Birendra, S.; Bhati, L.; Pandey, S.; Pandey, P.; Bannerjee, S.K. Drug delivery systems: An updated review. Int. J. Pharm. Investig. 2012, 2, 1. [Google Scholar] [CrossRef]
- Kong, X.; Feng, M.; Wu, L.; He, Y.; Mao, H.; Gu, Z. Biodegradable gemcitabine-loaded microdevice with sustained local drug delivery and improved tumor recurrence inhibition abilities for postoperative pancreatic tumor treatment. Drug. Deliv. 2022, 29, 1595–1607. [Google Scholar] [CrossRef] [PubMed]
- Yi, H.J.; Choi, Y.J.; Kang, K.S.; Hong, J.M.; Pati, R.G.; Park, M.N.; Shim, I.K.; Lee, C.M.; Kim, S.C.; Cho, D.W. A 3D-printed local drug delivery patch for pancreatic cancer growth suppression. J. Control. Release 2016, 238, 231–241. [Google Scholar] [CrossRef]
- Shim, I.K.; Yi, H.J.; Yi, H.-G.; Lee, C.M.; Lee, Y.N.; Choi, Y.-J.; Jeong, S.-Y.; Jun, E.; Hoffman, R.M.; Cho, D.-W.; et al. Locally-applied 5-fluorouracil-loaded slow-release patch prevents pancreatic cancer growth in an orthotopic mouse model. Oncotarget 2017, 8, 40140–40151. [Google Scholar] [CrossRef]
- Shabana, A.M.; Kambhampati, S.P.; Hsia, R.C.; Kannan, R.M.; Kokkoli, E. Thermosensitive and biodegradable hydrogel encapsulating targeted nanoparticles for the sustained co-delivery of gemcitabine and paclitaxel to pancreatic cancer cells. Int. J. Pharm. 2021, 593, 120139. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Benitez, R.; Benz, D.; Wu, Y.; Wu, X.; Chen, S.; Cruise, G.M. New interventional treatment model for pancreatic neoplasms using gemcitabine-eluting hydrogel devices: In vitro and in vivo results. Cardiovasc. Intervent. Radiol. 2017, 40, 1246–1254. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Valdivieso, J.; Garcia-Sampedro, A.; Hall, A.R.; Girotti, A.; Arias, F.J.; Pereira, S.P.; Acedo, P. Smart nanoparticles as advanced anti-akt kinase delivery systems for pancreatic cancer therapy. ACS Appl. Mater. Interfaces 2021, 13, 55790–55805. [Google Scholar] [CrossRef]
- Madamsetty, V.S.; Pal, K.; Keshavan, S.; Caulfield, T.R.; Dutta, S.K.; Wang, E.; Fadeel, B.; Mukhopadhyay, D. Development of multi-drug loaded PEGylated nanodiamonds to inhibit tumor growth and metastasis in genetically engineered mouse models of pancreatic cancer. Nanoscale 2019, 11, 22006–22018. [Google Scholar] [CrossRef]
- Atiyah, N.A.; Albayati, T.M.; Atiya, M.A. Functionalization of mesoporous MCM-41 for the delivery of curcumin as an anti-inflammatory therapy. Adv. Powder Technol. 2022, 33, 103417. [Google Scholar] [CrossRef]
- Atiyah, N.A.; Albayati, T.M.; Atiya, M.A. Interaction behavior of curcumin encapsulated onto functionalized SBA-15 as an efficient carrier and release in drug delivery. J. Mol. Struct. 2022, 1260, 132879. [Google Scholar] [CrossRef]
- Dasgupta, D.; Das, M.; Thakore, S.; Patel, A.; Kumar, S.; Seshadri, S. Development of a controlled sustainable anticancer drug delivery nanosystem comprising doxorubicin and functionalized MCM-48. J. Drug Deliv. Sci. Technol. 2022, 72, 103419. [Google Scholar] [CrossRef]
- Chi, H.Y.; Chan, V.; Li, C.; Hsieh, J.H.; Lin, P.H.; Tsai, Y.-H.; Chen, Y. Fabrication of polylactic acid/paclitaxel nano fibers by electrospinning for cancer therapeutics. BMC Chem. 2020, 14, 63. [Google Scholar] [CrossRef] [PubMed]
- Jun, E.; Kim, S.C.; Lee, C.M.; Oh, J.; Lee, S.; Shim, I.K. Synergistic effect of a drug loaded electrospun patch and systemic chemotherapy in pancreatic cancer xenograft. Sci. Rep. 2017, 7, 12381. [Google Scholar] [CrossRef] [PubMed]
- Goonoo, N.; Bhaw-Luximon, A.; Jhurry, D. Drug loading and release from electrospun biodegradable nanofibers. J. Biomed. Nanotechnol. 2014, 10, 2173–2199. [Google Scholar] [CrossRef]
- Subbiah, T.; Bhat, G.S.; Tock, R.W.; Parameswaran, S.; Ramkumar, S.S. Electrospinning of nanofibers. J. Appl. Polym. Sci. 2005, 96, 557–569. [Google Scholar] [CrossRef]
- Mitxelena-Iribarren, O.; Riera-Pons, M.; Pereira, S.; Calero-Castro, F.J.; Castillo Tuñón, J.M.; Padillo-Ruiz, J.; Mujika, M.; Arana, S. Drug-loaded PCL electrospun nanofibers as anti-pancreatic cancer drug delivery systems. Polymer. Bulletin 2022. [Google Scholar] [CrossRef]
- Ma, W.; Cao, W.; Lu, T.; Xiong, R.; Huang, C. Multifunctional nanofibrous membrane fabrication by a sacrifice template strategy for efficient emulsion oily wastewater separation and water purification. J. Environ. Chem. Eng. 2022, 10, 108908. [Google Scholar] [CrossRef]
- Singh, A.P.; Biswas, A.; Shukla, A.; Maiti, P. Targeted therapy in chronic diseases using nanomaterial-based drug delivery vehicles. Signal. Transduct. Target Ther. 2019, 4, 33. [Google Scholar] [CrossRef]
- Iqbal, S.; Rashid, M.H.; Arbab, A.S.; Khan, M. Encapsulation of anticancer drugs (5-fluorouracil and paclitaxel) into polycaprolactone (PCL) nanofibers and in vitro testing for sustained and targeted therapy. J. Biomed. Nanotechnol. 2017, 13, 355–366. [Google Scholar] [CrossRef]
- Habibi Jouybari, M.; Hosseini, S.; Mahboobnia, K.; Boloursaz, L.A.; Moradi, M.; Irani, M. Simultaneous controlled release of 5-FU, DOX and PTX from chitosan/PLA/5-FU/g-C3N4-DOX/g-C3N4-PTX triaxial nanofibers for breast cancer treatment in vitro. Colloids Surf. B Biointerfaces 2019, 179, 495–504. [Google Scholar] [CrossRef]
- Poursharifi, N.; Semnani, D.; Soltani, P.; Amanpour, S. Designing a novel and versatile multi-layered nanofibrous structure loaded with MTX and 5-FU for the targeted delivery of anticancer drugs. Polym. Degrad. Stab. 2020, 179, 109275. [Google Scholar] [CrossRef]
- Bao, X.; Wu, J.; Kim, S.; LoRusso, P.; Li, J. Pharmacometabolomics reveals irinotecan mechanism of action in cancer patients. J. Clin. Pharmacol. 2019, 59, 20–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, X.; Situ, A.; Kang, Y.; Rose Villabroza, K.; Liao, Y.; Chang, C.H.; Donahue, T.; Nel, A.E.; Meng, H. Supplementary materials irinotecan delivery by lipid-coated mesoporous silica nanoparticles show improved efficacy and safety over liposomes for pancreatic cancer. ACS Nano 2016, 10, 2702–2715. [Google Scholar] [CrossRef]
- Sastre, R.L.; Blanco, M.D.; Teijón, C.; Olmo, R.; Teijón, J.M. Preparation and characterization of 5-fluorouracil-loaded poly(ε-caprolactone) microspheres for drug administration. Drug Dev. Res. 2004, 63, 41–53. [Google Scholar] [CrossRef]
- Zhang, L.; Zhou, J.; Yan, Y.; Zhou, X.; Zhou, Q.; Du, R.; Hu, S.; Ge, W.; Huang, Y.; Xu, H.; et al. Excipient-free nanodispersion of 7-ethyl-10-hydroxycamptothecin exerts potent therapeutic effects against pancreatic cancer cell lines and patient-derived xenografts. Cancer Lett. 2019, 465, 36–44. [Google Scholar] [CrossRef]
- Piña, R.; Santos-Díaz, A.I.; Orta-Salazar, E.; Aguilar-Vazquez, A.R.; Mantellero, C.A.; Acosta-Galeana, I.; Estrada-Mondragon, A.; Prior-Gonzalez, M.; Martinez-Cruz, J.I.; Rosas-Arellano, A. Ten approaches that improve immunostaining: A review of the latest advances for the optimization of immunofluorescence. Int. J. Mol. Sci. 2022, 23, 1426. [Google Scholar] [CrossRef] [PubMed]
- Mattei, B.; Lira, R.B.; Perez, K.R.; Riske, K.A. Membrane permeabilization induced by triton X-100: The role of membrane phase state and edge tension. Chem. Phys. Lipids 2017, 202, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Hani, U.; Osmani, R.A.M.; Bhosale, R.R.; Shivakumar, H.G.; Kulkarni, P.K. Current perspectives on novel drug delivery systems and approaches for management of cervical cancer: A comprehensive review. Curr. Drug Targets 2016, 17, 337–352. [Google Scholar] [CrossRef] [PubMed]
- Singhal, P. Preparation and characterization of poly (E-CAPROLACTONE) nano fibers by electrospinning technique for tissue enginerring applications. Mater. Today Proc. 2021, 37, 2997–3001. [Google Scholar] [CrossRef]
- Chinna Babu, P.; Sundaraganesan, N.; Sudha, S.; Aroulmoji, V.; Murano, E. Molecular structure and vibrational spectra of irinotecan: A density functional theoretical study. Spectrochim. Acta A Mol. Biomol. Spectrosc. 2012, 98, 1–6. [Google Scholar] [CrossRef]
- Alazzawi, H.F.; Salih, I.K.; Albayati, T.M. Drug delivery of amoxicillin molecule as a suggested treatment for COVID-19 implementing functionalized mesoporous SBA-15 with aminopropyl groups. Drug Deliv. 2021, 28, 856–864. [Google Scholar] [CrossRef]
- Kong, Y.; Ma, Y.; Lei, L.; Wang, X.; Wang, H. Crystallization of poly(ε-caprolactone) in poly(vinylidene fluoride)/poly(ε-caprolactone) blend. Polymers 2017, 9, 42. [Google Scholar] [CrossRef] [Green Version]
- Lei, H.; Xie, M.; Zhao, Y.; Zhang, F.; Xu, Y.; Xie, J. Chitosan/sodium alginate modificated graphene oxide-based nanocomposite as a carrier for drug delivery. Ceram. Int. 2016, 42, 17798–17805. [Google Scholar] [CrossRef]
- Ozawa, S.; Miura, T.; Terashima, J.; Habano, W. Cellular irinotecan resistance in colorectal cancer and overcoming irinotecan refractoriness through various combination trials including DNA methyltransferase inhibitors: A review. Cancer Drug Resist. 2021, 4, 946–964. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Kaufman, P.D. Ki-67: More than a proliferation marker. Chromosoma 2018, 127, 175–186. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Villalona-Calero, M.A. Irinotecan: Mechanisms of tumor resistance and novel strategies for modulating its activity. Ann. Oncol. 2002, 13, 1841–1851. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Solution Combination | Inner Solution | Outer Solution |
|---|---|---|
| A | 14 w.t.% PCL with irinotecan (7 mg/mL) | 14 w.t.% PCL |
| B | 10 w.t.% PCL with irinotecan (7 mg/mL) | 10 w.t.% PCL |
| C | 10 w.t.% PCL with irinotecan (7 mg/mL) | 10 w.t.% PCL with irinotecan (7 mg/mL) |
| Electrospinning Configuration | Collector-Nozzle Distance (cm) | Power Supply (kV) | Outer Flow (mL/h) | Inner Flow (mL/h) | Process Time (hours) |
|---|---|---|---|---|---|
| 1 | 13.5 | 21 | 0.15 | 0.05 | 1.8 |
| 2 | 13.5 | 21 | 0.20 | 0.05 | 1.4 |
| 3 | 13.5 | 21 | 0.25 | 0.05 | 1.2 |
| Membrane | Morphology | Diameter (µm) | Porosity (%) |
|---|---|---|---|
| A1 | U | 0.19 ± 0.04 | 57.36 |
| A2 | U | 0.21 ± 0.05 | 46.25 |
| A3 | U | 0.18 ± 0.05 | 64.58 |
| B1 | U | 0.16 ± 0.03 | 48.35 |
| B2 | U | 0.19 ± 0.05 | 43.97 |
| B3 | U | 0.18 ± 0.03 | 60.1 |
| C1 | U | 0.15 ± 0.03 | 51.56 |
| C2 | U | 0.17 ± 0.05 | 50.65 |
| C3 | U | 0.14 ± 0.02 | 53.58 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cepeda-Franco, C.; Mitxelena-Iribarren, O.; Calero-Castro, F.J.; Astigarraga, M.; Castillo-Tuñon, J.M.; Laga, I.; Pereira, S.; Arana, S.; Mujika, M.; Padillo-Ruiz, J. TARTESSUS: A Customized Electrospun Drug Delivery System Loaded with Irinotecan for Local and Sustained Chemotherapy Release in Pancreatic Cancer. Bioengineering 2023, 10, 183. https://doi.org/10.3390/bioengineering10020183
Cepeda-Franco C, Mitxelena-Iribarren O, Calero-Castro FJ, Astigarraga M, Castillo-Tuñon JM, Laga I, Pereira S, Arana S, Mujika M, Padillo-Ruiz J. TARTESSUS: A Customized Electrospun Drug Delivery System Loaded with Irinotecan for Local and Sustained Chemotherapy Release in Pancreatic Cancer. Bioengineering. 2023; 10(2):183. https://doi.org/10.3390/bioengineering10020183
Chicago/Turabian StyleCepeda-Franco, Carmen, Oihane Mitxelena-Iribarren, Francisco José Calero-Castro, Malen Astigarraga, Juan M. Castillo-Tuñon, Iman Laga, Sheila Pereira, Sergio Arana, Maite Mujika, and Javier Padillo-Ruiz. 2023. "TARTESSUS: A Customized Electrospun Drug Delivery System Loaded with Irinotecan for Local and Sustained Chemotherapy Release in Pancreatic Cancer" Bioengineering 10, no. 2: 183. https://doi.org/10.3390/bioengineering10020183