
The Use of CAD/CAM Technology in Mandibular Canine Disimpaction: A Case Report

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case Report
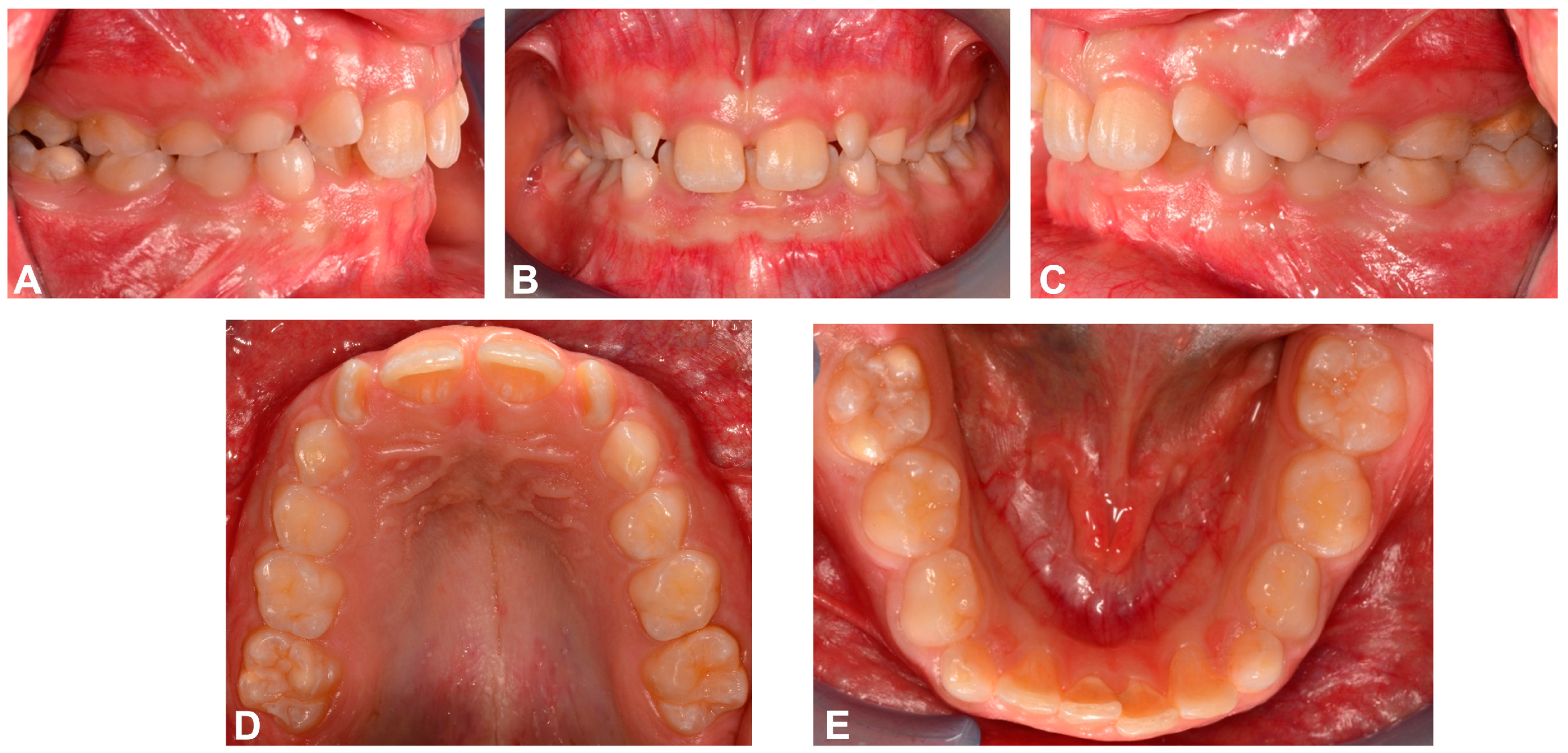
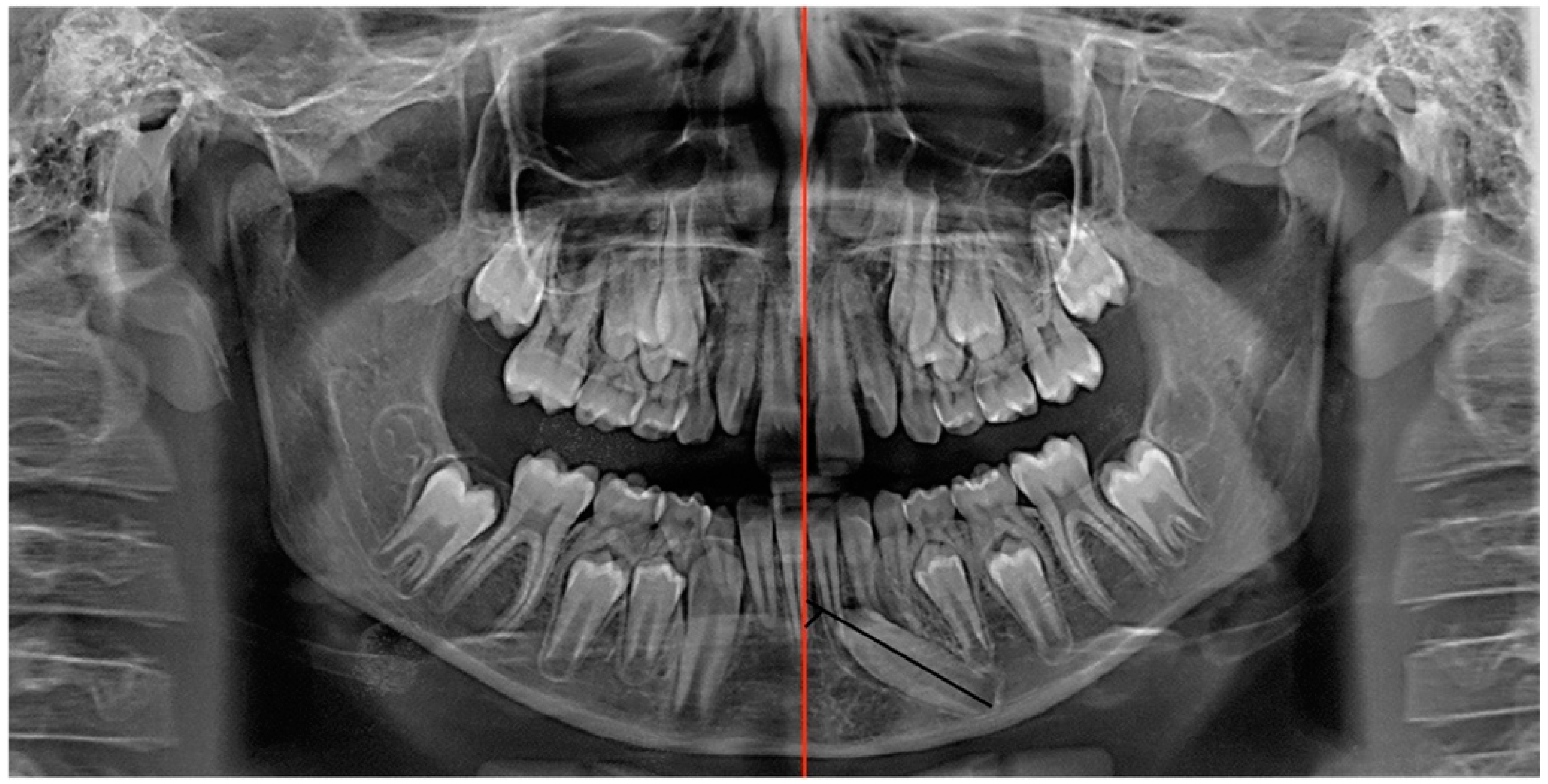
2.1. Diagnosis and Aetiology
2.2. Treatment Objectives
2.3. Treatment Alternatives
2.4. Treatment Progress
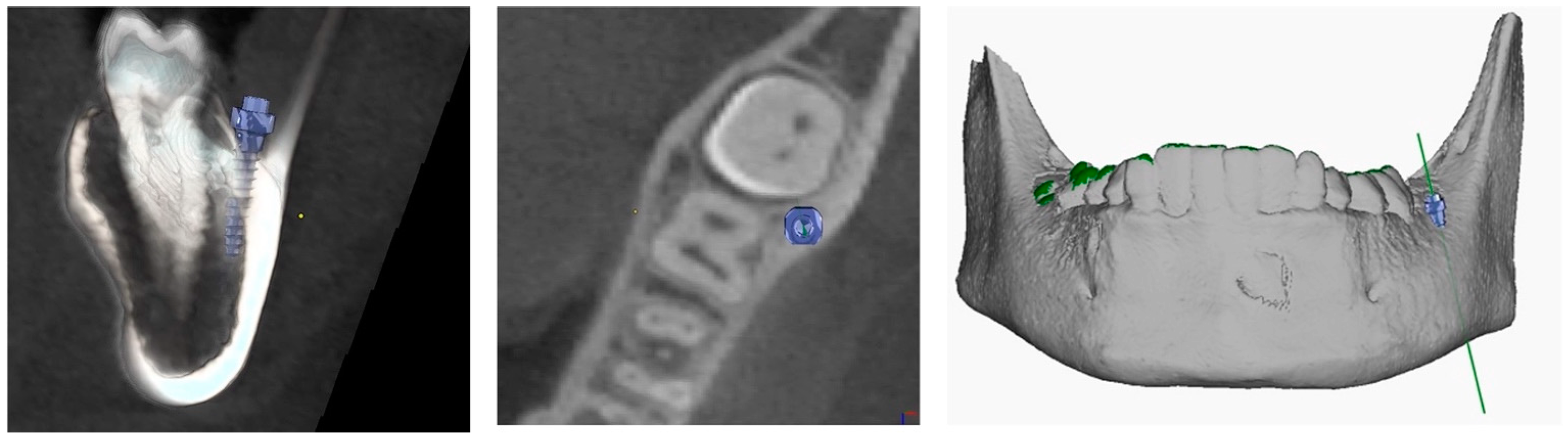
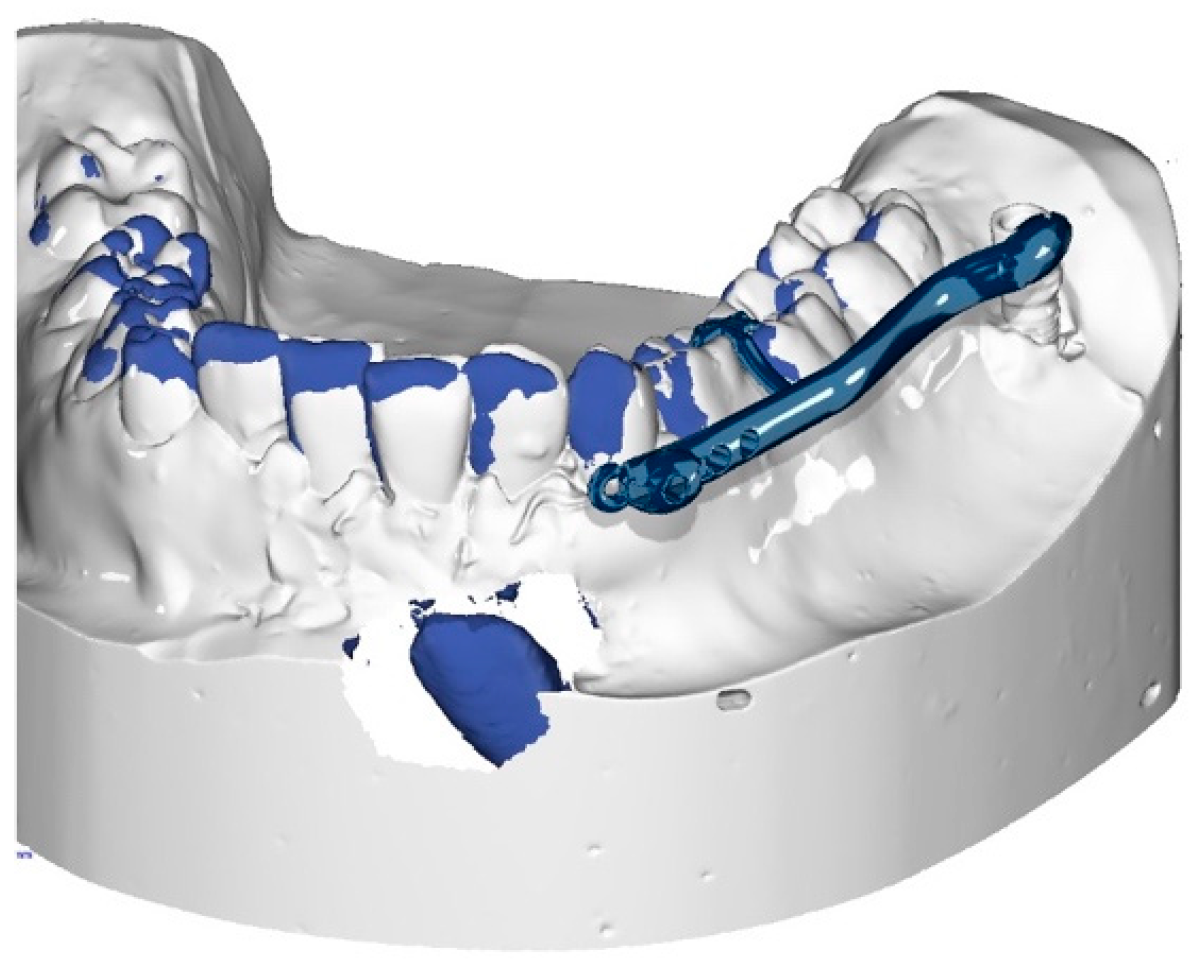
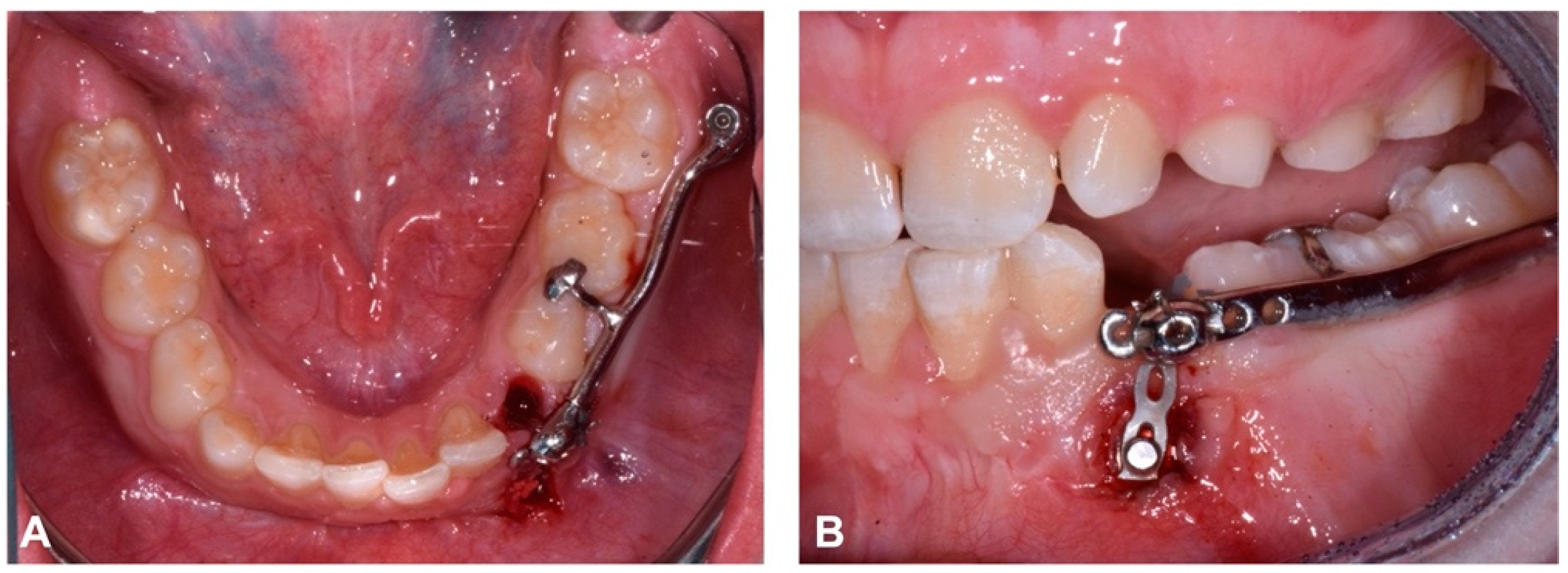
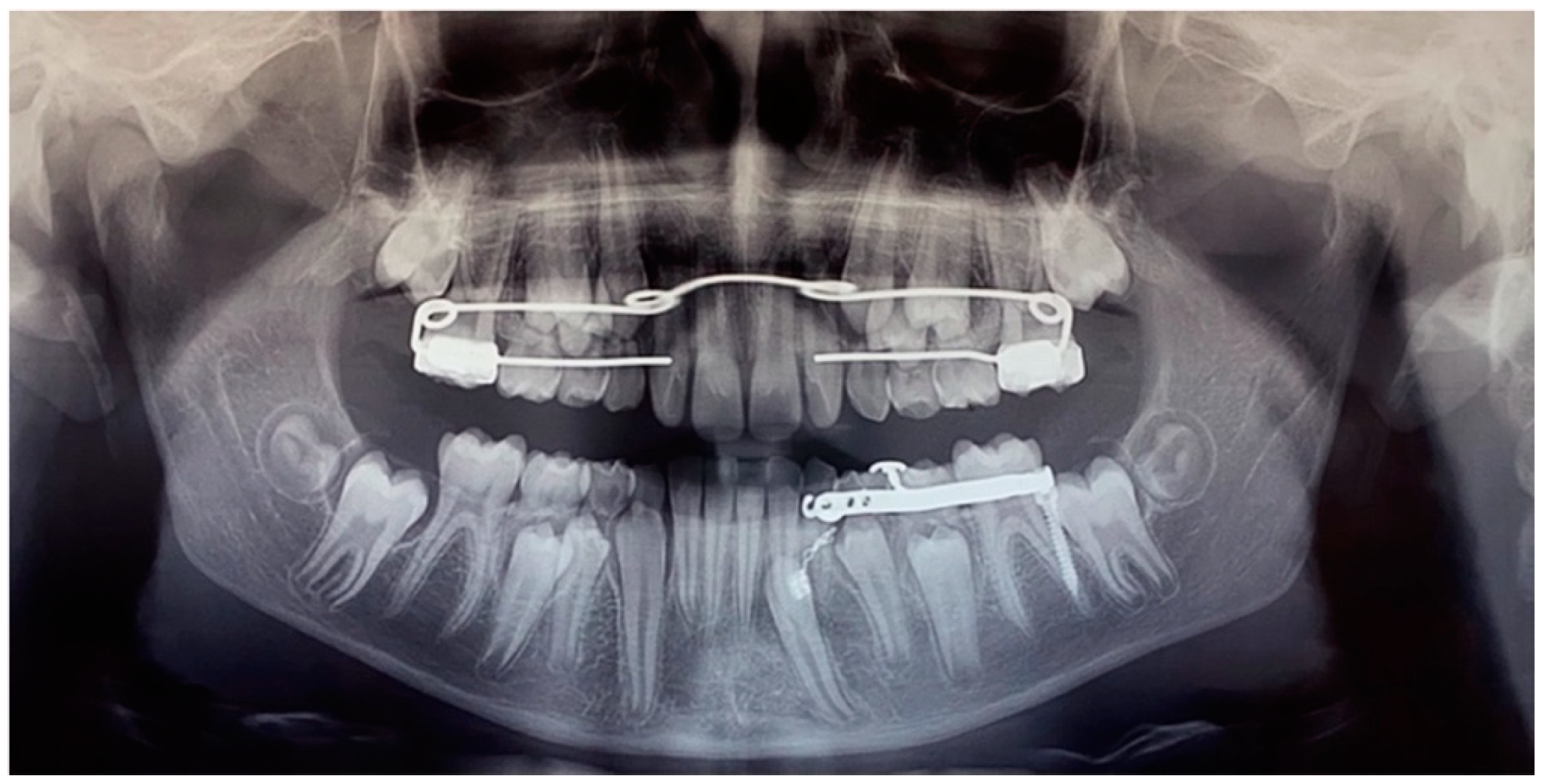
2.4.1. Surgery
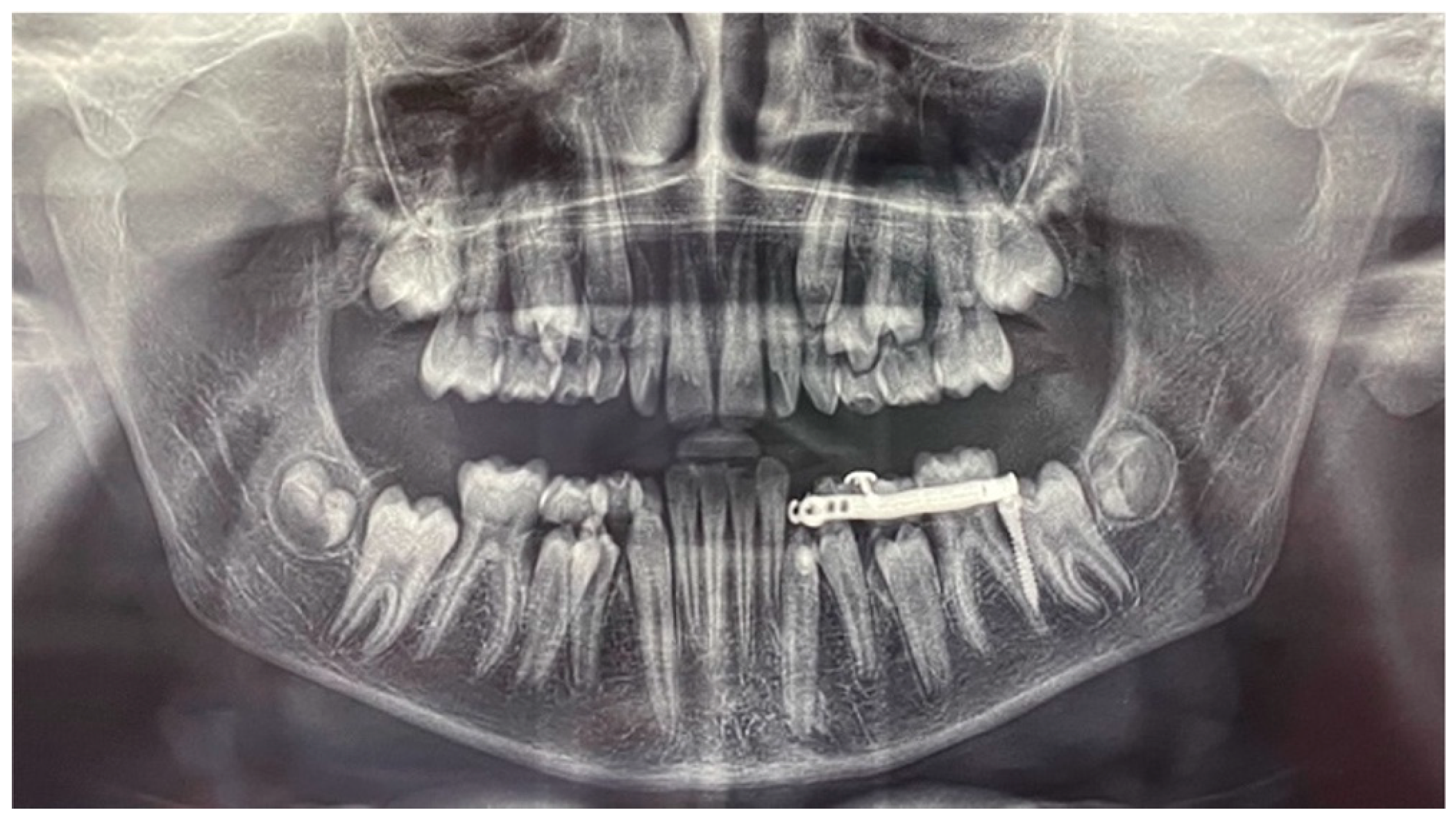
2.4.2. Orthodontic Traction
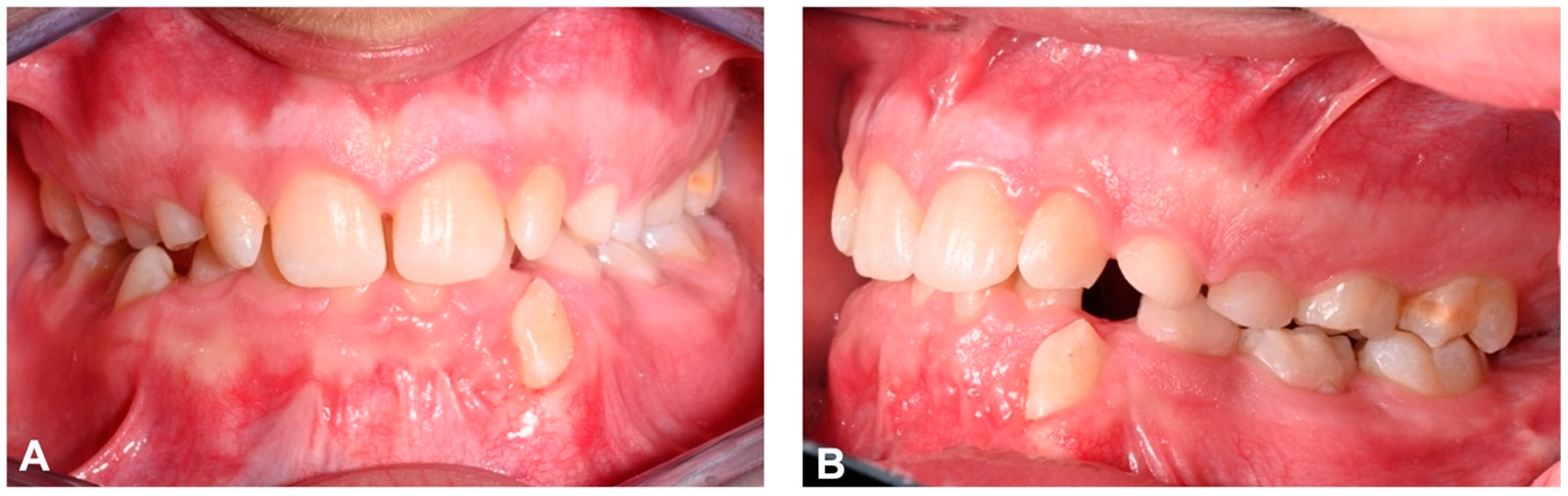
2.5. Treatment Results
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ngan, P.; Hornbrook, R.; Weaver, B. Early timely management of ectopically erupting maxillary canines. Semin. Orthod. 2005, 11, 152–163. [Google Scholar] [CrossRef]
- Sathyanarayana, H.P.; Nucci, L.; d’Apuzzo, F.; Perillo, L.; Padmanabhan, S.; Grassia, V. Prevalence, etiology, clinical features and management associated with impacted and transmigrated mandibular canines: A systematic review. BMC Oral Health 2023, 23, 975. [Google Scholar] [CrossRef] [PubMed]
- Dalessandri, D.; Parrini, S.; Rubiano, R.; Gallone, D.; Migliorati, M. Impacted and transmigrant mandibular canines incidence, aetiology, and treatment: A systematic review. Eur. J. Orthod. 2017, 39, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Bertl, M.H.; Frey, C.; Bertl, K.; Giannis, K.; Gahleitner, A.; Strbac, G.D. Impacted and transmigrated mandibular canines: An analysis of 3D radiographic imaging data. Clin. Oral Investig. 2018, 22, 2389–2399. [Google Scholar] [CrossRef] [PubMed]
- Bhullar, M.K.; Aggarwal, I.; Verma, R.; Uppal, A.S. Mandibular canine transmigration: Report of three cases and literature review. J. Int. Soc. Prev. Commun. Dent. 2017, 7, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Aras, M.H.; Halicioğlu, K.; Yavuz, M.S.; Çağlaroğlu, M. Evaluation of surgical-orthodontic treatments on impacted mandibular canines. Med. Oral Patol. Oral Cir. Bucal. 2011, 16, e925–e928. [Google Scholar] [CrossRef]
- Agastra, E.; Saettone, M.; Parrini, S.; Cugliari, G.; Deregibus, A.; Castroflorio, T. Impacted Permanent Mandibular Canines: Epidemiological Evaluation. J. Clin. Med. 2023, 12, 5375. [Google Scholar] [CrossRef]
- Mejía-Milian, M.; Arriola-Guillén, L.E.; Aliaga-Del Castillo, A.; Rodríguez-Cárdenas, Y.A.; Ruíz-Mora, G.A. Three-dimensional evaluation of mandibular canine impaction characteristics and their relationship with lower incisor root morphometry. J. Clin. Exp. Dent. 2022, 14, e791–e802. [Google Scholar] [CrossRef]
- Sharma, G.; Nagpal, A. A Study of Transmigrated Canine in an Indian Population. Int. Sch. Res. Not. 2014, 756516. [Google Scholar] [CrossRef]
- Stabryła, J.; Plakwicz, P.; Kukuła, K.; Zadurska, M.; Czochrowska, E.M. Comparisons of different treatment methods and their outcomes for impacted maxillary and mandibular canines: A retrospective study. J. Am. Dent. Assoc. 2021, 152, 919–926. [Google Scholar] [CrossRef]
- Buyukkurt, M.C.; Aras, M.H.; Caglaroglu, M.; Gungormus, M. Transmigrant mandibular canines. J. Oral Maxillofac. Surg. 2007, 65, 2025–2029. [Google Scholar] [CrossRef] [PubMed]
- Joshi, M.R. Transmigrant Mandibular Canines: A record of 28 Cases and a Retrospective Review of the Literature. Angle Orthod. 2001, 71, 12–22. [Google Scholar] [PubMed]
- Ferguson, J.W. Management of the unerupted maxillary canine. Br. Dent. J. 1990, 169, 113–114. [Google Scholar] [CrossRef] [PubMed]
- Naoumova, J.; Kurol, J.; Kjellberg, H. Extraction of the deciduous canine as an interceptive treatment in children with palatal displaced canines—Part I: Shall we extract the deciduous canine or not? Eur. J. Orthod. 2015, 37, 209–218. [Google Scholar] [CrossRef]
- Kim, J.H.; Park, Y.C. Evaluation of mandibular cortical bone thickness for placement of temporary anchorage devices (TADs). Korean J. Orthod. 2012, 42, 110–117. [Google Scholar] [CrossRef]
- Park, H.S.; Lee, Y.J.; Jeong, S.H.; Kwon, T.G. Density of the alveolar and basal bones of the maxilla and the mandible. Am. J. Orthod. Dentofac. Orthop. 2008, 133, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Plaza, S.P. Orthodontic traction of a transmigrated mandibular canine using mini-implant: A case report and review. J. Orthod. 2016, 43, 314–321. [Google Scholar] [CrossRef]
- Sinko, K.; Nemec, S.; Seemann, R.; Eder-Czembirek, C. Clinical Management of Impacted and Transmigrated Lower Canines. J. Oral Maxillofac. Surg. 2016, 74, 2142.e1–2142.e16. [Google Scholar] [CrossRef]
- Cassetta, M.; Brandetti, G.; Altieri, F. Are the Insertion Torque Value and Implant Stability Quotient Correlated, and If So, Can Insertion Torque Values Predict Secondary Implant Stability? A Prospective Parallel Cohort Study. Int. J. Oral Maxillofac. Implant. 2022, 37, 135–142. [Google Scholar] [CrossRef]
- McDonald, F.; Yap, W.L. The surgical exposure and application of direct traction of unerupted teeth. Am. J. Orthod. 1986, 89, 331–340. [Google Scholar] [CrossRef]
- Ciavarella, D.; Maci, M.; Fanelli, C.; Lorusso, M.; Laurenziello, M.; Lo Muzio, L.; Caroprese, M.; Cazzolla, A.P.; Tepedino, M. Treatment of Mandibular Impacted Canine in a Patient with Class II Division 1 Malocclusion with “Reverse Pin”: A Case Report. Medicina 2023, 59, 1774. [Google Scholar] [CrossRef]
- Ruíz-Mora, G.A.; Arriola-Guillén, L.E.; Aliaga-Del Castillo, A.; Rodríguez-Cárdenas, Y.A.; Dutra, V.; Mejía-Milian, M. Conservative Treatment of Bilateral Impacted Mandibular Canines Traction. Case Rep. Dent. 2023, 2023, 6943221. [Google Scholar] [CrossRef]
- Montasser, M.A.; Scribante, A. Root Injury During Interradicular Insertion is the most Common Complication Associated with Orthodontic Miniscrews. J. Evid. Based Dent. Pract. 2022, 22, 101688. [Google Scholar] [CrossRef] [PubMed]
- Moeini, N.; Sabri, H.; Galindo-Fernandez, P.; Mirmohamadsadeghi, H.; Valian, N.K. Periodontal status following orthodontic mini-screw insertion: A prospective clinical split-mouth study. Clin. Exp. Dent. Res. 2023, 9, 596–605. [Google Scholar] [CrossRef] [PubMed]
- Heravi, F.; Shafaee, H.; Forouzanfar, A.; Zarch, S.H.; Merati, M. Forced eruption of palatally impacted canines using bracket-head miniscrews. J. Clin. Orthod. 2014, 48, 576–580. [Google Scholar] [PubMed]
- Guarnieri, R.; Grenga, C.; Altieri, F.; Rocchetti, F.; Barbato, E.; Cassetta, M. Can computer-guided surgery help orthodontics in miniscrew insertion and corticotomies? A narrative review. Front. Oral Health 2023, 4, 1196813. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, E.Y.; Suzuki, B. Accuracy of miniscrew implant placement with a 3-dimensional surgical guide. J. Oral Maxillofac. Surg. 2008, 66, 1245–1252. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Riofrío, D.; Viñas, M.J.; Ustrell-Torrent, J.M. CBCT and CAD-CAM technology to design a minimally invasive maxillary expander. BMC Oral Health 2020, 20, 303. [Google Scholar] [CrossRef]














Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Germanò, F.; Guarnieri, R.; Mezio, M.; Barbato, E.; Cassetta, M. The Use of CAD/CAM Technology in Mandibular Canine Disimpaction: A Case Report. Dent. J. 2024, 12, 79. https://doi.org/10.3390/dj12030079
Germanò F, Guarnieri R, Mezio M, Barbato E, Cassetta M. The Use of CAD/CAM Technology in Mandibular Canine Disimpaction: A Case Report. Dentistry Journal. 2024; 12(3):79. https://doi.org/10.3390/dj12030079
Chicago/Turabian StyleGermanò, Francesca, Rosanna Guarnieri, Martina Mezio, Ersilia Barbato, and Michele Cassetta. 2024. "The Use of CAD/CAM Technology in Mandibular Canine Disimpaction: A Case Report" Dentistry Journal 12, no. 3: 79. https://doi.org/10.3390/dj12030079