
Prevalence of Essential Nutrient Supplement Use and Assessment of the Knowledge and Attitudes of Lebanese Mothers towards Dietary Supplement Practices in Maternal, Infancy and Preschool Ages: Findings of a National Representative Cross-Sectional Study
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Sampling Procedure, and Eligibility of Participants
2.2. Sample Size Calculation
2.3. Data Collection: Assessment of Oral Dietary Supplementation
2.4. Ethical Considerations
2.5. Statistical Analyses
3. Results
3.1. General Characteristics of Mothers and Their Under-5 Children in This Study
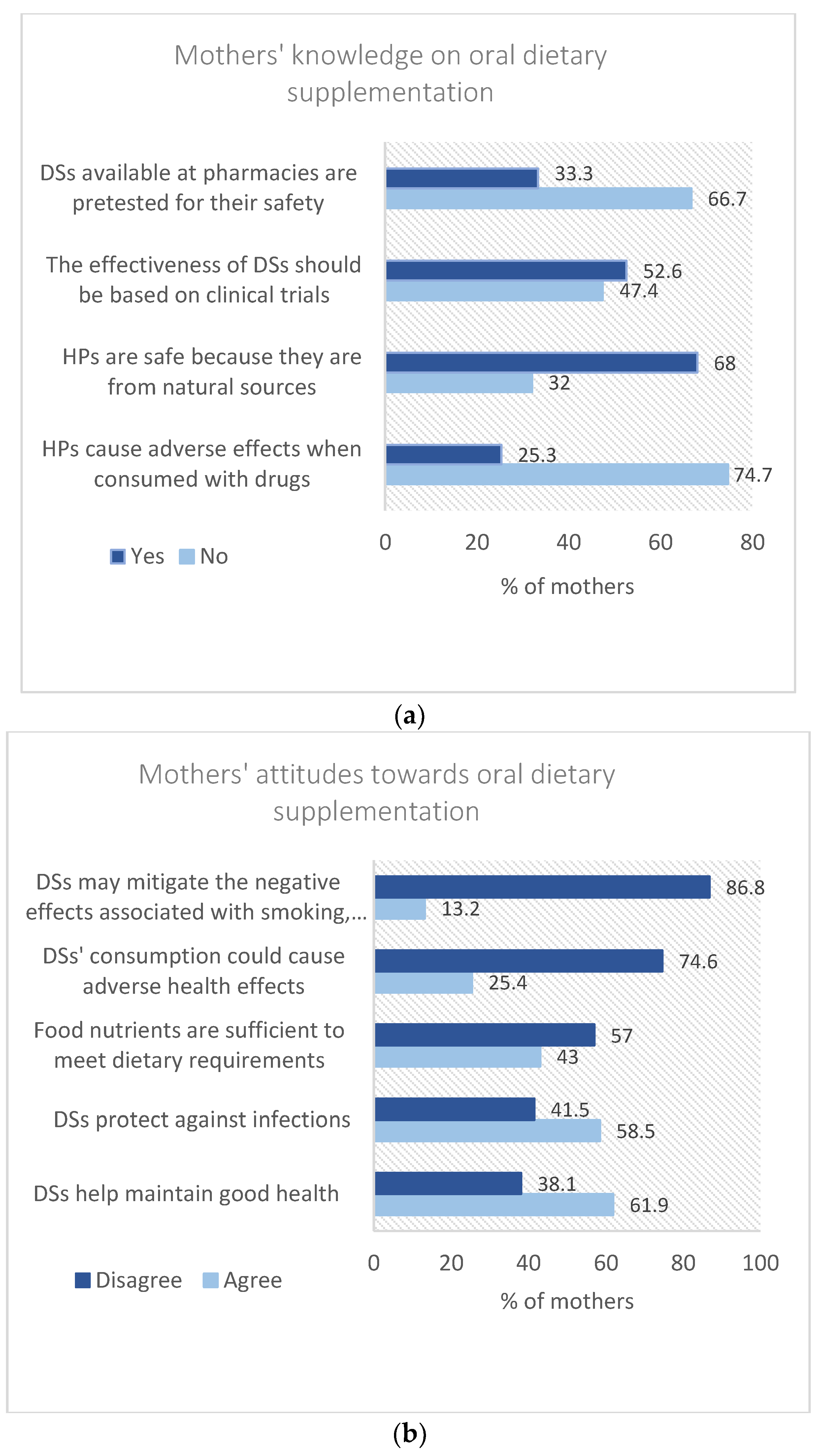
3.2. Mothers’ Knowledge and Attitudes towards Oral Dietary Supplementation
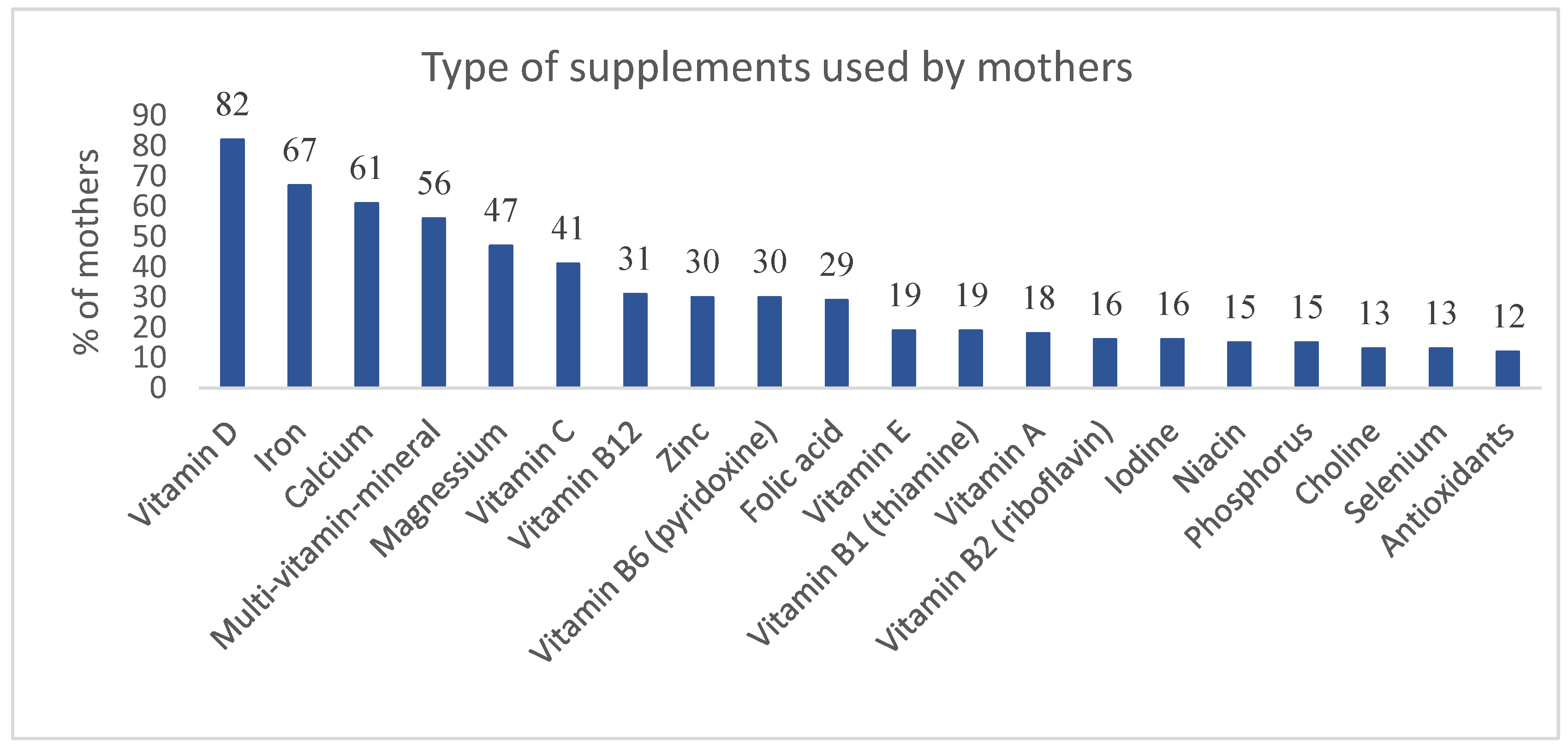
3.3. Practices Related to Oral Dietary Supplementation among Mothers
3.4. The Frequency and Duration of Use of Single Vitamin/or Mineral and Multi-Vitamin-Mineral Supplements among Mothers
3.5. Practices Related to Oral Dietary Supplementation among under-5 Children
3.6. The Frequency and Duration of Use of Single Vitamin/Or Mineral and Multi-Vitamin-Mineral Supplements among under-5 Children
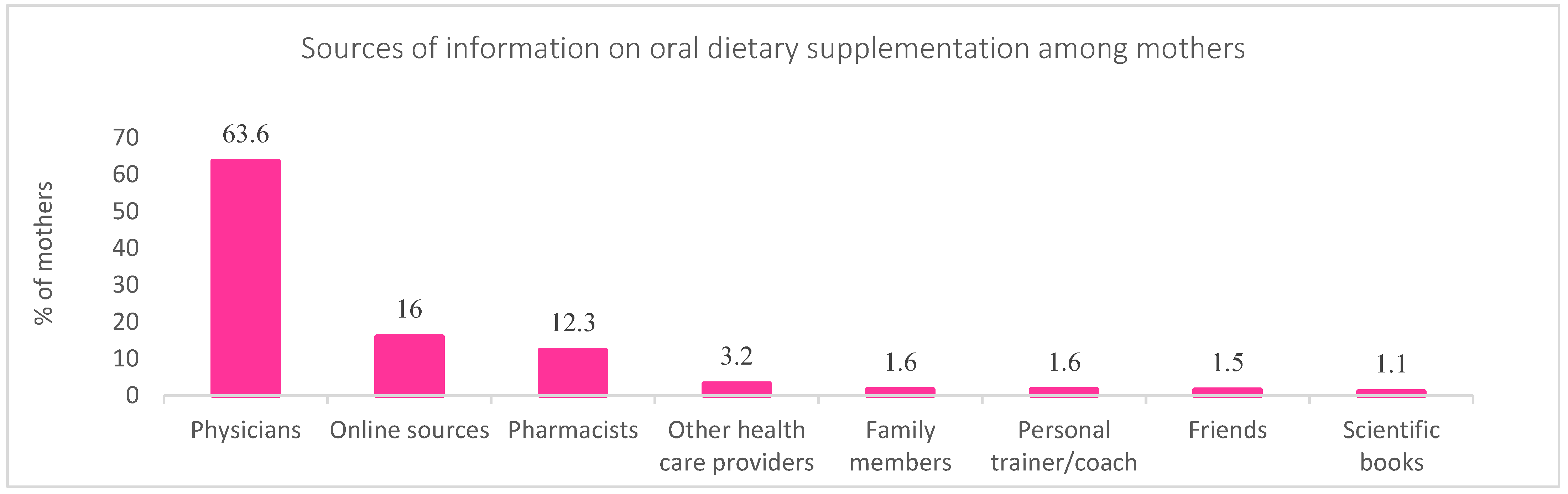
3.7. Mothers’ Sources of Information about Oral Dietary Supplementation
3.8. Side Effects Reported by Mothers Due to DSs Use
3.9. The Associations between Study Variables and Oral Dietary Supplementation among Mothers and Their under-5 Children
3.10. Correlates of Dietary Supplementation among Mothers and Their under-5 Children in This Study: Regression Analysis
4. Discussion
4.1. Mothers’ Knowledge and Attitudes towards Oral Dietary Supplementation
4.2. Practices Related to Oral Dietary Supplementation among Mothers
4.3. Practices Related to Oral Dietary Supplementation among under-5 Children
4.4. The Correlates of Oral Dietary Supplementation among Mothers and Their under-5 Children
4.5. Reported Side Effects Due to DSs Use
4.6. Limitations and Strengths of the Study
5. Conclusions
Future Directions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Crnusa. Dietary Supplement Use Reaches All-Time High. 2019. Available online: https://www.crnusa.org/newsroom/dietary-supplement-use-reaches-all-time-high (accessed on 22 July 2022).
- Mohsen, H.; Yazbeck, N.; Al-Jawaldeh, A.; Chahine, N.B.; Hamieh, H.; Mourad, Y.; Skaiki, F.; Salame, H.; Salameh, P.; Hoteit, M. Knowledge, Attitudes, and Practices Related to Dietary Supplementation, before and during the COVID-19 Pandemic: Findings from a Cross-Sectional Survey in the Lebanese Population. Int. J. Environ. Res. Public Health 2021, 18, 8856. [Google Scholar] [CrossRef]
- University of Michigan Health. Healthy Eating and Use of Dietary Supplements in Children. National Poll on Children’s Health. 2022. Available online: https://mottpoll.org/reports/healthy-eating-and-use-dietary-supplements-children (accessed on 22 July 2022).
- Musaiger, A.O.; Hassan, A.S.; Obeid, O. The Paradox of Nutrition-Related Diseases in the Arab Countries: The Need for Action. Int. J. Environ. Res. Public Health 2011, 8, 3637–3671. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Pediatrics. Dietary Supplements for Toddlers. 2017. Available online: https://www.healthychildren.org/English/ages-stages/toddler/nutrition/Pages/Dietary-Supplements-for-Toddlers.aspx (accessed on 12 July 2022).
- Food and Drug Administration. 2022. Available online: https://www.fda.gov/consumers/consumer-updates/dietary-supplements (accessed on 12 July 2022).
- Alowais, M.A.; Selim, M.A.E.-H. Knowledge, attitude, and practices regarding dietary supplements in Saudi Arabia. J. Fam. Med. Prim. Care 2019, 8, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Gardiner, P. Dietary Supplement Use in Children: Concerns of Efficacy and Safety. Am. Fam. Physician 2005, 71, 1068–1071. Available online: https://www.aafp.org/pubs/afp/issues/2005/0315/p1068.html#afp20050315p1068-b2 (accessed on 12 July 2022). [PubMed]
- Bailey, R.L.; Fulgoni, V.L., 3rd; Keast, D.R.; Lentino, C.V.; Dwyer, J. Do Dietary Supplements Improve Micronutrient Sufficiency in Children and Adolescents? J. Pediatr. 2012, 161, 837–842. [Google Scholar] [CrossRef]
- Hoteit, M.; Ibrahim, C.; Saadeh, D.; Al-Jaafari, M.; Atwi, M.; Alasmar, S.; Najm, J.; Sacre, Y.; Hanna-Wakim, L.; Al-Jawaldeh, A. Correlates of Sub-Optimal Feeding Practices among under-5 Children amid Escalating Crises in Lebanon: A National Representative CrossSectional Study. Children 2022, 9, 817. [Google Scholar] [CrossRef]
- Lebanon Statistics on Women of Reproductive Age (15–49 years)-2019–2020. Available online: https://moph.gov.lb/userfiles/files/Statistics2019.pdf (accessed on 14 July 2022).
- Centers for Disease Control and Prevention. Epi Info 7. Available online: http://wwwn.cdc.gov/epiinfo/7/index.htm (accessed on 14 July 2022).
- Neves, P.A.; Barros, A.J.; Baker, P.; Piwoz, E.; Santos, T.M.; Gatica-Domínguez, G.; Vaz, J.S.; Rollins, N.; Victora, C.G. Consumption of breast milk, formula and other non-human milk by children aged under 2 years: Analysis of eighty-six low- and middle-income countries. Public Health Nutr. 2020, 25, 680–688. [Google Scholar] [CrossRef]
- CDC. Questionnaires: Breastfeeding and Infant Feeding Practices. 2019. Available online: https://www.cdc.gov/breastfeeding/data/ifps/questionnaires.htm. (accessed on 14 July 2022).
- Chen, S.; Binns, C.W.; Maycock, B.; Liu, Y.; Zhang, Y. Prevalence of Dietary Supplement Use in Healthy Pre-School Chinese Children in Australia and China. Nutrients 2014, 6, 815–828. [Google Scholar] [CrossRef]
- Sadek, Z.; Mohsen, H.; Yazbek, S.; Nabulsi, Z.A.A.; Sarraj, A.R.; Hoteit, M. Dietary Supplements Use among Athletes in Lebanon: Knowledge, Attitudes, Practices, and Correlates. Foods 2022, 11, 1521. [Google Scholar] [CrossRef]
- Food and Drug Administration. FDA. Center for Food Safety, Applied Nutrition. Questions and Answers on Dietary Supplements. Available online: https://www.fda.gov/food/information-consumers-using-dietary-supplements/questions-and-answers-dietary-supplements. (accessed on 14 July 2022).
- Picciano, M.F.; Dwyer, J.T.; Radimer, K.L.; Wilson, D.H.; Fisher, K.D.; Thomas, P.R.; Yetley, E.A.; Moshfegh, A.J.; Levy, P.S.; Nielsen, S.J.; et al. Dietary Supplement Use Among Infants, Children, and Adolescents in the United States, 1999–2002. Arch. Pediatr. Adolesc. Med. 2007, 161, 978–985. [Google Scholar] [CrossRef] [Green Version]
- Madden, M.M.; DeBias, D.; Cook, G.E. Market analysis of vitamin supplementation in infants and children: Evidence from the dietary supplement label database: Evidence from the dietary supplement label database. JAMA Pediatr. 2014, 168, 291–292. [Google Scholar] [CrossRef]
- Basch, C.H.; Roberts, K.J.; Ethan, D.; Samayoa-Kozlowsky, S. An Examination of Marketing Techniques used to Promote Children’s Vitamins in Parenting Magazines. Glob. J. Health Sci. 2014, 7, 171–176. [Google Scholar] [CrossRef]
- Jun, S.; Gahche, J.J.; Potischman, N.; Dwyer, J.T.; Guenther, P.M.; Sauder, K.A.; Bailey, R.L. Dietary Supplement Use and Its Micronutrient Contribution During Pregnancy and Lactation in the United States. Obstet. Gynecol. 2020, 135, 623–633. [Google Scholar] [CrossRef]
- Keikha, M.; Shayan-Moghadam, R.; Bahreynian, M.; Kelishadi, R. Nutritional supplements and mother’s milk composition: A systematic review of interventional studies. Int. Breastfeed J. 2021, 16, 1. [Google Scholar] [CrossRef]
- CDC. 2020. Available online: https://www.cdc.gov/breastfeeding/breastfeeding-special-circumstances/diet-and-micronutrients/maternal-diet.html#:~:text=increase%20while%20breastfeeding%3F- (accessed on 10 July 2022).
- Blumfield, M.L.; Hure, A.J.; MacDonald-Wicks, L.; Smith, R.; Collins, C.E. A systematic review and meta-analysis of micronutrient intakes during pregnancy in developed countries. Nutr. Rev. 2013, 71, 118–132. [Google Scholar] [CrossRef]
- Kumari, S.; Garg, N.; Kumar, A.; Guru, P.K.I.; Ansari, S.; Anwar, S.; Singh, K.P.; Kumari, P.; Mishra, P.K.; Gupta, B.K.; et al. Maternal and severe anaemia in delivering women is associated with risk of preterm and low birth weight: A cross sectional study from Jharkhand, India. One Health 2019, 8, 100098. [Google Scholar] [CrossRef]
- Kusin, J.; Renqvist, U.; Kardjati, S.; Houtkooper, J. Energy supplementation during pregnancy and postnatal growth. Lancet 1992, 340, 623–626. [Google Scholar] [CrossRef]
- Khan, A.I.; Kabir, I.; Ekström, E.-C.; Åsling-Monemi, K.; Alam, D.S.; Frongillo, E.A.; Yunus, M.; Arifeen, S.; Persson, L. Effects of prenatal food and micronutrient supplementation on child growth from birth to 54 months of age: A randomized trial in Bangladesh. Nutr. J. 2011, 10, 134. [Google Scholar] [CrossRef]
- de Boer, A.; Bast, A.; Godschalk, R. Dietary supplement intake during pregnancy; better safe than sorry? Regul. Toxicol. Pharmacol. 2018, 95, 442–447. [Google Scholar] [CrossRef]
- Appel, K.; Jung, C.; Nowak, N.; Golsong, N.; Lindtner, O. Intake of dietary supplements in infants and (young) children in Germany Results of the KiESEL Study. Ernahr. Umsch. 2021, 68, 224–230. [Google Scholar] [CrossRef]
- Gahche, J.J.; Herrick, K.A.; Potischman, N.; Bailey, R.L.; Ahluwalia, N.; Dwyer, J.T. Dietary supplement use among infants and toddlers aged <24 months in the United States, NHANES 2007–2014. J. Nutr. 2019, 149, 314–322. [Google Scholar] [CrossRef]
- Briefel, R.; Hanson, C.; Fox, M.K.; Novak, T.; Ziegler, P. Feeding Infants and Toddlers Study: Do Vitamin and Mineral Supplements Contribute to Nutrient Adequacy or Excess among US Infants and Toddlers? J. Am. Diet. Assoc. 2006, 106, 52.e1–52.e15. [Google Scholar] [CrossRef]
- Chuang, C.-H.; Yang, S.-H.; Chang, P.-J.; Chen, P.-C.; Chen, Y.C. Dietary Supplement Intake by 6-month-old Taiwanese Infants. J. Pediatr. Gastroenterol. Nutr. 2012, 54, 71–76. [Google Scholar] [CrossRef]
- Ishitsuka, K.; Sasaki, S.; Mezawa, H.; Konishi, M.; Igarashi, M.; Yamamoto-Hanada, K.; Nakayama, S.F.; Ohya, Y. Dietary supplement use in elementary school children: A Japanese web-based survey. Environ. Health Prev. Med. 2021, 26, 63. [Google Scholar] [CrossRef]
- Kobayashi, E.; Nishijima, C.; Sato, Y.; Umegaki, K.; Chiba, T. The Prevalence of Dietary Supplement Use Among Elementary, Junior High, and High School Students: A Nationwide Survey in Japan. Nutrients 2018, 10, 1176. [Google Scholar] [CrossRef]
- Bailey, R.L.; Gahche, J.J.; Thomas, P.R.; Dwyer, J.T. Why US children use dietary supplements. Pediatr. Res. 2013, 74, 737–741. [Google Scholar] [CrossRef]
- Sicińska, E.; Pietruszka, B.; Januszko, O.; Kałuża, J. Different Socio-Demographic and Lifestyle Factors Can Determine the Dietary Supplement Use in Children and Adolescents in Central-Eastern Poland. Nutrients 2019, 11, 658. [Google Scholar] [CrossRef]
- Piórecka, B.; Koczur, K.; Cichocki, R.; Jagielski, P.; Kawalec, P. Socio-Economic Factors Influencing the Use of Dietary Supplements by Schoolchildren from Małopolska Voivodship (Southern Poland). Int. J. Environ. Res. Public Health 2022, 19, 7826. [Google Scholar] [CrossRef]
- McCrory, M.; Jaret, C.; Kim, J.; Reitzes, D. Dietary patterns among Vietnamese and Hispanic immigrant elementary school children participating in an after school program. Nutrients 2017, 9, 460. [Google Scholar] [CrossRef]
- Jeon, J.H.; Seo, M.Y.; Kim, S.-H.; Park, M.J. Dietary supplement use in Korean children and adolescents, KNHANES 2015–2017. Public Health Nutr. 2020, 24, 957–964. [Google Scholar] [CrossRef]
- Mazurek, M.; Mól, N.; Zasada, M.; Zasada, W.; Pyznar, O.; Kwinta, P. Dietary supplements use among children from south-eastern Poland. Pediatr. Polska 2022, 97, 13–19. [Google Scholar] [CrossRef]
- Leung, S.Y.; Lum, C.M. Use of nutritional health supplements and associated factors among parents with children at kindergartens in Hong Kong. Hong Kong Med. J. 2011, 17, 365–371. [Google Scholar] [PubMed]
- Mostafaavi Beata. Half of Parents Regularly Give Kids a Dietary Supplement. 2022. Available online: https://healthblog.uofmhealth.org/childrens-health/half-of-parents-regularly-give-kids-a-dietary-supplement. (accessed on 14 July 2022).
- Baker, R.D.; Greer, F.R. Diagnosis and prevention of iron deficiency and iron-deficiency anemia in infants and young children (0–3 years of age) (clinical report). In Pediatric Clinical Practice Guidelines & Policies; American Academy of Pediatrics: Itasca, IL, USA, 2013; p. 895. [Google Scholar]
- NHS. Vitamins for Children. 2020. Available online: https://www.nhs.uk/conditions/baby/weaning-and-feeding/vitamins-for-children/ (accessed on 14 July 2022).
- Black, L.I.; Clarke, T.C.; Patricia, H.M.; Barnes Stussman, B.J.; Nahin, R.L. Use of Complementary Health Approaches Among Children Aged 4–17 Years in the United States: National Health Interview Survey, 2007–2012. Number. 2015;78. Available online: https://www.cdc.gov/nchs/data/nhsr/nhsr078.pdf (accessed on 7 July 2022).
- Davis, S. Getting Too Much of Vitamins and Minerals. WebMD. 2011. Available online: https://www.webmd.com/diet/guide/effects-of-taking-too-many-vitamins. (accessed on 7 July 2022).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mothers (n = 511) | |
|---|---|
| Mean ± SD | |
| Age (years) | 30.25 ± 4.98 |
| BMI (kg/m2) | 24.85 ± 4.53 |
| n (%) | |
| Age category | |
| Youth (18–24 years old) | 58 (11.4) |
| Adults (25–49 years old) | 453 (88.6) |
| Weight status (n = 503) | |
| Underweight | 21 (4.2) |
| Normal weight | 262 (52.0) |
| Overweight | 153 (30.4) |
| Obese | 67 (13.4) |
| Current Residence | |
| Beirut and Mount Lebanon | 288 (56.4) |
| North Lebanon and Akkar | 124 (24.2) |
| Beqaa and Baalbeck/Hermel | 39 (7.6) |
| South Lebanon and Nabatieh | 60 (11.8) |
| Marital status | |
| Married | 509 (99.6) |
| Divorced | 2 (0.4) |
| Number of children per household | |
| One child | 241 (47.2) |
| 2–3 children | 240 (46.6) |
| More than 3 children | 30 (6.2) |
| Mothers of twins or triplets | |
| Yes | 26 (5.0) |
| No | 485 (95.0) |
| The mother is currently pregnant | |
| Yes | 53 (10.3) |
| No | 458 (89.7) |
| Family income per month (n = 510) | |
| Less than LBP 750,000 | 44 (8.6) |
| LBP 750,000–2,250,000 | 304 (59.6) |
| More than LBP 2,250,000 | 162 (31.8) |
| The mother is currently working | |
| Yes | 219 (42.8) |
| No | 292 (57.2) |
| Healthcare specialization among working mothers (n = 219) | |
| Yes | 56 (25.6) |
| No | 163 (74.4) |
| COVID-19 infection | |
| Yes | 123 (24.1) |
| No | 388 (75.9) |
| Household crowding index 1 (Mean ± SD) | 1.03 ± 0.40 |
| Overall (n = 511) | Boys (n = 230) | Girls (n = 281) | ||
|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | p-Value | |
| Age (months) | 18.7 ± 15.5 | 18.0 ± 15.5 | 19.5 ± 15.6 | 0.31 |
| Weight at birth in grams | 3168.9 ± 617.9 | 3074.18 ± 622.2 | 3283.35 ± 594.2 | <0.001 * |
| Height at birth in cm | 49.5 ± 5.2 | 49.2 ± 4.74 | 49.8 ± 5.7 | 0.31 |
| n (%) | n (%) | n (%) | ||
| Age categories | 0.13 | |||
| 0–6 months | 124 (25.3) | 54 (24.4) | 70 (25.7) | |
| 6–12 months | 105 (21.3) | 38 (17.3) | 67 (24.8) | |
| 1–3 years | 179 (36.4) | 91 (40.9) | 88 (32.5) | |
| 3–5 years | 84 (17.0) | 38 (17.4) | 46 (17.0) | |
| COVID-19 infection | 0.13 | |||
| Yes | 83 (16.4) | 32 (13.7) | 52 (18.6) | |
| No | 428 (83.6) | 198 (86.3) | 229 (81.4) | |
| The child is ever breastfed | 0.26 | |||
| No | 25 (4.8) | 14 (5.9) | 11 (3.9) | |
| Yes | 486 (95.2) | 216 (94.1) | 270 (96.1) | |
| The child is exclusively breastfed (n = 486) | 0.24 | |||
| Less than 6 months of age | 287 (59.1) | 121 (56.1) | 166 (61.3) | |
| 6 months and above | 199 (40.9) | 95 (43.9) | 105 (38.7) | |
| Initiation of complementary feeding (n = 373) | 0.001 * | |||
| Less than 6 months of age | 193 (51.7) | 98 (61.5) | 95 (44.5) | |
| 6 months and above | 180 (48.2) | 61 (38.5) | 118 (55.5) |
| MVM * n (%) | Antioxidants n (%) | Vitamin A n (%) | Vitamin C n (%) | Vitamin D n (%) | Vitamin E n (%) | Vitamin B1 n (%) | Vitamin B2 n (%) | Vitamin B6 n (%) | Vitamin B12 n (%) | |
|---|---|---|---|---|---|---|---|---|---|---|
| Daily | 95 (39.2) | 15 (6.2) | 28 (11.6) | 49 (20.3) | 73 (30.2) | 29 (12.0) | 26 (10.7) | 23 (9.5) | 39 (16.1) | 37 (15.3) |
| 2–6 times per week | 24 (9.9) | 6 (2.4) | 9 (3.7) | 30 (12.4) | 66 (27.3) | 8 (3.3) | 5 (2.1) | 4 (1.6) | 22 (9.1) | 22 (9.1) |
| Once per week | 13 (5.4) | 6 (2.4) | 5 (2.0) | 16 (6.6) | 35 (14.5) | 7 (2.9) | 11 (4.5) | 10 (4.1) | 11 (4.5) | 10 (4.1) |
| Once per month | 3 (1.2) | 1 (0.3) | 2 (0.8) | 3 (1.2) | 24 (10.0) | 2 (0.8) | 4 (1.6) | 3 (1.2) | 1 (0.3) | 5 (2.1) |
| Niacin n (%) | Folic acid n (%) | Calcium n (%) | Magnesium n (%) | Iodine n (%) | Iron n (%) | Zinc n (%) | Choline n (%) | Phosphorus n (%) | Selenium n (%) | |
| Daily | 22 (9.1) | 47 (19.4) | 95 (39.3) | 71 (29.4) | 22 (9.1) | 122 (50.4) | 35 (14.5) | 17 (7.0) | 19 (7.9) | 20 (8.3) |
| 2–6 times per week | 7 (2.9) | 14 (5.8) | 34 (14.0) | 32 (13.2) | 6 (2.4) | 24 (10.0) | 20 (8.3) | 2 (0.8) | 8 (3.3) | 2 (0.8) |
| Once per week | 5 (2.1) | 7 (2.9) | 8 (3.3) | 10 (4.1) | 10 (4.1) | 13 (5.4) | 16 (6.6) | 10 (4.1) | 6 (2.5) | 8 (3.3) |
| Once per month | 1 (0.3) | 2 (0.8) | 9 (3.7) | 1 (0.3) | 1 (0.3) | 5 (2.1) | 1 (0.3) | 2 (0.8) | 2 (0.8) | 1 (0.3) |
| Among Supplement Users (n = 328) | Vitamin A | Vitamin E | Vitamin C | Vitamin B1 | Vitamin B2 | Vitamin B6 | Vitamin B12 | Niacin | Folic Acid |
|---|---|---|---|---|---|---|---|---|---|
| Frequency of use | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) |
| Once per day | 73 (22.2) | 54 (16.4) | 91 (27.6) | 50 (15.2) | 51 (15.5) | 49 (14.9) | 59 (17.9) | 40 (12.2) | 45 (13.7) |
| Twice per day | 2 (0.6) | 1 (0.3) | 2 (0.6) | 1 (0.3) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Duration of use | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) |
| Less than 3 months | 33 (9.9) | 25 (7.6) | 34 (10.3) | 26 (7.9) | 20 (6.1) | 13 (4.0) | 21 (6.4) | 16 (4.9) | 20 (6.1) |
| 3–6 months | 22 (6.8) | 16 (4.9) | 30 (9.1) | 14 (4.3) | 17 (5.2) | 20 (6.1) | 19 (5.8) | 10 (3.1) | 10 (3.1) |
| 1 year | 13 (3.8) | 8 (2.4) | 19 (5.8) | 5 (1.5) | 7 (2.1) | 9 (2.7) | 7 (2.1) | 7 (2.1) | 7 (2.1) |
| More than 1 year | 8 (2.3) | 6 (1.8) | 10 (3.1) | 6 (1.8) | 6 (1.8) | 6 (1.8) | 12 (3.6) | 6 (1.8) | 8 (2.3) |
| Calcium | Magnesium | Iodine | Iron | Zinc | Choline | Multivitamin drops | Soft gel multivitamin | Probiotics; n-3 fatty acid | |
| Frequency of use | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) |
| Once per day | 71 (21.7) | 56 (17.0) | 41 (12.5) | 194 (58.9) | 58 (17.6) | 40 (12.1) | 198 (60.2) | 30 (9.1) | 47 (14.2) |
| Twice per day | 1 (0.3) | 0 (0) | 0 (0) | 3 (1.0) | 0 (0) | 0 (0) | 1 (0.3) | 0 (0) | 3 (0.9) |
| Duration of use | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) |
| Less than 3 months | 30 (9.1) | 20 (6.8) | 15 (4.6) | 51 (15.5) | 16 (4.8) | 16 (4.8) | 137 (41.6) | 11 (3.3) | 16 (4.8) |
| 3–6 months | 25 (7.6) | 21 (6.4) | 11 (3.3) | 94 (28.6) | 19 (7.9) | 10 (3.0) | 43 (13.0) | 10 (3.0) | 8 (2.4) |
| 1 year | 6 (1.8) | 6 (1.8) | 7 (2.1) | 39 (11.8) | 10 (3.0) | 9 (2.7) | 13 (3.9) | 5 (1.5) | 16 (4.8) |
| More than 1 year | 11 (3.3) | 8 (2.4) | 8 (2.4) | 14 (4.2) | 13 (3.9) | 6 (1.8) | 6 (1.8) | 4 (1.2) | 10 (3.0) |
| Variables | Dietary Supplementation among Mothers | Dietary Supplementation among under-5 Children | p-Value (a) | p-Value (b) | ||
|---|---|---|---|---|---|---|
| No (n = 269) | Yes (n = 242) | No (n = 182) | Yes (n = 329) | |||
| n (%) | n (%) | n (%) | n (%) | |||
| Mother’s age | 0.28 | 0.56 | ||||
| Youth (18–24 years old) | 35 (12.9) | 23 (9.8) | 19 (10.2) | 39 (12.1) | ||
| Adults (24–49 years old) | 234 (87.1) | 219 (90.2) | 163 (89.8) | 290 (87.9) | ||
| Mother’s weight status | 0.60 | 0.50 | ||||
| Underweight | 11 (4.2) | 10 (4.2) | 5 (2.8) | 16 (5.0) | ||
| Normal weight | 132 (49.6) | 130 (54.7) | 100 (55.6) | 162 (50.0) | ||
| Overweight | 88 (33.1) | 65 (27.4) | 53 (29.3) | 100 (31.1) | ||
| Obese | 35 (13.1) | 32 (13.7) | 22 (12.3) | 45 (14.0) | ||
| Child’s birth weight (mean ± SD) | 3177.0 ± 658 | 3160 ± 572 | 3222.0 ± 592 | 3140.0 ± 631 | 0.61 | 0.05 |
| Residency | 0.12 | 0.75 | ||||
| Mount Lebanon/Beirut | 145 (54) | 143 (59) | 102 (55.8) | 186 (56.7) | ||
| North Lebanon and Akkar | 61 (22.7) | 63 (25.9) | 42 (23.1) | 82 (24.8) | ||
| Beqaa and Baalbeck-Hermel | 23 (8.6) | 16 (6.5) | 13 (7.3) | 26 (7.8) | ||
| South Lebanon and Nabatieh | 40 (14.7) | 20 (8.6) | 25 (13.8) | 35 (10.7) | ||
| Marital Status | 0.18 | 0.67 | ||||
| Married | 267 (99.3) | 242 (99.9) | 181 (99.4) | 328 (99.7) | ||
| Divorced | 2 (0.7) | 0 (0.1) | 1 (0.6) | 1 (0.3) | ||
| Number of children | 0.04 * | 0.34 | ||||
| One child | 122 (45.5) | 119 (49.2) | 76 (41.9) | 165 (50.2) | ||
| 2–3 | 124 (46.2) | 116 (47.8) | 91 (50.1) | 149 (45.2) | ||
| More than 3 | 22 (8.3) | 7 (3.0) | 14 (8.0) | 15 (4.6) | ||
| Mother of twins or triplets | ||||||
| No | 252 (94.0) | 233 (96.0) | 175 (96.0) | 310 (94.4) | 0.34 | 0.41 |
| Yes | 16 (6.0) | 10 (4.0) | 7 (4.0) | 19 (5.6) | ||
| Age of the child | 0.01 * | 0.22 | ||||
| 0–6 months | 57 (21.8) | 69 (29.5) | 45 (25.0) | 82(25.7) | ||
| 6–12 months | 51 (19.4) | 62 (26.6) | 35 (19.2) | 78 (24.8) | ||
| 1–3 years | 124 (47.8) | 81 (35.1) | 75 (42.6) | 130 (41.4) | ||
| 3–5 years | 28 (10.9) | 20 (8.8) | 23 (13.1) | 25 (14.8) | ||
| Gender of the child | 0.98 | 0.01 * | ||||
| Girl | 148 (55.0) | 133 (54.9) | 109 (60.1) | 172 (52.2) | ||
| Boy | 121 (45.0) | 109 (45.1) | 73 (39.9) | 157 (47.8) | ||
| Child is ever breastfed | 0.06 | 0.05 | ||||
| No | 17 (6.5) | 7 (2.9) | 13 (7.3) | 11 (3.4) | ||
| Yes | 251 (93.5) | 235 (97.1) | 169 (92.7) | 318 (96.6) | ||
| Child is exclusively breastfed | 0.21 | 0.87 | ||||
| Less than 6 months | 155 (61.6) | 132 (56.2) | 99 (58.6) | 188 (59.2) | ||
| More than 6 months | 96 (38.4) | 103 (43.8) | 70 (41.4) | 129 (40.8) | ||
| Initiation of complementary feeding | 0.17 | 0.08 | ||||
| Less than 6 months | 109 (55.0) | 84 (48.1) | 55 (45.4) | 137 (54.8) | ||
| 6 months and more | 89 (45.0) | 91 (51.9) | 67 (54.6) | 113 (45.2) | ||
| History of COVID-19 in mothers | 0.75 | 0.21 | ||||
| No | 205 (76.5) | 183 (75.4) | 144 (78.9) | 244 (74.3) | ||
| Yes | 63 (23.5) | 60 (24.6) | 38 (21.1) | 85 (25.7) | ||
| History of COVID-19 in children | 0.88 | 0.14 | ||||
| No | 225 (83.9) | 202 (83.3) | 158 (86.9) | 269 (81.8) | ||
| Yes | 43 (16.1) | 40 (16.7) | 23 (13.1) | 60 (18.2) | ||
| Mother as healthcare worker (n = 219 working mothers) | 0.09 | 0.14 | ||||
| No | 72 (69.1) | 91 (79.4) | 55 (68.8) | 108 (77.7) | ||
| Yes | 32 (30.9) | 24 (20.6) | 25 (31.2) | 31 (22.3) | ||
| Mother is pregnant | <0.001 ** | 0.79 | ||||
| No | 257 (95.7) | 201 (83.0) | 164 (90.1) | 294 (89.4) | ||
| Yes | 12 (4.3) | 41 (17.0) | 18 (9.9) | 35 (10.6) | ||
| Mothers’ attitudes: DSs are necessary to maintain good health | 0.01 * | <0.001 ** | ||||
| Agree | 149 (55.9) | 161 (68.6) | 66 (36.1) | 245 (76.5) | ||
| Disagree | 118 (44.1) | 74 (31.4) | 116 (63.9) | 76 (23.5) | ||
| Mothers’ attitudes: DSs help fight infections by strengthening the immunity | 0.001 * | <0.001 ** | ||||
| Agree | 137 (51.5) | 157 (66.4) | 62 (33.8) | 233 (72.5) | ||
| Disagree | 129 (48.5) | 80 (33.6) | 120 (66.2) | 88 (27.5) | ||
| Mothers’ attitudes: DS use could cause health adverse effects | 0.91 | 0.85 | ||||
| Agree | 68 (25.7) | 60 (25.1) | 45 (25.0) | 83 (25.6) | ||
| Disagree | 198 (74.3) | 179 (74.9) | 136 (75.0) | 241 (74.4) | ||
| Mothers’ attitudes: Food nutrients are sufficient to meet dietary requirements with no need for dietary supplementation | 0.88 | 0.06 | ||||
| Agree | 115 (43.3) | 103 (42.5) | 68 (37.4) | 150 (46.0) | ||
| Disagree | 151 (56.7) | 139 (57.5) | 114 (62.6) | 176 (54.0) | ||
| Mothers’ knowledge: HPs can cause adverse effects if consumed with drugs | 0.001 * | 0.84 | ||||
| No | 218 (81.0) | 164 (67.7) | 137 (75.4) | 245 (74.4) | ||
| Yes | 51 (19.0) | 78 (32.3) | 45 (24.6) | 84 (25.6) | ||
| Mothers’ knowledge: HPs are safe because they are from natural sources | <0.001 ** | 0.03 * | ||||
| No | 63 (23.3) | 101 (41.8) | 47 (25.8) | 116 (35.5) | ||
| Yes | 206 (76.7) | 140 (58.2) | 135 (74.2) | 211 (64.5) | ||
| Mothers’ practices: DS use among mothers | NA | <0.001 ** | ||||
| No | NA | NA | 126 (69.4) | 142 (43.3) | ||
| Yes | NA | NA | 56 (30.6) | 187 (56.7) | ||
| Model 1: Binary Backward Stepwise Regression Taking Oral Dietary Supplementation among Mothers as the Dependent Variable (Yes vs. No (Reference)) | ||
|---|---|---|
| aOR (95% CI) | p-Value | |
| Number of children (Reference: One child) | ||
| 2–3 children | 1.1 (0.7–1.6) | 0.97 |
| More than 3 | 0.3 (0.1–0.9) | 0.02 * |
| Age of the child (Reference: 0–6 months) | ||
| 6–12 months | 1.2 (0.7–2.1) | 0.56 |
| 1–3 years | 0.4 (0.3–0.7) | 0.002 * |
| 3–5 years | 0.6 (0.3–1.2) | 0.16 |
| Mother is pregnant (Reference: No) | ||
| Yes | 7.0 (3.2–15.2) | <0.001 ** |
| Mothers’ attitude: DSs are necessary to maintain good health (Reference: Agree) | ||
| Disagree | 0.6 (0.4–0.9) | 0.01 * |
| Mothers’ knowledge: HPs can cause adverse effects if consumed with drugs (Reference: No) | ||
| Yes | 1.9 (1.2–3.0) | 0.01 * |
| Mothers’ knowledge: HPs are safe because they are from natural sources (Reference: No) | ||
| Yes | 0.4 (0.3–0.6) | <0.001 ** |
| Model 2: Binary backward stepwise regression taking oral dietary supplementation among under-5 children as the dependent variable (Yes vs. No (reference)) | ||
| AOR (95% CI) | p-value | |
| DS use among mothers (Reference: No) | ||
| Yes | 2.6 (1.7–4.0) | <0.001 * |
| Mothers’ attitude: DSs are necessary to maintain good health (Reference: Agree) | ||
| Disagree | 0.3 (0.2–0.6) | <0.001 |
| Mothers’ attitude: DSs help fight infections by strengthening the immunity (Reference: Agree) | ||
| Disagree | 0.5 (0.3–0.8) | 0.01 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mohsen, H.; Ibrahim, C.; Bookari, K.; Saadeh, D.; Al-Jawaldeh, A.; Sacre, Y.; Hanna-Wakim, L.; Al-Jaafari, M.; Atwi, M.; AlAsmar, S.; et al. Prevalence of Essential Nutrient Supplement Use and Assessment of the Knowledge and Attitudes of Lebanese Mothers towards Dietary Supplement Practices in Maternal, Infancy and Preschool Ages: Findings of a National Representative Cross-Sectional Study. Foods 2022, 11, 3005. https://doi.org/10.3390/foods11193005
Mohsen H, Ibrahim C, Bookari K, Saadeh D, Al-Jawaldeh A, Sacre Y, Hanna-Wakim L, Al-Jaafari M, Atwi M, AlAsmar S, et al. Prevalence of Essential Nutrient Supplement Use and Assessment of the Knowledge and Attitudes of Lebanese Mothers towards Dietary Supplement Practices in Maternal, Infancy and Preschool Ages: Findings of a National Representative Cross-Sectional Study. Foods. 2022; 11(19):3005. https://doi.org/10.3390/foods11193005
Chicago/Turabian StyleMohsen, Hala, Carla Ibrahim, Khlood Bookari, Danielle Saadeh, Ayoub Al-Jawaldeh, Yonna Sacre, Lara Hanna-Wakim, Marwa Al-Jaafari, Marwa Atwi, Sabine AlAsmar, and et al. 2022. "Prevalence of Essential Nutrient Supplement Use and Assessment of the Knowledge and Attitudes of Lebanese Mothers towards Dietary Supplement Practices in Maternal, Infancy and Preschool Ages: Findings of a National Representative Cross-Sectional Study" Foods 11, no. 19: 3005. https://doi.org/10.3390/foods11193005