1. Introduction
Autism spectrum disorder (ASD) is a neurodevelopmental disorder characterized by three primary characteristics: functioning difficulties with social interaction, communication barriers, and behavioral restrictions and repetitive patterns [
1,
2,
3,
4]. Despite the lack of a comprehensive understanding of ASD causes, numerous hypotheses and theories have been proposed concerning the etiology of its underlying mechanism. These hypotheses and theories suggest that genes and environmental factors play a significant role in determining ASD severity. Anatomical abnormalities of the brain [
5], functioning of the brain during rest or while performing different tasks [
6], or abnormal connectivity of the white matter [
7,
8] are hypothesized to be responsible for ASD symptoms. Several magnetic resonance imaging (MRI)-based imaging methods have been utilized to study a variety of abnormalities correlated with ASD, including: (i) structural magnetic resonance imaging (sMRI) for anatomical anomalies; (ii) functional magnetic resonance imaging (fMRI), either at rest or while performing a task, for abnormalities in brain activity; (iii) diffusion tensor imaging (DTI) for abnormalities in connectivity. In this study, we utilize fMRI to provide an understanding of assessing autism.
There are two major types of experiments used to analyze the fMRI modality in order to study functional activation anomalies in the brain: (i) resting state fMRI (rs-fMRI) and (ii) task-based fMRI [
9]. In task-based functional MRI, the subject performs a particular task, such as: (1) figures [
10], (2) facial expressions [
11], (3) rewards [
12], or (4) other specific tasks, and then, the brain activity is analyzed. In rs-fMRI, brain activity is captured, in terms of blood-oxygen-level-dependent (BOLD) signals, while the subject is at rest. Since connectivity patterns reveal the resting state, they have proven to be beneficial in diagnosing mental disorders, such as schizophrenia [
13] and Alzheimer’s disease [
14]. For instance, a high degree of accuracy was achieved in diagnosing schizophrenia using deep neural networks [
13]. In addition, another deep-learning approach used rs-fMRI and ResNet to achieve an effective multi-class classification of Alzheimer’s disease [
14]. There is evidence that the functional connectivity between major networks, as well as the functional connectivity within individual networks, is altered in ASD, as demonstrated by numerous studies [
15,
16]. Based on a multivariate autoregressive model, an algorithm based on a machine learning algorithm for analyzing functional connectivity in ASD subjects was used in a previous study [
17]. In this study, it was found that people with ASDs have reduced functional connectivity, which supports the hypothesis that autism is characterized by a deficit in functional connectivity, or ’underconnectivity’. In accordance with the underconnectivity theory [
18], cognitive disorders manifest themselves in reduced synchronized brain activity during integrative processing tasks, such as the synthesis of a sentence from a set of words. There is evidence in previous literature [
17,
19] for the hypothesis of underconnectivity. Similarly, there was lower functional connectivity in the superior parietal and visuospatial regions of ASD when compared to TD [
10]. In another study by Tyszka et al. [
20], there was reduced connectivity between the temporal and frontal cortex, but no global abnormalities were found. In a study by Plitt et al. [
21], abnormalities were reported in functional networks, which were more evident in networks related to social information processing.
Nevertheless, brain networks associated with ASDs exhibit both under-connectivity and over-connectivity [
21,
22]. Unlike previous studies, ASD has not only reported results that indicated brain underconnectivity but also increased brain connectivity in some areas when compared to healthy controls [
22]. In the latter study, functional connectivity patterns were analyzed, specifically interhemispheric connectivity analysis, and it was found that ASD subjects had both under- and over-connectivity. Furthermore, the presence of altered connectivity was verified in Di Martino et al. work [
23]. The subjects with ASD displayed both under- and over-connectivity between different brain regions. Furthermore, a study by Supekar et al. [
24] identified hyperconnectivity in severely socially challenged autistic children.
Providing the appropriate reduction technique is another major component of our proposed work. Bellman [
25] introduced the term ‘curse of dimensionality’ to describe the problem of exponential complexity resulting from the addition of new dimensions to feature space, commonly defined as the
problem. MRI imaging research and medical data are commonly affected by this phenomenon, resulting in over-fitting. There are several ways to reduce the number of features, such as principal component analysis, linear discriminant analysis, or autoencoders [
26,
27,
28]. Due to the fact that these methods do not preserve the semantics of the original feature space, it is typically difficult to identify what clinical findings underlie such classification results. This, in turn, makes them less useful for actual use by physicians to provide them with more information or to better understand the pathological abnormalities underlying each autistic brain and, thus, are less attractive and less practical.
Due to autism’s heterogeneous nature, brain connectivity can vary widely among individuals with the disorder, making classification of the condition difficult. The design of a less-sensitive functional connectivity feature that is less affected by age, sex, and designs of the resting-state scan and studying its correlation with autism is a hot research area [
29], emerging into two popular brain connectivity representations: the conventional, more popular, static functional connectivity (FC), and the newer dynamic functional connectivity (dFC) representations. Those functional connectivity metrics are believed to capture different internal states of the brain while at rest [
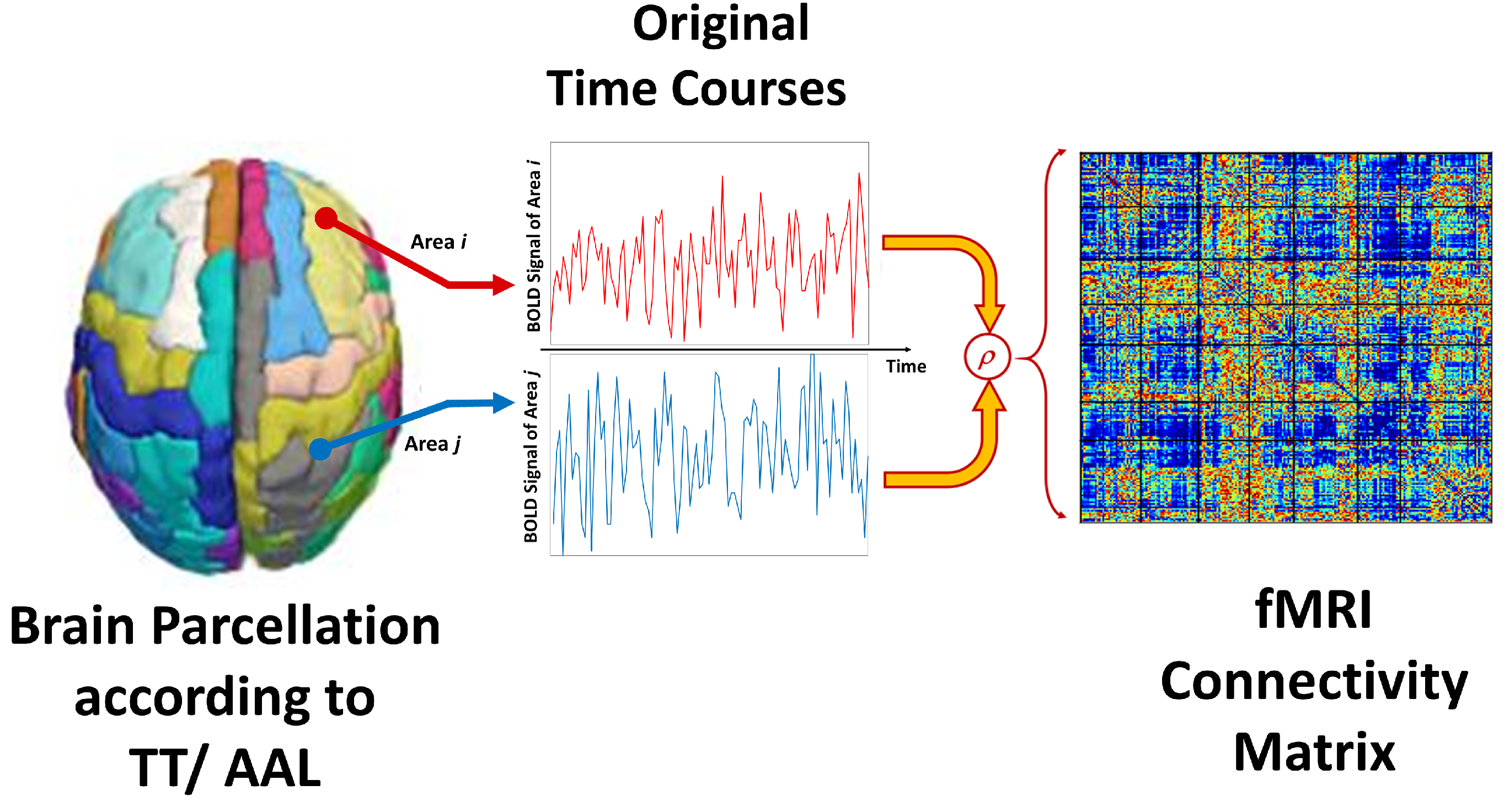
30]. The static FC is a matrix obtained by calculating the Pearson cross-correlation coefficient of the BOLD signals across pairs of pre-defined brain areas. Following statistical analysis and depending on whether one examines local or global networks, there is evidence of both under- and over-connectivity in autism in the majority of the literature [
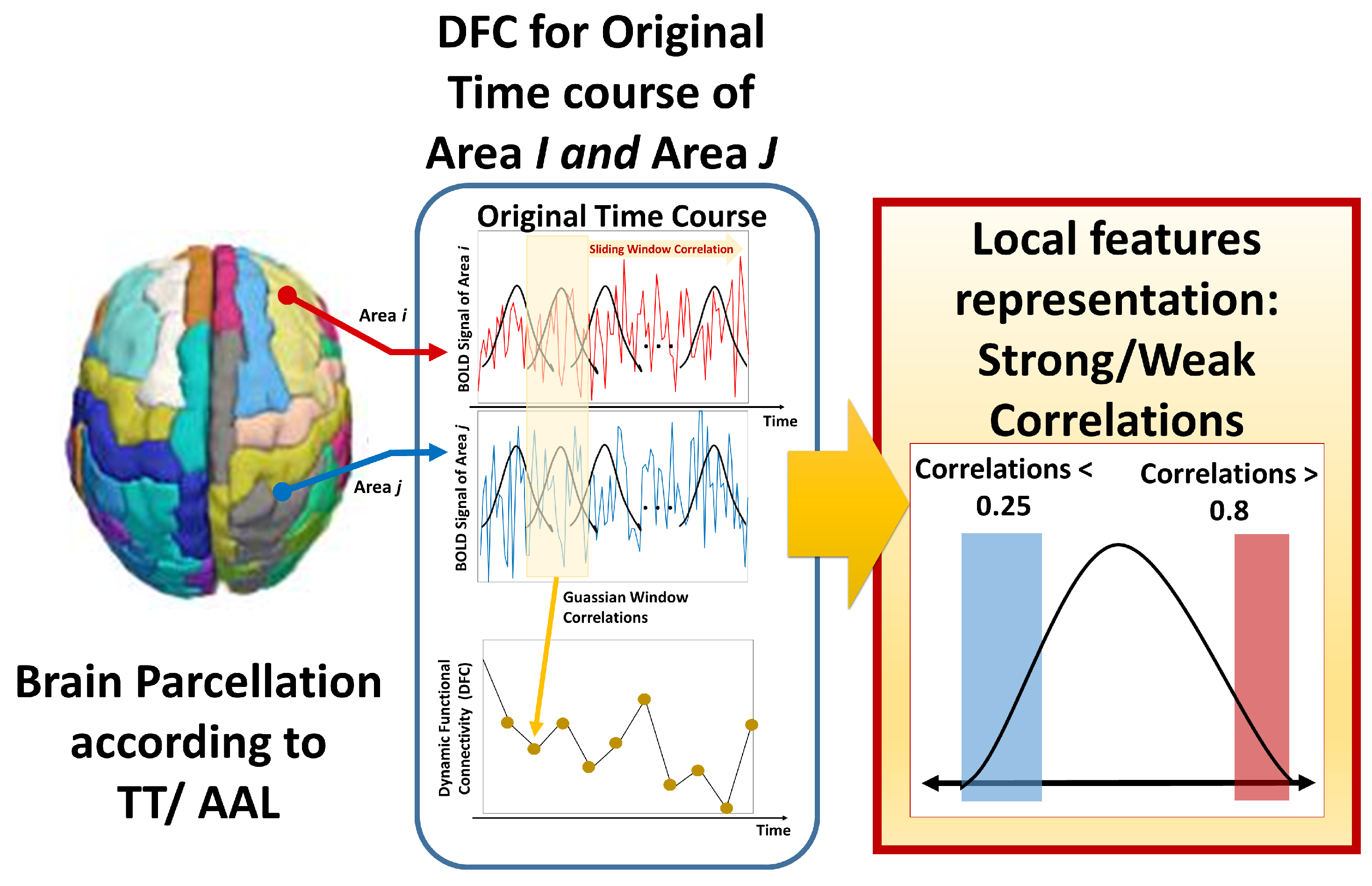
29]. As most of the literature implies temporally stationary functional networks in resting state, dynamic or time-varying changes to functional connectivity that occur during brain scanning are not sufficiently considered by static FC. Newer studies suggest periodically changing spatial patterns of functional networks. To capture those dynamic connectivity patterns, multiple computational strategies were used to find dFC that consider such temporal fluctuations of functional connectivity [
31]. dFC analyses allow identifying not only common brain states but also transitions between them. The most commonly used approach for dFC computation is sliding window techniques [
32], while other approaches include clustering methods, dynamic connectivity regression, time–frequency analysis, wavelet transforms [
33], dynamic connectivity detection, and time series models [
31,
34].
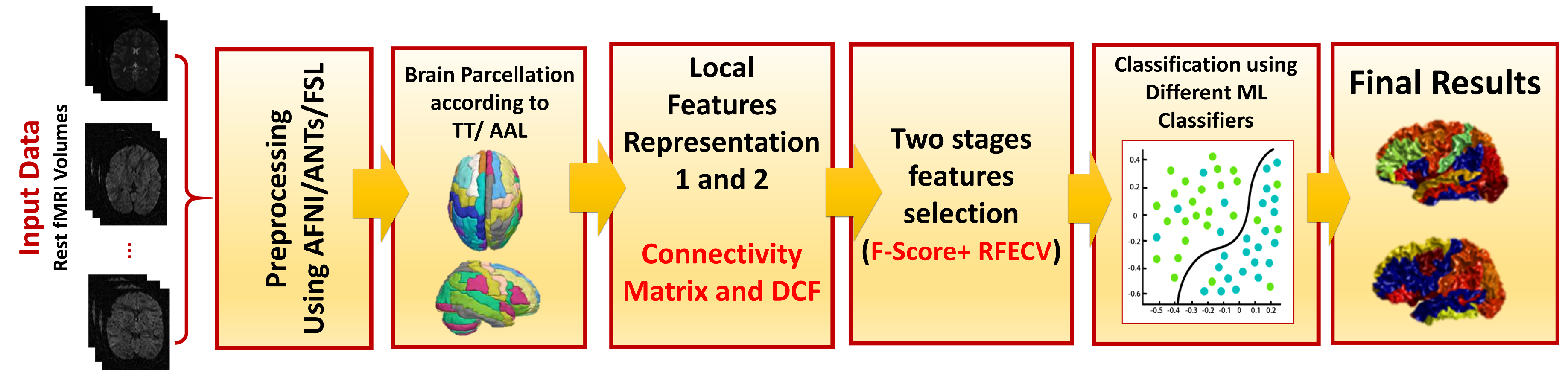
The main limitation of the previous works is that each only gives a limited perspective on the bolts of an efficient CAD system. As the characteristics of autism vary from individual to individual in terms of symptoms and severity, a more personalized approach to predicting and analyzing the behavior and functional capabilities of each autistic subject has become increasingly necessary. Consequently, we can create a treatment plan that is tailored specifically to the needs of each autistic individual. This work uses both a static FC matrix, as well as a novel dFC approach, to investigate the role of rs-fMRI in the diagnosis of autism in a large cohort of 884 subjects, testing different processing and machine learning pipelines. It allows not only an accurate diagnosis but also the identification of the brain regions contributing to this decision. More importantly, it quantifies the effect of different choices along the neuroimaging machine learning pipeline on diagnostic accuracy, including the use of dynamic over static connectivity, which is important for future research. This work presents a unified framework that addresses the following:
The impact of using different atlases, including the automated anatomical labeling (AAL) and Talaraich and Tournoux (TT) atlases.
The effect of using different preprocessing strategies.
The effect of using our novel dFC, in comparison to using conventional static FC.
The dimensionality reduction problem, using two-stage feature selection, with four types of kernels.
The role of the classification strategy, investigating six different classifiers.
The ability to highlight the importance of each of the previous choices on the overall performance.
The remainder of this paper is organized as follows:
Section 2 describes the entire methodology of feature representation, preprocessing, and diagnostic classification. We present the various results on the ABIDE-I rs-fMRI in
Section 3.
Section 4 provides an overall discussion of the presented work. Finally, the conclusions are presented in
Section 5.
4. Discussion
We found a striking overlap between the top brain regions associated with ASD in our study with those identified in other fMRI studies. For example, left sup temporal (Temporal_Sup_L) was identified among regions of great contribution to ASD classification [
40]. Boddaert et al. [
41] also reported superior temporal cortex activation in autistic patients. Several regions of the cingulum have been associated with social cognition and language [
42], which is a common deficiency in autistic subjects. Effective Connectivity of areas Postcentral_L, Frontal_Sup_Medial_R, Precuneus_R, SupraMarginal_R, Supp_Motor_Area_L, and Hippocampus_R, were identified as playing an important role in distinguishing between individuals with autism and controls [
43]. Regions Temporal_Sup_L, Postcentral_R, Frontal_Sup_Medial_R, Precuneus_R, Cingulum_Ant_R, and Hippocampus_R were among ASD-related regions highlighted by Chen et al. [
44]. Children with ASD also showed decreased functional connectivity in the right angular gyrus [
45] as part of the cognition network. The same overlap with the selected brain regions can be seen in many other studies [
46,
47,
48,
49]. While this work only identifies such disrupted connectivity, an explanation of the impaired development of underlying connectivity can be linked to the same etiology of autism. Spotting those differences in brain connectivity is an important step toward a better understanding of autism.
A comparison of the experimental results of some other existing classification systems in the last five years can be found in
Table 6. Our results are clearly higher than most of the literature for the ABIDE-I dataset, taking into consideration that some are only on part of the dataset (not all sites). The added value of this work not only establishes better accuracy on a large dataset but also shows comprehensive experimentation of different blocks along the pipeline. Moreover, the ‘average’ performance across our novel dynamic connectivity feature
across all configurations, including other atlas and inferior strategies, is still greater than most of the literature (78.09% average accuracy, see
Supplementary S3). This is a powerful indication of the potential of our proposed work.
We would emphasize, however, that the promising results were obtained and validated on one dataset only, and adding more data should ensure the generalizability of our proposed framework, an intriguing avenue for future research. In conjunction with fMRI, incorporating other modalities such as sMRI or DTI is believed to provide more accurate and specific results, thus improving diagnostic sensitivity, accuracy, and specificity.

 ,
, 





{kind=link}
{kind=link}
{kind=link}