
ADME Gene-Related Pharmacogenomic Labeling of FDA-Approved Drugs: Comparison with Clinical Pharmacogenetics Implementation Consortium (CPIC) Evidence Levels



Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources/Collection
2.2. Data Characteristics and Annotations
2.3. Data Analysis
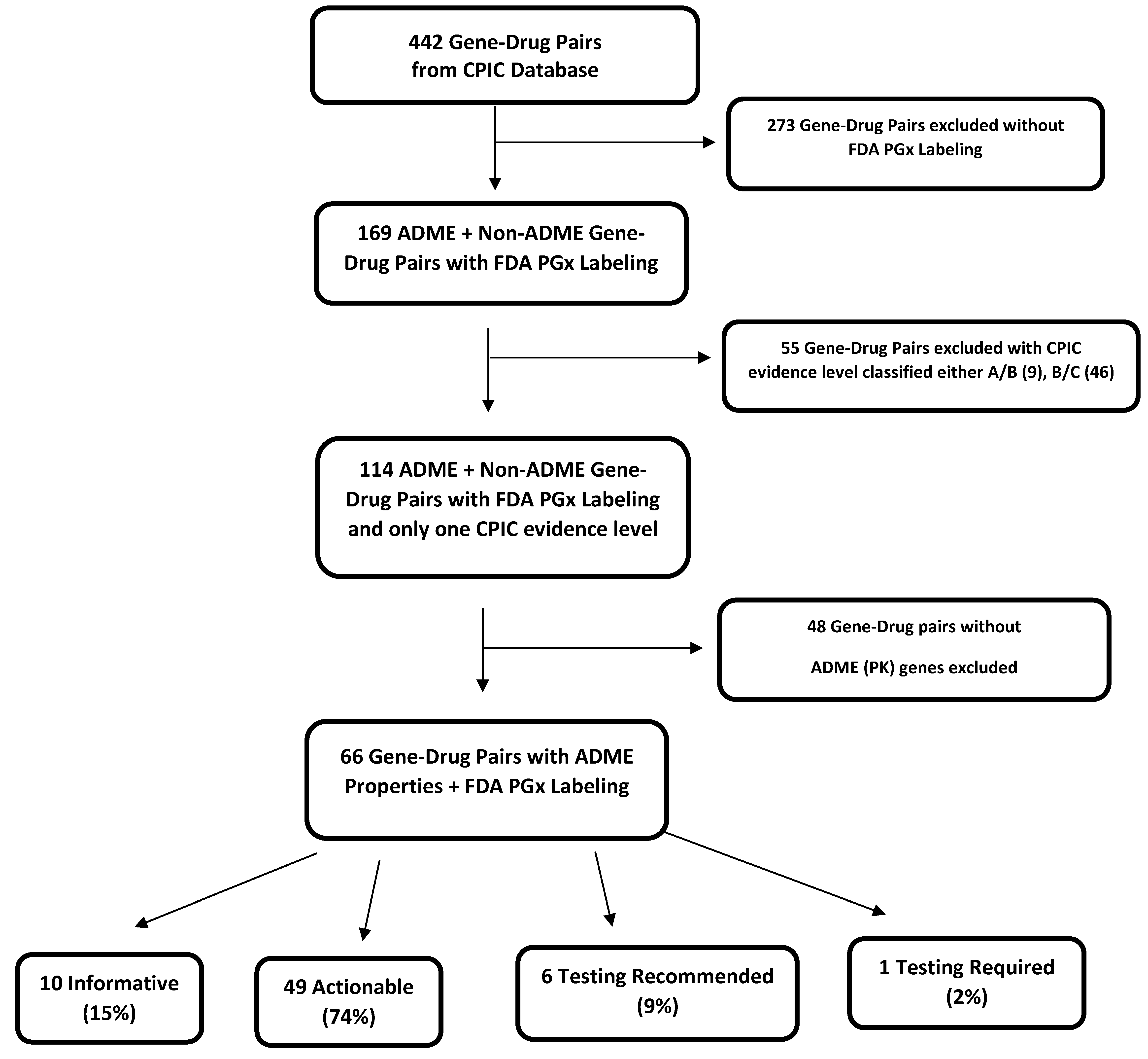
2.3.1. ADME Gene and Drug Pairs with PGx FDA Labeling
2.3.2. CPIC Evidence Levels of ADME Gene–Drug Pairs with FDA Labeling Classification
2.3.3. ADME Gene Categories in FDA Labeling Classification
3. Results
3.1. Disease Spectrum of ADME Gene–Drug Pairs with CPIC and FDA PGx Labeling
3.2. ADME Gene–Drug Pairs with Both PGx FDA Labeling and CPIC Categorizations
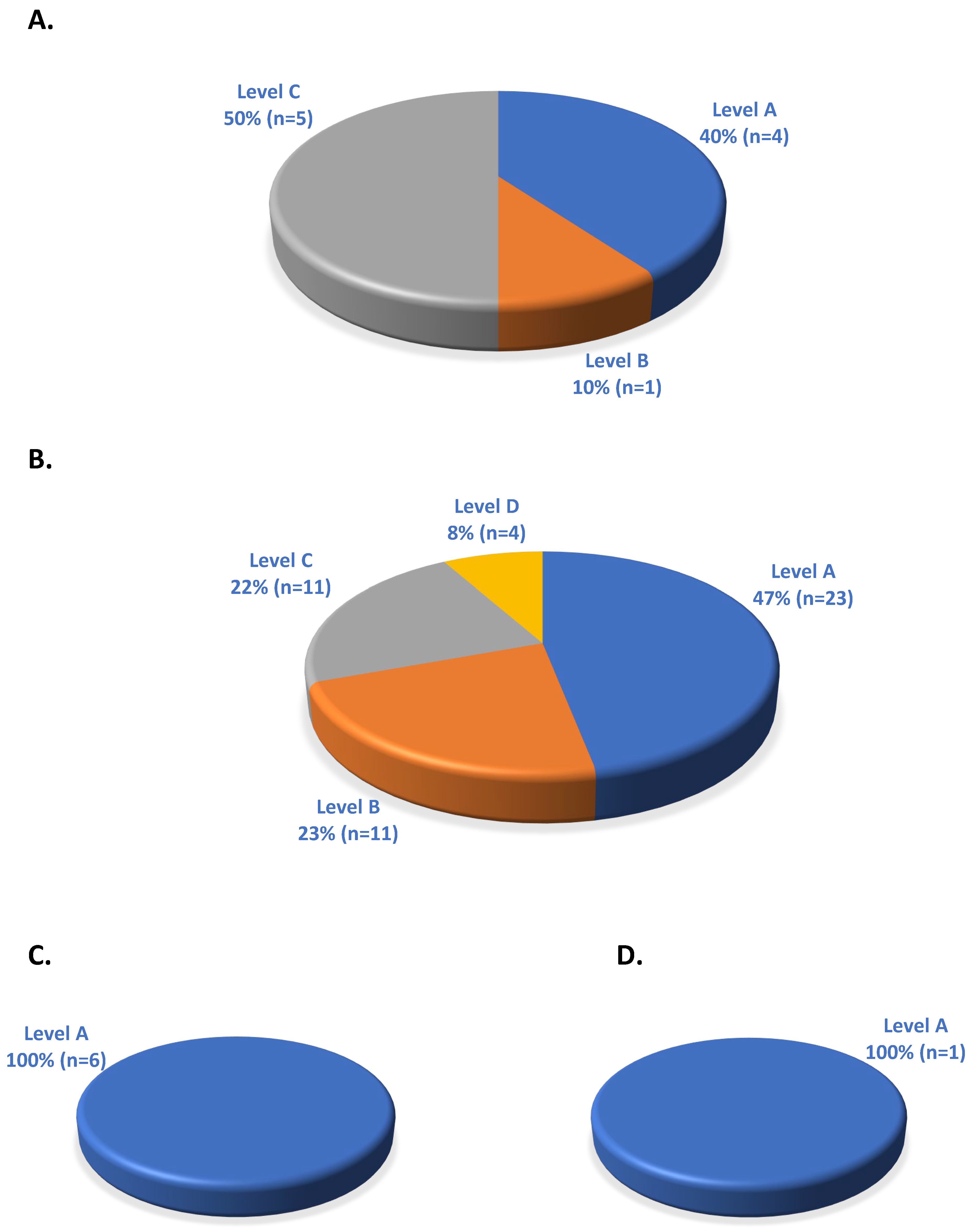
3.3. Distribution of CPIC Evidence Levels in FDA Classifications of ADME Gene–Drug Pairs
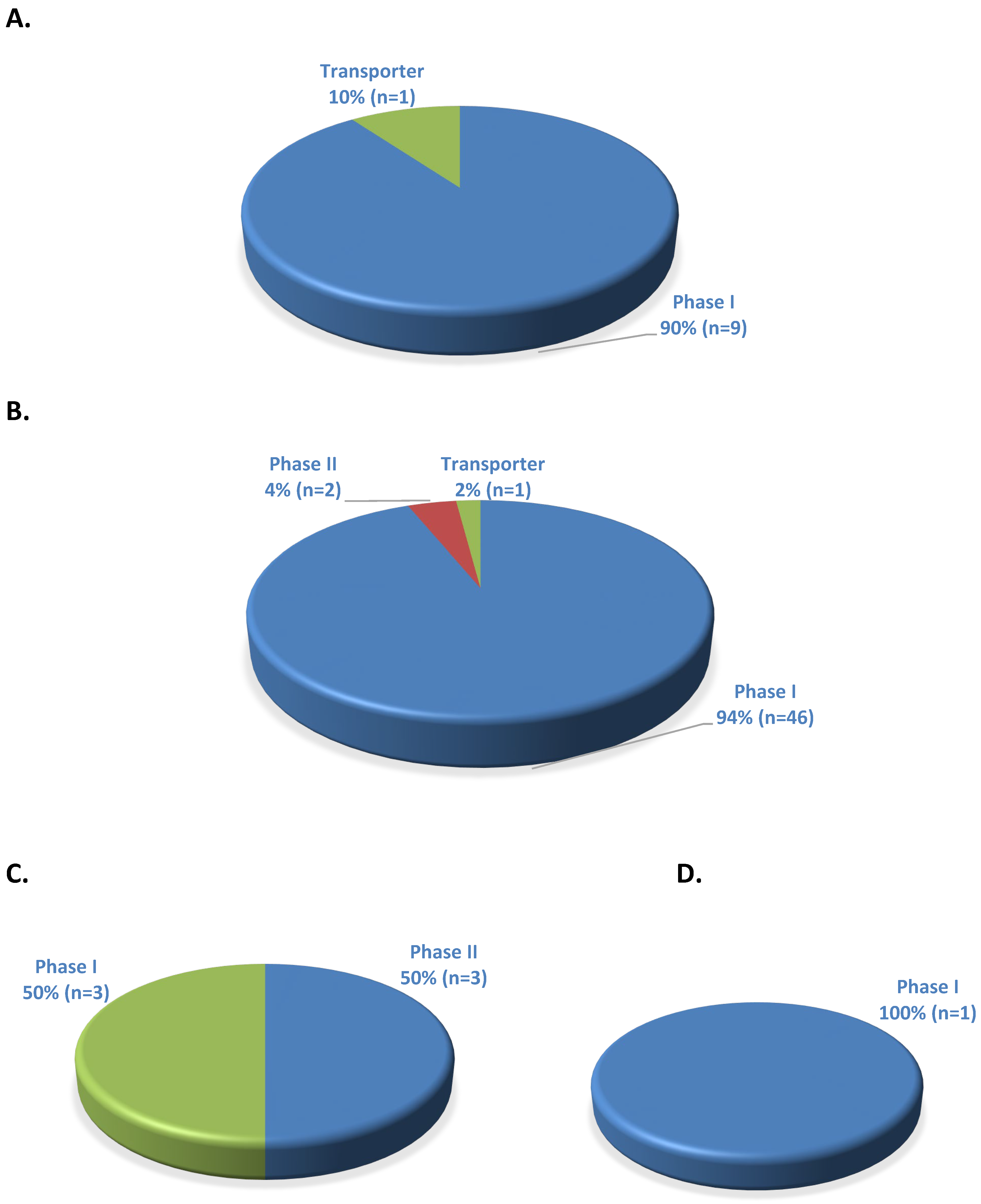
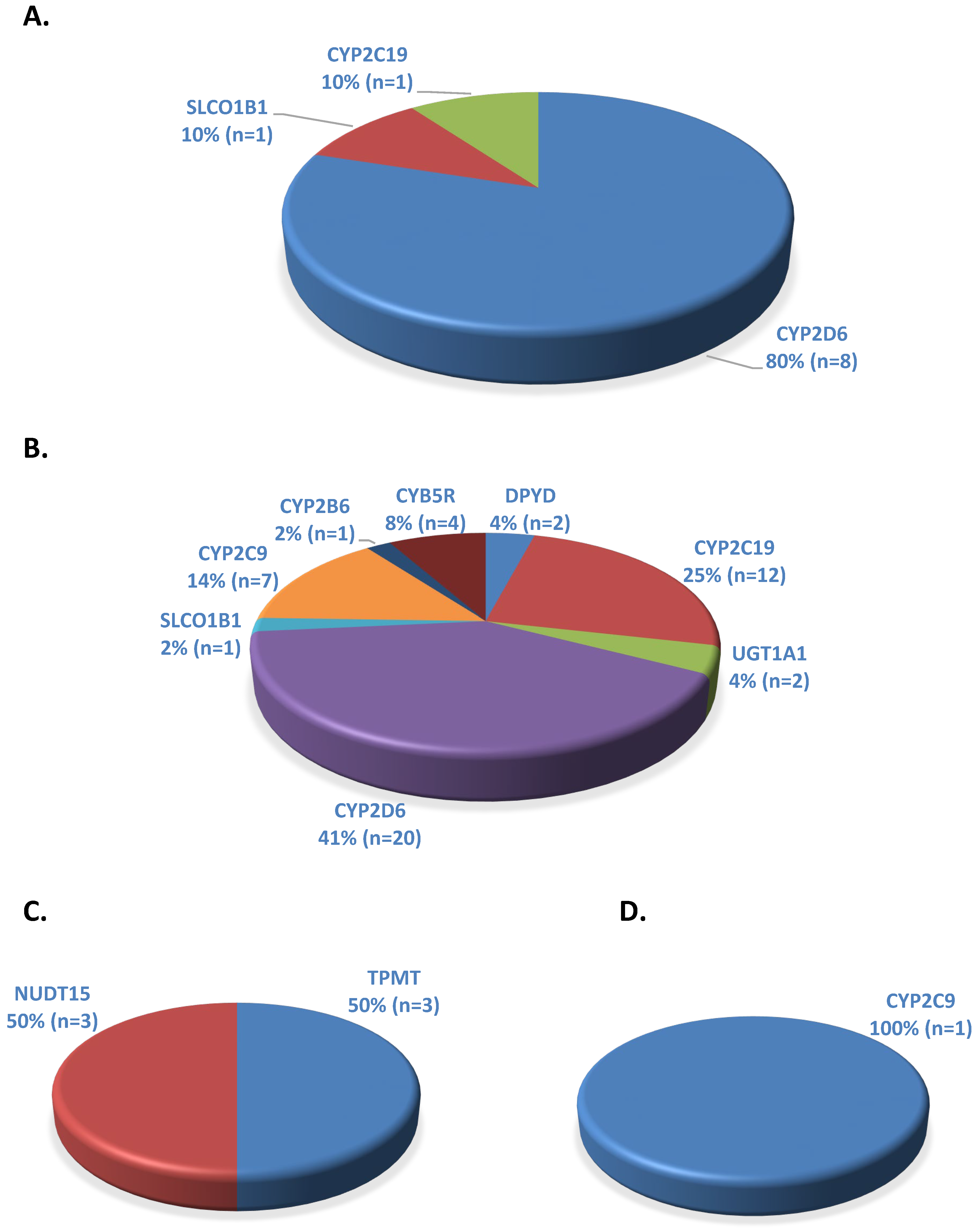
3.4. Prevalence of ADME Genes in PGx FDA Classifications
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Weinshilboum, R.M.; Wang, L. Pharmacogenomics: Precision Medicine and Drug Response. Mayo Clin. Proc. 2017, 92, 1711–1722. [Google Scholar] [CrossRef] [PubMed]
- Doogue, M.P.; Polasek, T.M. The ABCD of clinical pharmacokinetics. Ther. Adv. Drug Saf. 2013, 4, 5–7. [Google Scholar] [CrossRef] [PubMed]
- Bozina, N.; Bradamante, V.; Lovric, M. Genetic polymorphism of metabolic enzymes P450 (CYP) as a susceptibility factor for drug response, toxicity, and cancer risk. Arh. Hig. Rada Toksikol. 2009, 60, 217–242. [Google Scholar] [CrossRef] [PubMed]
- Elfaki, I.; Mir, R.; Almutairi, F.M.; Duhier, F.M.A. Cytochrome P450: Polymorphisms and Roles in Cancer, Diabetes and Atherosclerosis. Asian Pac. J. Cancer Prev. 2018, 19, 2057–2070. [Google Scholar] [CrossRef] [PubMed]
- Rafi, I.; Crinson, I.; Dawes, M.; Rafi, D.; Pirmohamed, M.; Walter, F.M. The implementation of pharmacogenomics into UK general practice: A qualitative study exploring barriers, challenges and opportunities. J. Community Genet. 2020, 11, 269–277. [Google Scholar] [CrossRef]
- Almazroo, O.A.; Miah, M.K.; Venkataramanan, R. Drug Metabolism in the Liver. Clin. Liver Dis. 2017, 21, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Carvalho Henriques, B.; Yang, E.H.; Lapetina, D.; Carr, M.S.; Yavorskyy, V.; Hague, J.; Aitchison, K.J. How Can Drug Metabolism and Transporter Genetics Inform Psychotropic Prescribing? Front. Genet. 2020, 11, 491895. [Google Scholar] [CrossRef]
- Johnson, J.A.; Cavallari, L.H. Warfarin pharmacogenetics. Trends Cardiovasc. Med. 2015, 25, 33–41. [Google Scholar] [CrossRef]
- Pereira, N.L.; Rihal, C.S.; So, D.Y.F.; Rosenberg, Y.; Lennon, R.J.; Mathew, V.; Goodman, S.G.; Weinshilboum, R.M.; Wang, L.; Baudhuin, L.M.; et al. Clopidogrel Pharmacogenetics. Circ. Cardiovasc. Interv. 2019, 12, e007811. [Google Scholar] [CrossRef]
- Pharmacogenomics Knowledge Base (PharmGKB). Drug Label Annotations 2021. Available online: https://www.pharmgkb.org/ (accessed on 17 December 2022).
- Whirl-Carrillo, M.; McDonagh, E.M.; Hebert, J.M.; Gong, L.; Sangkuhl, K.; Thorn, C.F.; Altman, R.B.; Klein, T.E. Pharmacogenomics knowledge for personalized medicine. Clin. Pharmacol. Ther. 2012, 92, 414–417. [Google Scholar] [CrossRef]
- Relling, M.V.; Klein, T.E. CPIC: Clinical Pharmacogenetics Implementation Consortium of the Pharmacogenomics Research Network. Clin. Pharmacol. Ther. 2011, 89, 464–467. [Google Scholar] [CrossRef] [PubMed]
- Clinical Pharmacogenetics Implementation Consortium (CPIC). Considerations for Assignment of CPIC Level for Genes/Drugs. 2021. Available online: https://cpicpgx.org/prioritization/#flowchart (accessed on 17 December 2022).
- U.S. Food & Drug Administration Center for Drug Evaluation and Research. Table of Pharmacogenomic Biomarkers in Drug Labeling. 2022. Available online: https://www.fda.gov/drugs/science-and-research-drugs/table-pharmacogenomic-biomarkers-drug-labeling (accessed on 5 July 2021).
- Shugg, T.; Pasternak, A.L.; London, B.; Luzum, J.A. Prevalence and types of inconsistencies in clinical pharmacogenetic recommendations among major U.S. sources. NPJ Genom. Med. 2020, 5, 48. [Google Scholar] [CrossRef] [PubMed]
- Lim, C.X.; Bozkurt, A.; Chen, Z.Y.; Hird, A.; Wickens, J.; Lazarakis, S.; Hussainy, S.Y.; Alexander, M. Healthcare professionals’ and consumers’ knowledge, attitudes, perspectives, and education needs in oncology pharmacogenomics: A systematic review. Clin. Transl. Sci. 2023, 16, 2467–2482. [Google Scholar] [CrossRef] [PubMed]
- Pearce, A.; Terrill, B.; Alffenaar, J.W.; Patanwala, A.E.; Kummerfeld, S.; Day, R.; Young, M.A.; Stocker, S.L. Pharmacogenomic testing: Perception of clinical utility, enablers and barriers to adoption in Australian hospitals. Intern. Med. J. 2022, 52, 1135–1143. [Google Scholar] [CrossRef]
- Rahawi, S.; Naik, H.; Blake, K.V.; Owusu Obeng, A.; Wasserman, R.M.; Seki, Y.; Funanage, V.L.; Oishi, K.; Scott, S.A. Knowledge and attitudes on pharmacogenetics among pediatricians. J. Hum. Genet. 2020, 65, 437–444. [Google Scholar] [CrossRef]
- Koopmans, A.B.; Braakman, M.H.; Vinkers, D.J.; Hoek, H.W.; van Harten, P.N. Meta-analysis of probability estimates of worldwide variation of CYP2D6 and CYP2C19. Transl. Psychiatry 2021, 11, 141. [Google Scholar] [CrossRef]
- Carranza-Leon, D.; Dickson, A.L.; Gaedigk, A.; Stein, C.M.; Chung, C.P. CYP2D6 genotype and reduced codeine analgesic effect in real-world clinical practice. Pharmacogenomics J. 2021, 21, 484–490. [Google Scholar] [CrossRef]
- Dean, L.; Kane, M. Codeine Therapy and CYP2D6 Genotype. In Medical Genetics Summaries; Pratt, V.M., Scott, S.A., Pirmohamed, M., Esquivel, B., Kane, M.S., Kattman, B.L., Malheiro, A.J., Eds.; National Center for Biotechnology Information (US): Bethesda, MD, USA, 2012. [Google Scholar]
- Haufroid, V.; Hantson, P. CYP2D6 genetic polymorphisms and their relevance for poisoning due to amfetamines, opioid analgesics and antidepressants. Clin. Toxicol. 2015, 53, 501–510. [Google Scholar] [CrossRef]
- Smith, D.M.; Weitzel, K.W.; Elsey, A.R.; Langaee, T.; Gong, Y.; Wake, D.T.; Duong, B.Q.; Hagen, M.; Harle, C.A.; Mercado, E.; et al. CYP2D6-guided opioid therapy improves pain control in CYP2D6 intermediate and poor metabolizers: A pragmatic clinical trial. Genet. Med. 2019, 21, 1842–1850. [Google Scholar] [CrossRef]
- Kam, H.; Jeong, H. Pharmacogenomic Biomarkers and Their Applications in Psychiatry. Genes 2020, 11, 1445. [Google Scholar] [CrossRef]
- Hicks, J.K.; Sangkuhl, K.; Swen, J.J.; Ellingrod, V.L.; Muller, D.J.; Shimoda, K.; Bishop, J.R.; Kharasch, E.D.; Skaar, T.C.; Gaedigk, A.; et al. Clinical pharmacogenetics implementation consortium guideline (CPIC) for CYP2D6 and CYP2C19 genotypes and dosing of tricyclic antidepressants: 2016 update. Clin. Pharmacol. Ther. 2017, 102, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Fang, H.; Harris, S.C.; Liu, Z.; Zhou, G.; Zhang, G.; Xu, J.; Rosario, L.; Howard, P.C.; Tong, W. FDA drug labeling: Rich resources to facilitate precision medicine, drug safety, and regulatory science. Drug Discov. Today 2016, 21, 1566–1570. [Google Scholar] [CrossRef] [PubMed]
- Seminerio, M.J.; Ratain, M.J. Are drug labels static or dynamic? Clin. Pharmacol. Ther. 2013, 94, 302–304. [Google Scholar] [CrossRef] [PubMed]
- Yoon, D.Y.; Lee, S.; Ban, M.S.; Jang, I.J.; Lee, S. Pharmacogenomic information from CPIC and DPWG guidelines and its application on drug labels. Transl. Clin. Pharmacol. 2020, 28, 189–198. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ADME Process | Gene | Examples of Drugs | Disease State/Drug Class |
|---|---|---|---|
| Phase I enzymes | |||
| CYP2C19 | Citalopram, Escitalopram, Doxepin | Depression | |
| Clopidogrel | Antiplatelet | ||
| Omeprazole, Lansoprazole, Pantoprazole, Esomeprazole, Dexlansoprazole, Rabeprazole | Gastroesophageal reflux disorder | ||
| Voriconazole | Antifungal | ||
| Brivaracetam | Antiepileptic | ||
| CYP2D6 | Amitriptyline, Nortriptyline, Paroxetine, Clomipramine Desipramine, Doxepin Fluvoxamine, Imipramine, Trimipramine, Duloxetine, Fluoxetine | Depression | |
| Atomoxetine | ADHD | ||
| Codeine, Tramadol | Pain | ||
| Ondansetron, Palonosetron | Nausea | ||
| Pitolisant, Modafinil | Narcolepsy | ||
| Tamoxifen | Breast cancer | ||
| Aripiprazole, Risperidone | Antipsychotic | ||
| Darifenacin, Fesoterodine, Tolterodine | Urinary incontinence | ||
| CYP2C9 | Celecoxib, Flurbiprofen, Meloxicam, Piroxicam | Pain | |
| Phenytoin, Fosphenytoin | Antiepileptic | ||
| Siponimod | Multiple sclerosis | ||
| Warfarin | Anticoagulant | ||
| CYP2B6 | Efavirenz | HIV | |
| DPYD | Fluorouracil, Capecitabine | Cancer | |
| NUDT15 | Azathioprine | Immunosuppressant | |
| Mercaptopurine, Thioguanine | Cancer | ||
| Phase II enzymes | |||
| UGT1A1 | Irinotecan, Belinostat | Cancer | |
| TPMT | Azathioprine | Immunosuppressant | |
| Mercaptopurine, Thioguanine | Cancer | ||
| Transporters | SLCO1B1 | Rosuvastatin, Simvastatin | Dyslipidemia |
| CPIC Level A | CPIC Level B | CPIC Level C | CPIC Level D | |
|---|---|---|---|---|
| Informative (10) | CYP2C19-lansoprazole | CYP2D6-risperidone | CYP2D6-fluoxetine | |
| CYP2D6-ondansetron | CYP2D6-galantamine | |||
| CYP2D6-paroxetine | CYP2D6-palonosetron | |||
| SLCO1B1-simvastatin | CYP2D6-quinidine | |||
| CYP2D6-terbinafine | ||||
| Actionable (49) | CYP2D6-amitriptyline | CYP2D6-aripiprazole | CYP2D6-darifenacin | CYB5R1-metoclopramide |
| CYP2D6- atomoxetine | CYP2C19-brivaracetam | CYP2D6-duloxetine | CYB5R2-metoclopramide | |
| DPYD-capecitabine | CYP2D6-clomipramine | CYP2C19-esomeprazole | CYB5R3-metoclopramide | |
| CYP2C9-celecoxib | CYP2D6-desipramine | CYP2D6-fesoterodine | CYB5R4-metoclopramide | |
| CYP2C19-citalopram | CYP2C19-dexlansoprazole | CYP2C19-flibanserin | ||
| CYP2C19-clopidogrel | CYP2C19-doxepin | CYP2C9-flibanserin | ||
| CYP2D6-codeine | CYP2D6-doxepin | CYP2D6-flibanserin | ||
| CYP2B6-efavirenz | CYP2D6-fluvoxamine | CYP2D6-quinine | ||
| CYP2C19-escitalopram | CYP2D6-imipramine | CYP2C19-rabeprazole | ||
| DPYD-fluorouracil | CYP2D6-trimipramine | SLCO1B1-rosuvastatin | ||
| CYP2C9-flurbiprofen | UGT1A1-belinostat | CYP2D6-tolterodine | ||
| CYP2C9-meloxicam | ||||
| CYP2D6-nortriptyline | ||||
| CYP2C19-omeprazole | ||||
| CYP2C19-pantoprazole | ||||
| CYP2C9-phenytoin | ||||
| CYP2C9-piroxicam | ||||
| CYP2D6-pitolisant | ||||
| CYP2D6-tamoxifen | ||||
| CYP2D6-tramadol | ||||
| CYP2C19-voriconazole | ||||
| CYP2C9-warfarin | ||||
| UGT1A1-irinotecan | ||||
| Testing Recommended (6) | NUDT15-azathioprine | |||
| NUDT15-mercaptopurine | ||||
| NUDT15-thioguanine | ||||
| TPMT-azathioprine | ||||
| TPMT-mercaptopurine | ||||
| TPMT-thioguanine | ||||
| Testing Required (1) | CYP2C9-siponimod |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Deb, S.; Hopefl, R.; Reeves, A.A.; Cvetkovic, D. ADME Gene-Related Pharmacogenomic Labeling of FDA-Approved Drugs: Comparison with Clinical Pharmacogenetics Implementation Consortium (CPIC) Evidence Levels. Medicines 2024, 11, 6. https://doi.org/10.3390/medicines11030006
Deb S, Hopefl R, Reeves AA, Cvetkovic D. ADME Gene-Related Pharmacogenomic Labeling of FDA-Approved Drugs: Comparison with Clinical Pharmacogenetics Implementation Consortium (CPIC) Evidence Levels. Medicines. 2024; 11(3):6. https://doi.org/10.3390/medicines11030006
Chicago/Turabian StyleDeb, Subrata, Robert Hopefl, Anthony Allen Reeves, and Dena Cvetkovic. 2024. "ADME Gene-Related Pharmacogenomic Labeling of FDA-Approved Drugs: Comparison with Clinical Pharmacogenetics Implementation Consortium (CPIC) Evidence Levels" Medicines 11, no. 3: 6. https://doi.org/10.3390/medicines11030006