
Effect of Apple Consumption on Postprandial Blood Glucose Levels in Normal Glucose Tolerance People versus Those with Impaired Glucose Tolerance

 ,
,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Test Meals
2.3. Test Protocol, Blood Sample Collection, and Analysis of Glucose and Insulin Levels
2.4. Statistical Analysis
2.5. Determination of Carbohydrates
2.6. Conditions for LC Measurements
2.7. Sample Preparation for Analysis of Total Phenolics
2.8. Preparation of Folin Reagent and Total Phenolics
3. Results
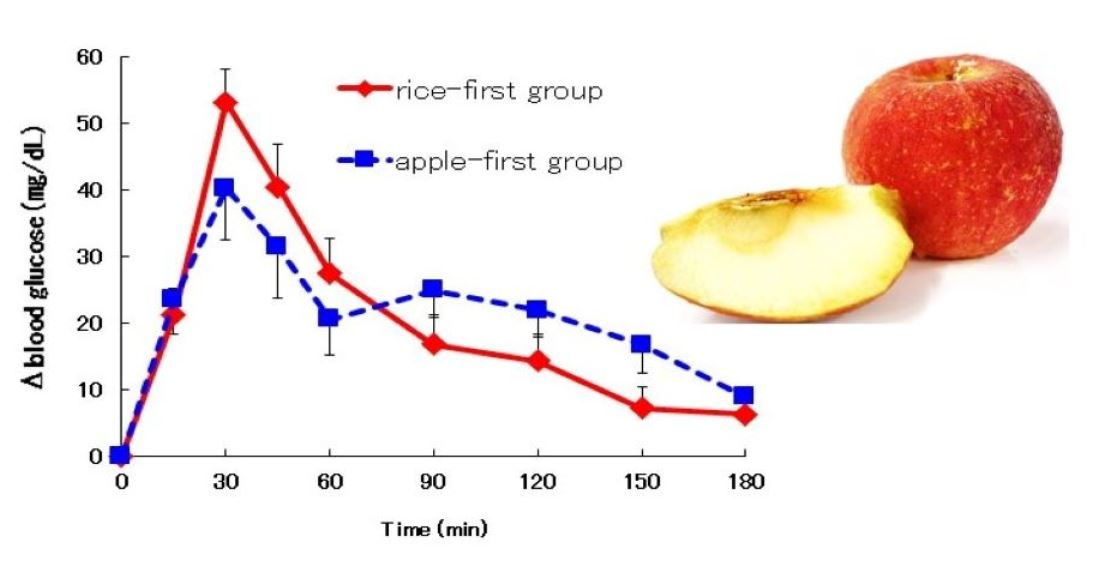
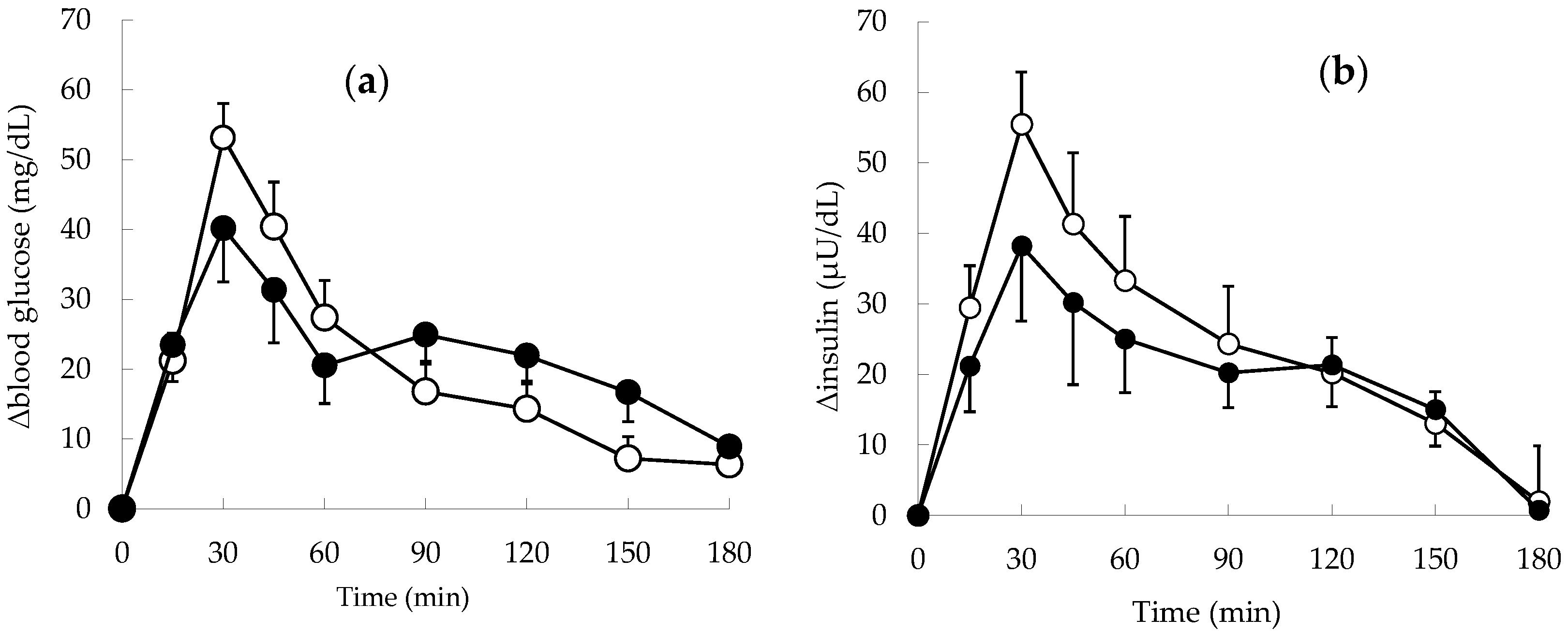
3.1. Changes in Blood Glucose and Insulin Levels in Normal Subjects
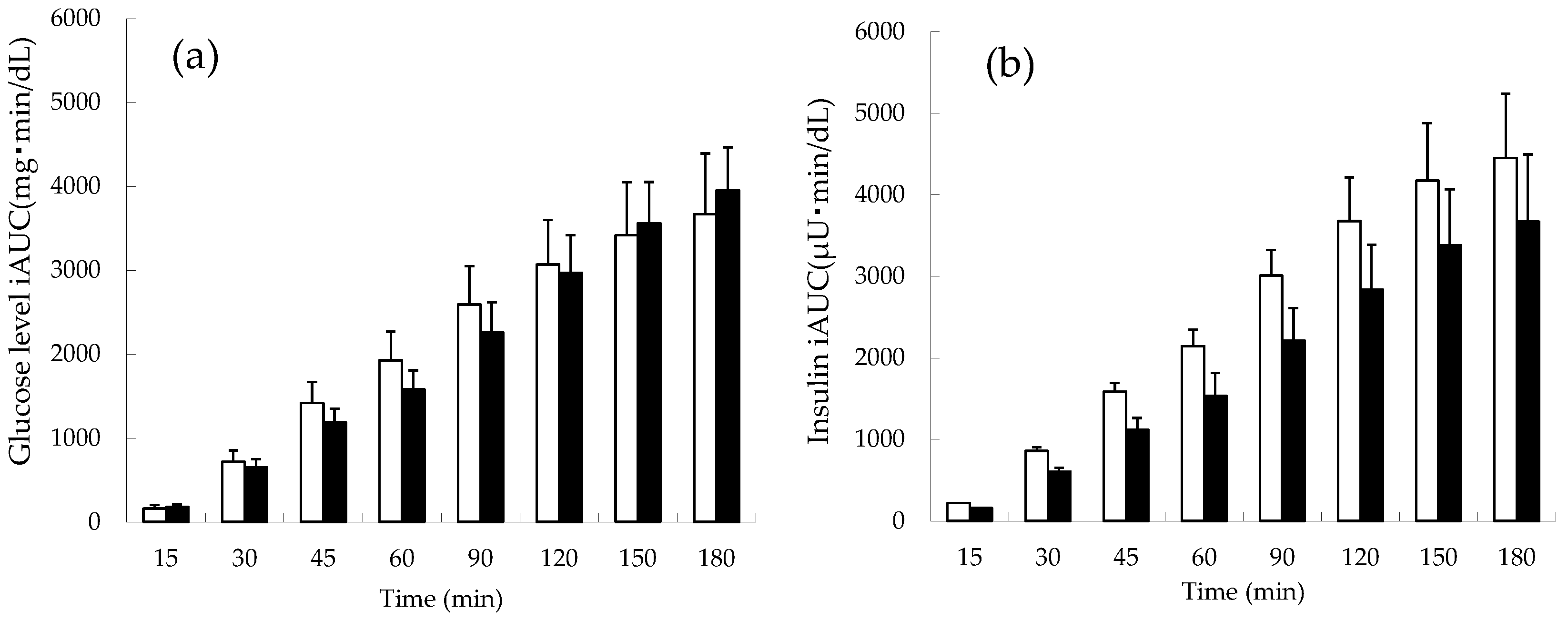
3.2. Changes in the Cumulative iAUC of Blood Glucose and Insulin in Normal Subjects
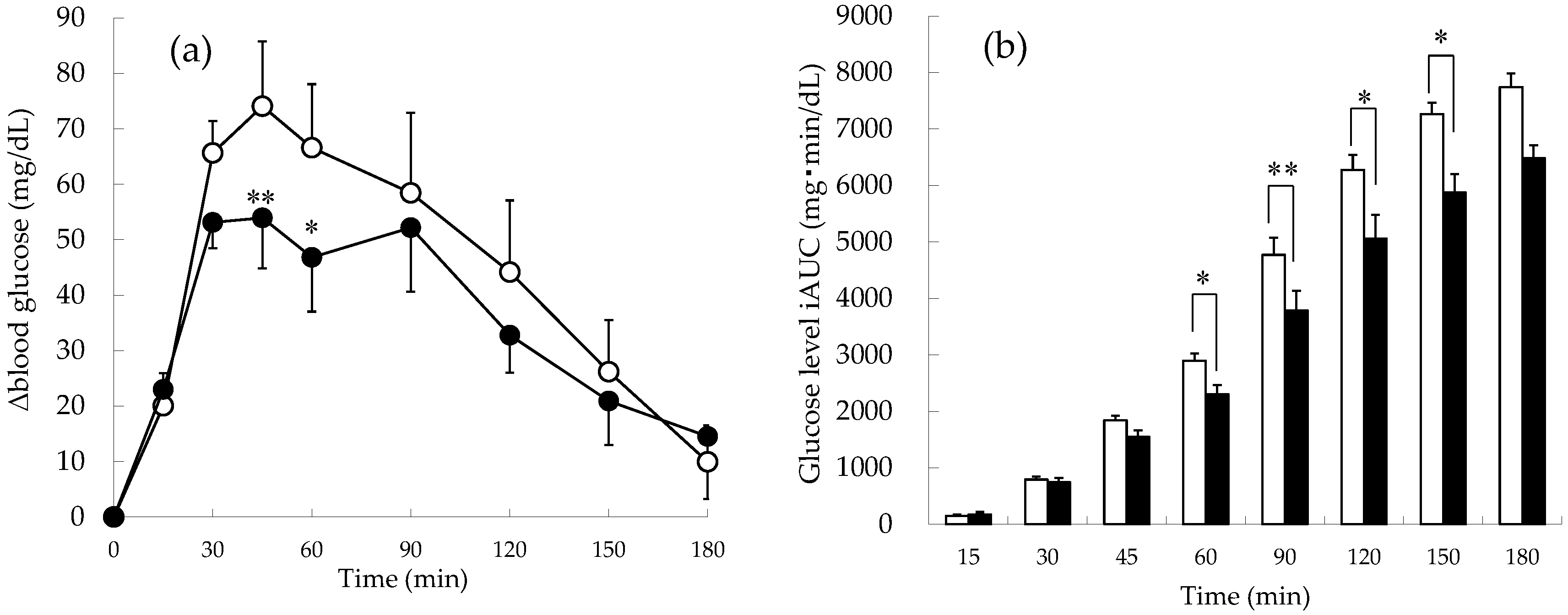
3.3. Changes in Blood Glucose Levels and Cumulative iAUC of Blood Glucose in Patients with Impaired Glucose Tolerance
3.4. Dynamic Parameters in Normal and Impaired Glucose Tolerance Subjects
3.5. Determination of Carbohydrate (Glucose, Fructose, and Sucrose) Contents
3.6. Determination of Polyphenol Contents
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dietary Reference Intakes for Japanese. 2015. Available online: https://www.mhlw.go.jp/file/06-Seisakujouhou-10900000-Kenkoukyoku/Full_DRIs2015.pdf (accessed on 28 March 2018).
- Steg, P.G.; Bhatt, D.L.; Wilson, P.W.F.; D’Agostino, R.; Ohman, E.M.; Röther, J.; Liau, C.-S.; Hirsch, A.T.; Mas, J.-L.; Ikeda, Y.; et al. One-year cardiovascular event rates in outpatients with atherothrombosis. JAMA 2007, 297, 1197–1206. [Google Scholar] [CrossRef]
- Wu, Y.; Ding, Y.; Tanaka, Y.; Zhang, W. Risk Factors Contributing to Type 2 Diabetes and Recent Advances in the Treatment and Prevention. Int. J. Med. Sci. 2014, 6, 1185–1200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trikkalinou, A.; Papazafiropoulou, A.K.; Melidonis, A. Type 2 diabetes and quality of life. World J. Diabetes 2017, 15, 120–129. [Google Scholar] [CrossRef] [PubMed]
- Jensen, T.; Deckert, T. Diabetic retinopathy, nephropathy and neuropathy. Generalized vascular damage in insulin-dependent diabetic patients. Horm. Metab. Res. Suppl. 1992, 26, 68–70. [Google Scholar] [PubMed]
- Johansson, B.L.; Borg, K.; Fernqvist-Forbes, E.; Kernell, A.; Odergren, T.; Wahren, J. Beneficial effects of C-peptide on incipient nephropathy and neuropathy in patients with Type 1 diabetes mellitus. Diabet. Med. 2000, 17, 181–189. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, D.J.; Wolever, T.M.; Taylor, R.H.; Barker, H.; Fielden, H.; Baldwin, J.M.; Bowling, A.C.; Newman, H.C.; Jenkins, A.L.; Goff, D.V. Glycemic index of foods: A physiological basis for carbohydrate exchange. Am. J. Clin. Nutr. 1981, 34, 362–366. [Google Scholar] [CrossRef] [Green Version]
- Jenkins, D.J.; Kendall, C.W.; McKeown-Eyssen, G.; Josse, R.G.; Silverberg, L.; Booth, G.L.; Vidgen, E.; Josse, A.R.; Nguyen, T.H.; Corrigan, S.; et al. Effect of a low-glycemic index or a high-cereal fiber diet on type 2 diabetes: A randomized trial. JAMA 2008, 300, 2742–2753. [Google Scholar] [CrossRef] [Green Version]
- Murakami, K.; Sasaki, S.; Takahashi, Y.; Okubo, H.; Hosoi, Y.; Horiguchi, H.; Oguma, E.; Kayama, F. Dietary glycemic index and load in relation to metabolic risk factors in Japanese female farmers with traditional dietary habits. Am. J. Clin. Nutr. 2006, 83, 1161–1169. [Google Scholar] [CrossRef] [Green Version]
- Tominaga, M.; Eguchi, H.; Manaka, H.; Igarashi, K.; Kato, T.; Sekikawa, A. Impaired glucose tolerance is a risk factor for cardiovascular disease. But not impaired fasting glucose. The Funagata Diabetes Study. Diabetes Care 1999, 22, 920–924. [Google Scholar] [CrossRef]
- Ceriello, A. Postprandial hyperglycemia and diabetes complications: Is it time to treat? Diabetes 2005, 54, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Rosak, C.; Nitzsche, G.; Konig, P.; Hofmann, U. The effect of the timing and the administration of acarbose on postprandial hyperglycaemia. Diabet. Med. 1995, 12, 979–984. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; Goh, H.J.; Govindharajulu, P.; Leow, M.K.-S.; Henry, C.J. Postprandial glucose, insulin and incretin responses differ by test meal macronutrient ingestion sequence (PATTERN study). Clin. Nutr. 2020, 39, 950–957. [Google Scholar] [CrossRef] [PubMed]
- Kubota, S.; Yanyan, L.; Iizuka, K.; Kuwata, H.; Seino, Y.; Yabe, D. A Review of Recent Findings on Meal Sequence: An Attractive Dietary Approach to Prevention and Management of Type 2 Diabetes. Nutrients 2020, 12, 2502. [Google Scholar] [CrossRef] [PubMed]
- Nishiyama, I.; Fukuda, T.; Shimohashi, A.; Oota, T. Sugar and Organic Acid Composition in the Fruit Juice of Different Actinidia Varieties. Food Sci. Technol. Res. 2008, 14, 67–73. [Google Scholar] [CrossRef] [Green Version]
- Ogawa, N.; Satsu, H.; Watanabe, H.; Fukaya, M.; Tsukamoto, Y.; Miyamoto, Y.; Shimizu, M. Acetic acid suppresses the increase in disaccharidase activity that occurs during culture of caco-2 cells. J. Nutr. 2000, 130, 507–513. [Google Scholar] [CrossRef]
- Liljeberg, H.G.; Björck, I.M. Delayed gastric emptying rate as a potential mechanism for lowered glycemia after eating sourdough bread: Studies in humans and rats using test products with added organic acids or an organic salt. Am. J. Clin. Nutr. 1996, 64, 886–893. [Google Scholar] [CrossRef] [Green Version]
- Groudeva, J.; Kratchanova, M.G.; Panchev, I.N.; Kratchanova, C.G. Application of granulated apple pectin in the treatment of hyperlipoproteinaemia. Z. Lebensm. Forsch. A 1997, 204, 374–378. [Google Scholar] [CrossRef]
- Schulze, C.; Bangert, A.; Kottra, G.; Geillinger, K.E.; Schwanck, B.; Vollert, H.; Blaschek, W.; Daniel, H. Inhibition of the intestinal sodium-coupled glucose transporter 1 (SGLT1) by extracts and polyphenols from apple reduces postprandial blood glucose levels in mice and humans. Mol. Nutr. Food Res. 2014, 58, 1795–1808. [Google Scholar] [CrossRef]
- Kasuya, N.; Inoue, N.; Inoue, Y.; Murata, I.; Kanamoto, I. Effect of vegetable juice consumption prior to eating rice on postprandial blood glucose and insulin levels. Exp. Ther. Med. 2019, 18, 3817–3822. [Google Scholar] [CrossRef] [Green Version]
- Inoue, Y.; Kitani, Y.; Osakabe, S.; Yamamoto, Y.; Murata, I.; Kanamoto, I. The Effects of Gold Kiwifruit Intake Timing with or without Pericarp on Postprandial Blood Glucose Level. Nutrients 2021, 19, 2103. [Google Scholar] [CrossRef]
- Sugiyama, H.; Akazome, Y.; Shoji, T.; Yamaguchi, A.; Yasue, M.; Kanda, T.; Ohtake, Y. Oligomeric procyanidins in apple polyphenol are main active components for inhibition of pancreatic lipase and triglyceride absorption. J. Agric. Food Chem. 2007, 30, 4604–4609. [Google Scholar] [CrossRef] [PubMed]
- Mancini, F.R.; Affret, A.; Dow, C.; Balkau, B.; Bonnet, F.; Boutron-Ruault, M.-C.; Fagherazzi, G. Dietary antioxidant capacity and risk of type 2 diabetes in the large prospective E3N-EPIC cohort. Diabetologia 2018, 61, 308–316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krishnamachar, S.; Mickelsen, O. The influence of different carbohydrate sources on blood glucose levels and satiety effect of physical activity on blood glucose response. Nutr. Food Sci. 1987, 41F, 29–40. [Google Scholar] [CrossRef]
- Swain, T.; Hillis, W.E. The phenolic constituents of prunus domestica. I.—The quantitative analysis of phenolic constituents. J. Sci. Food Agric. 1959, 10, 63–68. [Google Scholar] [CrossRef]
- Guo, X.-F.; Yang, B.; Tang, J.; Jiang, J.J.; Li, D. Apple and pear consumption and type 2 diabetes mellitus risk: A meta-analysis of prospective cohort studies. Food Funct. 2017, 22, 927–934. [Google Scholar] [CrossRef] [PubMed]
- Crapo, P.A.; Koltermann, O.G.; Olefsky, J.M. Effects of oral fructose in normal, diabetic and impaired glucose tolerance subjects. Diabetes Care 1980, 3, 575–582. [Google Scholar] [CrossRef]
- Alongi, M.; Verardo, G.; Gorassini, A.; Anese, M. Effect of pasteurization on in vitro α-glucosidase inhibitory activity of apple juice. LWT Food Sci. Technol. 2018, 98, 366–371. [Google Scholar] [CrossRef]
- Yu, K.; Ke, M.-Y.; Li, W.H.; Zhang, S.-Q.; Fang, X.-C. The impact of soluble dietary fibre on gastric emptying, postprandial blood glucose and insulin in patients with type 2 diabetes. Asia Pac. J. Clin. Nutr. 2014, 23, 210–218. [Google Scholar] [CrossRef]
- Jang, C.; Wada, S.; Yang, S.; Bridget, G.; Zeng, X.; Zhang, Z.; Shen, Y.; Lee, G.; Arany, Z.; Rabinowitz, D.J. The small intestine shields the liver from fructose induced steatosis. Nat. Metab. 2020, 2, 586–593. [Google Scholar] [CrossRef]
- Adyanthaya, I.; Kwon, Y.-I.; Apostolidis, E.; Shetty, K. Health benefits of apple phenolics from post-harvest stages for potential Type 2 diabetes management using in vitro models. J. Food Biochem. 2010, 34, 31–49. [Google Scholar] [CrossRef]
- Nilsson, L.H.; Hultman, E. Liver and muscle glycogen in man after glucose and fructose infusion. Scand. J. Clin. Lab. Investig. 1974, 33, 5–10. [Google Scholar] [CrossRef] [PubMed]
- Bantle, J. Clinical aspects of sucrose and fructose metabolism. Diabetes Care 1989, 12, 56–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asp, N.G.; Agardh, C.D.; Ahren, B.; Dencker, I.; Johansson, C.G.; Lundquist, I.; Nyman, M.; Sartor, G.; Schersten, B. Dietary fibre in type II diabetes. Acta Med. Scand. Suppl. 1981, 656, 47–50. [Google Scholar] [CrossRef] [PubMed]
- Bornhorst, G.M.; Chang, L.Q.; Rutherfurd, S.M.; Moughan, P.J.; Singh, R.P. Gastric emptying rate and chyme characteristics for cooked brown and white rice meals in vivo. J. Sci. Food Agric. 2013, 93, 2900–2908. [Google Scholar] [CrossRef]
- Hinninghofen, H.; Musial, F.; Kowalski, A.; Enck, P. Gastric emptying effects of dietary fiber during 8 hours at two simulated cabin altitudes. Aviat. Space Environ. Med. 2006, 77, 121–123. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (g) | Protein (g) | Fat (g) | CHO A Vial (g) | Energy (kcal) | |
|---|---|---|---|---|---|
| Rice | 147.5 | 3.1 | 0.6 | 50.0 | 223.2 |
| Apple | 150.0 | 0.3 | 0.2 | 21.9 | 80.0 |
| Total | 297.5 | 3.4 | 0.8 | 71.9 | 303.2 |
| Glucose Level | ΔCmax (mg/dL) | Tmax (min) | iAUC (mg·min/dL) |
|---|---|---|---|
| Rice-first group | 54.0 ± 5.0 | 33.0 ± 2.0 | 3666 ± 458 |
| Apple-first group | 46.2 ± 5.9 | 54.0 ± 12.7 | 3952 ± 652 |
| Insulin Level | ΔCmax (µU/dL) | Tmax (min) | iAUC (µU·min/dL) |
| Rice-first group | 61.9 ± 7.2 | 31.3 ± 4.2 | 4452 ± 878 |
| Apple-first group | 49.8 ± 8.5 | 45.0 ± 9.2 | 3669 ± 916 |
| Glucose Level | ΔCmax (mg/dL) | Tmax (min) | iAUC (mg·min/dL) |
|---|---|---|---|
| Rice-first group | 90.0 ± 10.0 | 48.3 ± 6.5 | 7739 ± 1474 |
| Apple-first group | 75.2 ± 7.2 * | 55.0 ± 9.0 | 6481 ± 1105 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Inoue, Y.; Cormanes, L.; Yoshimura, K.; Sano, A.; Hori, Y.; Suzuki, R.; Kanamoto, I. Effect of Apple Consumption on Postprandial Blood Glucose Levels in Normal Glucose Tolerance People versus Those with Impaired Glucose Tolerance. Foods 2022, 11, 1803. https://doi.org/10.3390/foods11121803
Inoue Y, Cormanes L, Yoshimura K, Sano A, Hori Y, Suzuki R, Kanamoto I. Effect of Apple Consumption on Postprandial Blood Glucose Levels in Normal Glucose Tolerance People versus Those with Impaired Glucose Tolerance. Foods. 2022; 11(12):1803. https://doi.org/10.3390/foods11121803
Chicago/Turabian StyleInoue, Yutaka, Lianne Cormanes, Kana Yoshimura, Aiko Sano, Yumiko Hori, Ryuichiro Suzuki, and Ikuo Kanamoto. 2022. "Effect of Apple Consumption on Postprandial Blood Glucose Levels in Normal Glucose Tolerance People versus Those with Impaired Glucose Tolerance" Foods 11, no. 12: 1803. https://doi.org/10.3390/foods11121803