1. Introduction
Preterm birth (PTB), defined as delivery prior to 37 weeks’ gestation, is a common complication in pregnancy and a leading cause of neonatal morbidity [
1]. Risk factors for spontaneous PTB include prior PTB, smoking, Black race, extremes of maternal age, genital tract infections, and low socioeconomic status [
2]. The majority of preterm deliveries in the United States (US) occur in the late preterm period, defined as delivery greater than 34 weeks’ but less than 37 weeks’ gestation, with a rate of 7.1% in 2016 [
3,
4]. Infants of late preterm birth (LPTB) have increased morbidity compared to term infants given their developmental immaturity [
5], but little is known about specific risk factors for LPTB [
6,
7]. Environmental factors, such as psychosocial stressors and chemical exposures, are associated with increased risk of PTB but have not been explored in specific relation to LPTB [
1,
8].
Phthalates are a class of chemicals found in 99–100% of pregnant women tested within the US National Health Nutrition and Examination Survey (NHANES) [
9]. They are ubiquitous chemicals found in commonly used plastics and are contaminants in food production. Phthalates are also used as color stabilizers and fragrance in personal care products [
10]. These chemicals are known to be endocrine disruptors and increase oxidative stress and inflammation [
11]. Exposure has been associated with multiple adverse outcomes in adults and children such as increased reproductive toxicity in males, decreased thyroid function, and changes in pubertal development [
12]. In a study including Black women in South Carolina, even after adjusting for socioeconomic status, they were found to have higher exposure to phthalates than other women. This may be due to higher concentrations of phthalates found in certain personal care products and other phthalate exposures [
13,
14].
Mechanistic pathways of preterm labor include pro-inflammatory cytokine release that leads to inflammation, increase in prostaglandins, or progesterone withdrawal [
15]. Phthalates may play a role in initiating pro-inflammatory cytokines [
16], activation of prostaglandin synthesis through peroxisome proliferator-activated receptors (PPAR) [
17] and decreasing progesterone. This cascade theoretically could lead to preterm labor and delivery; however, the conclusions from prior studies evaluating prenatal phthalate exposure and preterm delivery are mixed [
1,
18,
19,
20,
21,
22,
23,
24]. Some studies have suggested an association with increasing maternal urinary phthalate concentrations and increased risk of preterm birth or oxidative stress [
1,
18,
19,
25], while other studies noted no association based on exposure assessed as maternal urinary phthalates [
24], self-reported phthalate exposure [
22] or amniotic fluid phthalate levels [
23].
Maternal stress during pregnancy has also been associated with an increased risk of PTB [
26,
27,
28]. Exposure to intimate partner violence, specifically, was associated with PTB in two systematic reviews [
29,
30]. Although the pathophysiology by which stress can increase risk is not completely defined, several pathways have been suggested such as increased TNF-
and IL-6 [
26], increased oxidative stress [
31,
32], or increased corticotropin releasing hormone [
33]. It is well known that maternal stress alters the hypothalamic-pituitary-adrenal axis, thus augmenting the risk of PTB [
26,
27,
28]. Given greater stress and disparities in patients with lower socioeconomic status (SES) and non-white race, the physiological response to stress may be contributing to disparities in poor birth outcomes in the US [
8].
The primary objective of this study is to evaluate the association between prenatal phthalate exposure and risk of LPTB as well as continuous gestational age at delivery. We evaluated if the association was modified by maternal race, as we hypothesized that given the higher burden of stressors Black women face, this may sensitize them to the adverse effects of phthalate exposures. We further explore whether associations are modified by prenatal stress, given the similar proposed mechanisms by which phthalates and stress may increase risk of PTB. We also perform a secondary analysis on women with spontaneous labor without medical indication for delivery to investigate the relationship of phthalate exposure on women with non-medically indicated births. We hypothesize that higher levels of phthalate concentration will be associated with greater risk for LPTB and that these associations will be stronger for Black women or for those exposed to IPV in pregnancy.
3. Results
The mean age of the 1408 women included in the current analysis was 26.5 years (SD: 5.4), and 61.0% self-identified as Black (
Table 1).
At enrollment, 38.9% of the women had a household income less than
$25,000, and 58.2% of them had a high school degree or less. Many of them (58.7%) were multiparous and the majority (92.1%) had no history of PTB. Two thirds of the women (66.7%) reported experiencing at least one type of abuse or injury by their partner over the past 12 months, with 48.8% of the overall population reporting one type of IPV and 1.8% reporting four unique types of IPV. We did not observe meaningful differences in baseline characteristics comparing the primary analytic sample and the sample with complete data (
Table A1).
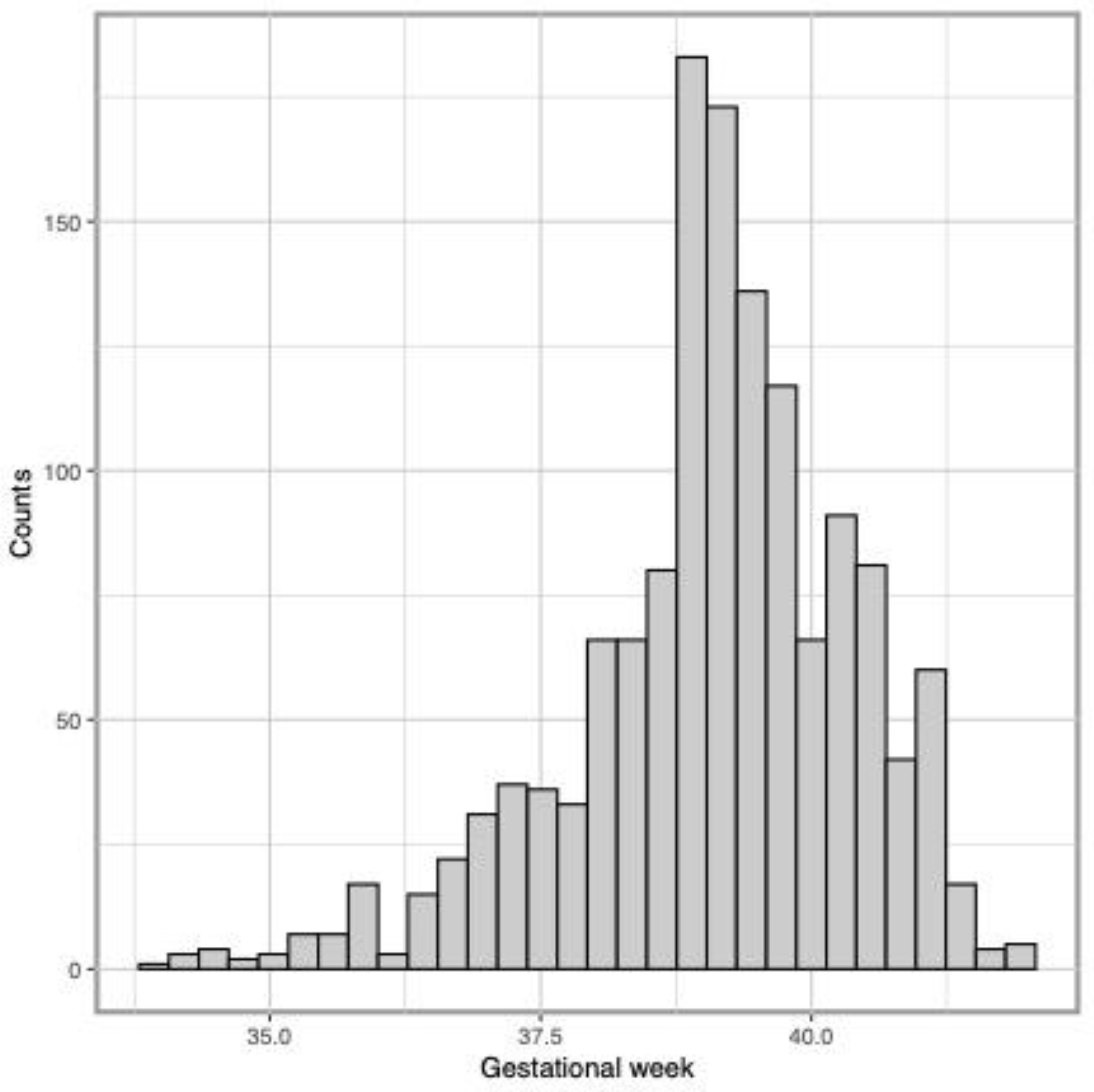
The distribution of gestational week was slightly left-skewed with a mean of 39.1 (SD: 1.3) weeks (
Figure 1), and the LPTB rate was 6.7%.
Phthalate metabolites included in the analysis were detected in 71.3–100% of samples (
Table 2).
The Spearman correlations between phthalates in both visits ranged from 0.12 to 0.58. Majority (
N = 13) of the 14 individual phthalates were higher in the second trimester than the third. MEP was found in highest concentration (geometric mean 133.2 ng/mL and 125.8 ng/mL in the second and third trimesters, respectively), whereas MHPP was the lowest (geometric mean 1.2 ng/mL and 0.4 ng/mL in the second and third trimesters, respectively). Phthalates were in similar concentrations to values found in the National Health and Nutrition Examination Survey (NHANES) 2009–2010 study [
43], except for MEP which was found in higher concentration in our study samples. On average, Black women had higher concentrations of MEHP, MEP, MBzP, MBP and MiBP, while other metabolites were similar between Black and non-Black women (
Table A2).
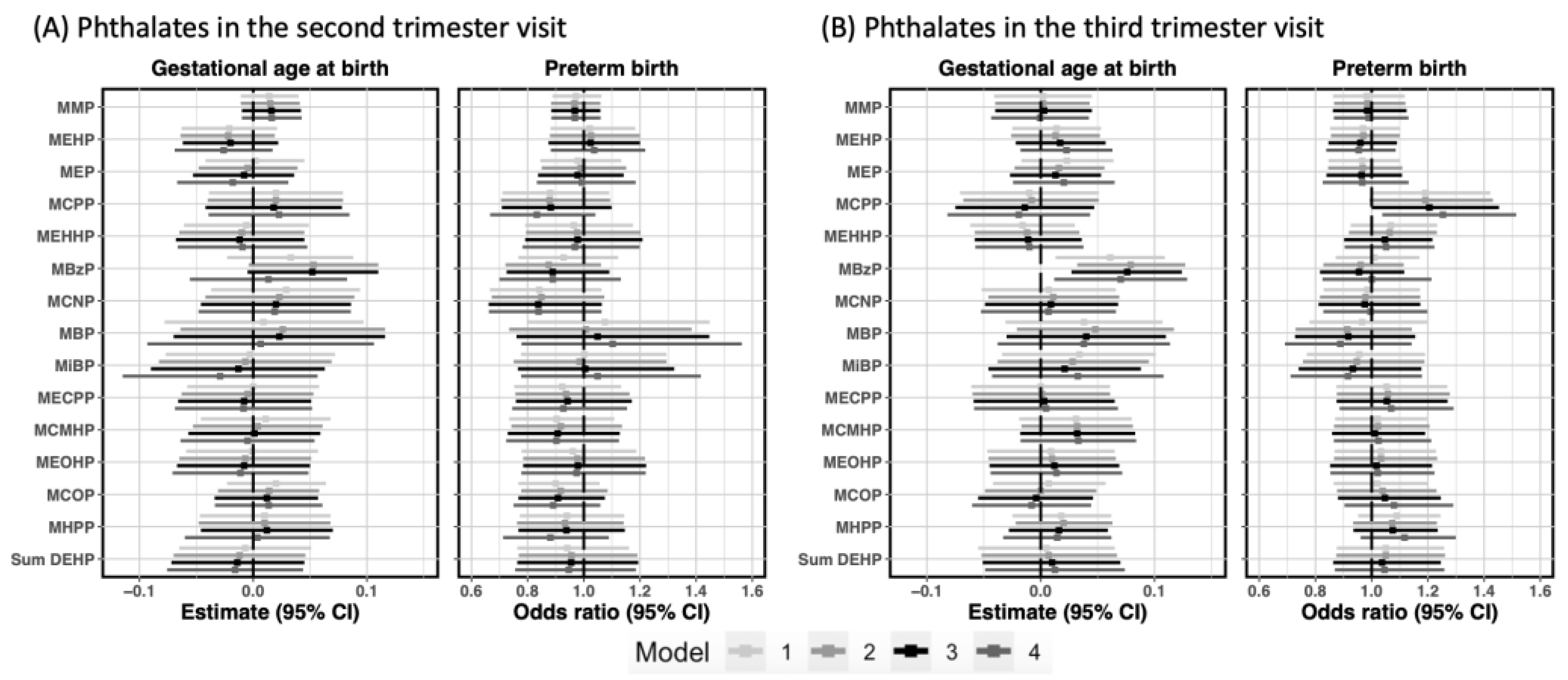
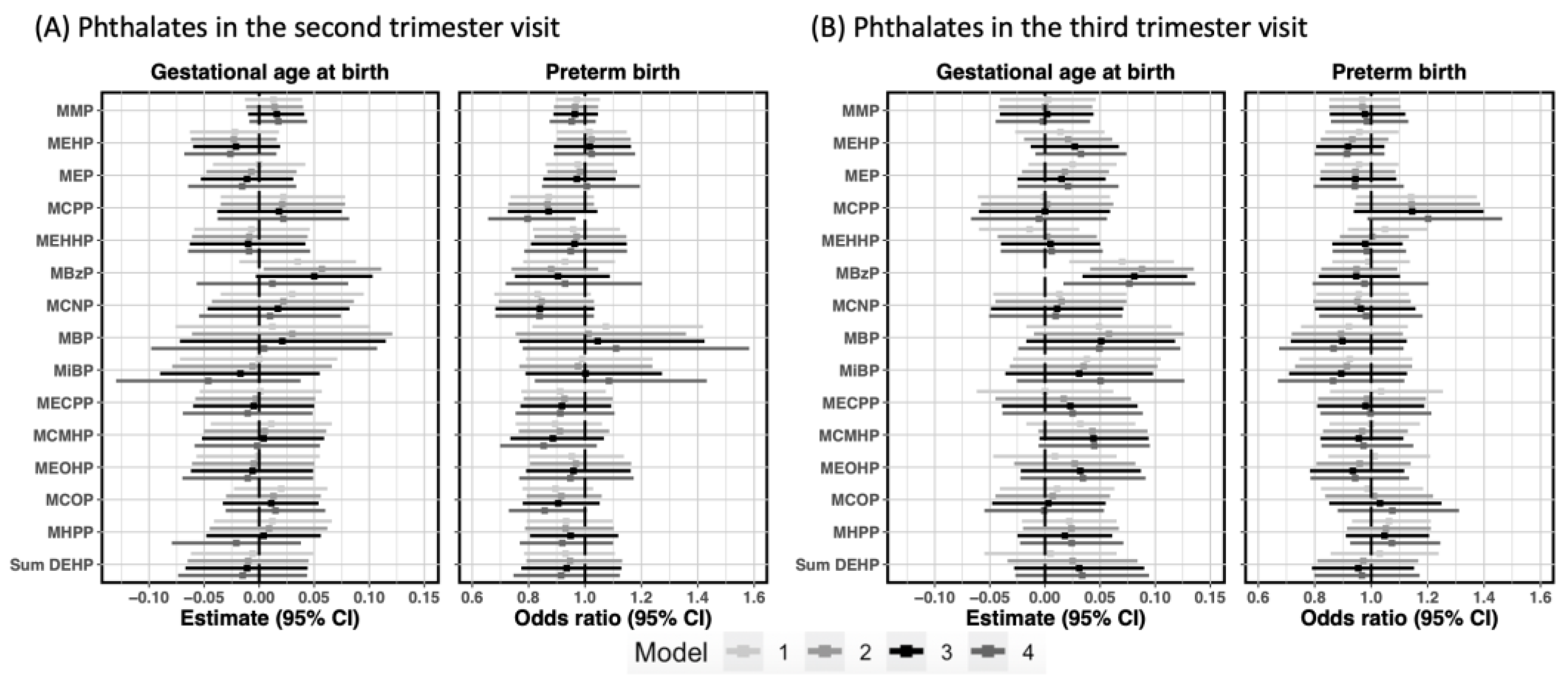
We did not observe significant inverse relationships between individual phthalates in each visit and gestational age at birth (
Figure 2).
For each 2-fold increase in the second trimester MBzP concentrations, we observed a positive association of 0.05 more gestational weeks (
: 0.05, 95% CI: −0.01, 0.11) while each 2-fold increase in the third trimester was associated with 0.08 more gestational weeks (
: 0.08, 95% CI: 0.03, 0.12). In the model with mutual adjustment for both trimesters, the association remained only for the third trimester (
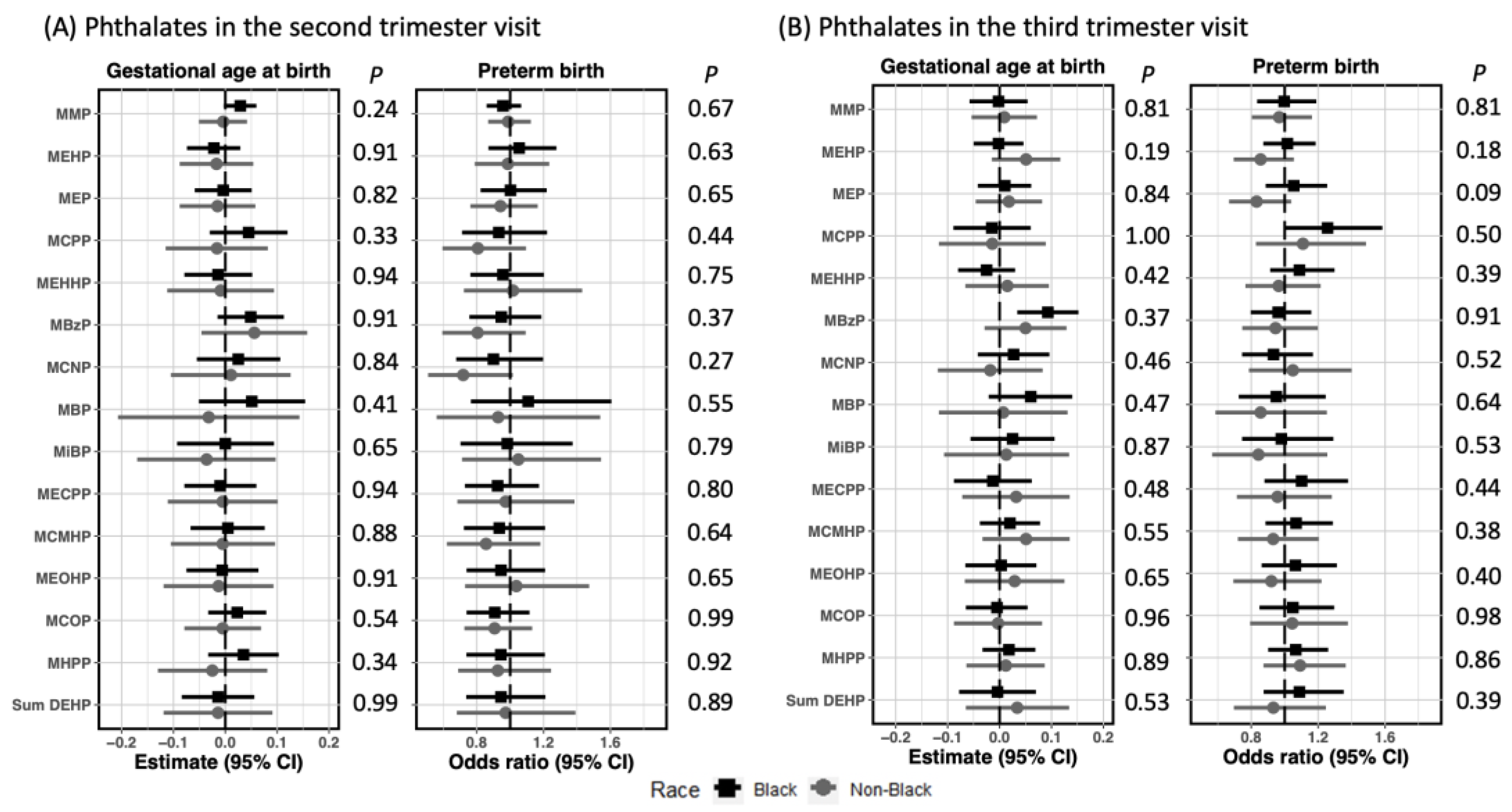
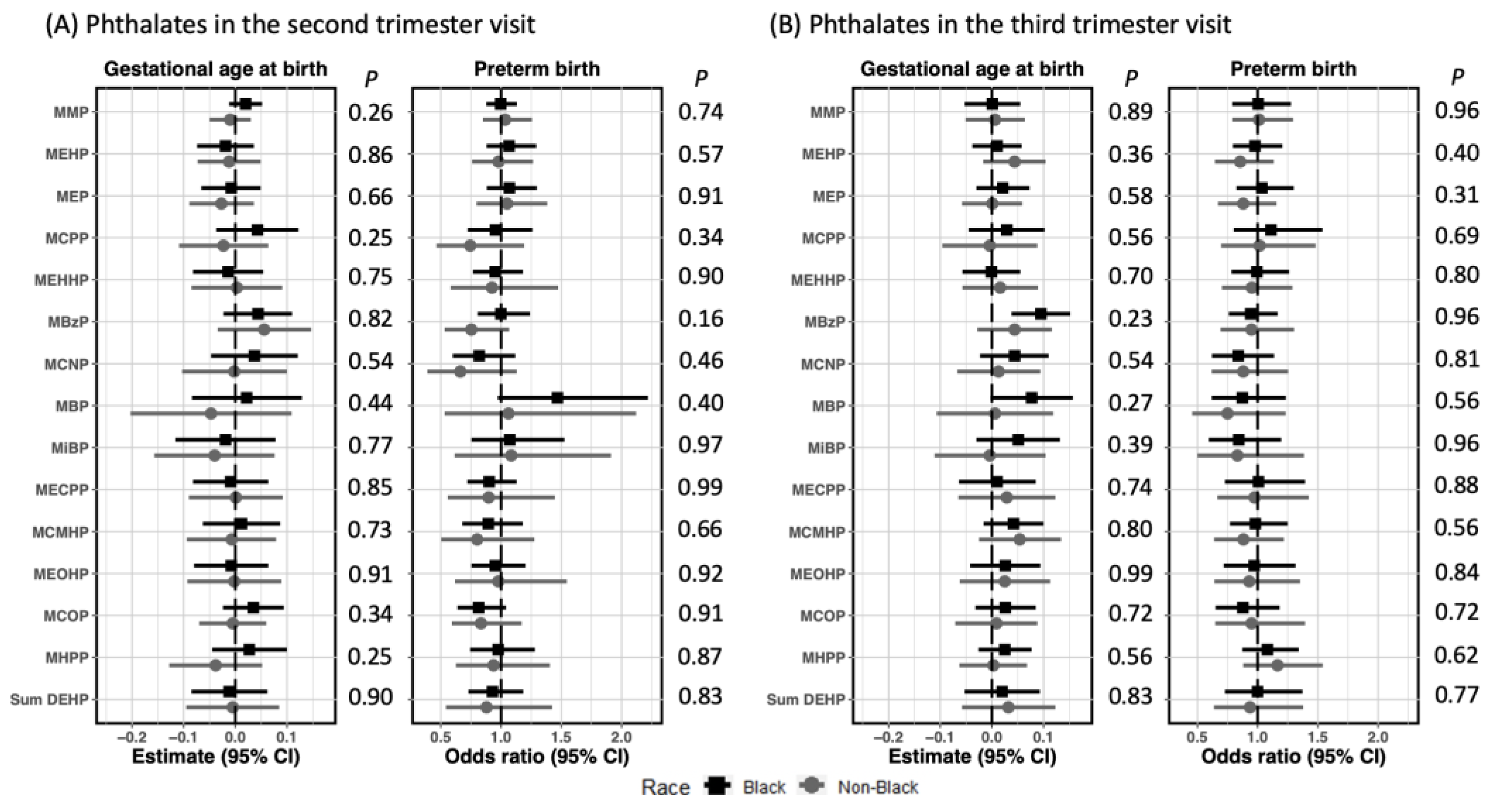
: 0.07, 95% CI: 0.01, 0.13). When LPTB was analyzed as a dichotomous outcome, we observed increased odds of LPTB (OR: 1.21, 95% CI: 1.00, 1.45) in relation to MCPP in the third trimester, which was strengthened when adjusting for MCPP in the second trimester (OR: 1.25, 95% CI: 1.04, 1.51). Nevertheless, in the mutually adjusted model, the association between second trimester MCPP and LPTB reversed to negative. Evaluation of associations between phthalates in each visit and birth outcomes were not modified by maternal race (
Figure A1). No modification by IPV for the associations of interest was found (
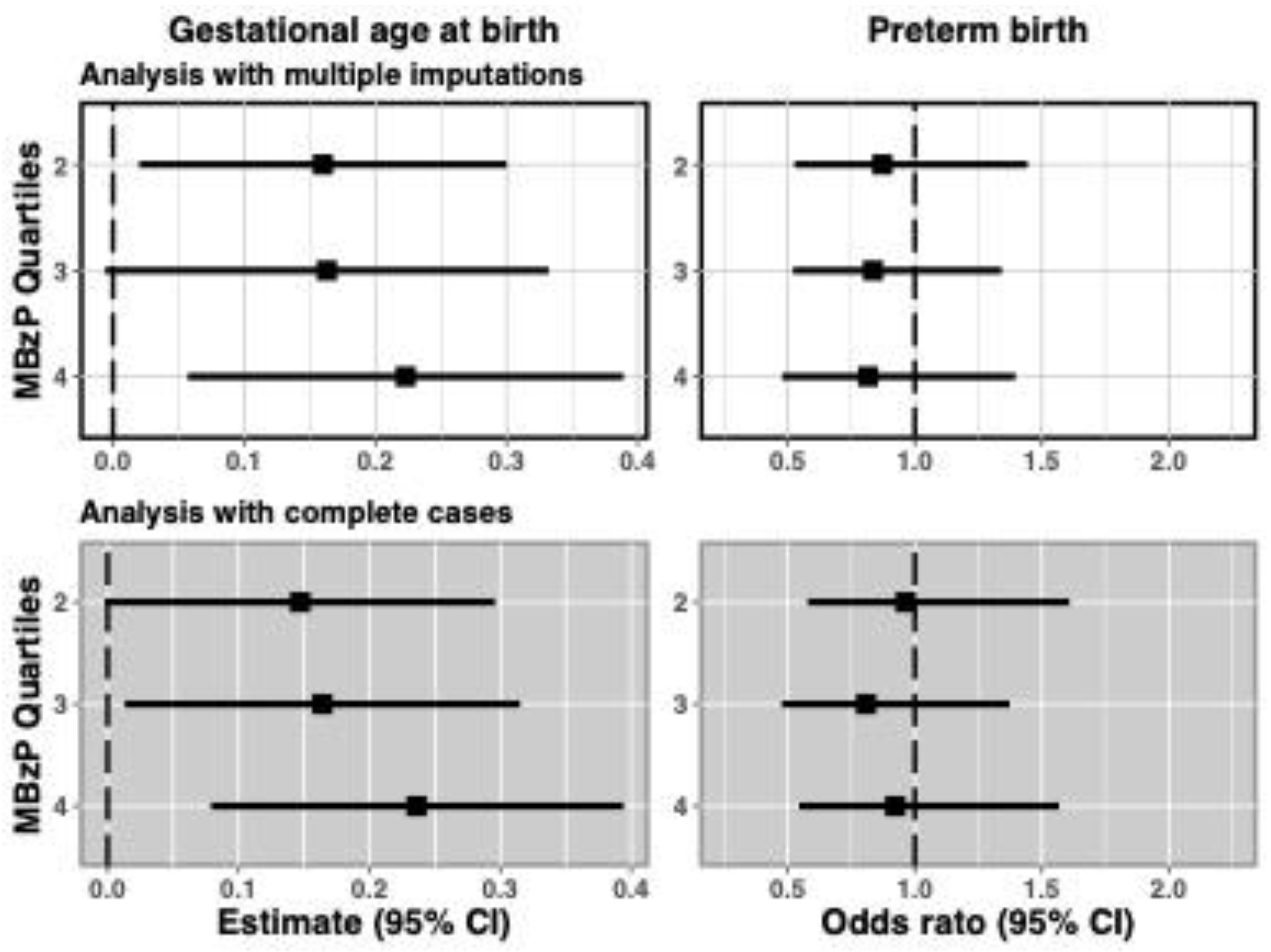
Table A3). When the analyses of individual phthalates and GA/LPTB were repeated using complete data, findings agreed with those obtained using multiple imputation (
Figure A2). When MBzP in the third trimester was divided into quartiles, we found longer gestation in women with MBzP in the 2nd to 4th quartiles compared to women with MBzP in the 1st quartile (
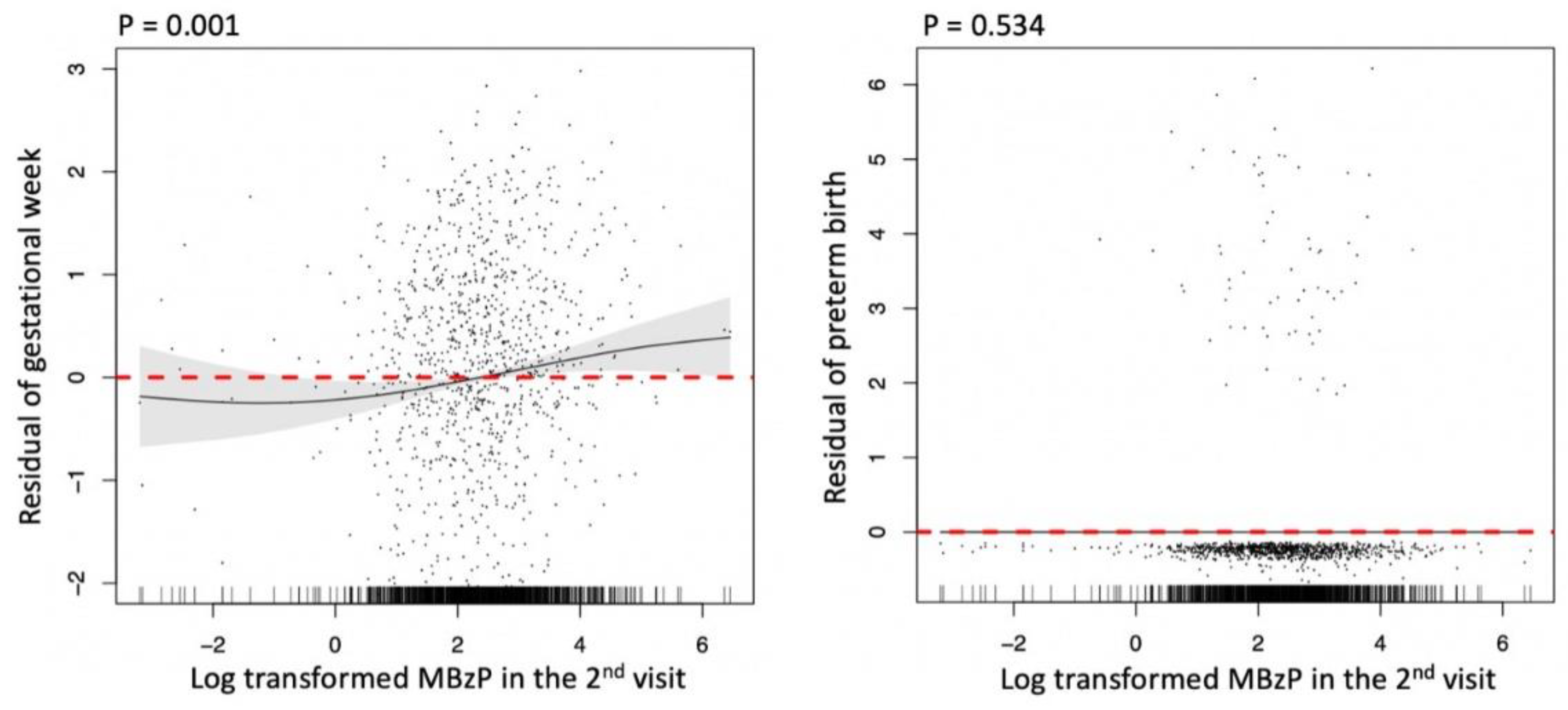
Figure A3). The smooth effect curves generated from GAMs based on complete data (
Figure A4) was consistent with a linear trend for the association between MBzP in the third trimester and gestational week (
p: 0.001).
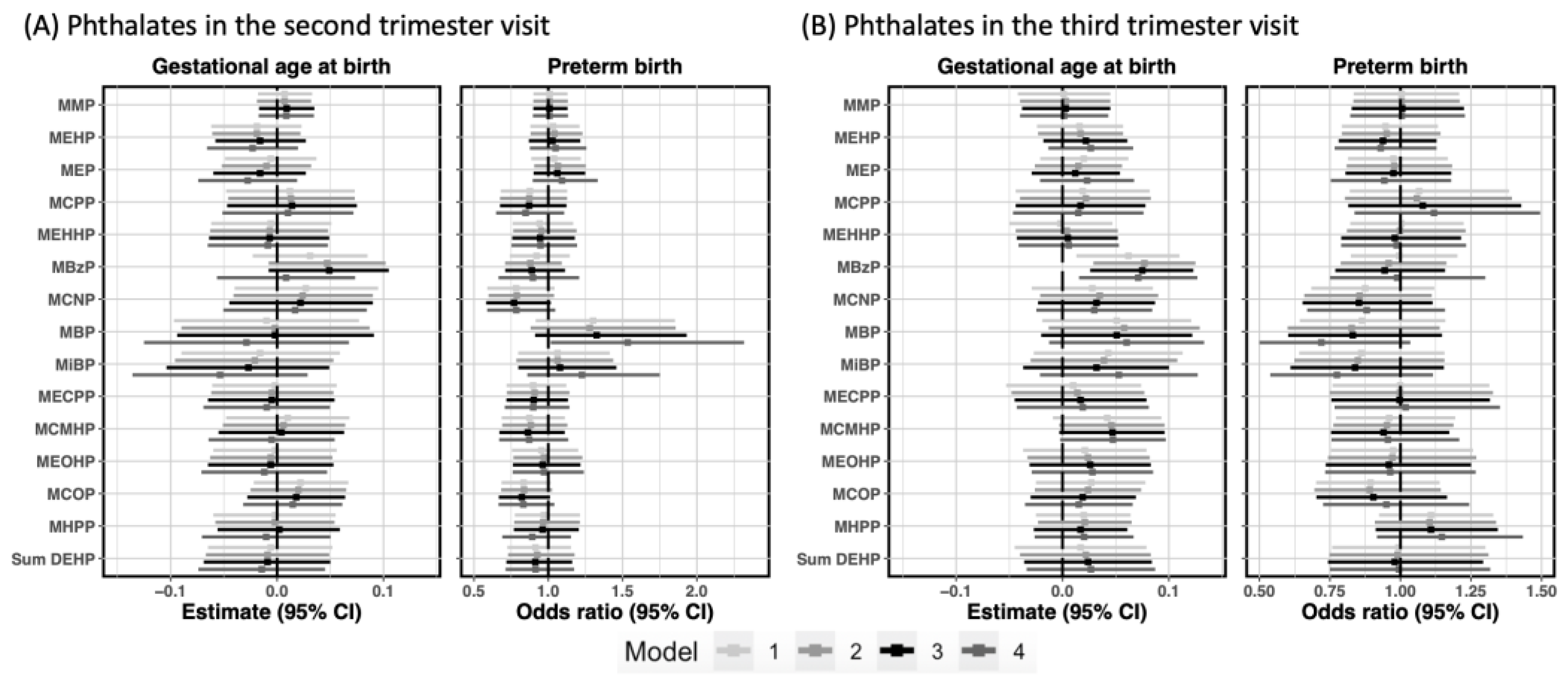
When restricting the study population to those with a spontaneous labor, we observed similar associations with MBzP as those in the primary analysis. An association between MBzP in the third trimester and longer gestation was detected in the overall sample (
: 0.08, 95% CI: 0.03, 0.12) (
Figure 3).
One unique finding in this restricted population was an increased odds of LPTB (OR: 1.54, 95% CI: 1.02, 2.32) per two-fold increase in second trimester MBP, after third trimester MBP was controlled. No other associations were observed. As in the primary analysis, we did not observe evidence of modification by IPV or maternal race (
Table A4).
4. Discussion
In a large diverse study population that is underrepresented in the literature, we observed mixed results in the association between prenatal phthalate exposure and gestational age at time of delivery but some similar results to a recently published 16 study pooled analysis examining prenatal phthalate exposure and preterm births [
25] in which higher prenatal MCPP and MBP exposure was significantly associated with an increased risk of preterm birth. We observed no adverse relationships between phthalate exposure and continuous GA at delivery in the combined spontaneous and medically indicated births cohort after robust control for covariates. We observed a small positive relationship between third trimester MBzP and gestational age at delivery (0.08 more gestational weeks for every 2 fold increase in MBzP). There is also an association between third trimester MCPP and increased risk of LPTB (OR: 1.21, 95% CI: 1.00, 1.45), which was strengthened when adjusting for the second trimester MCPP concentration. In restricting to spontaneous labor, exposure to MBP increased odds of spontaneous LPTB by 54% for every 2-fold increase of MBP. There was no evidence that associations varied by maternal race or IPV.
The primary findings of our study only partially agree from four previous studies that suggest that prenatal phthalate exposure is linked to a reduction in gestational age and increased risk of preterm birth [
1,
18,
19,
25,
44]. Our analysis of spontaneous LPTB does agree with the associated increased risk of PTB with exposure to MBP in two unique cohort studies and the recent 16 cohort pooled analysis [
1,
18,
25,
44]. Additionally, we observed an association of MCPP (while adjusting for second trimester exposure) with increased rates of LPTB. This has been noted previously in a restricted sample of spontaneous preterm birth patients and now the pooled study [
1,
25]. Reasons for discrepancies in other findings may be related to associations with LPTB vs. overall preterm birth and our larger sample size and robust control for covariates not normally available in most epidemiologic analyses. In addition, the study population is more diverse in educational status, income, race and martial status than most of those included in previous reports. In two studies [
1,
18], Ferguson et al. found MEHP, MECPP, and ∑DEHP metabolites were associated with increased odds of preterm birth and MBzP, MBP, MiBP with increased markers of oxidative stress When particularly evaluating the women with spontaneous PTB (
N = 57), Ferguson noted the association with MBP and decreased gestational age [
1]. This study cohort was smaller (
N = 482) and comprised of mostly White and privately insured patients. A pooled study of 16 prospective cohorts, totaling 6000 pregnant patients, found that MBP, MiBP, MECPP, MCPP were associated with increased odds of PTB (12–16%) [
25]. This is the largest cohort study to date, but the authors were unable to separate between spontaneous and indicated preterm birth. Additionally, this cohort was not restricted to LPTB. In a study conducted in Mexico City (
N = 60), Meeker et al. [
19] observed that MBP, MBzP and 5 metabolites of DEHP increased risk of preterm delivery. This cohort was predominantly LatinX included both spontaneous and medically indicated preterm birth, and urine samples were taken at a later gestational age. A cohort in Puerto Rico, DBP and DiBP metabolites were associated with increased spontaneous preterm birth. This included MBP, which was associated with 1.55 days shorter gestation [
44]. Our study suggested an adverse risk of MBP only in women with spontaneous LPTB and did not find this association in the overall cohort.
Others have reported no associations between maternal phthalate exposures and preterm birth [
22,
23,
24]. In a low income and underrepresented minority population in Rotterdam, The Netherlands (
N = 6302), Burdorf [
22] did not find significant associations however exposure was determined based on self-reported occupational exposures, which are less accurate than biomarker analyses. Huang et al. [
23] found no correlation between amniotic fluid phthalate levels and preterm birth in a study of 65 women in Taiwan. Lastly, in a design using maternal urinary phthalates for exposure characterization as done in our study, Suzuki et al. [
24] analyzed maternal urinary phthalates and preterm birth in Japan in a cohort of 149 women, and also observed no associations. Notably, this study had a small sample size and low preterm birth rate in the population (1.5%).
In the current literature, only one study [
45] examined the joint impact of phthalates and maternal stress on preterm birth, finding that increased maternal stress modified the association with PTB by increasing effect estimates. No studies have examined stress-phthalate interactions in the prediction of LPTB. Contrary to our hypothesis, we did not observe evidence of modification by maternal stress in this study population. We also explored effect modification by maternal race. Although small differences by maternal race were observed in the relationships between phthalates and preterm birth outcomes, effect modification was not evident. While not statistically significant, the minor differences observed may be due to social factors such as racism and other socioeconomic stressors that could affect susceptibility. This analysis was not designed to be able to further disentangle these complex relationships.
Our results in the CANDLE population were largely null for the combined spontaneous and medically indicated preterm birth subsample, but findings of MBP related to higher odds of preterm birth in spontaneous births only were consistent with four other cohort studies [
1,
18,
19,
44]. We observed a statistically significant but modest increase in gestational length associated with third trimester MBzP in both the full cohort and women with spontaneous LPTB. When considering the unexpected finding with MBzP, we identified some literature demonstrating MBzP can activate PPAR-gamma [
17], which is a receptor that has anti-inflammatory properties in the preterm birth cascade pathway [
46]. Further study is needed on the affinity of activation by MBzP and the impact of PPAR-gamma on altering the LTPB pathway. Two previous studies [
20,
21] have also noted a positive relationships between prenatal phthalate exposure and gestational age at time of delivery such as this study noted with MBzP. Adibi et al. [
20] noted that 75th percentile of
had a prolongation association of 2 days gestation in their study compared to the 25th percentile. Given that DEHP is the aggregate measure of several metabolites, this study could not identify which of the three studied metabolites was driving this association. Wolff et al. [
21] found a protective association of all low molecular weight metabolites on gestational age at delivery. Of note, the study population was over 50% of women being Hispanic ethnicity.
Exposure to phthalates is ubiquitous in our daily environment [
24]. The risk of spontaneous LPTB is increased with exposure to MBP. Higher levels of MBP have been detected in pregnant women that used eye makeup, sunscreen, nail polish and hair nutrient products [
47]. By limiting use of these products in pregnancy, women may decrease their exposure to MBP and risk of spontaneous LPTB. Exposure to maternal stress through IPV in pregnancy does not appear to impact the relationship between phthalates and LPTB in this population.
Previous studies have shown that modification and reduction of exposure to all endocrine disruptors may be beneficial in pregnancy [
10,
25,
48]. Using G computation in the pooled analysis, hypothetical reductions in phthalate levels were associated with decreased rates of PTB that were dose-dependent [
25]. The best evidence of link to preterm birth is with more thoroughly studied endocrine disrupting chemicals such as lead [
49,
50]. and mercury [
51]. Although this study showed mixed results of the association of phthalates on LPTB, overall reduction in phthalate exposure can help decrease other more well established adverse maternal and neonatal health outcomes [
52,
53,
54,
55].
This study highlights the importance of expanding the literature to include more ethnically diverse, well characterized and prospective cohort studies. Our cohort, with a large prevalence of risk factors for PTB, such as non-White race and low SES, highlights that there may be other factors that contribute much more to the attributable risk of LTPB in such a diverse patient population. Finally, to address the possibility of critical windows of phthalate exposure increasing the risk of LPTB, our study incorporated multiple measures of urinary phthalates across pregnancy, allowing examination of variation in exposure and excretion that may occur across pregnancy. If a critical window for phthalate exposure exists, future studies could then evaluate risk of LPTB as well as early term birth, a time period which also causes increased neonatal morbidity.
This is the most diverse prospective cohort study in the current literature on phthalate exposure and preterm delivery. The CANDLE cohort includes a large proportion of Black women in the urban Southeastern US, an underrepresented population in the literature. We were able to collect urine samples from two time points to assess the congregate risk of phthalate exposure over pregnancy. Another strength is that we adjusted for a comprehensive set of control variables, including many risk factors for preterm delivery, reducing the likelihood that observed associations were impacted by residual confounding. We were additionally able to perform a secondary analysis on women with spontaneous labor, as this may have different mechanistic implications to phthalate exposure.
Limitations of this study include there was minimal maternal medical comorbidity data collected for these pregnancies, which may impact the pathophysiology of labor. Given CANDLE enrollment of low-risk pregnancies, fewer women delivered preterm. This reduced variability in the outcome may have reduced our chances of detecting a true association. Because phthalates were measured only for mother-child dyads who attended clinic visits in early childhood, exposure was missing for several women. We addressed this using multiple imputation and compared all findings to those obtained using complete case analysis; in all cases we obtained similar results. Finally, it is possible that phthalate exposure does increase risk of LPTB, but our study failed to detect this association. Exposure to phthalates may need to occur at a critical time window in pregnancy to increase risk for LPTB. Given that urinary phthalate assessment occurred only twice per pregnancy at a non-standardized gestational age, we may have been unable to detect this exposure window. Alternatively, a spot urine may not represent integrated exposures during pregnancy, which may increase risk of LPTB.

 ,
, 





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}


