Author Contributions
Conceptualization, M.A.W.; methodology, M.A.W.; software, M.A.W. and S.A.L.; validation, M.A.W. and S.A.L.; formal analysis, M.A.W.; investigation, M.A.W.; resources, M.A.W. and S.T.D.; data curation, M.A.W. and S.T.D.; writing—original draft preparation, M.A.W., S.A.L. and S.T.D.; writing—review and editing, M.A.W., S.A.L. and S.T.D.; visualization, M.A.W.; supervision, M.A.W.; project administration, M.A.W.; funding acquisition, S.A.L. and S.T.D. All authors have read and agreed to the published version of the manuscript.
Figure 1.
Overview of the process of generating patient-specific statistical reconstructions of healthy anatomical structures.
Figure 1.
Overview of the process of generating patient-specific statistical reconstructions of healthy anatomical structures.
Figure 2.
Damaged femur structure; PAS-W-SRA (a–d) and PAS-W-SRB (e–f): (a) damaged femur with traditional hip prosthesis, anterior view; (b) damaged femur with traditional hip prosthesis, medial view; (c) damaged femur 3D anatomical model only, anterior view; (d) damaged femur 3D anatomical model only, medial view; (e) damaged femur with traditional hip prosthesis, anterior view; (f) damaged femur with traditional hip prosthesis, medial view; (g) damaged femur 3D anatomical model only, anterior view; (h) damaged femur 3D anatomical model only, medial view. Bone is shown in beige, and prostheses are shown in gray.
Figure 2.
Damaged femur structure; PAS-W-SRA (a–d) and PAS-W-SRB (e–f): (a) damaged femur with traditional hip prosthesis, anterior view; (b) damaged femur with traditional hip prosthesis, medial view; (c) damaged femur 3D anatomical model only, anterior view; (d) damaged femur 3D anatomical model only, medial view; (e) damaged femur with traditional hip prosthesis, anterior view; (f) damaged femur with traditional hip prosthesis, medial view; (g) damaged femur 3D anatomical model only, anterior view; (h) damaged femur 3D anatomical model only, medial view. Bone is shown in beige, and prostheses are shown in gray.
Figure 3.
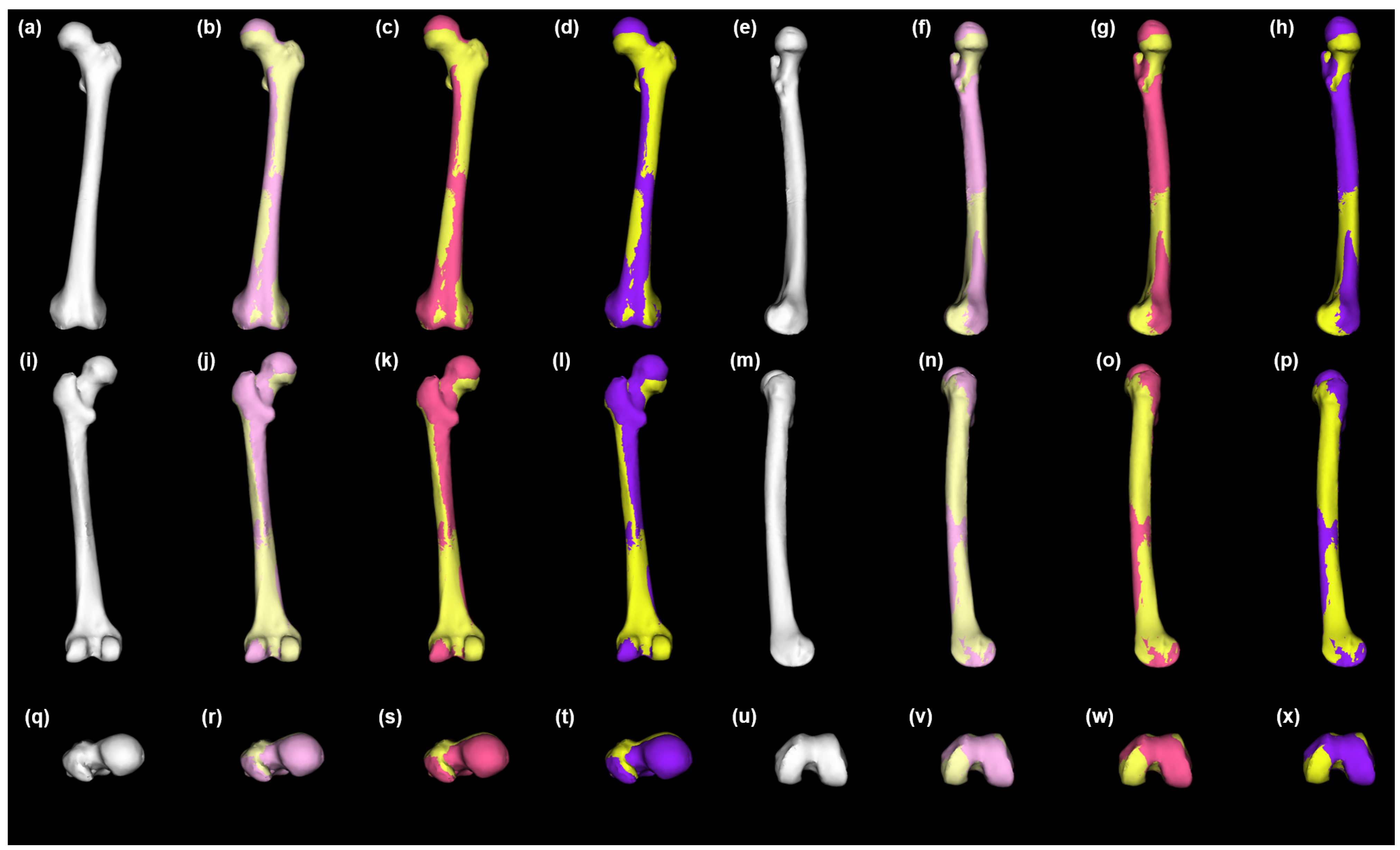
Healthy left femur statistical shape model and variation across the population. Anterior view (a–d), medial view (e–h), posterior view (i–l), lateral view = (m–p), superior view = (q–t), and inferior view (u–x). Mean = white (a,e,i,m,q,u); +1 SD = pink (b,f,j,n,r,v); −1 SD = pastel yellow (b,f,j,n,r,v); +2 SD = magenta (c,g,k,o,s,w); −2 SD = lemon chiffon (c,g,k,o,s,w); +3 SD = purple (d,h,l,p,t,x); −3 SD = yellow (d,h,l,p,t,x). SD = standard deviation.
Figure 3.
Healthy left femur statistical shape model and variation across the population. Anterior view (a–d), medial view (e–h), posterior view (i–l), lateral view = (m–p), superior view = (q–t), and inferior view (u–x). Mean = white (a,e,i,m,q,u); +1 SD = pink (b,f,j,n,r,v); −1 SD = pastel yellow (b,f,j,n,r,v); +2 SD = magenta (c,g,k,o,s,w); −2 SD = lemon chiffon (c,g,k,o,s,w); +3 SD = purple (d,h,l,p,t,x); −3 SD = yellow (d,h,l,p,t,x). SD = standard deviation.
Figure 4.
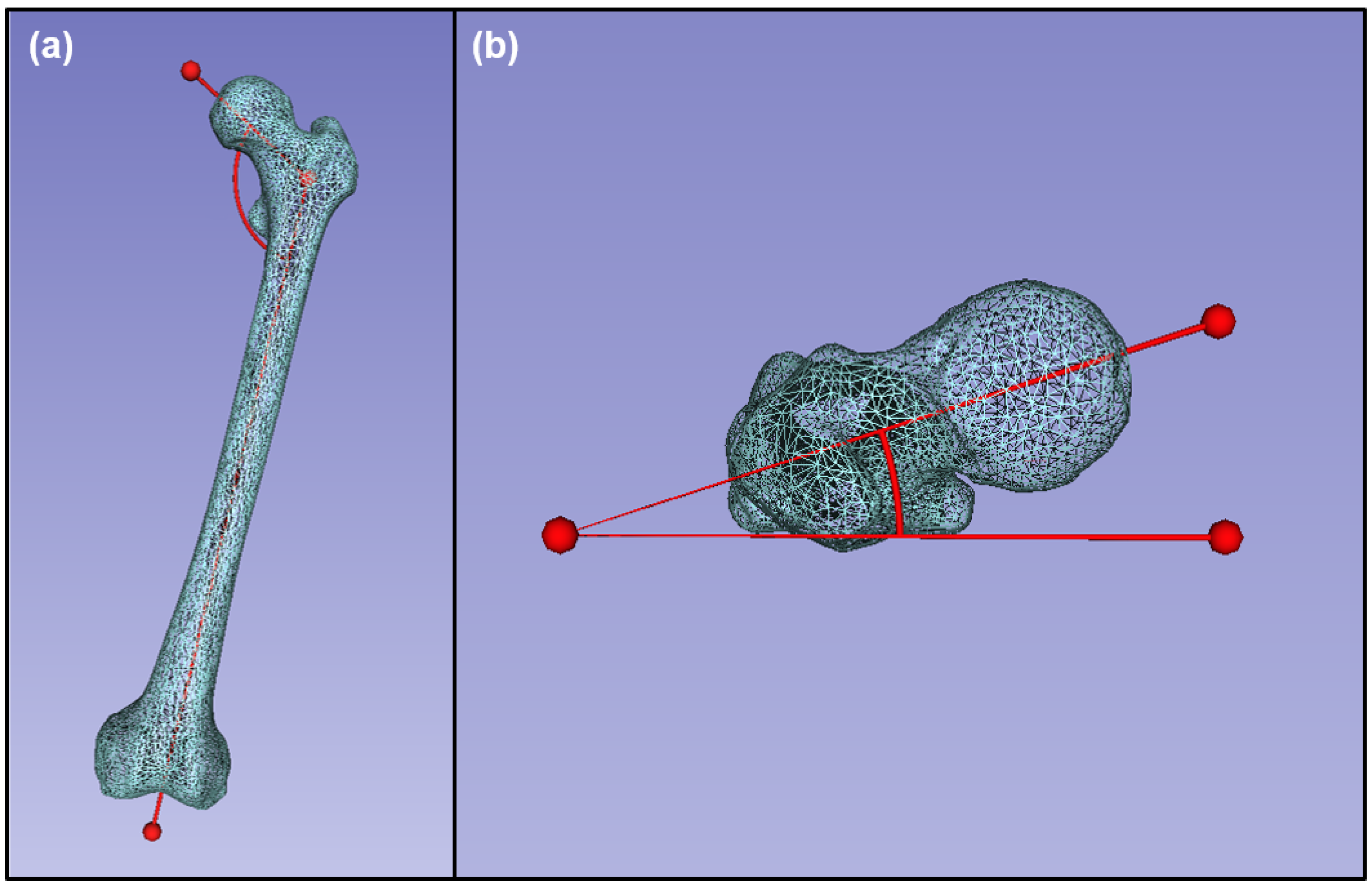
Morphological data collected from an example healthy femur: (a) angle of inclination, anterior view; (b) femoral neck anteversion, superior view.
Figure 4.
Morphological data collected from an example healthy femur: (a) angle of inclination, anterior view; (b) femoral neck anteversion, superior view.
Figure 5.
The 3D models of damaged anatomy and patient-specific statistical reconstructions of healthy anatomical structure: (a) damaged left femur; (b) whole left femur after statistical reconstruction of missing structure. Bone is shown in beige, and statistically reconstructed anatomy is shown in transparent white; anterior view.
Figure 5.
The 3D models of damaged anatomy and patient-specific statistical reconstructions of healthy anatomical structure: (a) damaged left femur; (b) whole left femur after statistical reconstruction of missing structure. Bone is shown in beige, and statistically reconstructed anatomy is shown in transparent white; anterior view.
Figure 6.
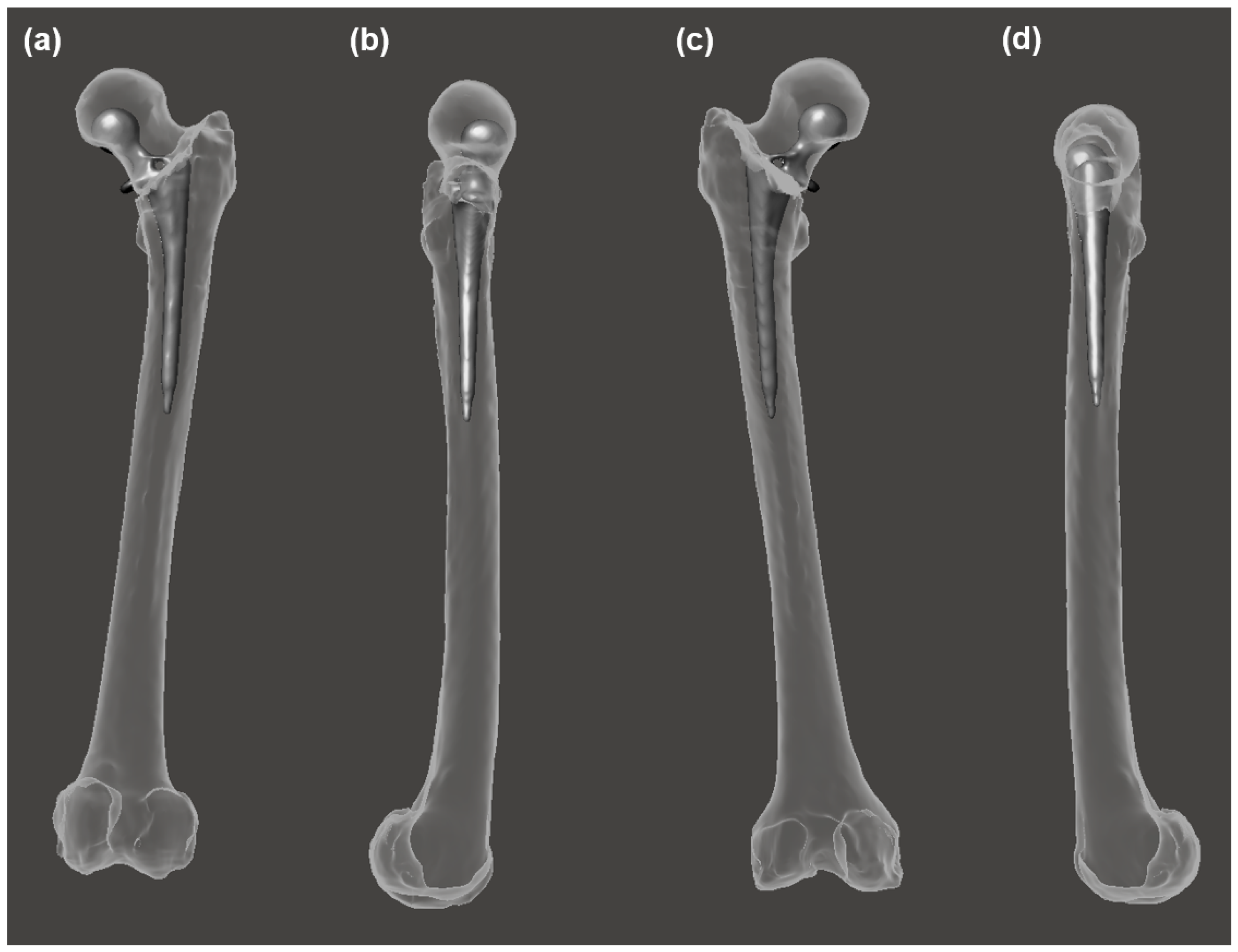
Comparison of the statistical reconstruction of healthy structure and the traditional prosthesis morphology and orientation for the same individual. Prosthesis is shown in gray; bone and statistically reconstructed bone are transparent: (a) anterior view; (b) medial view; (c) posterior view; (d) lateral view.
Figure 6.
Comparison of the statistical reconstruction of healthy structure and the traditional prosthesis morphology and orientation for the same individual. Prosthesis is shown in gray; bone and statistically reconstructed bone are transparent: (a) anterior view; (b) medial view; (c) posterior view; (d) lateral view.
Figure 7.
Morphological variation between statistically reconstructed healthy anatomy and that of a traditional prosthesis. Bone is shown in white. Prosthesis is shown in gray. Statistical reconstructions: Mean is shown in gold, −1 SD is shown in blue, and +1 SD is shown in green. SD = standard deviation.
Figure 7.
Morphological variation between statistically reconstructed healthy anatomy and that of a traditional prosthesis. Bone is shown in white. Prosthesis is shown in gray. Statistical reconstructions: Mean is shown in gold, −1 SD is shown in blue, and +1 SD is shown in green. SD = standard deviation.
Table 1.
Maximum femoral length (mm) data of femur structures with traditional prostheses and healthy femur structures obtained by statistical reconstruction. TrPr = traditional prosthesis; StatRecon = statistical reconstructions; SD = standard deviation.
Table 1.
Maximum femoral length (mm) data of femur structures with traditional prostheses and healthy femur structures obtained by statistical reconstruction. TrPr = traditional prosthesis; StatRecon = statistical reconstructions; SD = standard deviation.
| | TrPr | StatRecon | StatRecon | StatRecon | StatRecon | StatRecon | StatRecon | StatRecon |
|---|
| | | −3SD | −2SD | −1SD | Mean | +1SD | +2SD | +3SD |
|---|
| PASWSRA | 461.3 | 475.7 | 478.1 | 480.7 | 483.4 | 486.2 | 488.7 | 491.6 |
| PASWSRB | 439.5 | 454.8 | 457.3 | 459.9 | 462.5 | 465.2 | 467.8 | 470.6 |
Table 2.
Hausdorff distance (mm) data of femur structures with traditional prostheses and healthy femur structures obtained by statistical reconstruction. All values represent the Hausdorff distance between the particular specimen and the respective statistical reconstruction mean. TrPr = traditional prosthesis; StatRecon = statistical reconstruction; SD = standard deviation.
Table 2.
Hausdorff distance (mm) data of femur structures with traditional prostheses and healthy femur structures obtained by statistical reconstruction. All values represent the Hausdorff distance between the particular specimen and the respective statistical reconstruction mean. TrPr = traditional prosthesis; StatRecon = statistical reconstruction; SD = standard deviation.
| | TrPr | StatRecon | StatRecon | StatRecon | StatRecon | StatRecon | StatRecon |
|---|
| | | −3SD | −2SD | −1SD | +1SD | +2SD | +3SD |
|---|
| PASWSRA | 25.5 | 8.5 | 5.7 | 2.9 | 2.9 | 5.9 | 8.8 |
| PASWSRB | 29.0 | 8.4 | 5.7 | 2.8 | 2.9 | 5.7 | 8.6 |
Table 3.
Femoral neck anteversion (°) data of femur structures with traditional prostheses and healthy femur structures obtained by statistical reconstruction. TrPr = traditional prosthesis; StatRecon = statistical reconstructions; SD = standard deviation.
Table 3.
Femoral neck anteversion (°) data of femur structures with traditional prostheses and healthy femur structures obtained by statistical reconstruction. TrPr = traditional prosthesis; StatRecon = statistical reconstructions; SD = standard deviation.
| | TrPr | StatRecon | StatRecon | StatRecon | StatRecon | StatRecon | StatRecon | StatRecon |
|---|
| | | −3SD | −2SD | −1SD | Mean | +1SD | +2SD | +3SD |
|---|
| PASWSRA | 17.2 | 6.2 | 6.1 | 6.0 | 5.8 | 5.6 | 5.5 | 5.4 |
| PASWSRB | 13.0 | 4.5 | 4.4 | 4.3 | 3.9 | 3.8 | 3.7 | 3.6 |
Table 4.
Length of rotational center divergence (mm) data of femur structures with traditional prostheses and healthy femur structures obtained by statistical reconstruction. All values represent length of rotational center divergence between the particular specimen and the respective statistical reconstruction mean. TrPr = traditional prosthesis; StatRecon = statistical reconstructions; SD = standard deviation.
Table 4.
Length of rotational center divergence (mm) data of femur structures with traditional prostheses and healthy femur structures obtained by statistical reconstruction. All values represent length of rotational center divergence between the particular specimen and the respective statistical reconstruction mean. TrPr = traditional prosthesis; StatRecon = statistical reconstructions; SD = standard deviation.
| | TrPr | StatRecon | StatRecon | StatRecon | StatRecon | StatRecon | StatRecon |
|---|
| | | −3SD | −2SD | −1SD | +1SD | +2SD | +3SD |
|---|
| PASWSRA | 21.1 | 7.0 | 4.7 | 2.2 | 1.6 | 4.6 | 8.3 |
| PASWSRB | 16.6 | 7.4 | 5.5 | 2.8 | 3.0 | 4.9 | 8.6 |
Table 5.
Angle of inclination (°) data of femur structures with traditional prostheses and healthy femur structures obtained by statistical reconstruction. TrPr = traditional prosthesis; StatRecon = statistical reconstructions; SD = standard deviation.
Table 5.
Angle of inclination (°) data of femur structures with traditional prostheses and healthy femur structures obtained by statistical reconstruction. TrPr = traditional prosthesis; StatRecon = statistical reconstructions; SD = standard deviation.
| | TrPr | StatRecon | StatRecon | StatRecon | StatRecon | StatRecon | StatRecon | StatRecon |
|---|
| | | −3SD | −2SD | −1SD | Mean | +1SD | +2SD | +3SD |
|---|
| PASWSRA | 129.3 | 129.8 | 132.7 | 134.6 | 135.7 | 137.9 | 139.2 | 142.2 |
| PASWSRB | 128.1 | 131.4 | 132.5 | 133.8 | 135.0 | 136.4 | 137.9 | 138.5 |










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}