
Current Knowledge on the Healing of the Extraction Socket: A Narrative Review
 , ,
, ,
Abstract
:1. Introduction
2. Stages of Socket Healing
3. Hemostasis and Coagulation
4. Inflammatory Stage
5. Proliferative Stage
6. Modeling and Remodeling of Extraction Socket and Alveolar Bone
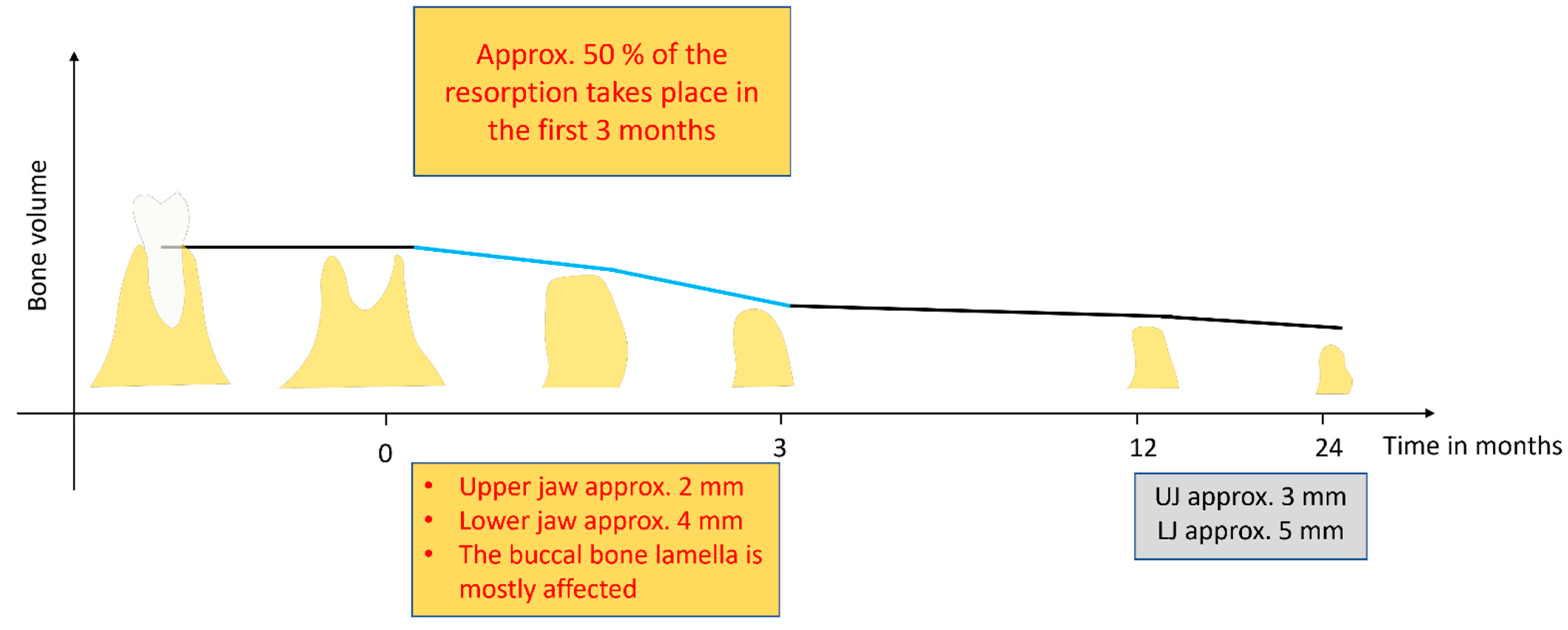
7. Dimensional Changes in Alveolar Bone following Socket Healing

8. Factors That Affect Socket Healing
9. Effects of Alveolar Ridge Preservation Techniques on Socket Healing Outcome
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Steiner, G.G.; Francis, W.; Burrell, R.; Kallet, M.P.; Steiner, D.M.; Macias, R. The healing socket and socket regeneration. Compend. Contin. Educ. Dent. 2008, 29, 114–116, 118, 120–124. [Google Scholar]
- Van der Weijden, F.; Dell’Acqua, F.; Slot, D.E. Alveolar bone dimensional changes of post-extraction sockets in humans: A systematic review. J. Clin. Periodontol. 2009, 36, 1048–1058. [Google Scholar] [CrossRef] [PubMed]
- Udeabor, S.E.; Halwani, M.A.; Alqahtani, S.A.; Alshaiki, S.A.; Alqahtani, A.M.; Alqahtani, S.M. Effects of altitude and relative hypoxia on postextraction socket wound healing: A clinical pilot study. Int. J. Trop. Dis. Health 2017, 25, 1–7. [Google Scholar] [CrossRef]
- Araújo, M.G.; Silva, C.O.; Misawa, M.; Sukekava, F. Alveolar socket healing: What can we learn? Periodontology 2000 2015, 68, 122–134. [Google Scholar] [CrossRef]
- Farina, R.; Trombelli, L. Wound healing of extraction sockets. Endod. Top. 2011, 25, 16–43. [Google Scholar] [CrossRef]
- Trombelli, L.; Farina, R.; Marzola, A.; Bozzi, L.; Liljenberg, B.; Lindhe, J. Modeling and remodeling of human extraction sockets. J. Clin. Periodontol. 2008, 35, 630–639. [Google Scholar] [CrossRef] [PubMed]
- Cardaropoli, G.; Araújo, M.; Hayacibara, R.; Sukekava, F.; Lindhe, J. Healing of extraction sockets and surgically produced—Augmented and non-augmented—Defects in the alveolar ridge. An experimental study in the dog. J. Clin. Periodontol. 2005, 32, 435–440. [Google Scholar] [CrossRef]
- Schropp, L.; Wenzel, A.; Kostopoulos, L.; Karring, T. Bone healing and soft tissue contour changes following single-tooth extraction: A clinical and radiographic 12-month prospective study. Int. J. Periodontics Restor. Dent. 2003, 23, 313–323. [Google Scholar]
- Buser, D.; Martin, W.; Belser, U.C. Optimizing esthetics for implant restorations in the anterior maxilla: Anatomic and surgical considerations. Int. J. Oral Maxillofac. Implants 2004, 19, 43–61. [Google Scholar]
- Grunder, U. Stability of the mucosal topography around single-tooth implants and adjacent teeth: 1-year results. Int. J. Periodontics Restor. Dent. 2000, 20, 11–17. [Google Scholar]
- Hämmerle, C.H.; Araújo, M.G.; Simion, M.; Osteology Consensus Group 2011. Evidence-based knowledge on the biology and treatment of extraction sockets. Clin Oral Implants Res. 2012, 23 (Suppl. 5), 80–82, Erratum in Clin. Oral Implants Res. 2012, 23, 641. [Google Scholar] [CrossRef] [PubMed]
- Horváth, A.; Mardas, N.; Mezzomo, L.A.; Needleman, I.G.; Donos, N. Alveolar ridge preservation. A systematic review. Clin. Oral Investig. 2013, 17, 341–363. [Google Scholar] [CrossRef] [PubMed]
- Avila-Ortiz, G.; Elangovan, S.; Kramer, K.W.; Blanchette, D.; Dawson, D.V. Effect of alveolar ridge preservation after tooth extraction: A systematic review and meta-analysis. J. Dent. Res. 2014, 93, 950–958. [Google Scholar] [CrossRef] [PubMed]
- Avila-Ortiz, G.; Chambrone, L.; Vignoletti, F. Effect of alveolar ridge preservation interventions following tooth extraction: A systematic review and meta-analysis. J. Clin. Periodontol. 2019, 46 (Suppl. 21), 195–223, Erratum in J. Clin. Periodontol. 2020, 47, 129. [Google Scholar] [CrossRef] [PubMed]
- MacBeth, N.; Trullenque-Eriksson, A.; Donos, N.; Mardas, N. Hard and soft tissue changes following alveolar ridge preservation: A systematic review. Clin. Oral Implants Res. 2017, 28, 982–1004. [Google Scholar] [CrossRef]
- MacBeth, N.D.; Donos, N.; Mardas, N. Alveolar ridge preservation with guided bone regeneration or socket seal technique. A randomised, single-blind controlled clinical trial. Clin. Oral Implants Res. 2022, 33, 681–699. [Google Scholar] [CrossRef]
- Chisci, G.; Hatia, A.; Chisci, E.; Chisci, D.; Gennaro, P.; Gabriele, G. Socket Preservation after Tooth Extraction: Particulate Autologous Bone vs. Deproteinized Bovine Bone. Bioengineering 2023, 10, 421. [Google Scholar]
- Chisci, G.; Fredianelli, L. Therapeutic Efficacy of Bromelain in Alveolar Ridge Preservation. Antibiotics 2022, 11, 1542. [Google Scholar] [CrossRef]
- Devlin, H.; Sloan, P. Early bone healing events in the human extraction socket. Int. J. Oral Maxillofac. Surg. 2002, 31, 641–645. [Google Scholar] [CrossRef]
- de Sousa Gomes, P.; Daugela, P.; Poskevicius, L.; Mariano, L.; Fernandes, M.H. Molecular and Cellular Aspects of Socket Healing in the Absence and Presence of Graft Materials and Autologous Platelet Concentrates: A Focused Review. J. Oral Maxillofac. Res. 2019, 10, e2. [Google Scholar]
- Cardaropoli, G.; Araújo, M.; Lindhe, J. Dynamics of bone tissue formation in tooth extraction sites. An. experimental study in dogs. J. Clin. Periodontol. 2003, 30, 809–818. [Google Scholar] [CrossRef] [PubMed]
- Srinivas, B.; Das, P.; Rana, M.M.; Qureshi, A.Q.; Vaidya, K.C.; Ahmed Raziuddin, S.J. Wound Healing and Bone Regeneration in Postextraction Sockets with and without Platelet-rich Fibrin. Ann. Maxillofac. Surg. 2018, 8, 28–34. [Google Scholar] [PubMed]
- Davies, J.E.; Hosseini, M.M. Histodynamics of Endosseous Wound Healing. In Bone Engineering; Davies, J.E., Ed.; EM Squared Inc.: Toronto, ON, Canada, 2000; pp. 1–14. [Google Scholar]
- Barrientos, S.; Stojadinovic, O.; Golinko, M.S.; Brem, H.; Tomic-Canic, M. Growth factors and cytokines in wound healing. Wound Repair. Regen. 2008, 16, 585–601. [Google Scholar] [CrossRef]
- Koh, T.J.; DiPietro, L.A. Inflammation and wound healing: The role of the macrophage. Expert Rev. Mol. Med. 2011, 13, e23. [Google Scholar] [CrossRef] [PubMed]
- Garlet, G.P.; Horwat, R.; Ray, H.L., Jr.; Garlet, T.P.; Silveira, E.M.; Campanelli, A.P.; Trombone, A.P.; Letra, A.; Silva, R.M. Expression analysis of wound healing genes in human periapical granulomas of progressive and stable nature. J. Endod. 2012, 38, 185–190. [Google Scholar] [CrossRef]
- Fisher, J.P.; Lalani, Z.; Bossano, C.M.; Brey, E.M.; Demian, N.; Johnston, C.M.; Dean, D.; Jansen, J.A.; Wong, M.E.; Mikos, A.G. Effect of biomaterial properties on bone healing in a rabbit tooth extraction socket model. J. Biomed. Mater. Res. A 2004, 68, 428–438. [Google Scholar] [CrossRef]
- Scala, A.; Lang, N.P.; Schweikert, M.T.; de Oliveira, J.A.; Rangel-Garcia, I., Jr.; Botticelli, D. Sequential healing of open extraction sockets. An experimental study in monkeys. Clin. Oral Implants Res. 2014, 25, 288–295. [Google Scholar] [CrossRef]
- Beck-Broichsitter, B.E.; Werk, A.N.; Smeets, R.; Gröbe, A.; Heiland, M.; Cascorbi, I.; Wiltfang, J.; Häsler, R.; Becker, S.T. Targeting gene expression during the early bone healing period in the mandible: A base for bone tissue engineering. J. Craniomaxillofac. Surg. 2015, 43, 1452–1460. [Google Scholar] [CrossRef]
- Doherty, M.J.; Ashton, B.A.; Walsh, S.; Beresford, J.N.; Grant, M.E.; Canfield, A.E. Vascular pericytes express osteogenic potential in vitro and in vivo. J. Bone Miner. Res. 1998, 13, 828–838. [Google Scholar] [CrossRef]
- Supakul, S.; Yao, K.; Ochi, H.; Shimada, T.; Hashimoto, K.; Sunamura, S.; Mabuchi, Y.; Tanaka, M.; Akazawa, C.; Nakamura, T.; et al. Pericytes as a Source of Osteogenic Cells in Bone Fracture Healing. Int. J. Mol. Sci. 2019, 20, 1079. [Google Scholar] [CrossRef]
- Hosokawa, Y.; Sakakura, Y.; Irie, K.; Kudo, K.; Kashiwakura, I. Effects of local and whole body irradiation on the appearance of osteoblasts during wound healing in tooth extraction sockets in rats. J. Radiat. Res. 2010, 51, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Bunnell, B.A. Adipose Tissue-Derived Mesenchymal Stem Cells. Cells 2021, 10, 3433. [Google Scholar] [CrossRef] [PubMed]
- Nahles, S.; Nack, C.; Gratecap, K.; Lage, H.; Nelson, J.J.; Nelson, K. Bone physiology in human grafted and non-grafted extraction sockets—An immunohistochemical study. Clin. Oral Implants Res. 2013, 24, 812–819. [Google Scholar] [CrossRef] [PubMed]
- Evian, C.I.; Rosenberg, E.S.; Coslet, J.G.; Corn, H. The osteogenic activity of bone removed from healing extraction sockets in humans. J. Periodontol. 1982, 53, 81–85. [Google Scholar] [CrossRef]
- Ahn, J.J.; Shin, H.I. Bone tissue formation in extraction sockets from sites with advanced periodontal disease: A histomorphometric study in humans. Int. J. Oral Maxillofac. Implants 2008, 23, 1133–1138. [Google Scholar]
- Aimetti, M.; Romano, F.; Griga, F.B.; Godio, L. Clinical and histologic healing of human extraction sockets filled with calcium sulfate. Int. J. Oral Maxillofac. Implants 2009, 24, 902–909. [Google Scholar]
- Heberer, S.; Al-Chawaf, B.; Jablonski, C.; Nelson, J.J.; Lage, H.; Nelson, K. Healing of ungrafted and grafted extraction sockets after 12 weeks: A prospective clinical study. Int. J. Oral Maxillofac. Implants 2011, 26, 385–392. [Google Scholar]
- Lindhe, J.; Cecchinato, D.; Bressan, E.A.; Toia, M.; Araújo, M.G.; Liljenberg, B. The alveolar process of the edentulous maxilla in periodontitis and non-periodontitis subjects. Clin. Oral Implants Res. 2012, 23, 5–11. [Google Scholar] [CrossRef]
- Kim, J.H.; Susin, C.; Min, J.H.; Suh, H.Y.; Sang, E.J.; Ku, Y.; Wikesjö, U.M.; Koo, K.T. Extraction sockets: Erratic healing impeding factors. J. Clin. Periodontol. 2014, 41, 80–85. [Google Scholar] [CrossRef]
- Araújo, M.G.; Lindhe, J. Dimensional ridge alterations following tooth extraction. An experimental study in the dog. J. Clin. Periodontol. 2005, 32, 212–218. [Google Scholar] [CrossRef]
- Vignoletti, F.; Discepoli, N.; Müller, A.; de Sanctis, M.; Muñoz, F.; Sanz, M. Bone modelling at fresh extraction sockets: Immediate implant placement versus spontaneous healing: An experimental study in the beagle dog. J. Clin. Periodontol. 2012, 39, 91–97. [Google Scholar] [CrossRef]
- Sheng, Z.; Zheng, F.; Li, J.; Wang, Y.; Du, Y.; Liu, X.; Yu, X. Denervation delays initial bone healing of rat tooth extraction socket. Odontology 2023, 111, 640–648. [Google Scholar] [CrossRef] [PubMed]
- Hassumi, J.S.; Mulinari-Santos, G.; Fabris, A.L.D.S.; Jacob, R.G.M.; Gonçalves, A.; Rossi, A.C.; Freire, A.R.; Faverani, L.P.; Okamoto, R. Alveolar bone healing in rats: Micro-CT, immunohistochemical and molecular analysis. J. Appl. Oral Sci. 2018, 26, e20170326. [Google Scholar] [CrossRef] [PubMed]
- Yugoshi, L.I.; Sala, M.A.; Brentegani, L.G.; Lamano Carvalho, T.L. Histometric study of socket healing after tooth extraction in rats treated with diclofenac. Braz. Dent. J. 2002, 13, 92–96. [Google Scholar] [CrossRef]
- Younis, W.H.; Al-Rawi, N.H.; Mohamed, M.A.; Yaseen, N.Y. Molecular events on tooth socket healing in diabetic rabbits. Br. J. Oral Maxillofac. Surg. 2013, 51, 932–936. [Google Scholar] [CrossRef]
- Li, Y.; Ling, J.; Jiang, Q. Inflammasomes in Alveolar Bone Loss. Front. Immunol. 2021, 12, 691013. [Google Scholar] [CrossRef]
- Covani, U.; Giammarinaro, E.; Panetta, D.; Salvadori, P.A.; Cosola, S.; Marconcini, S. Alveolar Bone Remodeling with or without Collagen Filling of the Extraction Socket: A High-Resolution X-ray Tomography Animal Study. J. Clin. Med. 2022, 11, 2493. [Google Scholar] [CrossRef]
- Morelli, T.; Zhang, S.; Monaghan, E.; Moss, K.L.; Lopez, B.; Marchesan, J. Three-Dimensional Volumetric Changes After Socket Augmentation with Deproteinized Bovine Bone and Collagen Matrix. Int. J. Oral Maxillofac. Implants 2020, 35, 566–575. [Google Scholar] [CrossRef]
- Pagni, G.; Pellegrini, G.; Giannobile, W.V.; Rasperini, G. Postextraction alveolar ridge preservation: Biological basis and treatments. Int. J. Dent. 2012, 2012, 151030. [Google Scholar] [CrossRef]
- Jahangiri, L.; Devlin, H.; Ting, K.; Nishimura, I. Current perspectives in residual ridge remodeling and its clinical implications: A review. J. Prosthet. Dent. 1998, 80, 224–237. [Google Scholar] [CrossRef]
- Tan, W.L.; Wong, T.L.; Wong, M.C.; Lang, N.P. A systematic review of post-extractional alveolar hard and soft tissue dimensional changes in humans. Clin. Oral Implants Res. 2012, 23 (Suppl. 5), 1–21. [Google Scholar] [CrossRef] [PubMed]
- Lekovic, V.; Camargo, P.M.; Klokkevold, P.R.; Weinlaender, M.; Kenney, E.B.; Dimitrijevic, B.; Nedic, M. Preservation of alveolar bone in extraction sockets using bioabsorbable membranes. J. Periodontol. 1998, 69, 1044–1049. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, O.; Bartee, B.K.; Beaumont, C.; Kasaj, A.; Deli, G.; Zafiropoulos, G.G. Alveolar bone preservation in extraction sockets using non-resorbable dPTFE membranes: A retrospective non-randomized study. J. Periodontol. 2008, 79, 1355–1369. [Google Scholar] [CrossRef] [PubMed]
- Choquet, V.; Hermans, M.; Adriaenssens, P.; Daelemans, P.; Tarnow, D.P.; Malevez, C. Clinical and radiographic evaluation of the papilla level adjacent to single-tooth dental implants. A retrospective study in the maxillary anterior region. J. Periodontol. 2001, 72, 1364–1371. [Google Scholar] [CrossRef] [PubMed]
- Tarnow, D.; Elian, N.; Fletcher, P.; Froum, S.; Magner, A.; Cho, S.C.; Salama, M.; Salama, H.; Garber, D.A. Vertical distance from the crest of bone to the height of the interproximal papilla between adjacent implants. J. Periodontol. 2003, 74, 1785–1788. [Google Scholar] [CrossRef]
- Pinho, M.N.; Roriz, V.L.; Novaes, A.B., Jr.; Taba, M., Jr.; Grisi, M.F.; de Souza, S.L.; Palioto, D.B. Titanium membranes in prevention of alveolar collapse after tooth extraction. Implant. Dent. 2006, 15, 53–61. [Google Scholar] [CrossRef]
- Atwood, D.A. Reduction of residual ridges: A major oral disease entity. J. Prosthet. Dent. 1971, 26, 266–279. [Google Scholar] [CrossRef]
- Pramstraller, M.; Farina, R.; Franceschetti, G.; Pramstraller, C.; Trombelli, L. Ridge dimensions of the edentulous posterior maxilla: A retrospective analysis of a cohort of 127 patients using computerized tomography data. Clin. Oral Implants Res. 2011, 22, 54–61, Erratum in Clin. Oral Implants Res. 2011, 22, 235. [Google Scholar] [CrossRef]
- Fickl, S.; Zuhr, O.; Wachtel, H.; Bolz, W.; Huerzeler, M. Tissue alterations after tooth extraction with and without surgical trauma: A volumetric study in the beagle dog. J. Clin. Periodontol. 2008, 35, 356–363. [Google Scholar] [CrossRef]
- Saldanha, J.B.; Casati, M.Z.; Neto, F.H.; Sallum, E.A.; Nociti, F.H., Jr. Smoking may affect the alveolar process dimensions and radiographic bone density in maxillary extraction sites: A prospective study in humans. J. Oral Maxillofac. Surg. 2006, 64, 1359–1365. [Google Scholar] [CrossRef]
- Levin, L.; Levine, J. Cigarette smoking and radiographic alveolar bone height and density. N. Y. State Dent. J. 2010, 76, 31–35. [Google Scholar] [PubMed]
- Rosa, G.M.; Lucas, G.Q.; Lucas, O.N. Cigarette smoking and alveolar bone in young adults: A study using digitized radiographs. J. Periodontol. 2008, 79, 232–244. [Google Scholar] [CrossRef] [PubMed]
- Devlin, H.; Garland, H.; Sloan, P. Healing of tooth extraction sockets in experimental diabetes mellitus. J. Oral Maxillofac. Surg. 1996, 54, 1087–1091. [Google Scholar] [CrossRef] [PubMed]
- Marin, S.; Popovic-Pejicic, S.; Radosevic-Caric, B.; Trtić, N.; Tatic, Z.; Selakovic, S. Hyaluronic acid treatment outcome on the post-extraction wound healing in patients with poorly controlled type 2 diabetes: A randomized controlled split-mouth study. Med. Oral Patol. Oral Cir. Bucal 2020, 25, e154–e160. [Google Scholar] [CrossRef]
- Zhao, N.; Wang, X.; Qin, L.; Zhai, M.; Yuan, J.; Chen, J.; Li, D. Effect of hyaluronic acid in bone formation and its applications in dentistry. J. Biomed. Mater. Res. A 2016, 104, 1560–1569. [Google Scholar] [CrossRef]
- Liao, J.; Ren, J.; Qing, W.; Mu, Y.D.; Li, P. Impact of Hyperbaric Oxygen on the Healing of Teeth Extraction Sockets and Alveolar Ridge Preservation. Clin. Oral Investig. 2020, 24, 2591–2601. [Google Scholar] [CrossRef]
- Canullo, L.; Del Fabbro, M.; Khijmatgar, S.; Panda, S.; Ravidà, A.; Tommasato, G.; Sculean, A.; Pesce, P. Dimensional and histomorphometric evaluation of biomaterials used for alveolar ridge preservation: A systematic review and network meta-analysis. Clin. Oral Investig. 2022, 26, 141–158. [Google Scholar] [CrossRef]
- Abellán, D.; Barallat, L.; Vilarrasa, J.; Cabezas, M.; Pascual La Rocca, A.; Valles, C.; Nart, J. Ridge preservation in molar sites comparing xenograft versus mineralized freeze-dried bone allograft: A randomized clinical trial. Clin. Oral Implants Res. 2022, 33, 511–523. [Google Scholar] [CrossRef]
- Solyom, E.; Szalai, E.; Czumbel, M.L.; Szabo, B.; Váncsa, S.; Mikulas, K.; Radoczy-Drajko, Z.; Varga, G.; Hegyi, P.; Molnar, B.; et al. The use of autogenous tooth bone graft is an efficient method of alveolar ridge preservation—Meta-analysis and systematic review. BMC Oral Health 2023, 23, 226. [Google Scholar] [CrossRef]
- Majzoub, J.; Ravida, A.; Starch-Jensen, T.; Tattan, M.; Suárez-López Del Amo, F. The Influence of Different Grafting Materials on Alveolar Ridge Preservation: A Systematic Review. J. Oral Maxillofac. Res. 2019, 10, e6. [Google Scholar] [CrossRef]
- Araújo, M.G.; Linder, E.; Lindhe, J. Bio-Oss collagen in the buccal gap at immediate implants: A 6-month study in the dog. Clin. Oral Implants Res. 2011, 22, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Del Fabbro, M.; Tommasato, G.; Pesce, P.; Ravidà, A.; Khijmatgar, S.; Sculean, A.; Galli, M.; Antonacci, D.; Canullo, L. Sealing materials for post-extraction site: A systematic review and network meta-analysis. Clin. Oral Investig. 2022, 26, 1137–1154. [Google Scholar] [CrossRef] [PubMed]
- Barone, A.; Ricci, M.; Tonelli, P.; Santini, S.; Covani, U. Tissue changes of extraction sockets in humans: A comparison of spontaneous healing vs. ridge preservation with secondary soft tissue healing. Clin. Oral Implants Res. 2013, 24, 1231–1237. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| S/No. | Study | Year | Study Design | Model | Tooth Type | Healing Period/Outcome | Evaluation Method |
|---|---|---|---|---|---|---|---|
| 1 | Trombelli et al. [6] | 2008 | Clinical study | Human | Single-rooted teeth | 12–24 weeks (Dominant tissue: Provisional matrix and woven bone) | Immunohistochemistry (IHC) |
| 2 | Delvin and Sloan [19] | 2002 | Clinical study | Human | Premolars | Not reported (Final tissue analysis was 2 weeks post extraction) | IHC |
| 3 | Kim et al. [40] | 2014 | Retrospective Explorative study | Human | All teeth | 5.5 ± 2.5 months | Panoramic radiography and CT scan |
| 4 | Srinivas et al. [22] | 2018 | Clinical study | Human | All teeth | 3 months | Cone beam computed tomography (CBCT) |
| 5 | Nahles et al. [34] | 2013 | Clinical study | Human | All teeth | 12 weeks (complete ossification in some patients) | IHC |
| 6 | Ahn and Shin [36] | 2008 | Clinical study | Human | All teeth | 10 weeks (complete socket healing) | Histology |
| 7 | Heberer et al. [38] | 2011 | Clinical study | Human | All teeth | 12 weeks (44% bone formation) | Histology |
| 8 | Lindhe et al. [39] | 2012 | Clinical study | Human | Posterior maxillary teeth | Not specified (varied) | Histology |
| 9 | Cardaropoli et al. [7] | 2005 | Experimental study | Dog | Premolar | 3 months (complete healing) | Histology |
| 10 | Araújo and Lindhe [41] | 2005 | Experimental study | Dog | Premolars | 4–8 weeks (Dominant tissue: Mineralized bone and bone marrow) | Histology |
| 11 | Vignoletti et al. [42] | 2012 | Experimental study | Dog | Premolars | 6 weeks (Socket closed with cortical bone) | Histology |
| 12 | Sheng et al. [43] | 2023 | Experimental study | Rat | Molars | 4 weeks | Immunofluorescence, Micro-CT, IHC, RT-PCR |
| 13 | Hassumi et al. [44] | 2018 | Experimental study | Rat | Incisors | 28 days | Micro-CT, IHC, RT-PCR |
| 14 | Yugoshi et al. [45] | 2002 | Experimental study | Rat | Incisors | 3 weeks (Large volumes of trabecular bone formed) | Histology |
| 15 | Younis et al. [46] | 2013 | Experimental study | Rabbit | Incisors | 4 weeks | IHC |
| 16 | Scala et al. [28] | 2014 | Experimental study | Monkey | Premolars | 90–180 days (Dominant tissue: Trabecular bone and bone marrow) | Histology |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Udeabor, S.E.; Heselich, A.; Al-Maawi, S.; Alqahtani, A.F.; Sader, R.; Ghanaati, S. Current Knowledge on the Healing of the Extraction Socket: A Narrative Review. Bioengineering 2023, 10, 1145. https://doi.org/10.3390/bioengineering10101145
Udeabor SE, Heselich A, Al-Maawi S, Alqahtani AF, Sader R, Ghanaati S. Current Knowledge on the Healing of the Extraction Socket: A Narrative Review. Bioengineering. 2023; 10(10):1145. https://doi.org/10.3390/bioengineering10101145
Chicago/Turabian StyleUdeabor, Samuel E., Anja Heselich, Sarah Al-Maawi, Ali F. Alqahtani, Robert Sader, and Shahram Ghanaati. 2023. "Current Knowledge on the Healing of the Extraction Socket: A Narrative Review" Bioengineering 10, no. 10: 1145. https://doi.org/10.3390/bioengineering10101145