
Perfluorooctanoic Acid (PFOA) Exposure and Abnormal Alanine Aminotransferase: Using Clinical Consensus Cutoffs Compared to Statistical Cutoffs for Abnormal Values

Abstract
:1. Introduction
2. Methods
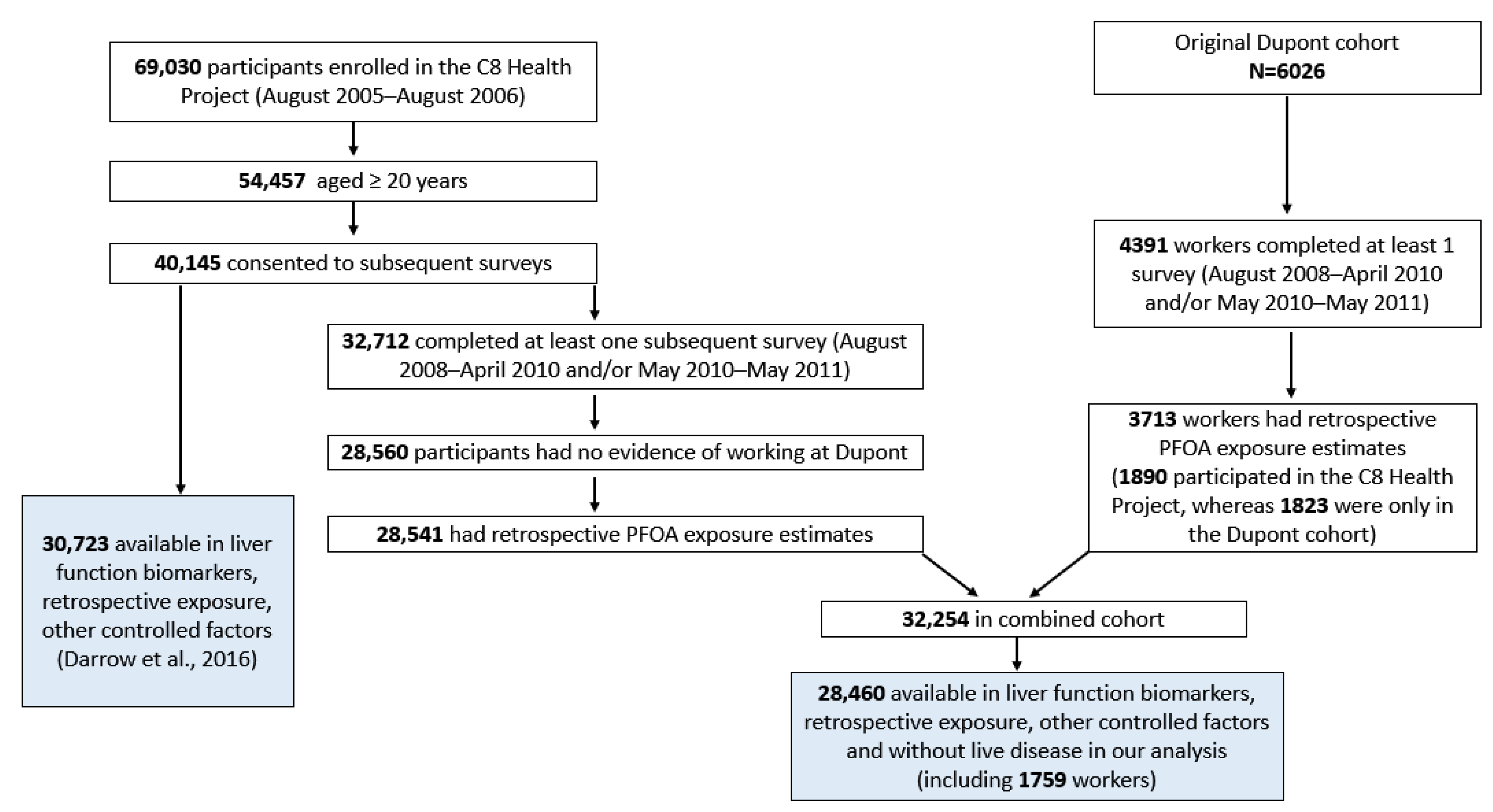
2.1. Study Population
2.2. PFOA Exposure Estimates
2.3. Measures of ALT and Other Factors
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AASLD | American Association of Liver Disease |
| ALT | Alanine aminotransferase |
| ACG | American College of Gastroenterology |
| AST | Aspartate aminotransferase |
| BMI | Body mass index |
| GGT | Gamma-glutamyl-transferase |
| IU | International units |
| mg | Milligram |
| ml | Milliliter |
| ng | Nanogram |
| NAFLD | Nonalcoholic fatty liver disease |
| NHANES | National Health and Nutrition Examination Survey (US Centers for Disease Control and Prevention) |
| OR | Odds Ratio |
| PFAS | Per- and polyfluoroalkyl substances |
| PFHxS | Perfluorohexanesulfonic acid |
| PFNA | Perfluorononanoic acid |
| PFOA | Perfluorooctanoic acid |
| PFOS | Perfluorooctanesulfonic acid |
| US | United States |
| VCTE | Vibration-controlled tensor elastography |
References
- Darrow, L.A.; Growth, A.C.; Winquist, A.; Shin, H.M.; Bartell, S.M.; Steenland, K. Modeled Perfluorooctanoic Acid (PFOA) Exposure and Liver Function in a Mid-Ohio Valley Community. Environ. Health Perspect. 2016, 124, 1227–1233. [Google Scholar] [CrossRef]
- Gluge, J.; Scheringer, M.; Cousins, I.T.; DeWitt, J.C.; Goldenman, G.; Herzke, D.; Lohmann, R.; Ng, C.A.; Trier, X.; Wang, Z. An overview of the uses of per- and polyfluoroalkyl substances (PFAS). Environ. Sci. Process. Impacts 2020, 22, 2345–2373. [Google Scholar] [CrossRef] [PubMed]
- Cordner, A.; De La Rosa, V.Y.; Schaider, L.A.; Rudel, R.A.; Richter, L.; Brown, P. Guideline levels for PFOA and PFOS in drinking water:The role of scientific uncertainty, risk assessment decisions, and social factors. J. Expo. Sci. Environ. Epidemiol. 2019, 29, 157–171. [Google Scholar] [CrossRef]
- Kannan, K.; Corsolini, S.; Falandysz, J.; Fillmann, G.; Kumar, K.S.; Loganathan, B.G.; Mohd, M.A.; Olivero, J.; Van Wouwe, N.; Yang, J.H.; et al. Perfluorooctanesulfonate and related fluorochemicals in human blood from several countries. Environ. Sci. Technol. 2004, 38, 4489–4495. [Google Scholar] [CrossRef] [PubMed]
- Hardell, E.; Karrman, A.; van Bavel, B.; Bao, J.; Carlberg, M.; Hardell, L. Case-control study on perfluorinated alkyl acids (PFAAs) and the risk of prostate cancer. Environ. Int. 2013, 63, 35–39. [Google Scholar] [CrossRef]
- Yeung, L.W.; Guruge, K.S.; Taniyasu, S.; Yamashita, N.; Angus, P.W.; Herath, C.B. Profiles of perfluoroalkyl substances in the liver and serum of patients with liver cancer and cirrhosis in Australia. Ecotoxicol. Environ. Saf. 2013, 96, 139–146. [Google Scholar] [CrossRef]
- Olsen, G.W.; Hansen, K.J.; Stevenson, L.A.; Burris, J.M.; Mandel, J.H. Human donor liver and serum concentrations of perfluorooctanesulfonate and other perfluorochemicals. Environ. Sci. Technol. 2003, 37, 888–891. [Google Scholar] [CrossRef]
- Fenton, S.E.; Ducatman, A.; Boobis, A.; DeWitt, J.C.; Lau, C.; Ng, C.; Smith, J.S.; Roberts, S.M. Per- and Polyfluoroalkyl Substance Toxicity and Human Health Review: Current State of Knowledge and Strategies for Informing Future Research. Environ. Toxicol. Chem. 2021, 40, 606–630. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, L.E.; Guo, G.L. Understanding Environmental Contaminants’ Direct Effects on Non-alcoholic Fatty Liver Disease Progression. Curr. Environ. Health Rep. 2019, 6, 95–104. [Google Scholar] [CrossRef] [PubMed]
- US Environmental Protection Agency. EPA Proposes Designating Certain PFAS Chemicals as Hazardous Substances under Superfund to Protect People’s Health. 2022. Available online: https://www.epa.gov/newsreleases/epa-proposes-designating-certain-pfas-chemicals-hazardous-substances-under-superfund (accessed on 26 August 2022).
- Bureau Veritas. Japan Restricts PFOA and Its Salts on Certain Products Bureau Veritas. 2021. Available online: https://www.cps.bureauveritas.com/newsroom/japan-restricts-pfoa-and-its-salts-certain-products (accessed on 18 May 2021).
- Soltani, M.; Pourfarzam, M.; Sharifabad, A.H.; Neisiani, A.K.; Mousavi, M.K.; Aliomrani, M. Effect of pretreatment with a synbiotic on Perfluorooctanoic acid-induced liver damage after sub-acute oral exposure in C57BL/6J mice. Toxicol. Appl. Pharmacol. 2022, 459, 116360. [Google Scholar] [CrossRef] [PubMed]
- Costello, E.; Rock, S.; Stratakis, N.; Eckel, S.P.; Walker, D.I.; Valvi, D.; Cserbik, D.; Jenkins, T.; Xanthakos, S.A.; Kohli, R.; et al. Exposure to per- and Polyfluoroalkyl Substances and Markers of Liver Injury: A Systematic Review and Meta-Analysis. Environ. Health Perspect. 2022, 130, 46001. [Google Scholar] [CrossRef]
- Ho, S.H.; Soh, S.X.H.; Wang, M.X.; Ong, J.; Seah, A.; Wong, Y.; Fang, Z.; Sim, S.; Lim, J.T. Perfluoroalkyl substances and lipid concentrations in the blood: A systematic review of epidemiological studies. Sci. Total Environ. 2022, 850, 158036. [Google Scholar] [CrossRef]
- Fragki, S.; Dirven, H.; Fletcher, T.; Grasl-Kraupp, B.; Bjerve Gutzkow, K.; Hoogenboom, R.; Kersten, S.; Lindeman, B.; Louisse, J.; Peijnenburg, A.; et al. Systemic PFOS and PFOA exposure and disturbed lipid homeostasis in humans: What do we know and what not? Crit. Rev. Toxicol. 2021, 51, 141–164. [Google Scholar] [CrossRef]
- Trapani, L.; Segatto, M.; Pallottini, V. Regulation and deregulation of cholesterol homeostasis: The liver as a metabolic “power station”. World J. Hepatol. 2012, 4, 184–190. [Google Scholar] [CrossRef]
- Bassler, J.; Ducatman, A.; Elliott, M.; Wen, S.; Wahlang, B.; Barnett, J.; Cave, M.C. Environmental perfluoroalkyl acid exposures are associated with liver disease characterized by apoptosis and altered serum adipocytokines. Environ. Pollut. 2019, 247, 1055–1063. [Google Scholar] [CrossRef] [PubMed]
- Heindel, J.J.; Blumberg, B.; Cave, M.; Machtinger, R.; Mantovani, A.; Mendez, M.A.; Nadal, A.; Palanza, P.; Panzica, G.; Sargis, R.; et al. Metabolism disrupting chemicals and metabolic disorders. Reprod. Toxicol. 2017, 68, 3–33. [Google Scholar] [CrossRef]
- Wahlang, B.; Jin, J.; Beier, J.I.; Hardesty, J.E.; Daly, E.F.; Schnegelberger, R.D.; Falkner, K.C.; Prough, R.A.; Kirpich, I.A.; Cave, M.C. Mechanisms of Environmental Contributions to Fatty Liver Disease. Curr. Environ. Health Rep. 2019, 6, 80–94. [Google Scholar] [CrossRef]
- Marques, E.; Pfohl, M.; Auclair, A.; Jamwal, R.; Barlock, B.J.; Sammoura, F.M.; Goedken, M.; Akhlaghi, F.; Slitt, A.L. Perfluorooctanesulfonic acid (PFOS) administration shifts the hepatic proteome and augments dietary outcomes related to hepatic steatosis in mice. Toxicol. Appl. Pharmacol. 2020, 408, 115250. [Google Scholar] [CrossRef] [PubMed]
- Kim, O.J.; Kim, S.; Park, E.Y.; Oh, J.K.; Jung, S.K.; Park, S.; Hong, S.; Jeon, H.L.; Kim, H.-J.; Park, B.; et al. Exposure to serum perfluoroalkyl substances and biomarkers of liver function: The Korean national environmental health survey 2015–2017. Chemosphere 2023, 322, 138208. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.; Kim, J.Y.; Lee, H.J. Human Evidence of Perfluorooctanoic Acid (PFOA) Exposure on Hepatic Disease: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 11318. [Google Scholar] [CrossRef]
- Wang, P.; Liu, D.; Yan, S.; Cui, J.; Liang, Y.; Ren, S. Adverse Effects of Perfluorooctane Sulfonate on the Liver and Relevant Mechanisms. Toxics 2022, 10, 265. [Google Scholar] [CrossRef] [PubMed]
- Sakr, C.J.; Leonard, R.C.; Kreckmann, K.H.; Slade, M.D.; Cullen, M.R. Longitudinal study of serum lipids and liver enzymes in workers with occupational exposure to ammonium perfluorooctanoate. J. Occup. Environ. Med. 2007, 49, 872–879. [Google Scholar] [CrossRef] [PubMed]
- Gallo, V.; Leonardi, G.; Genser, B.; Lopez-Espinosa, M.J.; Frisbee, S.J.; Karlsson, L.; Ducatman, A.; Fletcher, T. Serum perfluorooctanoate (PFOA) and perfluorooctane sulfonate (PFOS) concentrations and liver function biomarkers in a population with elevated PFOA exposure. Environ. Health Perspect. 2012, 120, 655–660. [Google Scholar] [CrossRef]
- Gleason, J.A.; Post, G.B.; Fagliano, J.A. Associations of perfluorinated chemical serum concentrations and biomarkers of liver function and uric acid in the US population (NHANES), 2007–2010. Environ. Res. 2014, 136, 8–14. [Google Scholar] [CrossRef]
- Yamaguchi, M.; Arisawa, K.; Uemura, H.; Katsuura-Kamano, S.; Takami, H.; Sawachika, F.; Nakamoto, M.; Juta, T.; Toda, E.; Mori, K.; et al. Consumption of seafood, serum liver enzymes, and blood levels of PFOS and PFOA in the Japanese population. J. Occup. Health. 2013, 55, 184–194. [Google Scholar] [CrossRef]
- Nian, M.; Li, Q.Q.; Bloom, M.; Qian, Z.M.; Syberg, K.M.; Vaughn, M.G.; Wang, S.-Q.; Wei, Q.; Zeeshan, M.; Gurram, N.; et al. Liver function biomarkers disorder is associated with exposure to perfluoroalkyl acids in adults: Isomers of C8 Health Project in China. Environ. Res. 2019, 172, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Cakmak, S.; Lukina, A.; Karthikeyan, S.; Atlas, E.; Dales, R. The association between blood PFAS concentrations and clinical biochemical measures of organ function and metabolism in participants of the Canadian Health Measures Survey (CHMS). Sci. Total Environ. 2022, 827, 153900. [Google Scholar] [CrossRef]
- Liu, J.J.; Cui, X.X.; Tan, Y.W.; Dong, P.X.; Ou, Y.Q.; Li, Q.Q.; Chu, C.; Wu, L.Y.; Liang, L.X.; Qin, S.J.; et al. Per- and perfluoroalkyl substances alternatives, mixtures and liver function in adults: A community-based population study in China. Environ. Int. 2022, 163, 107179. [Google Scholar] [CrossRef] [PubMed]
- Olsen, G.W.; Burris, J.M.; Burlew, M.M.; Mandel, J.H. Plasma cholecystokinin and hepatic enzymes, cholesterol and lipoproteins in ammonium perfluorooctanoate production workers. Drug Chem. Toxicol. 2000, 23, 603–620. [Google Scholar] [CrossRef]
- Olsen, G.W.; Ehresman, D.J.; Buehrer, B.D.; Gibson, B.A.; Butenhoff, J.L.; Zobel, L.R. Longitudinal assessment of lipid and hepatic clinical parameters in workers involved with the demolition of perfluoroalkyl manufacturing facilities. J. Occup. Environ. Med. 2012, 54, 974–983. [Google Scholar] [CrossRef] [PubMed]
- Borghese, M.M.; Liang, C.L.; Owen, J.; Fisher, M. Individual and mixture associations of perfluoroalkyl substances on liver function biomarkers in the Canadian Health Measures Survey. Environ. Health A Glob. Access Sci. Source 2022, 21, 85. [Google Scholar] [CrossRef]
- Sherman, K.E. Alanine aminotransferase in clinical practice. A review. Arch. Intern. Med. 1991, 151, 260–265. [Google Scholar] [CrossRef]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Charlton, M.; Cusi, K.; Rinella, M.; Harrison, S.A.; Brunt, E.M.; Sanyal, A.J. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology 2018, 67, 328–357. [Google Scholar] [CrossRef] [PubMed]
- Pandyarajan, V.; Gish, R.G.; Alkhouri, N.; Noureddin, M. Screening for Nonalcoholic Fatty Liver Disease in the Primary Care Clinic. Gastroenterol. Hepatol. 2019, 15, 357–365. [Google Scholar]
- Kwo, P.Y.; Cohen, S.M.; Lim, J.K. ACG Clinical Guideline: Evaluation of Abnormal Liver Chemistries. Am. J. Gastroenterol. 2017, 112, 18–35. [Google Scholar] [CrossRef] [PubMed]
- Rinella, M.E. Nonalcoholic fatty liver disease:A systematic review. JAMA J. Am. Med. Assoc. 2015, 313, 2263–2273. [Google Scholar] [CrossRef]
- Ito, T.; Ishigami, M.; Zou, B.; Tanaka, T.; Takahashi, H.; Kurosaki, M.; Maeda, M.; Thin, K.N.; Tanaka, K.; Takahashi, Y.; et al. The epidemiology of NAFLD and lean NAFLD in Japan: A meta-analysis with individual and forecasting analysis, 1995–2040. Hepatol. Int. 2021, 15, 366–379. [Google Scholar] [CrossRef]
- Kasarala, G.; Tillmann, H.L. Standard liver tests. Clin. Liver Dis. 2016, 8, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Choi, J.; Jun, D.W.; Han, S.W.; Yeo, Y.H.; Nguyen, M.H. Low Alanine Aminotransferase Cut-Off for Predicting Liver Outcomes; A Nationwide Population-Based Longitudinal Cohort Study. J. Clin. Med. 2019, 8, 1445. [Google Scholar] [CrossRef] [PubMed]
- Valenti, L.; Pelusi, S.; Bianco, C.; Ceriotti, F.; Berzuini, A.; Iogna Prat, L.; Trotti, R.; Malvestiti, F.; D’Ambrosio, R.; Lampertico, P.; et al. Definition of Healthy Ranges for Alanine Aminotransferase Levels: A 2021 Update. Hepatol. Commun. 2021, 5, 1824–1832. [Google Scholar] [CrossRef]
- Schumann, G.; Klauke, R. New IFCC reference procedures for the determination of catalytic activity concentrations of five enzymes in serum:Preliminary upper reference limits obtained in hospitalized subjects. Clin. Chim. Acta. 2003, 327, 69–79. [Google Scholar] [CrossRef] [PubMed]
- Frisbee, S.J.; Brooks, A.P., Jr.; Maher, A.; Flensborg, P.; Arnold, S.; Fletcher, T.; Steenland, K.; Shankar, A.; Knox, S.S.; Pollard, C.; et al. The C8 health project: Design, methods, and participants. Environ. Health Perspect. 2009, 117, 1873–1882. [Google Scholar] [CrossRef] [PubMed]
- Winquist, A.; Lally, C.; Shin, H.M.; Steenland, K. Design, methods, and population for a study of PFOA health effects among highly exposed mid-Ohio valley community residents and workers. Environ. Health Perspect. 2013, 121, 893–899. [Google Scholar] [CrossRef] [PubMed]
- Shin, H.M.; Vieira, V.M.; Ryan, P.B.; Detwiler, R.; Sanders, B.; Steenland, K.; Bartell, S.M. Environmental fate and transport modeling for perfluorooctanoic acid emitted from the Washington Works Facility in West Virginia. Environ. Sci. Technol. 2011, 45, 1435–1442. [Google Scholar] [CrossRef]
- Shin, H.M.; Vieira, V.M.; Ryan, P.B.; Steenland, K.; Bartell, S.M. Retrospective exposure estimation and predicted versus observed serum perfluorooctanoic acid concentrations for participants in the C8 Health Project. Environ. Health Perspect. 2011, 119, 1760–1765. [Google Scholar] [CrossRef]
- Woskie, S.R.; Gore, R.; Steenland, K. Retrospective exposure assessment of perfluorooctanoic acid serum concentrations at a fluoropolymer manufacturing plant. Ann. Occup. Hyg. 2012, 56, 1025–1037. [Google Scholar] [CrossRef]
- Olsen, G.W.; Burris, J.M.; Ehresman, D.J.; Froehlich, J.W.; Seacat, A.M.; Butenhoff, J.L.; Zobel, L.R. Half-life of serum elimination of perfluorooctanesulfonate, perfluorohexanesulfonate, and perfluorooctanoate in retired fluorochemical production workers. Environ. Health Perspect. 2007, 115, 1298–1305. [Google Scholar] [CrossRef]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment:Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef]
- DiStefano, J.K.; Gerhard, G.S. NAFLD in normal weight individuals. Diabetol. Metab. Syndr. 2022, 14, 45. [Google Scholar] [CrossRef]
- Jain, R.B.; Ducatman, A. Selective Associations of Recent Low Concentrations of Perfluoroalkyl Substances with Liver Function Biomarkers: NHANES 2011 to 2014 Data on US Adults Aged >/=20 Years. J. Occup. Environ. Med. 2019, 61, 293–302. [Google Scholar] [CrossRef]
- Jain, R.B. Concentration of selected liver enzymes across the states of glomerular function: The associations of PFOA and PFOS. Heliyon. 2022, 5, e02168. [Google Scholar] [CrossRef]
- Lin, C.Y.; Lin, L.Y.; Chiang, C.K.; Wang, W.J.; Su, Y.N.; Hung, K.Y.; Chen, P.-C. Investigation of the associations between low-dose serum perfluorinated chemicals and liver enzymes in US adults. Am. J. Gastroenterol. 2010, 105, 1354–1363. [Google Scholar] [CrossRef]
- Marques, E.S.; Agudelo, J.; Kaye, E.M.; Modaresi, S.M.S.; Pfohl, M.; Becanova, J.; Wei, W.; Polunas, M.; Goedken, M.; Slitt, A.L. The role of maternal high fat diet on mouse pup metabolic endpoints following perinatal PFAS and PFAS mixture exposure. Toxicology 2021, 462, 152921. [Google Scholar] [CrossRef] [PubMed]
- Roth, K.; Yang, Z.; Agarwal, M.; Liu, W.; Peng, Z.; Long, Z.; Birbeck, J.; Westrick, J.; Liu, W.; Petriello, M.C. Exposure to a mixture of legacy, alternative, and replacement per- and polyfluoroalkyl substances (PFAS) results in sex-dependent modulation of cholesterol metabolism and liver injury. Environ. Int. 2021, 157, 106843. [Google Scholar] [CrossRef] [PubMed]
- Modaresi, S.M.S.; Wei, W.; Emily, M.; DaSilva, N.A.; Slitt, A.L. Per- and polyfluoroalkyl substances (PFAS) augment adipogenesis and shift the proteome in murine 3T3-L1 adipocytes. Toxicology 2022, 465, 153044. [Google Scholar] [CrossRef] [PubMed]
- Schlezinger, J.J.; Hyotylainen, T.; Sinioja, T.; Boston, C.; Puckett, H.; Oliver, J.; Heiger-Bernays, W.; Webster, T.F. Perfluorooctanoic acid induces liver and serum dyslipidemia in humanized PPARalpha mice fed an American diet. Toxicol. Appl. Pharmacol. 2021, 426, 115644. [Google Scholar] [CrossRef]
- Sen, P.; Qadri, S.; Luukkonen, P.K.; Ragnarsdottir, O.; McGlinchey, A.; Jantti, S.; Juuti, A.; Arola, J.; Schlezinger, J.J.; Webster, T.F.; et al. Exposure to environmental contaminants is associated with altered hepatic lipid metabolism in non-alcoholic fatty liver disease. J. Hepatol. 2022, 76, 283–293. [Google Scholar] [CrossRef]
- Wan, H.T.; Zhao, Y.G.; Wei, X.; Hui, K.Y.; Giesy, J.P.; Wong, C.K. PFOS-induced hepatic steatosis, the mechanistic actions on beta-oxidation and lipid transport. Biochim. Biophys. Acta. 2012, 1820, 1092–1101. [Google Scholar] [CrossRef]
- Blake, B.E.; Miller, C.N.; Nguyen, H.; Chappell, V.A.; Phan, T.P.; Phadke, D.P.; Balik-Meisner, M.R.; Mav, D.; Shah, R.R.; Fenton, S.E. Transcriptional pathways linked to fetal and maternal hepatic dysfunction caused by gestational exposure to perfluorooctanoic acid (PFOA) or hexafluoropropylene oxide-dimer acid (HFPO-DA or GenX) in CD-1 mice. Ecotoxicol. Environ. Saf. 2022, 248, 114314. [Google Scholar] [CrossRef]
- Li, K.; Sun, J.; Yang, J.; Roberts, S.M.; Zhang, X.; Cui, X.; Wei, S.; Ma, L.Q. Molecular Mechanisms of Perfluorooctanoate-Induced Hepatocyte Apoptosis in Mice Using Proteomic Techniques. Environ. Sci. Technol. 2017, 51, 11380–11389. [Google Scholar] [CrossRef]
- Berube, R.; LeFauve, M.K.; Heldman, S.; Chiang, Y.T.; Birbeck, J.; Westrick, J.; Hoffman, K.; Kassotis, C.D. Adipogenic and endocrine disrupting mixture effects of organic and inorganic pollutant mixtures. Sci. Total Environ. 2023, 876, 162587. [Google Scholar] [CrossRef] [PubMed]
- Alemany-Pages, M.; Moura-Ramos, M.; Araujo, S.; Macedo, M.P.; Ribeiro, R.T.; Ó, D.d.; Ramalho-Santos, J.; Azul, A.M. Insights from qualitative research on NAFLD awareness with a cohort of T2DM patients:Time to go public with insulin resistance? BMC Public Health 2020, 20, 1142. [Google Scholar] [CrossRef] [PubMed]
- Alqahtani, S.A.; Paik, J.M.; Biswas, R.; Arshad, T.; Henry, L.; Younossi, Z.M. Poor Awareness of Liver Disease among Adults with NAFLD in the United States. Hepatol. Commun. 2021, 5, 1833–1847. [Google Scholar] [CrossRef] [PubMed]
- Puri, P.; Fuchs, M. Population Management of Nonalcoholic Fatty Liver Disease. Fed. Pract. 2019, 36, 72–82. [Google Scholar] [PubMed]
- Byrne, C.D.; Targher, G. NAFLD: A multisystem disease. J. Hepatol. 2015, 62 (Suppl. S1), S47–S64. [Google Scholar] [CrossRef]
- Nadim, M.K.; Garcia-Tsao, G. Acute Kidney Injury in Patients with Cirrhosis. New Engl. J. Med. 2023, 388, 733–745. [Google Scholar] [CrossRef]
- Mantovani, A.; Petracca, G.; Beatrice, G.; Csermely, A.; Lonardo, A.; Schattenberg, J.M.; Tilg, H.; Byrne, C.D.; Targher, G. Non-alcoholic fatty liver disease and risk of incident chronic kidney disease: An updated meta-analysis. Gut 2022, 71, 156–162. [Google Scholar] [CrossRef]
- Jain, R.B.; Ducatman, A. Perfluoroalkyl acids serum concentrations and their relationship to biomarkers of renal failure: Serum and urine albumin, creatinine, and albumin creatinine ratios across the spectrum of glomerular function among US adults. Environ. Res. 2019, 174, 143–151. [Google Scholar] [CrossRef]
- Lin, P.D.; Cardenas, A.; Hauser, R.; Gold, D.R.; Kleinman, K.P.; Hivert, M.F.; Calafat, A.M.; Webster, T.F.; Horton, E.S.; Oken, E. Per- and polyfluoroalkyl substances and kidney function: Follow-up results from the Diabetes Prevention Program trial. Environ. Int. 2021, 148, 106375. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Noureddin, M.; Bernstein, D.; Kwo, P.; Russo, M.; Shiffman, M.L.; Younes, Z.; Abdelmalek, M. Role of Noninvasive Tests in Clinical Gastroenterology Practices to Identify Patients with Nonalcoholic Steatohepatitis at High Risk of Adverse Outcomes: Expert Panel Recommendations. Am. J. Gastroenterol. 2021, 116, 254–262. [Google Scholar] [CrossRef]
- Girardi, P.; Merler, E. A mortality study on male subjects exposed to polyfluoroalkyl acids with high internal dose of perfluorooctanoic acid. Environ. Res. 2019, 179 Pt A, 108743. [Google Scholar] [CrossRef]
- Goodrich, J.A.; Walker, D.; Lin, X.; Wang, H.; Lim, T.; McConnell, R.; Conti, D.V.; Chatzi, L.; Setiawan, V.W. Exposure to perfluoroalkyl substances and risk of hepatocellular carcinoma in a multiethnic cohort. JHEP Rep. 2022, 4, 100550. [Google Scholar] [CrossRef]
- Limei, E.; Zhang, S.; Jiang, X. Association between perfluoroalkyl substances exposure and the prevalence of nonalcoholic fatty liver disease in the different sexes:A study from the National Health and Nutrition Examination Survey 2005–2018. Environ. Sci. Pollut. Res. Int. 2023, 30, 44292–44303. [Google Scholar]
- Siddiqui, M.S.; Vuppalanchi, R.; Van Natta, M.L.; Hallinan, E.; Kowdley, K.V.; Abdelmalek, M.; Neuschwander-Tetri, B.A.; Loomba, R.; Dasarathy, S.; Brandman, D.; et al. Vibration-Controlled Transient Elastography to Assess Fibrosis and Steatosis in Patients with Nonalcoholic Fatty Liver Disease. Clin. Gastroenterol. Hepatol. 2019, 17, 156–163.e2. [Google Scholar] [CrossRef]
- Zhang, X.; Zhao, L.; Ducatman, A.; Deng, C.; Ellen von Stackelberg, K.; Danford, C.J.; Zhang, X. Association of per- and polyfluoroalkyl substance exposure with fatty liver disease risk in US Adults. JHEP Rep. 2023, 5, 100694. [Google Scholar] [CrossRef]
- Fernandez, T.; Vinuela, M.; Vidal, C.; Barrera, F. Lifestyle changes in patients with non-alcoholic fatty liver disease: A systematic review and meta-analysis. PLoS ONE 2022, 17, e0263931. [Google Scholar] [CrossRef]
- Deng, P.; Durham, J.; Liu, J.; Zhang, X.; Wang, C.; Li, D.; Gwag, T.; Ma, M.; Hennig, B. Metabolomic, Lipidomic, Transcriptomic, and Metagenomic Analyses in Mice Exposed to PFOS and Fed Soluble and Insoluble Dietary Fibers. Environ. Health Perspect. 2022, 130, 117003. [Google Scholar] [CrossRef]
- Liu, Z.; Suo, C.; Fan, H.; Zhang, T.; Jin, L.; Chen, X. Dissecting causal relationships between nonalcoholic fatty liver disease proxied by chronically elevated alanine transaminase levels and 34 extrahepatic diseases. Metab. Clin. Exp. 2022, 135, 155270. [Google Scholar] [CrossRef]
- Kim, W.R.; Flamm, S.L.; Di Bisceglie, A.M.; Bodenheimer, H.C. Public Policy Committee of the American Association for the Study of Liver, D. Serum activity of alanine aminotransferase (ALT) as an indicator of health and disease. Hepatology 2008, 47, 1363–1370. [Google Scholar] [CrossRef]
- Ioannou, G.N.; Weiss, N.S.; Boyko, E.J.; Mozaffarian, D.; Lee, S.P. Elevated serum alanine aminotransferase activity and calculated risk of coronary heart disease in the United States. Hepatology 2006, 43, 1145–1151. [Google Scholar] [CrossRef]


{kind=link}
| Male (n = 12,672) d | Female (n = 15,788) e | ||
|---|---|---|---|
| Estimated cumulative PFOA (ng/mL) | Continuous | 1.035 (1.005, 1.066) | 1.039 (1.015, 1.063) |
| Quintile2 b | 1.127 (0.999, 1.272) | 1.067 (0.962, 1.183) | |
| Quintile3 | 1.193 (1.058, 1.346) | 1.083 (0.976, 1.202) | |
| Quintile4 | 1.216 (1.075, 1.375) | 1.044 (0.941, 1.160) | |
| Quintile5 | 1.180 (1.025, 1.358) | 1.219 (1.095, 1.356) | |
| Test for trend c | 0.01 | 0.0005 | |
| Measured serum PFOA in 2005–2006 (ng/mL) | Continuous | 1.090 (1.055, 1.126) | 1.070 (1.041, 1.099) |
| Quintile2 b | 1.120 (0.992, 1.264) | 1.145 (1.032, 1.270) | |
| Quintile3 | 1.194 (1.057, 1.348) | 1.207 (1.087, 1.340) | |
| Quintile4 | 1.208 (1.068, 1.366) | 1.175 (1.057, 1.306) | |
| Quintile5 | 1.333 (1.173, 1.516) | 1.294 (1.162, 1.440) | |
| Test for trend c | 0.02 | <0.001 |
| Male (n = 12,672) d | Female (n = 15,788) e | ||
|---|---|---|---|
| Estimated cumulative PFOA (ng/mL) | Continuous | 1.040 (1.009, 1.072) | 1.033 (1.005, 1.062) |
| Quintile2 b | 1.135 (0.999, 1.290) | 1.118 (0.988, 1.266) | |
| Quintile3 | 1.244 (1.096, 1.413) | 1.056 (0.931, 1.199) | |
| Quintile4 | 1.273 (1.118, 1.448) | 1.068 (0.940, 1.213) | |
| Quintile5 | 1.205 (1.038, 1.398) | 1.192 (1.048, 1.355) | |
| Test for trend c | 0.006 | 0.02 | |
| Measured serum PFOA in 2005–2006 (ng/mL) | Continuous | 1.094 (1.057, 1.133) | 1.043 (1.010, 1.077) |
| Quintile2 b | 1.128 (0.993, 1.283) | 1.150 (1.014, 1.304) | |
| Quintile3 | 1.233 (1.084, 1.402) | 1.116 (0.982, 1.267) | |
| Quintile4 | 1.202 (1.054, 1.370) | 1.086 (0.955, 1.236) | |
| Quintile5 | 1.351 (1.179, 1.549) | 1.202 (1.056, 1.369) | |
| Test for trend c | <0.001 | 0.005 |
| Estimated Cumulative PFOA (ng/mL) | Measured Serum PFOA in 2005–2006 (ng/mL) | |
|---|---|---|
| Normal or underweight, BMI ≤ 25, n = 8215 | ||
| Continuous | 0.010 (0.003, 0.016) | 0.019 (0.012, 0.027) |
| Quintile2 b | 0.044 (0.014, 0.074) | 0.003 (−0.028, 0.033) |
| Quintile3 | 0.037 (0.007, 0.068) | 0.020 (−0.010, 0.051) |
| Quintile4 | 0.030 (−0.001, 0.060) | 0.029 (−0.001, 0.060) |
| Quintile5 | 0.062 (0.031, 0.094) | 0.068 (0.038, 0.099) |
| Test for trend e | 0.006 | <0.001 |
| Overweight, BMI > 25, ≤ 30, n = 10,074 | ||
| Continuous | 0.011 (0.004, 0.017) | 0.031 (0.024, 0.039) |
| Quintile2 c | −0.001 (−0.029, 0.027) | 0.053 (0.025, 0.081) |
| Quintile3 | 0.031 (0.003, 0.059) | 0.090 (0.061, 0.118) |
| Quintile4 | 0.042 (0.013, 0.070) | 0.102 (0.074, 0.131) |
| Quintile5 | 0.033 (0.002, 0.064) | 0.117 (0.088, 0.147) |
| Test for trend e | 0.001 | <0.001 |
| Obese BMI > 30, n = 10,171 | ||
| Continuous | 0.010 (0.003, 0.016) | 0.030 (0.022, 0.038) |
| Quintile2 d | 0.032 (0.004, 0.060) | 0.064 (0.036, 0.092) |
| Quintile3 | 0.041 (0.012, 0.069) | 0.073 (0.044, 0.101) |
| Quintile4 | 0.033 (0.005, 0.062) | 0.074 (0.046, 0.103) |
| Quintile5 | 0.057 (0.027, 0.088) | 0.115 (0.086, 0.145) |
| Test for trend e | 0.006 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ducatman, A.; Tan, Y.; Nadeau, B.; Steenland, K. Perfluorooctanoic Acid (PFOA) Exposure and Abnormal Alanine Aminotransferase: Using Clinical Consensus Cutoffs Compared to Statistical Cutoffs for Abnormal Values. Toxics 2023, 11, 449. https://doi.org/10.3390/toxics11050449
Ducatman A, Tan Y, Nadeau B, Steenland K. Perfluorooctanoic Acid (PFOA) Exposure and Abnormal Alanine Aminotransferase: Using Clinical Consensus Cutoffs Compared to Statistical Cutoffs for Abnormal Values. Toxics. 2023; 11(5):449. https://doi.org/10.3390/toxics11050449
Chicago/Turabian StyleDucatman, Alan, Youran Tan, Brian Nadeau, and Kyle Steenland. 2023. "Perfluorooctanoic Acid (PFOA) Exposure and Abnormal Alanine Aminotransferase: Using Clinical Consensus Cutoffs Compared to Statistical Cutoffs for Abnormal Values" Toxics 11, no. 5: 449. https://doi.org/10.3390/toxics11050449