
Cadmium-Induced Tubular Dysfunction in Type 2 Diabetes: A Population-Based Cross-Sectional Study
 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Cohort Participants
2.2. Urine and Blood Sampling and Analysis
2.3. Normalization of ECd to Ccr and Ecr
2.4. Estimated Glomerular Filtration Rate
2.5. Statistical Analysis
3. Results
3.1. Cohort Composition and Characteristics
3.2. Predictors of Tubular Proteinuria and Reduced eGFR
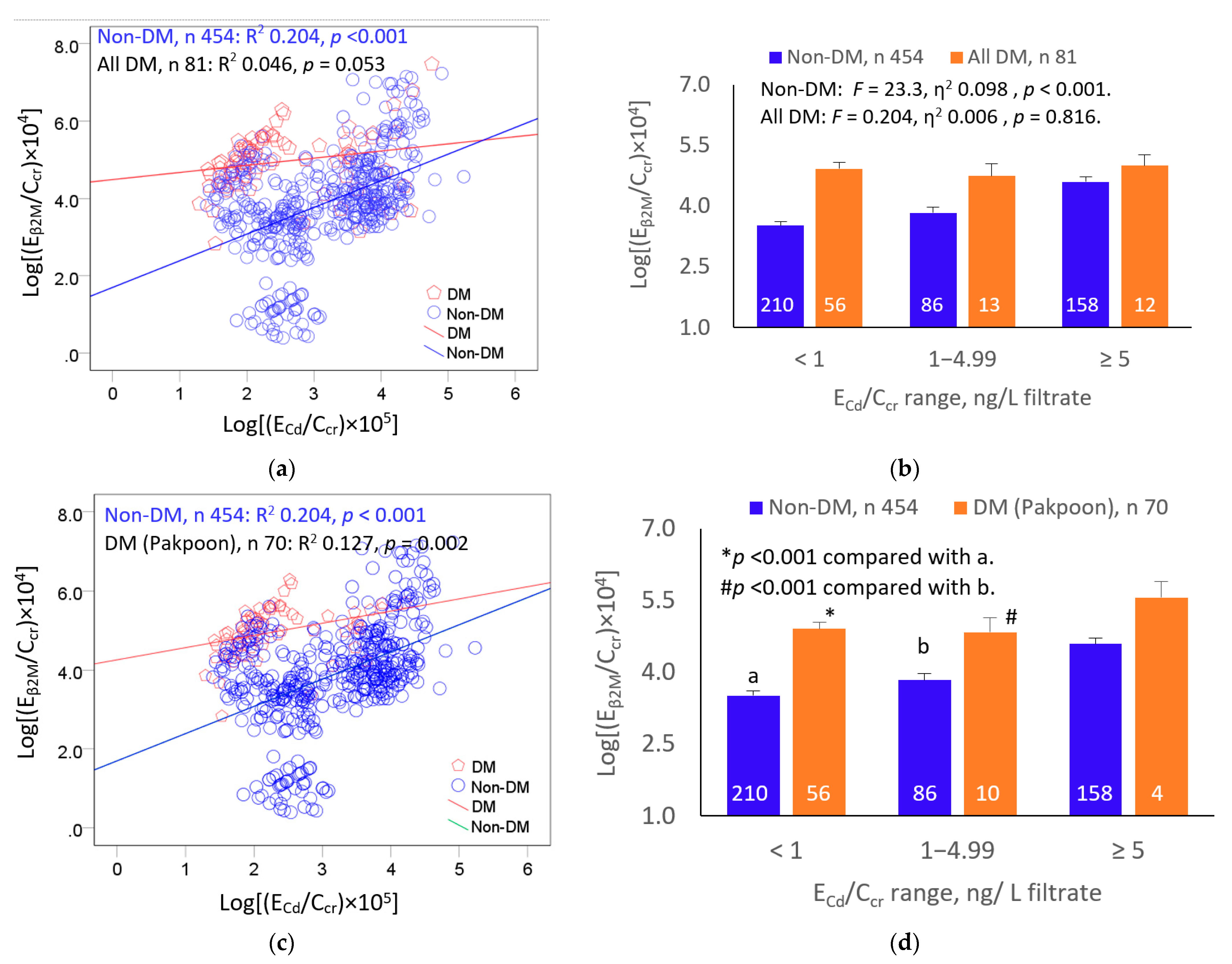
3.3. Effects of Cadmium and Diabetes on β2M Excretion
3.4. Inverse Association of eGFR and Cadmium
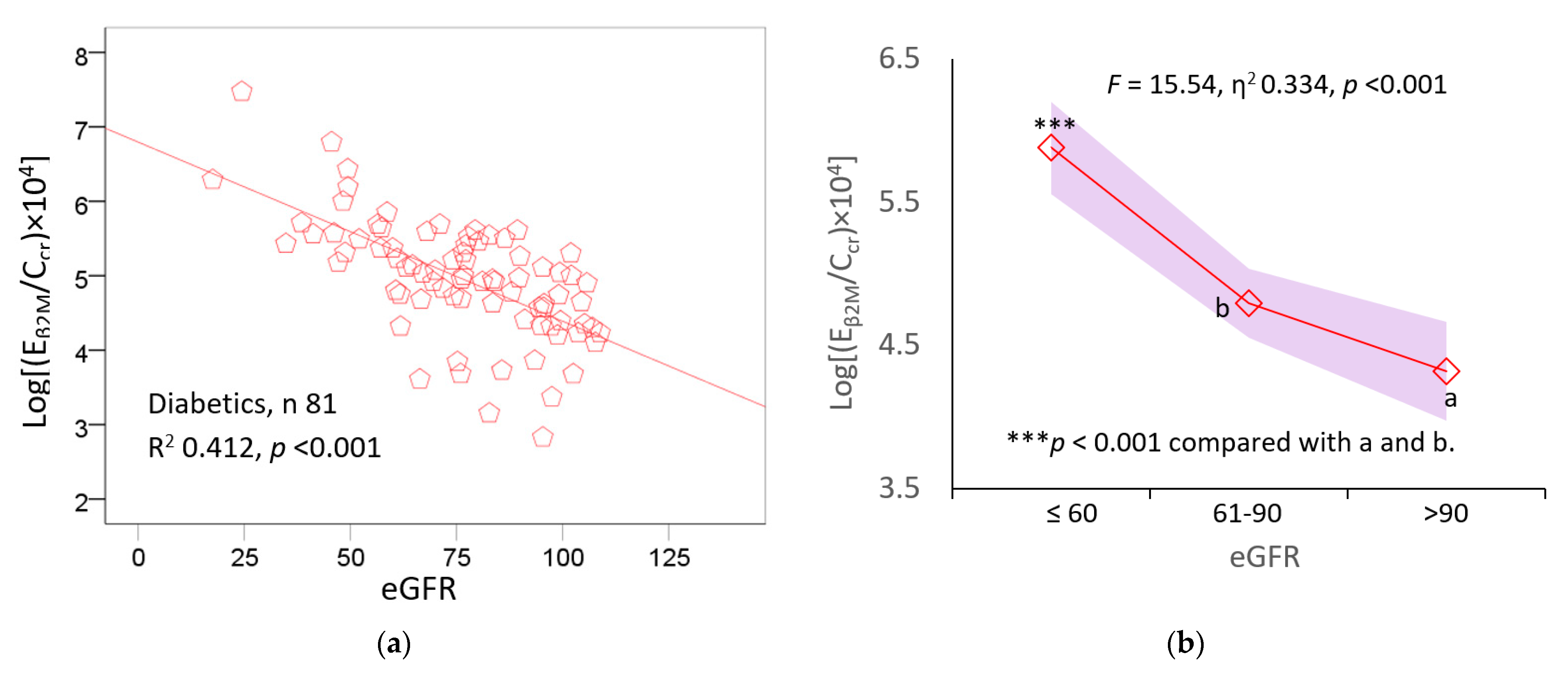
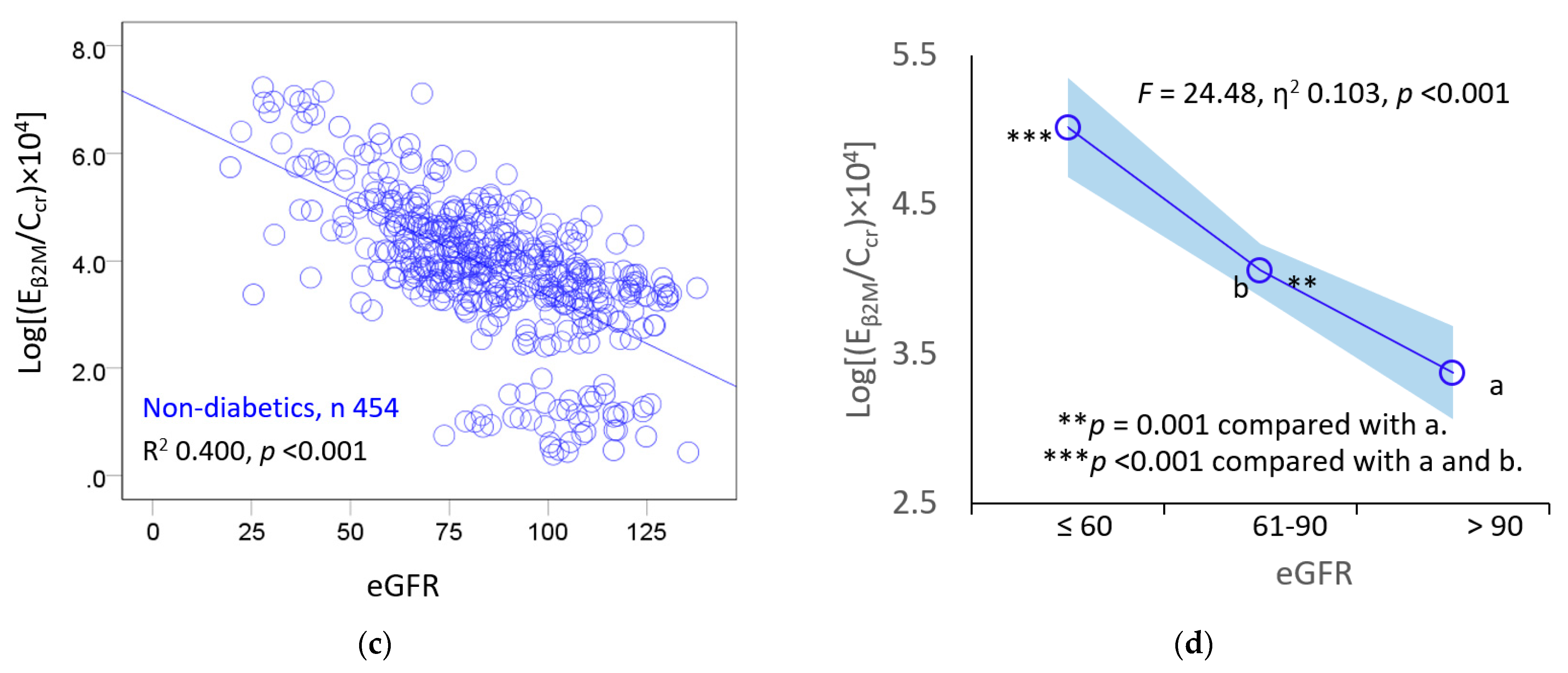
3.5. Inverse Association of β2M Excretion and eGFR
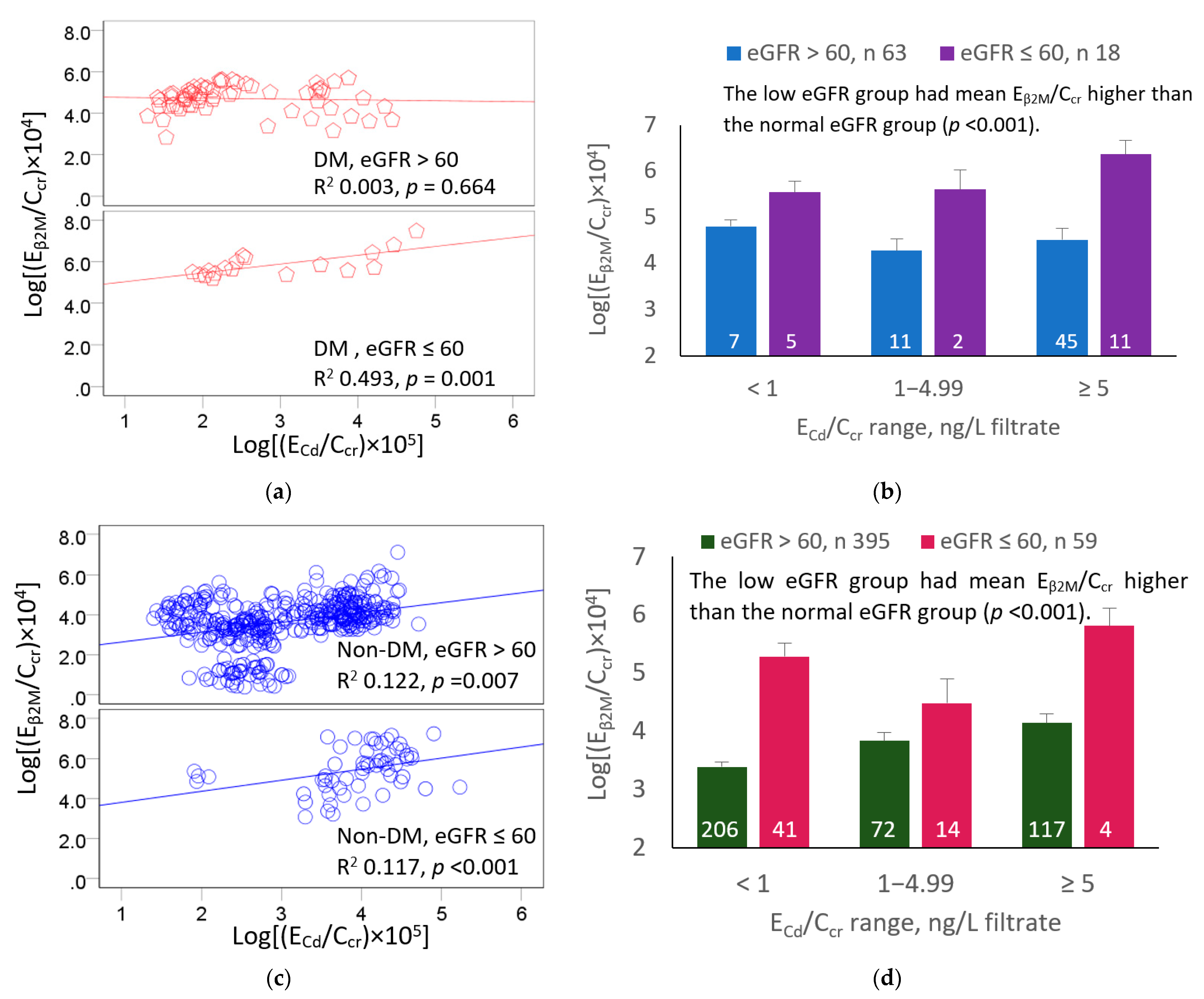
3.6. β2M Excretion as a Function of GFR and Kidney Cadmium Burden
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schwartz, G.G.; Il’yasova, D.; Ivanova, A. Urinary cadmium, impaired fasting glucose, and diabetes in the NHANES III. Diabetes Care 2003, 26, 468–470. [Google Scholar] [CrossRef] [PubMed]
- Wallia, A.; Allen, N.B.; Badon, S.; El Muayed, M. Association between urinary cadmium levels and prediabetes in the NHANES 2005–2010 population. Int. J. Hyg. Environ. Health 2014, 217, 854–860. [Google Scholar] [CrossRef] [PubMed]
- Little, B.B.; Reilly, R.; Walsh, B.; Vu, G.T. Cadmium is associated with type 2 diabetes in a Superfund Site Lead Smelter Community in Dallas, Texas. Int. J. Environ. Res. Public Health 2020, 17, 4558. [Google Scholar] [CrossRef]
- Xiao, L.; Li, W.; Zhu, C.; Yang, S.; Zhou, M.; Wang, B.; Wang, X.; Wang, D.; Ma, J.; Zhou, Y.; et al. Cadmium exposure, fasting blood glucose changes, and type 2 diabetes mellitus: A longitudinal prospective study in China. Environ. Res. 2021, 192, 110259. [Google Scholar] [CrossRef]
- Guo, F.F.; Hu, Z.Y.; Li, B.Y.; Qin, L.Q.; Fu, C.; Yu, H.; Zhang, Z.L. Evaluation of the association between urinary cadmium levels below threshold limits and the risk of diabetes mellitus: A dose-response meta-analysis. Environ. Sci. Pollut. Res. Int. 2019, 26, 19272–19281. [Google Scholar] [CrossRef] [PubMed]
- Filippini, T.; Wise, L.A.; Vinceti, M. Cadmium exposure and risk of diabetes and prediabetes: A systematic review and dose-response meta-analysis. Environ. Int. 2022, 158, 106920. [Google Scholar] [CrossRef]
- Buchet, J.P.; Lauwerys, R.; Roels, H.; Bernard, A.; Bruaux, P.; Claeys, F.; Ducoffre, G.; de Plaen, P.; Staessen, J.; Amery, A.; et al. Renal effects of cadmium body burden of the general population. Lancet 1990, 336, 699–702. [Google Scholar] [CrossRef]
- Akesson, A.; Lundh, T.; Vahter, M.; Bjellerup, P.; Lidfeldt, J.; Nerbrand, C.; Samsioe, G.; Strömberg, U.; Skerfving, S. Tubular and glomerular kidney effects in Swedish women with low environmental cadmium exposure. Environ. Health Perspect. 2005, 113, 1627–1631. [Google Scholar] [CrossRef]
- Barregard, L.; Bergstrom, G.; Fagerberg, B. Cadmium, type 2 diabetes, and kidney damage in a cohort of middle-aged women. Environ. Res. 2014, 135, 311–316. [Google Scholar] [CrossRef]
- Haswell-Elkins, M.; Satarug, S.; O’Rourke, P.; Moore, M.; Ng, J.; McGrath, V.; Walmby, M. Striking association between urinary cadmium level and albuminuria among Torres Strait Islander people with diabetes. Environ. Res. 2008, 106, 379–383. [Google Scholar] [CrossRef]
- Madrigal, J.M.; Ricardo, A.C.; Persky, V.; Turyk, M. Associations between blood cadmium concentration and kidney function in the U.S. population: Impact of sex, diabetes and hypertension. Environ. Res. 2018, 169, 180–188. [Google Scholar] [CrossRef]
- Hwangbo, Y.; Weaver, V.M.; Tellez-Plaza, M.; Guallar, E.; Lee, B.K.; Navas-Acien, A. Blood cadmium and estimated glomerular filtration rate in Korean adults. Environ. Health Perspect. 2011, 119, 1800–1805. [Google Scholar] [CrossRef] [PubMed]
- Wallin, M.; Sallsten, G.; Lundh, T.; Barregard, L. Low-level cadmium exposure and effects on kidney function. Occup. Environ. Med. 2014, 71, 848–854. [Google Scholar] [CrossRef] [PubMed]
- Satarug, S.; Vesey, D.A.; Gobe, G.C. Cadmium-induced proteinuria: Mechanistic insights from dose–effect analyses. Int. J. Mol. Sci. 2023, 24, 1893. [Google Scholar] [CrossRef] [PubMed]
- Järup, L.; Persson, B.; Elinder, C.G. Decreased glomerular filtration rate in solderers exposed to cadmium. Occup. Environ. Med. 1995, 52, 818–822. [Google Scholar] [CrossRef]
- Järup, L.; Persson, B.; Edling, C.; Elinder, C.G. Renal function impairment in workers previously exposed to cadmium. Nephron 1993, 64, 75–81. [Google Scholar] [CrossRef]
- Ferraro, P.M.; Costanzi, S.; Naticchia, A.; Sturniolo, A.; Gambaro, G. Low level exposure to cadmium increases the risk of chronic kidney disease: Analysis of the NHANES 1999–2006. BMC Public Health 2010, 10, 304. [Google Scholar] [CrossRef]
- Navas-Acien, A.; Tellez-Plaza, M.; Guallar, E.; Muntner, P.; Silbergeld, E.; Jaar, B.; Weaver, V. Blood cadmium and lead and chronic kidney disease in US adults: A joint analysis. Am. J. Epidemiol. 2009, 170, 1156–1164. [Google Scholar] [CrossRef]
- Li, Y.S.; Ho, W.C.; Caffrey, J.L.; Sonawane, B. Low serum zinc is associated with elevated risk of cadmium nephrotoxicity. Environ. Res. 2014, 134, 33–38. [Google Scholar]
- Satarug, S.; Gobe, G.C.; Ujjin, P.; Vesey, D.A. A comparison of the nephrotoxicity of low doses of cadmium and lead. Toxics 2020, 8, 18. [Google Scholar] [CrossRef]
- Butler-Dawson, J.; James, K.A.; Krisher, L.; Jaramillo, D.; Dally, M.; Neumann, N.; Pilloni, D.; Cruz, A.; Asensio, C.; Johnson, R.J.; et al. Environmental metal exposures and kidney function of Guatemalan sugarcane workers. J. Expo. Sci. Environ. Epidemiol. 2022, 32, 461–471. [Google Scholar] [CrossRef] [PubMed]
- Win-Thu, M.; Myint-Thein, O.; Win-Shwe, T.-T.; Mar, O. Environmental cadmium exposure induces kidney tubular and glomerular dysfunction in the Myanmar adults. J. Toxicol. Sci. 2021, 46, 319–328. [Google Scholar] [CrossRef]
- Tsai, K.F.; Hsu, P.C.; Lee, C.T.; Kung, C.T.; Chang, Y.C.; Fu, L.M.; Ou, Y.C.; Lan, K.C.; Yen, T.H.; Lee, W.C. Association between enzyme-linked immunosorbent assay-measured kidney injury markers and urinary cadmium levels in chronic kidney disease. J. Clin. Med. 2021, 11, 156. [Google Scholar] [CrossRef] [PubMed]
- Myong, J.-P.; Kim, H.-R.; Baker, D.; Choi, B. Blood cadmium and moderate-to-severe glomerular dysfunction in Korean adults: Analysis of KNHANES 2005–2008 data. Int. Arch. Occup. Environ. Health 2012, 85, 885–893. [Google Scholar] [CrossRef] [PubMed]
- Chung, S.; Chung, J.H.; Kim, S.J.; Koh, E.S.; Yoon, H.E.; Park, C.W.; Chang, Y.S.; Shin, S.J. Blood lead and cadmium levels and renal function in Korean adults. Clin. Exp. Nephrol. 2014, 18, 726–734. [Google Scholar] [CrossRef]
- Satarug, S.; Vesey, D.A.; Ruangyuttikarn, W.; Nishijo, M.; Gobe, G.C.; Phelps, K.R. The source and pathophysiologic significance of excreted cadmium. Toxics 2019, 7, 55. [Google Scholar] [CrossRef]
- Satarug, S.; Vesey, D.A.; Gobe, G.C.; Phelps, K.R. Estimation of health risks associated with dietary cadmium exposure. Arch. Toxicol. 2023, 97, 329–358. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Scmid, C.H.; Zhang, Y.; Castro, A.F., III; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Phelps, K.R.; Gosmanova, E.O. A generic method for analysis of plasma concentrations. Clin. Nephrol. 2020, 94, 43–49. [Google Scholar] [CrossRef]
- Satarug, S.; Swaddiwudhipong, W.; Ruangyuttikarn, W.; Nishijo, M.; Ruiz, P. Modeling cadmium exposures in low- and high-exposure areas in Thailand. Environ. Health Perspect. 2013, 121, 531–536. [Google Scholar] [CrossRef]
- Yimthiang, S.; Pouyfung, P.; Khamphaya, T.; Kuraeiad, S.; Wongrith, P.; Vesey, D.A.; Gobe, G.C.; Satarug, S. Effects of environmental exposure to cadmium and lead on the risks of diabetes and kidney dysfunction. Int. J. Environ. Res. Public Health 2022, 19, 2259. [Google Scholar] [CrossRef]
- Zhang, Z.W.; Shimbo, S.; Watanabe, T.; Srianujata, S.; Banjong, O.; Chitchumroonchokchai, C.; Nakatsuka, H.; Matsuda-Inoguchi, N.; Higashikawa, K.; Ikeda, M. Non-occupational lead and cadmium exposure of adult women in Bangkok, Thailand. Sci. Total Environ. 1999, 226, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Zarcinas, B.A.; Pongsakul, P.; McLaughlin, M.J.; Cozens, G. Heavy metals in soils and crops in Southeast Asia. 2. Thailand. Environ. Geochem. Health 2004, 26, 359–371. [Google Scholar] [CrossRef] [PubMed]
- Suwatvitayakorn, P.; Ko, M.S.; Kim, K.W.; Chanpiwat, P. Human health risk assessment of cadmium exposure through rice consumption in cadmium-contaminated areas of the Mae Tao sub-district, Tak, Thailand. Environ. Geochem. Health 2020, 42, 2331–2344. [Google Scholar] [CrossRef] [PubMed]
- Swaddiwudhipong, W.; Nguntra, P.; Kaewnate, Y.; Mahasakpan, P.; Limpatanachote, P.; Aunjai, T.; Jeekeeree, W.; Punta, B.; Funkhiew, T.; Phopueng, I. Human health effects from cadmium exposure: Comparison between persons living in cadmium-contaminated and non-contaminated areas in northwestern Thailand. Southeast Asian J. Trop. Med. Publ. Health 2015, 46, 133–142. [Google Scholar]
- Hornung, R.W.; Reed, L.D. Estimation of average concentration in the presence of nondetectable values. Appl. Occup. Environ. Hyg. 1990, 5, 46–51. [Google Scholar] [CrossRef]
- White, C.A.; Allen, C.M.; Akbari, A.; Collier, C.P.; Holland, D.C.; Day, A.G.; Knoll, G.A. Comparison of the new and traditional CKD-EPI GFR estimation equations with urinary inulin clearance: A study of equation performance. Clin. Chim. Acta 2019, 488, 189–195. [Google Scholar] [CrossRef]
- Grau-Perez, M.; Pichler, G.; Galan-Chilet, I.; Briongos-Figuero, L.S.; Rentero-Garrido, P.; Lopez-Izquierdo, R.; Navas-Acien, A.; Weaver, V.; García-Barrera, T.; Gomez-Ariza, J.L.; et al. Urine cadmium levels and albuminuria in a general population from Spain: A gene-environment interaction analysis. Environ. Int. 2017, 106, 27–36. [Google Scholar] [CrossRef]
- Tsai, H.J.; Hung, C.H.; Wang, C.W.; Tu, H.P.; Li, C.H.; Tsai, C.C.; Lin, W.Y.; Chen, S.C.; Kuo, C.H. Associations among heavy metals and proteinuria and chronic kidney disease. Diagnostics 2021, 11, 282. [Google Scholar] [CrossRef]
- Kalantar-Zadeh, K.; Jafar, T.H.; Nitsch, D.; Neuen, B.L.; Perkovic, V. Chronic kidney disease. Lancet 2021, 398, 786–802. [Google Scholar] [CrossRef]
- Jin, T.; Frankel, B.J. Cadmium-metallothionein nephrotoxicity is increased in genetically diabetic as compared with normal Chinese hamsters. Pharmacol. Toxicol. 1996, 79, 105–108. [Google Scholar] [CrossRef]
- Jin, T.; Nordberg, G.F.; Sehlin, J.; Leffler, P.; Wu, J. The susceptibility of spontaneously diabetic mice to cadmium-metallothionein nephrotoxicity. Toxicol. 1994, 89, 81–90. [Google Scholar] [CrossRef]
- Riaz, M.A.; Nisa, Z.U.; Mehmood, A.; Anjum, M.S.; Shahzad, K. Metal-induced nephrotoxicity to diabetic and non-diabetic Wistar rats. Environ. Sci. Pollut. Res. Int. 2019, 26, 31111–31118. [Google Scholar] [CrossRef]
- Riaz, M.A.; Nisa, Z.U.; Anjum, M.S.; Butt, H.; Mehmood, A.; Riaz, A.; Akhtar, A.B.T. Assessment of metals induced histopathological and gene expression changes in different organs of non-diabetic and diabetic rats. Sci. Rep. 2020, 10, 5897. [Google Scholar] [CrossRef]
- Shi, Z.; Taylor, A.W.; Riley, M.; Byles, J.; Liu, J.; Noakes, M. Association between dietary patterns, cadmium intake and chronic kidney disease among adults. Clin. Nutr. 2018, 37, 276–284. [Google Scholar] [CrossRef] [PubMed]
- Kelly, J.T.; Su, G.; Zhang, L.; Qin, X.; Marshall, S.; González-Ortiz, A.; Clase, C.M.; Campbell, K.L.; Xu, H.; Carrero, J.J. Modifiable lifestyle factors for primary prevention of CKD: A systematic review and meta-analysis. J. Am. Soc. Nephrol. 2021, 32, 239–253. [Google Scholar] [CrossRef] [PubMed]
- Jin, A.; Koh, W.P.; Chow, K.Y.; Yuan, J.M.; Jafar, T.H. Smoking and risk of kidney failure in the Singapore Chinese health study. PLoS ONE 2013, 8, e62962. [Google Scholar] [CrossRef]
- Pappas, R.S.; Fresquez, M.R.; Watson, C.H. Cigarette smoke cadmium breakthrough from traditional filters: Implications for exposure. J. Anal. Toxicol. 2015, 39, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Hagedoorn, I.J.M.; Gant, C.M.; Huizen, S.V.; Maatman, R.G.H.J.; Navis, G.; Bakker, S.J.L.; Laverman, G.D. Lifestyle-related exposure to cadmium and lead is associated with diabetic kidney disease. J. Clin. Med. 2020, 9, 2432. [Google Scholar] [CrossRef]
- Oosterwijk, M.M.; Hagedoorn, I.J.M.; Maatman, R.G.H.J.; Bakker, S.J.L.; Navis, G.; Laverman, G.D. Cadmium, active smoking and renal function deterioration in patients with type 2 diabetes. Nephrol. Dial. Transplant 2023, 38, 876–883. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | All Participants, n = 674 | Diabetics, n = 81 | Non-Diabetics, n = 593 | p |
|---|---|---|---|---|
| Low-exposure locality (%) | 67.1 | 86.4 | 64.4 | <0.001 |
| Female, % | 57.6 | 74.1 | 55.3 | <0.001 |
| Smoking, % | 31.9 | 14.8 | 34.2 | <0.001 |
| Hypertension c % | 25.8 | 55.6 | 21.8 | <0.001 |
| Age, years | 47.1 ± 16.3 | 58.5 ± 9.7 | 45.6 ± 16.4 | <0.001 |
| BMI, kg/m2 | 22.8 ± 4.2 | 26.0 ± 4.8 | 22.3 ± 3.9 | <0.001 |
| Obese a (%) | 3.9 | 2.4 | <0.001 | |
| eGFR b, mL/min/1.73 m2 | 87.4 ± 23.1 | 76.2 ± 21.0 | 89.0 ± 23.0 | <0.001 |
| Reduced eGFR c (%) | 11.4 | 22.2 | 9.9 | <0.001 |
| Plasma creatinine, mg/dL | 0.94 ± 0.28 | 0.96 ± 0.36 | 0.93 ± 0.27 | 0.911 |
| Urine creatinine, mg/dL | 98.8 ± 68.4 | 90.1 ± 58.2 | 99.9 ± 69.7 | 0.453 |
| Plasma-to-urine creatinine ratio | 0.016 ± 0.015 | 0.016 ± 0.012 | 0.016 ± 0.015 | 0.391 |
| Urine Cd, µg/L | 4.59 ± 11.92 | 2.75 ± 6.94 | 4.84 ± 12.44 | 0.003 |
| Urine β2M, µg/L | 2327 ± 11,517 | 4105 ± 21,667 | 2010 ± 8532 | <0.001 |
| Normalized to Ccr (Ex/Ccr) d | ||||
| (ECd/Ccr) × 100, µg/L filtrate | 4.48 ± 10.38 | 3.32 ± 8.40 | 4.64 ± 10.62 | <0.001 |
| (Eβ2M/Ccr) × 100, µg/L filtrate | 3858 ± 20,142 | 6694 ± 33,617 | 3352 ± 16,642 | <0.001 |
| (Eβ2M/Ccr) × 100, µg/L filtrate (%) | ||||
| ≥300 | 36.3 | 75.3 | 29.3 | <0.001 |
| ≥1000 | 20.4 | 49.4 | 14.8 | <0.001 |
| Normalized to Ecr (Ex/Ecr) e | ||||
| ECd/Ecr, µg/g creatinine | 4.12 ± 7.80 | 2.75 ± 5.52 | 4.30 ± 8.04 | <0.001 |
| Eβ2M/Ecr, µg/g creatinine | 2540 ± 11,420 | 4004 ± 13,978 | 2279 ± 10,899 | <0.001 |
| Eβ2M/Ecr, µg/g creatinine (%) | ||||
| ≥300 | 37.6 | 79.0 | 30.2 | <0.001 |
| ≥1000 | 21.3 | 53.1 | 15.6 | <0.001 |
| Parameters | Number of Participants | Tubular Dysfunction a | Reduced eGFR b | ||
|---|---|---|---|---|---|
| POR (95% CI) | p | POR (95% CI) | p | ||
| Age, year | 535 (674) | 1.100 (1.076, 1.126) | <0.001 | 1.146 (1.107, 1.188) | <0.001 |
| BMI, kg/m2 | 535 (674) | 0.963 (0.908, 1.021) | 0.202 | 1.070 (0.993, 1.153) | 0.075 |
| Log2[(ECd/Ccr) × 105] | 535 (674) | 1.149 (1.054, 1.253) | 0.002 | 1.500 (1.304, 1.724) | <0.001 |
| Hypertension | 162 (174) | 0.724 (0.444, 1.181) | 0.195 | 0.744 (0.387, 1.428) | 0.374 |
| Smoking | 195 (215) | 1.563 (0.863, 2.830) | 0.140 | 1.124 (0.511, 2.474) | 0.771 |
| Gender (male) | 223 (286) | 0.819 (0.480, 1.398) | 0.464 | 1.284 (0.615, 2.680) | 0.506 |
| Diabetes | 81 (81) | 8.690 (4.421, 17.08) | <0.001 | 2.973 (1.274, 6.937) | 0.012 |
| Independent Variables/Factors | Excretion Rate of β2M a | |||||
|---|---|---|---|---|---|---|
| All Diabetics, n = 81 | Diabetics, n = 70 | Non-Diabetics, n = 454 | ||||
| β b | p | β | p | β | p | |
| Age, years | 0.202 | 0.072 | 0.159 | 0.159 | 0.458 | <0.001 |
| Log2[(ECd/Ccr) × 105], µg/L filtrate | 0.181 | 0.113 | 0.375 | 0.001 | 0.269 | <0.001 |
| Smoking | 0.206 | 0.155 | 0.253 | 0.055 | 0.036 | 0.443 |
| Obesity | 0.145 | 0.194 | 0.273 | 0.015 | −0.049 | 0.193 |
| Gender | −0.136 | 0.328 | −0.209 | 0.122 | 0.025 | 0.572 |
| Hypertension | 0.105 | 0.346 | −0.032 | 0.767 | 0.024 | 0.532 |
| Adjusted R2 | 0.089 | 0.043 | 0.244 | 0.001 | 0.386 | <0.001 |
| Independent Variables/Factors | eGFR a, mL/min/1.73m2 | |||||
|---|---|---|---|---|---|---|
| All Diabetics, n = 81 | Diabetics, n = 70 | Non-Diabetics, n = 593 | ||||
| β b | p | β | p | β | p | |
| Age, year | −0.444 | <0.001 | −0.472 | <0.001 | −0.574 | <0.001 |
| Log2[(ECd/Ccr) × 105], µg/L filtrate | −0.244 | 0.014 | −0.145 | 0.167 | −0.263 | <0.001 |
| Smoking | −0.208 | 0.095 | −0.175 | 0.167 | 0.033 | 0.352 |
| Obesity | −0.151 | 0.116 | −0.146 | 0.170 | 0.037 | 0.190 |
| Gender | 0.163 | 0.173 | 0.162 | 0.214 | −0.024 | 0.448 |
| Hypertension | −0.045 | 0.634 | −0.066 | 0.530 | −0.014 | 0.633 |
| Adjusted R2 | 0.330 | <0.001 | 0.293 | <0.001 | 0.534 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Satarug, S.; Yimthiang, S.; Pouyfung, P.; Khamphaya, T.; Vesey, D.A. Cadmium-Induced Tubular Dysfunction in Type 2 Diabetes: A Population-Based Cross-Sectional Study. Toxics 2023, 11, 390. https://doi.org/10.3390/toxics11040390
Satarug S, Yimthiang S, Pouyfung P, Khamphaya T, Vesey DA. Cadmium-Induced Tubular Dysfunction in Type 2 Diabetes: A Population-Based Cross-Sectional Study. Toxics. 2023; 11(4):390. https://doi.org/10.3390/toxics11040390
Chicago/Turabian StyleSatarug, Soisungwan, Supabhorn Yimthiang, Phisit Pouyfung, Tanaporn Khamphaya, and David A. Vesey. 2023. "Cadmium-Induced Tubular Dysfunction in Type 2 Diabetes: A Population-Based Cross-Sectional Study" Toxics 11, no. 4: 390. https://doi.org/10.3390/toxics11040390