Cone-Beam Computed Tomography for the Evaluation of Dental Pulp Chamber Volume: Implications for Clinics and Teaching

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Selection
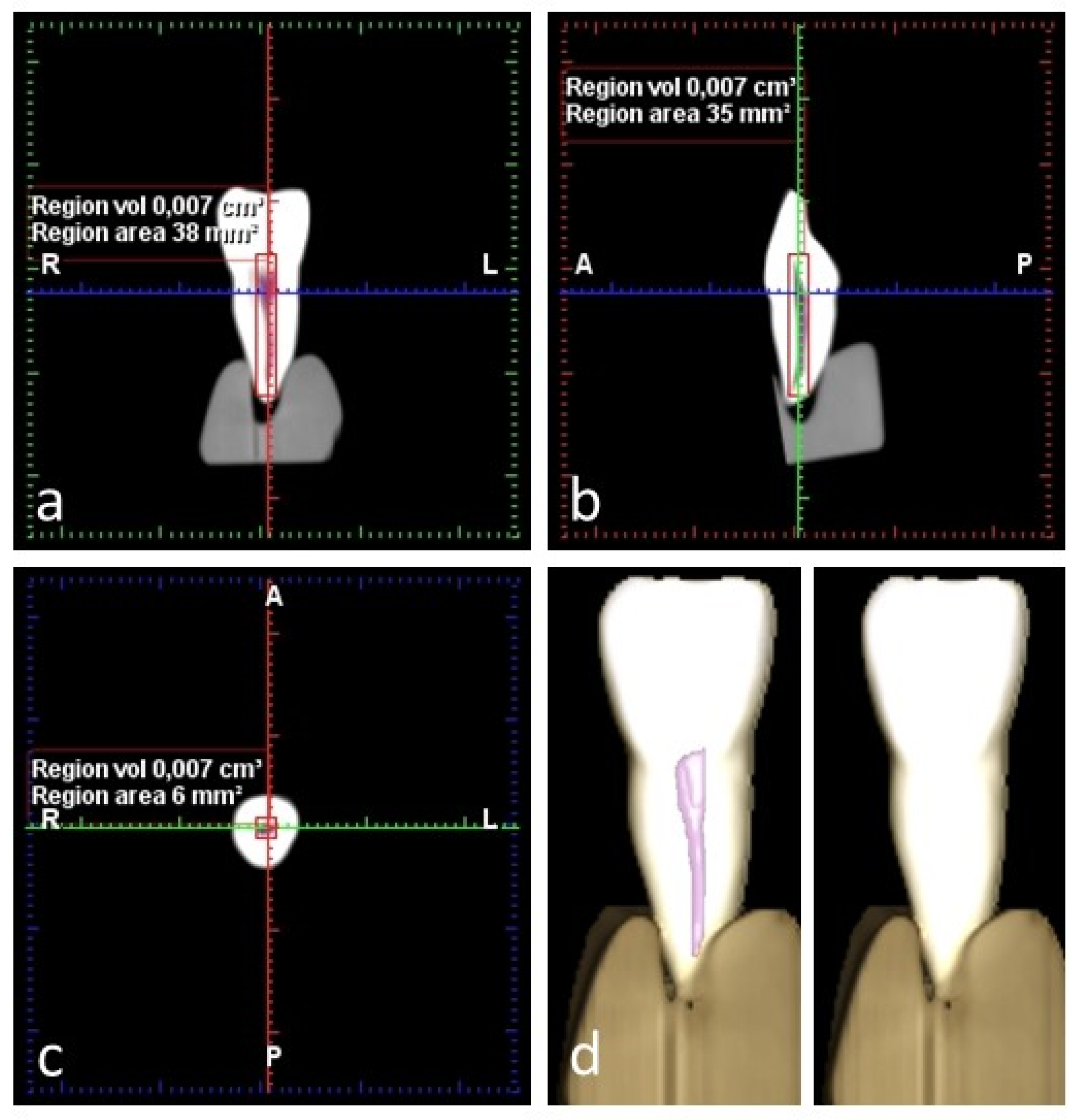
2.2. CBCT Study
2.3. Micro-CT Study
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Liu, Y.; Olszewski, R.; Alexandroni, E.S.; Enciso, R.; Xu, T.; Mah, J.K. The validity of in vivo tooth volume determinations from cone-beam computed tomography. Angle Orthod. 2010, 80, 160–166. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, R.B.; Alyassin, A.M.; Peters, D.D.; Carnes, D.L.; Lancaster, J. Microcomputed tomography: An advanced system for detailed endodontic research. J. Endod. 1995, 21, 561–568. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, J.S.; Ford, T.R.; Lynch, J.A.; Liepins, P.J.; Curtis, R.V. Micro-computed tomography: A new tool for experimental endodontology. Int. Endod. J. 1999, 32, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Park, J.W.; Lee, J.K.; Ha, B.H.; Choi, J.H.; Perinpanayagam, H. Three-dimensional analysis of maxillary first molar mesiobuccal root canal configuration and curvature using microcomputed tomography. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2009, 108, 437–442. [Google Scholar] [CrossRef] [PubMed]
- Liang, X.; Zhang, Z.; Gu, J.; Wang, Z.; Vandenberghe, B.; Jacobs, R.; Yang, J.; Ma, G.; Ling, H.; Ma, X. Comparison of micro-CT and cone beam CT on the feasibility of assessing trabecular structures in mandibular condyle. Dentomaxillofac. Radiol. 2017, 46, 20160435. [Google Scholar] [CrossRef] [PubMed]
- Michetti, J.; Maret, D.; Mallet, J.P.; Diemer, F. Validation of cone beam computed tomography as a tool to explore root canal anatomy. J. Endod. 2010, 36, 1187–1190. [Google Scholar] [CrossRef] [PubMed]
- Domark, J.D.; Hatton, J.F.; Benison, R.P.; Hildebolt, C.F. An ex vivo comparison of digital radiography and cone-beam and micro computed tomography in the detection of the number of canals in the mesiobuccal roots of maxillary molars. J. Endod. 2013, 39, 901–905. [Google Scholar] [CrossRef] [PubMed]
- Fokas, G.; Vaughn, V.M.; Scarfe, W.C.; Bornstein, M.M. Accuracy of linear measurements on CBCT images related to presurgical implant treatment planning: A systematic review. Clin. Oral Implants Res. 2018, 29, 393–415. [Google Scholar] [CrossRef] [PubMed]
- Asif, M.K.; Nambiar, P.; Mani, S.A.; Ibrahim, N.B.; Khan, I.M.; Lokman, N.B. Dental age estimation in Malaysian adults based on volumetric analysis of pulp/tooth ratio using CBCT data. Leg. Med. 2019, 36, 50–58. [Google Scholar] [CrossRef]
- Zhang, D.; Chen, J.; Lan, G.; Li, M.; An, J.; Wen, X.; Liu, L.; Deng, M. The root canal morphology in mandibular first premolars: A comparative evaluation of cone-beam computed tomography and micro-computed tomography. Clin. Oral Investig. 2017, 21, 1007–1012. [Google Scholar] [CrossRef]
- Creed, B.; Kau, C.H.; English, J.D.; Xia, J.J.; Lee, R.P. A Comparison of the Accuracy of Linear Measurements Obtained from Cone Beam Computerized Tomography Images and Digital Models. Semin. Orthod. 2011, 17, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Gulsahi, A.; Kulah, C.K.; Bakirarar, B.; Gulen, O.; Kamburoglu, K. Age estimation based on pulp/tooth volume ratio measured on cone-beam CT images. Dentomaxillofac. Radiol. 2018, 47, 20170239. [Google Scholar] [CrossRef] [PubMed]
- Ge, Z.P.; Yang, P.; Li, G.; Zhang, J.Z.; Ma, X.C. Age estimation based on pulp cavity/chamber volume of 13 types of teeth from cone beam computed tomography images. Int. J. Legal Med. 2016, 130, 1159–1167. [Google Scholar] [CrossRef] [PubMed]
- Orhan, A.I.; Orhan, K.; Ozgul, B.M.; Öz, F.T. Analysis of pulp chamber of primary maxillary second molars using 3D micro-CT system: An in vitro study. Eur. J. Paediatr. Dent. 2015, 16, 305–310. [Google Scholar] [PubMed]
- Pinchi, V.; Pradella, F.; Buti, J.; Baldinotti, C.; Focardi, M.; Norelli, G.A. A new age estimation procedure based on the 3D CBCT study of the pulp cavity and hard tissues of the teeth for forensic purposes: A pilot study. J. Forensic Leg. Med. 2015, 36, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Biuki, N.; Razi, T.; Faramarzi, M. Relationship between pulp-tooth volume ratios and chronological age in different anterior teeth on CBCT. J. Clin. Exp. Dent. 2017, 9, E688–E693. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Q.; Ge, Z.; Du, H.; Li, G. Age estimation based on 3D pulp chamber segmentation of first molars from cone-beam-computed tomography by integrated deep learning and level set. Int. J. Legal. Med. 2021, 135, 365–373. [Google Scholar] [CrossRef] [PubMed]
- Itoh, Y.; Sasaki, J.I.; Hashimoto, M.; Katata, C.; Hayashi, M.; Imazato, S. Pulp Regeneration by 3-dimensional Dental Pulp Stem Cell Constructs. J. Dent. Res. 2018, 97, 1137–1143. [Google Scholar] [CrossRef]
- Ma, Y.; Xie, L.; Yang, B.; Tian, W. Three-dimensional printing biotechnology for the regeneration of the tooth and tooth-supporting tissues. Biotechnol. Bioeng. 2019, 116, 452–468. [Google Scholar] [CrossRef]
- Hadjichristou, C.; About, I.; Koidis, P.; Bakopoulou, A. Advanced in Vitro Experimental Models for Tissue Engineering-based Reconstruction of a 3D Dentin/pulp Complex: A Literature Review. Stem Cell Rev. Rep. 2021, 17, 785–802. [Google Scholar] [CrossRef]
- Zehnder, M.S.; Connert, T.; Weiger, R.; Krastl, G.; Kühl, S. Guided endodontics: Accuracy of a novel method for guided access cavity preparation and root canal location. Int. Endod. J. 2016, 49, 966–992. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J.; Wealleans, J.; Ray, J. Endodontic applications of 3D printing. Int. Endod. J. 2018, 51, 1005–1018. [Google Scholar] [CrossRef] [PubMed]
- Höhne, C.; Schmitter, M. 3D Printed Teeth for the Preclinical Education of Dental Students. J. Dent. Educ. 2019, 83, 1100–1106. [Google Scholar] [CrossRef] [PubMed]
- Hanafi, A.; Donnermeyer, D.; Schäfer, E.; Bürklein, S. Perception of a modular 3D print model in undergraduate endodontic education. Int. Endod. J. 2020, 53, 1007–1016. [Google Scholar] [CrossRef] [PubMed]
- Celikten, B.; Jacobs, R.; deFaria Vasconcelos, K.; Huang, Y.; Nicolielo, L.F.P.; Orhan, K. Assessment of Volumetric Distortion Artifact in Filled Root Canals Using Different Cone-beam Computed Tomographic Devices. J. Endod. 2017, 43, 1517–1521. [Google Scholar] [CrossRef] [PubMed]
- Maddalone, M.; Citterio, C.; Pellegatta, A.; Gagliani, M.; Karanxha, L.; Del Fabbro, M. Cone-beam computed tomography accuracy in pulp chamber size evaluation: An ex vivo study. Aust. Endod. J. 2020, 46, 88–93. [Google Scholar] [CrossRef] [PubMed]
- Grande, N.M.; Plotino, G.; Pecci, R.; Bedini, R.; Pameijer, C.H.; Somma, F. Micro-computerized tomographic analysis of radicular and canal morphology of premolars with long oval canals. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008, 106, E70–E76. [Google Scholar] [CrossRef]
- Puleio, F.; Lizio, A.S.; Coppini, V.; Lo Giudice, R.; Lo Giudice, G. CBCT-Based Assessment of Vapor Lock Effects on Endodontic Disinfection. Appl. Sci. 2023, 13, 9542. [Google Scholar] [CrossRef]
- Porto, L.V.; Celestino da Silva Neto, J.; Anjos Pontual, A.D.; Catunda, R.Q. Evaluation of volumetric changes of teeth in a Brazilian population by using cone beam computed tomography. J. Forensic Leg. Med. 2015, 36, 4–9. [Google Scholar] [CrossRef]
- Maret, D.; Telmon, N.; Peters, O.A.; Lepage, B.; Treil, J.; Inglèse, J.M.; Peyre, A.; Kahn, J.L.; Sixou, M. Effect of voxel size on the accuracy of 3D reconstructions with cone beam CT. Dentomaxillofac. Radiol. 2012, 41, 649–655. [Google Scholar] [CrossRef]
- Chen, B.; Szabo, D.; Shen, Y.; Zhang, D.; Li, X.; Ma, J.; Haapasalo, M. Removal of calcifications from distal canals of mandibular molars by a non-instrumentational cleaning system: A micro-CT study. Aust. Endod. J. 2020, 46, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.; Brown, J.; Pimentel, T.; Kelly, R.D.; Abella, F.; Durack, C. Cone beam computed tomography in Endodontics—A review of the literature. Int. Endod. J. 2019, 52, 1138–1152. [Google Scholar] [CrossRef] [PubMed]
- Johnsen, G.F.; Sundnes, J.; Wengenroth, J.; Haugen, H.J. Methodology for morphometric analysis of modern human contralateral premolars. J. Comput. Assist. Tomogr. 2016, 40, 617–625. [Google Scholar] [CrossRef] [PubMed]
- Møller, L.; Wenzel, A.; Wegge-Larsen, A.M.; Ding, M.; Væth, M.; Hirsch, E.; Kirkevang, L.L. Comparison of images from digital intraoral receptors and cone beam computed tomography scanning for detection of voids in root canal fillings: An in vitro study using micro-computed tomography as validation. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2013, 115, 810–818. [Google Scholar] [CrossRef] [PubMed]
- Van der Meer, W.J.; Vissink, A.; Ng, Y.L.; Gulabivala, K. 3D Computer aided treatment planning in endodontics. J. Dent. 2016, 45, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Rosen, E.; Goldberger, T.; Beitlitum, I.; Littner, D.; Tsesis, I. Diagnosis Efficacy of Cone-Beam Computed Tomography in Endodontics—A Systematic Review of High-Level-Evidence Studies. Appl. Sci. 2022, 12, 938. [Google Scholar] [CrossRef]
- Ahmed, H.M.A.; Ibrahim, N.; Mohamad, N.S.; Nambiar, P.; Muhammad, R.F.; Yusoff, M.; Dummer, P.M.H. Application of a new system for classifying root and canal anatomy in studies involving micro-computed tomography and cone beam computed tomography: Explanation and elaboration. Int. Endod. J. 2021, 54, 1056–1082. [Google Scholar] [CrossRef] [PubMed]
- Merdietio Boedi, R.; Shepherd, S.; Mânica, S.; Franco, A. CBCT in dental age estimation: A systematic review and meta analysis. Dentomaxillofac. Radiol. 2022, 51, 20210335. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.G.; Malek, M.; Sigurdsson, A.; Lin, L.M.; Kahler, B. Regenerative endodontics: A comprehensive review. Int. Endod. J. 2018, 51, 1367–1388. [Google Scholar] [CrossRef]
- Höhne, C.; Schwarzbauer, R.; Schmitter, M. Introduction of a new teaching concept for crown preparation with 3D printed teeth. Eur. J. Dent. Educ. 2020, 24, 526–534. [Google Scholar] [CrossRef]
- Pouhaër, M.; Picart, G.; Baya, D.; Michelutti, P.; Dautel, A.; Pérard, M.; Le Clerc, J. Design of 3D-printed macro-models for undergraduates’ preclinical practice of endodontic access cavities. Eur. J. Dent. Educ. 2022, 26, 347–353. [Google Scholar] [CrossRef] [PubMed]
- Maret, D.; Peters, O.A.; Galibourg ADumoncel, J.; Esclassan, R.; Kahn, J.L.; Sixou, M.; Telmon, N. Comparison of the accuracy of 3-dimensional cone-beam computed tomography and micro-computed tomography reconstructions by using different voxel sizes. J. Endod. 2014, 40, 1321–1326. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Paired Differences | ||||||
|---|---|---|---|---|---|---|
| 95% Confidence Interval of the Difference | ||||||
| Mean | SD | SEM | Lower | Upper | p | |
| A. Differences in operator 1 and operator 2 measurements | ||||||
| Observer 1 | ||||||
| CBCT 1st | ||||||
| read-CBCT | −0.200 | 1.215 | 0.222 | −0.654 | 0.254 | 0.375 |
| 2nd read | ||||||
| Observer 2 | ||||||
| CBCT 1st | ||||||
| read-CBCT | −0.200 | 0.894 | 0.222 | −0.619 | 0.219 | 0.074 |
| 2nd read | ||||||
| B. Differences in operator 1 and operator 2 measurements | ||||||
| Observer 1 | ||||||
| −0.350 | 0.828 | 0.185 | −0.737 | 0.037 | 0.074 | |
| Observer 2 | ||||||
| C. Comparison of pulp volume measurements obtained from CBCT and micro-CT | ||||||
| CBCT | ||||||
| −0.108 | 0.674 | 0.164 | −0.239 | 0.454 | 0.50 | |
| micro-CT | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Llacer-Martínez, M.; Martín-Biedma, B.; Sanz, M.T.; Aura-Tormos, J.I.; Fos-Galve, P.; Fernández-Muñiz, Z.; Vega, J.A.; Jovani-Sancho, M. Cone-Beam Computed Tomography for the Evaluation of Dental Pulp Chamber Volume: Implications for Clinics and Teaching. Dent. J. 2024, 12, 95. https://doi.org/10.3390/dj12040095
Llacer-Martínez M, Martín-Biedma B, Sanz MT, Aura-Tormos JI, Fos-Galve P, Fernández-Muñiz Z, Vega JA, Jovani-Sancho M. Cone-Beam Computed Tomography for the Evaluation of Dental Pulp Chamber Volume: Implications for Clinics and Teaching. Dentistry Journal. 2024; 12(4):95. https://doi.org/10.3390/dj12040095
Chicago/Turabian StyleLlacer-Martínez, Maria, Benjamín Martín-Biedma, María T. Sanz, Juan I. Aura-Tormos, Pablo Fos-Galve, Zulima Fernández-Muñiz, José A. Vega, and Mar Jovani-Sancho. 2024. "Cone-Beam Computed Tomography for the Evaluation of Dental Pulp Chamber Volume: Implications for Clinics and Teaching" Dentistry Journal 12, no. 4: 95. https://doi.org/10.3390/dj12040095