
Per- and Polyfluoroalkyl Substances (PFAS) Mixture during Pregnancy and Postpartum Weight Retention in the New Hampshire Birth Cohort Study (NHBCS)
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
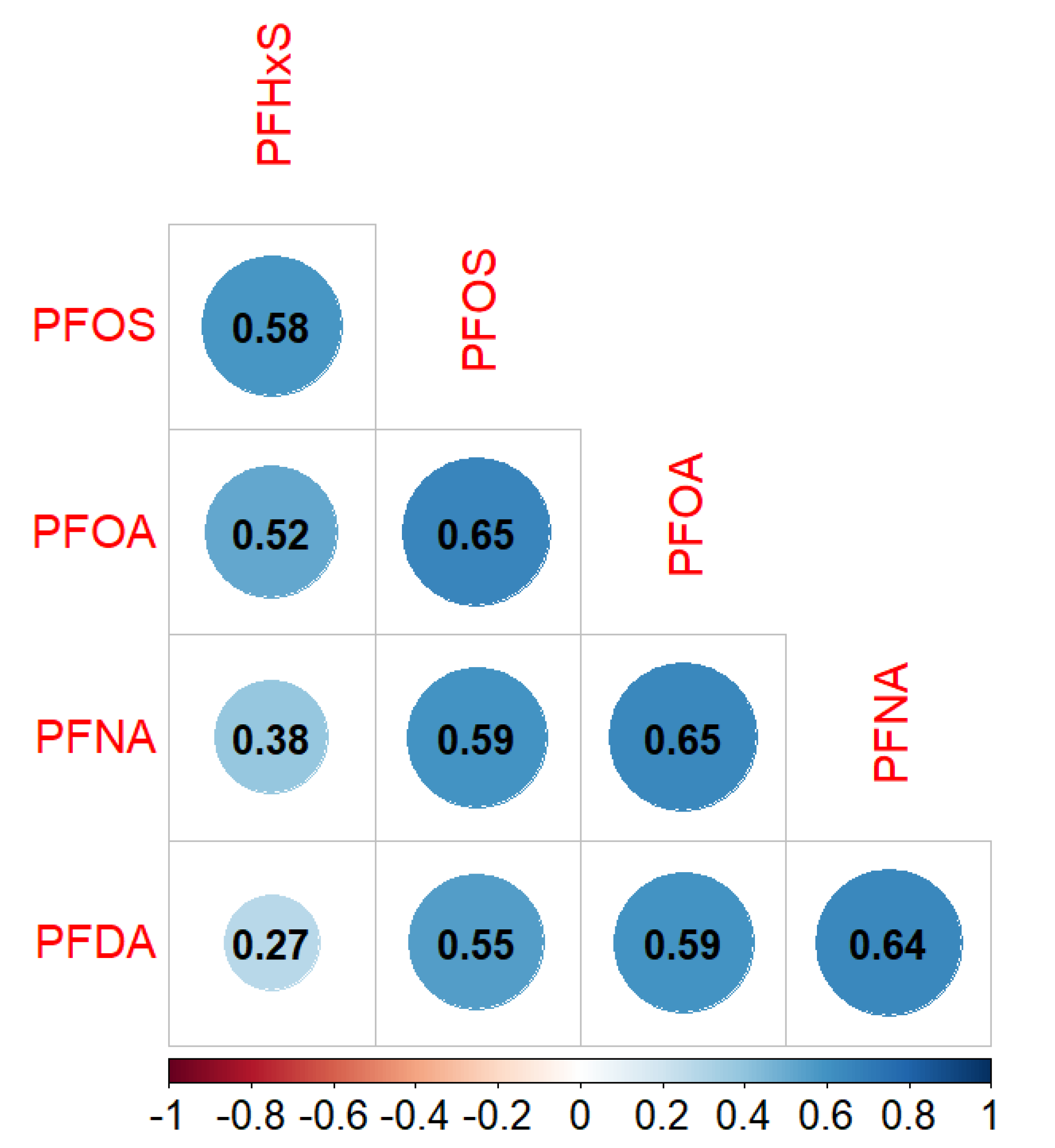
2.2. Plasma PFAS during Pregnancy
2.3. Weight Retention
2.4. Covariates
2.5. Statistical Analysis
2.5.1. Main Analyses
2.5.2. Secondary Analyses
2.5.3. Sensitivity Analyses
3. Results
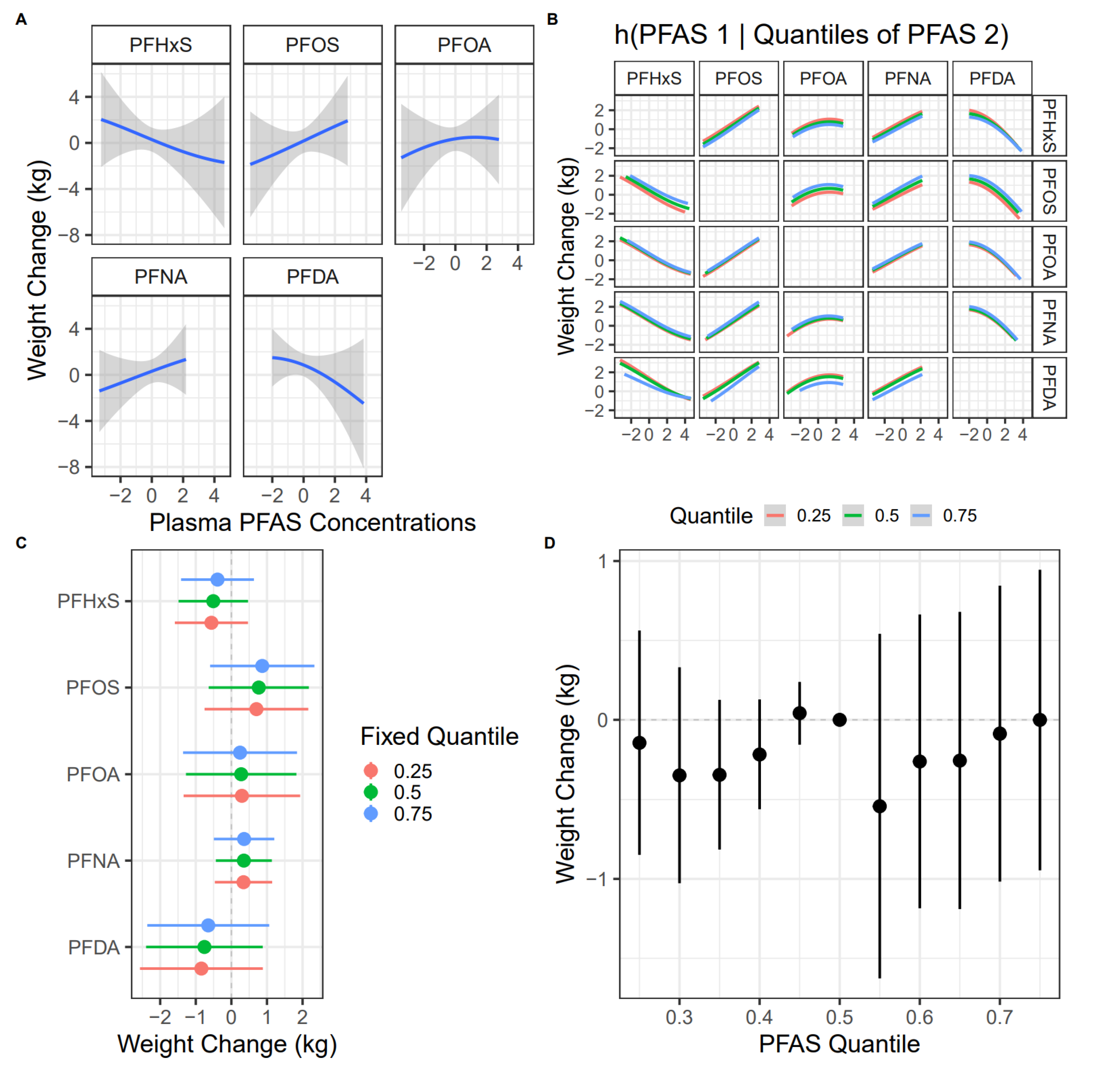
3.1. PFAS Mixture and Postpartum Weight Change
3.2. Individual PFAS and Postpartum Weight Change
3.3. Effect Modification by Pre-Pregnancy BMI
3.4. Effect Modification by GWG
3.5. Sensitivity Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| PFAS | Per- and polyfluoroalkyl substances |
| NHBCS | New Hampshire Birth Cohort Study |
| PFOS | Perfluorooctane sulfonate |
| PFOA | Perfluorooctanoate |
| PFNA | Perfluorononanoate |
| BMI | Body mass index |
| CVDs | Cardiovascular diseases |
| GWG | Gestational weight gain |
| PPAR | Peroxisome proliferator-activated receptor |
| SD | Standard deviation |
| CDC | Centers for Disease Control and Prevention |
| PFHxS | Perfluorohexane sulfonate |
| PFDA | Perfluorodecanoate |
| PFUnDA | Perfluoroundecanoate |
| MeFOSAA | 2–(N–methyl–perfluorooctane sulfonamido) acetate |
| LOD | Limit of detection |
| FFQ | Food frequency questionnaire |
| AHEI-2010 | Alternative Healthy Eating Index-2010 |
| BKMR | Bayesian kernel machine regression |
| PIP | Posterior inclusion probability |
| IQR | Interquartile range |
| CI | Confidence interval |
| NHANES | National Health and Nutrition Examination Survey |
| POUNDS | Preventing Overweight Using Novel Dietary Strategies |
| C/EBPα | CCAAT/enhancer-binding protein-α |
| ER | Estrogen receptor |
References
- Hales, C.M.; Carroll, M.D.; Fryar, C.D.; Ogden, C.L. Prevalence of Obesity and Severe Obesity among Adults: United States, 2017–2018. NCHS Data Brief 2020, 1–8. [Google Scholar]
- Santangeli, L.; Sattar, N.; Huda, S.S. Impact of Maternal Obesity on Perinatal and Childhood Outcomes. Best Pract. Res. Clin. Obstet. Gynaecol. 2015, 29, 438–448. [Google Scholar] [CrossRef] [PubMed]
- Williams, D. Pregnancy: A Stress Test for Life. Curr. Opin. Obstet. Gynecol. 2003, 15, 465–471. [Google Scholar] [CrossRef] [PubMed]
- Godfrey, K.M.; Reynolds, R.M.; Prescott, S.L.; Nyirenda, M.; Jaddoe, V.W.V.; Eriksson, J.G.; Broekman, B.F.P. Influence of Maternal Obesity on the Long-Term Health of Offspring. Lancet Diabetes Endocrinol. 2017, 5, 53–64. [Google Scholar] [CrossRef]
- Rössner, S.; Ohlin, A. Pregnancy as a Risk Factor for Obesity: Lessons from the Stockholm Pregnancy and Weight Development Study. Obes. Res. 1995, 3 (Suppl. S2), 267s–275s. [Google Scholar] [CrossRef]
- Gore, S.A.; Brown, D.M.; West, D.S. The Role of Postpartum Weight Retention in Obesity among Women: A Review of the Evidence. Ann. Behav. Med. 2003, 26, 149–159. [Google Scholar] [CrossRef]
- Soria-Contreras, D.C.; Trejo-Valdivia, B.; Cantoral, A.; Pizano-Zárate, M.L.; Baccarelli, A.A.; Just, A.C.; Colicino, E.; Deierlein, A.L.; Wright, R.O.; Oken, E.; et al. Patterns of Weight Change One Year after Delivery Are Associated with Cardiometabolic Risk Factors at Six Years Postpartum in Mexican Women. Nutrients 2020, 12, 170. [Google Scholar] [CrossRef]
- Gillman, M.W. Interrupting Intergenerational Cycles of Maternal Obesity. In Preventive Aspects of Early Nutrition: 85th Nestlé Nutrition Institute Workshop, London, UK, 17–19 November 2016; Nestlé Nutrition Institute Workshop Series; Karger Medical and Scientific Publishers: Basel, Switzerland, 2016; Volume 85, pp. 59–69. [Google Scholar] [CrossRef]
- van der Pligt, P.; Willcox, J.; Hesketh, K.D.; Ball, K.; Wilkinson, S.; Crawford, D.; Campbell, K. Systematic Review of Lifestyle Interventions to Limit Postpartum Weight Retention: Implications for Future Opportunities to Prevent Maternal Overweight and Obesity Following Childbirth. Obes. Rev. 2013, 14, 792–805. [Google Scholar] [CrossRef]
- Buck, R.C.; Franklin, J.; Berger, U.; Conder, J.M.; Cousins, I.T.; de Voogt, P.; Jensen, A.A.; Kannan, K.; Mabury, S.A.; van Leeuwen, S.P. Perfluoroalkyl and Polyfluoroalkyl Substances in the Environment: Terminology, Classification, and Origins. Integr. Environ. Assess. Manag. 2011, 7, 513–541. [Google Scholar] [CrossRef]
- Stahl, T.; Mattern, D.; Brunn, H. Toxicology of Perfluorinated Compounds. Environ. Sci. Eur. 2011, 23, 38. [Google Scholar] [CrossRef]
- AR226-0550; 3M Company Fluorochemical Use, Distribution and Release Overview. United States Environmental Protection Agency: Washington, DC, USA, 1999.
- Modaresi, S.M.S.; Wei, W.; Emily, M.; DaSilva, N.A.; Slitt, A.L. Per- and Polyfluoroalkyl Substances (PFAS) Augment Adipogenesis and Shift the Proteome in Murine 3T3-L1 Adipocytes. Toxicology 2022, 465, 153044. [Google Scholar] [CrossRef] [PubMed]
- Kirk, A.B.; Michelsen-Correa, S.; Rosen, C.; Martin, C.F.; Blumberg, B. PFAS and Potential Adverse Effects on Bone and Adipose Tissue Through Interactions with PPARγ. Endocrinology 2021, 162, bqab194. [Google Scholar] [CrossRef] [PubMed]
- Qi, W.; Clark, J.M.; Timme-Laragy, A.R.; Park, Y. Per- and Polyfluoroalkyl Substances and Obesity, Type 2 Diabetes and Non-Alcoholic Fatty Liver Disease: A Review of Epidemiologic Findings. Toxicol. Environ. Chem. 2020, 102, 1–36. [Google Scholar] [CrossRef] [PubMed]
- Costantine, M. Physiologic and Pharmacokinetic Changes in Pregnancy. Front. Pharmacol. 2014, 5, 65. [Google Scholar] [CrossRef]
- Mitro, S.D.; Sagiv, S.K.; Rifas-Shiman, S.L.; Calafat, A.M.; Fleisch, A.F.; Jaacks, L.M.; Williams, P.L.; Oken, E.; James-Todd, T.M. Per- and Polyfluoroalkyl Substance Exposure, Gestational Weight Gain, and Postpartum Weight Changes in Project Viva. Obesity 2020, 28, 1984–1992. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. National Report on Human Exposure to Environmental Chemicals; CDC: Atlanta, GA, USA, 2022.
- Kato, K.; Kalathil, A.A.; Patel, A.M.; Ye, X.; Calafat, A.M. Per- and Polyfluoroalkyl Substances and Fluorinated Alternatives in Urine and Serum by on-Line Solid Phase Extraction–Liquid Chromatography–Tandem Mass Spectrometry. Chemosphere 2018, 209, 338–345. [Google Scholar] [CrossRef]
- Hornung, R.W.; Reed, L.D. Estimation of Average Concentration in the Presence of Nondetectable Values. Null 1990, 5, 46–51. [Google Scholar] [CrossRef]
- Chiuve, S.E.; Fung, T.T.; Rimm, E.B.; Hu, F.B.; McCullough, M.L.; Wang, M.; Stampfer, M.J.; Willett, W.C. Alternative Dietary Indices Both Strongly Predict Risk of Chronic Disease. J. Nutr. 2012, 142, 1009–1018. [Google Scholar] [CrossRef]
- Emond, J.A.; Karagas, M.R.; Baker, E.R.; Gilbert-Diamond, D. Better Diet Quality during Pregnancy Is Associated with a Reduced Likelihood of an Infant Born Small for Gestational Age: An Analysis of the Prospective New Hampshire Birth Cohort Study. J. Nutr. 2018, 148, 22–30. [Google Scholar] [CrossRef]
- Hutcheon, J.A.; Platt, R.W.; Abrams, B.; Himes, K.P.; Simhan, H.N.; Bodnar, L.M. A Weight-Gain-for-Gestational-Age z Score Chart for the Assessment of Maternal Weight Gain in Pregnancy. Am. J. Clin. Nutr. 2013, 97, 1062–1067. [Google Scholar] [CrossRef]
- Nielsen, C.; Andersson Hall, U.; Lindh, C.; Ekström, U.; Xu, Y.; Li, Y.; Holmäng, A.; Jakobsson, K. Pregnancy-Induced Changes in Serum Concentrations of Perfluoroalkyl Substances and the Influence of Kidney Function. Environ. Health 2020, 19, 80. [Google Scholar] [CrossRef] [PubMed]
- Ashley-Martin, J.; Dodds, L.; Arbuckle, T.E.; Morisset, A.-S.; Fisher, M.; Bouchard, M.F.; Shapiro, G.D.; Ettinger, A.S.; Monnier, P.; Dallaire, R.; et al. Maternal and Neonatal Levels of Perfluoroalkyl Substances in Relation to Gestational Weight Gain. Int. J. Environ. Res. Public Health 2016, 13, 146. [Google Scholar] [CrossRef] [PubMed]
- Jaacks, L.M.; Boyd Barr, D.; Sundaram, R.; Grewal, J.; Zhang, C.; Buck Louis, G.M. Pre-Pregnancy Maternal Exposure to Persistent Organic Pollutants and Gestational Weight Gain: A Prospective Cohort Study. Int. J. Environ. Res. Public Health 2016, 13, 905. [Google Scholar] [CrossRef] [PubMed]
- Marks, K.J.; Jeddy, Z.; Flanders, W.D.; Northstone, K.; Fraser, A.; Calafat, A.M.; Kato, K.; Hartman, T.J. Maternal Serum Concentrations of Perfluoroalkyl Substances during Pregnancy and Gestational Weight Gain: The Avon Longitudinal Study of Parents and Children. Reprod. Toxicol. 2019, 90, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Romano, M.E.; Gallagher, L.G.; Eliot, M.N.; Calafat, A.M.; Chen, A.; Yolton, K.; Lanphear, B.; Braun, J.M. Per- and Polyfluoroalkyl Substance Mixtures and Gestational Weight Gain among Mothers in the Health Outcomes and Measures of the Environment Study. Int. J. Hyg. Environ. Health 2021, 231, 113660. [Google Scholar] [CrossRef]
- Liu, G.; Dhana, K.; Furtado, J.D.; Rood, J.; Zong, G.; Liang, L.; Qi, L.; Bray, G.A.; DeJonge, L.; Coull, B.; et al. Perfluoroalkyl Substances and Changes in Body Weight and Resting Metabolic Rate in Response to Weight-Loss Diets: A Prospective Study. PLoS Med. 2018, 15, e1002502. [Google Scholar] [CrossRef]
- Cardenas, A.; Hauser, R.; Gold, D.R.; Kleinman, K.P.; Hivert, M.-F.; Fleisch, A.F.; Lin, P.-I.D.; Calafat, A.M.; Webster, T.F.; Horton, E.S.; et al. Association of Perfluoroalkyl and Polyfluoroalkyl Substances with Adiposity. JAMA Netw. Open 2018, 1, e181493. [Google Scholar] [CrossRef]
- Heindel, J.J.; Newbold, R.; Schug, T.T. Endocrine Disruptors and Obesity. Nat. Rev. Endocrinol. 2015, 11, 653–661. [Google Scholar] [CrossRef]
- Vanden Heuvel, J.P.; Thompson, J.T.; Frame, S.R.; Gillies, P.J. Differential Activation of Nuclear Receptors by Perfluorinated Fatty Acid Analogs and Natural Fatty Acids: A Comparison of Human, Mouse, and Rat Peroxisome Proliferator-Activated Receptor-α, -β, and -γ, Liver X Receptor-β, and Retinoid X Receptor-α. Toxicol. Sci. 2006, 92, 476–489. [Google Scholar] [CrossRef]
- Gross, B.; Pawlak, M.; Lefebvre, P.; Staels, B. PPARs in Obesity-Induced T2DM, Dyslipidaemia and NAFLD. Nat. Rev. Endocrinol. 2017, 13, 36–49. [Google Scholar] [CrossRef]
- Jones, J.R.; Barrick, C.; Kim, K.-A.; Lindner, J.; Blondeau, B.; Fujimoto, Y.; Shiota, M.; Kesterson, R.A.; Kahn, B.B.; Magnuson, M.A. Deletion of PPARgamma in Adipose Tissues of Mice Protects against High Fat Diet-Induced Obesity and Insulin Resistance. Proc. Natl. Acad. Sci. USA 2005, 102, 6207–6212. [Google Scholar] [CrossRef]
- Wang, F.; Mullican, S.E.; DiSpirito, J.R.; Peed, L.C.; Lazar, M.A. Lipoatrophy and Severe Metabolic Disturbance in Mice with Fat-Specific Deletion of PPARγ. Proc. Natl. Acad. Sci. USA 2013, 110, 18656–18661. [Google Scholar] [CrossRef] [PubMed]
- Semple, R.K.; Chatterjee, V.K.K.; O’Rahilly, S. PPAR Gamma and Human Metabolic Disease. J. Clin. Investig. 2006, 116, 581–589. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Qin, H.; Pan, Y.; Luo, F.; Zhang, Z. Low Concentrations of Perfluorooctane Sulfonate Repress Osteogenic and Enhance Adipogenic Differentiation of Human Mesenchymal Stem Cells. Toxicol. Appl. Pharmacol. 2019, 367, 82–91. [Google Scholar] [CrossRef] [PubMed]
- Kjeldsen, L.S.; Bonefeld-Jørgensen, E.C. Perfluorinated Compounds Affect the Function of Sex Hormone Receptors. Environ. Sci. Pollut. Res. 2013, 20, 8031–8044. [Google Scholar] [CrossRef] [PubMed]
- Benninghoff, A.D.; Bisson, W.H.; Koch, D.C.; Ehresman, D.J.; Kolluri, S.K.; Williams, D.E. Estrogen-Like Activity of Perfluoroalkyl Acids In Vivo and Interaction with Human and Rainbow Trout Estrogen Receptors In Vitro. Toxicol. Sci. 2011, 120, 42–58. [Google Scholar] [CrossRef]
- Houck, K.A.; Patlewicz, G.; Richard, A.M.; Williams, A.J.; Shobair, M.A.; Smeltz, M.; Clifton, M.S.; Wetmore, B.; Medvedev, A.; Makarov, S. Bioactivity Profiling of Per- and Polyfluoroalkyl Substances (PFAS) Identifies Potential Toxicity Pathways Related to Molecular Structure. Toxicology 2021, 457, 152789. [Google Scholar] [CrossRef]
- Evans, N.; Conley, J.M.; Cardon, M.; Hartig, P.; Medlock-Kakaley, E.; Gray, L.E.J. In Vitro Activity of a Panel of Per- and Polyfluoroalkyl Substances (PFAS), Fatty Acids, and Pharmaceuticals in Peroxisome Proliferator-Activated Receptor (PPAR) Alpha, PPAR Gamma, and Estrogen Receptor Assays. Toxicol. Appl. Pharmacol. 2022, 449, 116136. [Google Scholar] [CrossRef]
- Villeneuve, D.L.; Blackwell, B.R.; Cavallin, J.E.; Collins, J.; Hoang, J.X.; Hofer, R.N.; Houck, K.A.; Jensen, K.M.; Kahl, M.D.; Kutsi, R.N.; et al. Verification of In Vivo Estrogenic Activity for Four Per- and Polyfluoroalkyl Substances (PFAS) Identified as Estrogen Receptor Agonists via New Approach Methodologies. Environ. Sci. Technol. 2023, 57, 3794–3803. [Google Scholar] [CrossRef]
- Li, J.; Cao, H.; Feng, H.; Xue, Q.; Zhang, A.; Fu, J. Evaluation of the Estrogenic/Antiestrogenic Activities of Perfluoroalkyl Substances and Their Interactions with the Human Estrogen Receptor by Combining In Vitro Assays and In Silico Modeling. Environ. Sci. Technol. 2020, 54, 14514–14524. [Google Scholar] [CrossRef]
- Mahboobifard, F.; Pourgholami, M.H.; Jorjani, M.; Dargahi, L.; Amiri, M.; Sadeghi, S.; Tehrani, F.R. Estrogen as a Key Regulator of Energy Homeostasis and Metabolic Health. Biomed. Pharmacother. 2022, 156, 113808. [Google Scholar] [CrossRef] [PubMed]
- Mauvais-Jarvis, F.; Clegg, D.J.; Hevener, A.L. The Role of Estrogens in Control of Energy Balance and Glucose Homeostasis. Endocr. Rev. 2013, 34, 309–338. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, K.M.; Yaktine, A.L. (Eds.) Weight Gain During Pregnancy: Reexamining the Guidelines; National Academies Press (US): Washington, DC, USA, 2009; ISBN 978-0-309-13113-1. [Google Scholar]
- Kozhimannil, K.B.; Interrante, J.D.; Corbett, A.; Heppner, S.; Burges, J.; Henning-Smith, C. Rural Focus and Representation in State Maternal Mortality Review Committees: Review of Policy and Legislation. Womens Health Issues 2019, 29, 357–363. [Google Scholar] [CrossRef] [PubMed]
- Pan, Y.; Zhu, Y.; Zheng, T.; Cui, Q.; Buka, S.L.; Zhang, B.; Guo, Y.; Xia, W.; Yeung, L.W.Y.; Li, Y.; et al. Novel Chlorinated Polyfluorinated Ether Sulfonates and Legacy Per-/Polyfluoroalkyl Substances: Placental Transfer and Relationship with Serum Albumin and Glomerular Filtration Rate. Environ. Sci. Technol. 2017, 51, 634–644. [Google Scholar] [CrossRef]
- Eryasa, B.; Grandjean, P.; Nielsen, F.; Valvi, D.; Zmirou-Navier, D.; Sunderland, E.; Weihe, P.; Oulhote, Y. Physico-Chemical Properties and Gestational Diabetes Predict Transplacental Transfer and Partitioning of Perfluoroalkyl Substances. Environ. Int. 2019, 130, 104874. [Google Scholar] [CrossRef]
- Gützkow, K.B.; Haug, L.S.; Thomsen, C.; Sabaredzovic, A.; Becher, G.; Brunborg, G. Placental Transfer of Perfluorinated Compounds Is Selective—A Norwegian Mother and Child Sub-Cohort Study. Int. J. Hyg. Environ. Health 2012, 215, 216–219. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Mean ± SD/N (%) | |
|---|---|---|
| Maternal Age (years) | 32 ± 4.6 | |
| Self-Reported Race/Ethnicity | ||
| Non-Hispanic White | 451 (93.6) | |
| Other | 30 (6.2) | |
| Missing | 1 (0.2) | |
| Maternal Highest Education | ||
| Less Than College | 110 (22.8) | |
| College Graduate or Above | 349 (72.4) | |
| Missing | 23 (4.8) | |
| Marital Status | ||
| Married | 406 (84.2) | |
| Other | 55 (11.4) | |
| Missing | 21 (4.4) | |
| Maternal Pre-Pregnancy BMI (kg/m2) | 26 ± 6.0 | |
| Parity | ||
| 0 | 186 (38.6) | |
| ≥1 | 293 (60.8) | |
| Missing | 3 (0.6) | |
| Lactation Duration Before the Study Pregnancy (months) | 9 ± 12.4 | |
| Weight Gain During Pregnancy (kg) | 15 ± 6.7 | |
| Smoking Status | ||
| Never | 427 (88.6) | |
| Current | 27 (5.6) | |
| Former | 28 (5.8) | |
| Alternative Healthy Eating Index (AHEI 2010) Score | 58 ± 12.7 | |
| Physical Activity | ||
| Sedentary Time (hours/week) | 8.5 ± 6.0 | |
| Vigorous Exercise Time (hours/week) | 3.0 ± 3.4 | |
| Gestational Week of Blood Sample (weeks) | 28 ± 2.4 | |
| Additional Pregnancies After the Study Pregnancy | ||
| Yes | 152 (31.5) | |
| No | 328 (68.0) | |
| Missing | 2 (0.4) | |
| Postpartum Weight Change (kg) | 4.1 ± 8.8 | |
| Median (IQR) | ||
| Plasma PFAS Concentrations (ng/mL) | ||
| PFHxS | 0.7 (0.50, 1.00) | |
| PFOS | 3.2 (2.22, 4.70) | |
| PFOA | 1.1 (0.74, 1.64) | |
| PFNA | 0.5 (0.32, 0.70) | |
| PFDA | 0.1 (<LOD 1, 0.20) | |
| Median (Range) | ||
| Enrollment Year | ||
| 2013 (2009–2018) | ||
| PFAS | Postpartum Weight Change (95% CI) | ||
|---|---|---|---|
| Overall (n = 433) | Obese/Overweight (n = 191) | Healthy/Underweight (n = 242) | |
| PFHxS | 0.02 (−0.81, 0.86) | 0.15 (−0.98, 1.27) | 0.05 (−1.09, 1.19) |
| PFOS | 0.80 (−0.28, 1.88) | 1.76 (0.31, 3.22) | 0.10 (−1.24, 1.44) |
| PFOA | 0.57 (−0.70, 1.84) | 1.39 (−0.27, 3.04) | 0.17 (−1.31, 1.65) |
| PFNA | 0.54 (−0.26, 1.34) | 1.04 (−0.19, 2.28) | 0.22 (−0.74, 1.18) |
| PFDA | −0.01 (−0.93, 0.92) | 0.49 (−0.84, 1.81) | −0.40 (−1.59, 0.78) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.; Howe, C.; Gallagher, L.G.; Botelho, J.C.; Calafat, A.M.; Karagas, M.R.; Romano, M.E. Per- and Polyfluoroalkyl Substances (PFAS) Mixture during Pregnancy and Postpartum Weight Retention in the New Hampshire Birth Cohort Study (NHBCS). Toxics 2023, 11, 450. https://doi.org/10.3390/toxics11050450
Wang Y, Howe C, Gallagher LG, Botelho JC, Calafat AM, Karagas MR, Romano ME. Per- and Polyfluoroalkyl Substances (PFAS) Mixture during Pregnancy and Postpartum Weight Retention in the New Hampshire Birth Cohort Study (NHBCS). Toxics. 2023; 11(5):450. https://doi.org/10.3390/toxics11050450
Chicago/Turabian StyleWang, Yuting, Caitlin Howe, Lisa G. Gallagher, Julianne Cook Botelho, Antonia M. Calafat, Margaret R. Karagas, and Megan E. Romano. 2023. "Per- and Polyfluoroalkyl Substances (PFAS) Mixture during Pregnancy and Postpartum Weight Retention in the New Hampshire Birth Cohort Study (NHBCS)" Toxics 11, no. 5: 450. https://doi.org/10.3390/toxics11050450