
Multilevel Modeling Analysis of Odontogenic Risk Factors and Nasal Septum Deviation Associated with Maxillary Sinus Mucosal Thickening: A Cone-Beam Computed Tomography Study
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. CBCT Scanning Procedure
2.3. Statistical Analysis
3. Results
Statistical Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kuligowski, P.; Jaroń, A.; Preuss, O.; Gabrysz-Trybek, E.; Bladowska, J.; Trybek, G. Association between Odontogenic and Maxillary Sinus Conditions: A Retrospective Cone-Beam Computed Tomographic Study. J. Clin. Med. 2021, 10, 2849. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.-F.; Brigitta, X.L.; Wang, Y.-J.; Dai, J.-S.; Ren, Y.-Y.; Zhang, Y.; Li, W.; Wang, N.-Y. Clinical Characteristics of Patients with Odontogenic Sinusitis Underwent Endoscopic Sinus Surgery. Zhonghua er bi yan hou tou Jing wai ke za zhi Chin. J. Otorhinolaryngol. Head Neck Surg. 2021, 56, 848–853. [Google Scholar]
- Sato, K. Pathology of Recent Odontogenic Maxillary Sinusitis and the Usefulness of Endoscopic Sinus Surgery. Nippon Jibiinkoka Gakkai Kaiho 2001, 104, 715–720. [Google Scholar] [CrossRef] [PubMed]
- Peñarrocha-Oltra, S.; Soto-Peñaloza, D.; Bagan-Debon, L.; Bagán-sebastián, J.; Peñarrocha-Oltra, D. Association between Maxillary Sinus Pathology and Odontogenic Lesions in Patients Evaluated by Cone Beam Computed Tomography. A Systematic Review and Meta-Analysis. Med. Oral Patol. Oral Cir. Bucal 2019, 25, e34–e48. [Google Scholar] [CrossRef] [PubMed]
- Whyte, A.; Boeddinghaus, R. The Maxillary Sinus: Physiology, Development and Imaging Anatomy. Dentomaxillofac. Radiol. 2019, 48, 20190205. [Google Scholar] [CrossRef]
- Vitali, F.C.; Santos, P.; Massignan, C.; Maia, L.; Cardoso, M.; Teixeira, C. Global Prevalence of Maxillary Sinusitis of Odontogenic Origin and Associated Factors: A Systematic Review and Meta-Analysis. J. Endod. 2023, 49, 369–381. [Google Scholar] [CrossRef] [PubMed]
- Turfe, Z.; Ahmad, A.; Peterson, E.I.; Craig, J.R. Odontogenic Sinusitis Is a Common Cause of Unilateral Sinus Disease with Maxillary Sinus Opacification. In International Forum of Allergy & Rhinology; Wiley Online Library: Hoboken, NJ, USA, 2019; Volume 9, pp. 1515–1520. [Google Scholar]
- Cymerman, J.J.; Cymerman, D.H.; O’Dwyer, R.S. Evaluation of Odontogenic Maxillary Sinusitis Using Cone-Beam Computed Tomography: Three Case Reports. J. Endod. 2011, 37, 1465–1469. [Google Scholar] [CrossRef]
- Nurchis, M.C.; Pascucci, D.; Lopez, M.A.; Moffa, A.; Passarelli, P.C.; Bressi, F.; Casale, M.; Damiani, G. Epidemiology of Odontogenic Sinusitis: An Old, Underestimated Disease, Even Today. A Narrative Literature Review. J. Biol. Regul. Homeost. Agents 2020, 34 (Suppl. 3), 195–200. [Google Scholar]
- Hoskison, E.; Daniel, M.; Rowson, J.E.; Jones, N.S. Evidence of an Increase in the Incidence of Odontogenic Sinusitis over the Last Decade in the UK. J. Laryngol. Otol. 2012, 126, 43–46. [Google Scholar] [CrossRef]
- Bogaerts, P.; Hanssens, J.F.; Siquet, J.P. Healing of Maxillary Sinusitis of Odontogenic Origin Following Conservative Endodontic Retreatment. Acta Otorhinolaryngol. Belg. 2003, 57, 91–97. [Google Scholar]
- Bajoria, A.; Sarkar, S.; Sinha, P. Evaluation of Odontogenic Maxillary Sinusitis with Cone Beam Computed Tomography: A Retrospective Study with Review of Literature. J. Int. Soc. Prev. Community Dent. 2019, 9, 194–204. [Google Scholar] [CrossRef] [PubMed]
- Aksoy, U.; Orhan, K. Association between Odontogenic Conditions and Maxillary Sinus Mucosal Thickening: A Retrospective CBCT Study. Clin. Oral Investig. 2019, 23, 123–131. [Google Scholar] [CrossRef] [PubMed]
- Ren, S.; Zhao, H.; Liu, J.; Wang, Q.; Pan, Y. Significance of Maxillary Sinus Mucosal Thickening in Patients with Periodontal Disease. Int. Dent. J. 2015, 65, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Aguori, E.A.B.; Ersan, N.; Dölekoğlu, Z.S.; Ilgüy, D. Proximity of Healthy Posterior Teeth to the Maxillary Sinus Floor in Relation to Mucosal Thickening: A CBCT Study. Oral Radiol. 2022, 39, 536–543. [Google Scholar] [CrossRef]
- Jouhar, R.; Alkhames, H.M.; Ahmed, M.A.; Almadeh, N.M.; Faheemuddin, M.; Umer, M.F. CBCT Evaluation of Periapical Pathologies in Maxillary Posterior Teeth and Their Relationship with Maxillary Sinus Mucosal Thickening. Healthcare 2023, 11, 787. [Google Scholar] [CrossRef] [PubMed]
- Althobiti, G.A.; Alzaidi, T.A.; Almingash, J.M.; Alobaida, R.M.; ALYahya, R.E.; Binthunayyan, S.N. Association between Periapical Odontogenic Lesions and Maxillary Sinus Mucosal Thickening: A Retrospective Computed Tomography Analysis. Saudi Endod. J. 2024, 14, 10–18. [Google Scholar]
- Şendişçi, R.; Sancar, B.S.; Ekinci, A.; Yilmaz, S.G. Evaluation of the Relationship between Maxillary Sinus Pathologies and Odontogenic Factors by Cone Beam Computed Tomography. Akdeniz Diş Hekim. Derg. 2023, 2, 61–68. [Google Scholar]
- Kaimal, V.G.; Patil, B. Evaluation of Association between Maxillary Posterior Teeth Periapical Pathologies and Maxillary Sinus Mucosal Changes—A Cone-Beam Computed Tomography (CBCT) Study. Indian J. Radiol. Imaging 2023. [Google Scholar] [CrossRef]
- Shanbhag, S.; Karnik, P.; Shirke, P.; Shanbhag, V. Association between Periapical Lesions and Maxillary Sinus Mucosal Thickening: A Retrospective Cone-Beam Computed Tomographic Study. J. Endod. 2013, 39, 853–857. [Google Scholar] [CrossRef]
- Troeltzsch, M. Risk Factors and Significance of Residual Disease after Surgical Treatment of Odontogenic Sinusitis. Int. J. Oral Maxillofac. Surg. 2024, 52, 143. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement. Epidemiology 2007, 18, 800–804. [Google Scholar] [CrossRef] [PubMed]
- Sharan, A.; Madjar, D. Correlation between Maxillary Sinus Floor Topography and Related Root Position of Posterior Teeth Using Panoramic and Cross-Sectional Computed Tomography Imaging. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2006, 102, 375–381. [Google Scholar] [CrossRef]
- Engebretson, S.P.; Lamster, I.B.; Elkind, M.S.V.; Rundek, T.; Serman, N.J.; Demmer, R.T.; Sacco, R.L.; Papapanou, P.N.; Desvarieux, M. Radiographic Measures of Chronic Periodontitis and Carotid Artery Plaque. Stroke 2005, 36, 561–566. [Google Scholar] [CrossRef] [PubMed]
- Mladina, R.; Čujić, E.; Šubarić, M.; Vuković, K. Nasal Septal Deformities in Ear, Nose, and Throat Patients: An International Study. Am. J. Otolaryngol. 2008, 29, 75–82. [Google Scholar] [CrossRef]
- Lu, Y.; Liu, Z.; Zhang, L.; Zhou, X.; Zheng, Q.; Duan, X.; Zheng, G.; Wang, H.; Huang, D. Associations between Maxillary Sinus Mucosal Thickening and Apical Periodontitis Using Cone-Beam Computed Tomography Scanning: A Retrospective Study. J. Endod. 2012, 38, 1069–1074. [Google Scholar] [CrossRef]
- Sheikhi, M.; Pozve, N.J.; Khorrami, L. Using Cone Beam Computed Tomography to Detect the Relationship between the Periodontal Bone Loss and Mucosal Thickening of the Maxillary Sinus. Dent. Res. J. 2014, 11, 495. [Google Scholar]
- Zadsirjan, S.; Sheikhi, M.; Dakhilalian, A.; Feli, M. Association of Inflammatory Periapical Lesions with Maxillary Sinus Abnormalities: A Retrospective Cone-Beam Computed Tomography Study. J. Dent. 2021, 22, 273–280. [Google Scholar] [CrossRef]
- Goller-Bulut, D.; Sekerci, A.; Köse, E.; Şişman, Y. Cone Beam Computed Tomographic Analysis of Maxillary Premolars and Molars to Detect the Relationship between Periapical and Marginal Bone Loss and Mucosal Thickness of Maxillary Sinus. Med. Oral Patol. Oral Cir. Bucal 2015, 20, e572–e579. [Google Scholar] [CrossRef]
- Boutsioukis, C.; Psimma, Z.; Van der Sluis, L.W.M. Factors Affecting Irrigant Extrusion during Root Canal Irrigation: A Systematic Review. Int. Endod. J. 2013, 46, 599–618. [Google Scholar] [CrossRef]
- Hauman, C.H.J.; Chandler, N.P.; Tong, D.C. Endodontic Implications of the Maxillary Sinus: A Review. Int. Endod. J. 2002, 35, 127–141. [Google Scholar] [CrossRef]
- Engström, H.; Chamberlain, D.; Kiger, R.; Egelberg, J. Radiographic Evaluation of the Effect of Initial Periodontal Therapy on Thickness of the Maxillary Sinus Mucosa. J. Periodontol. 1988, 59, 604–608. [Google Scholar] [CrossRef] [PubMed]
- Matsuda, H.; Borzabadi-Farahani, A.; Le, B.T. Three-Dimensional Alveolar Bone Anatomy of the Maxillary First Molars: A Cone-Beam Computed Tomography Study with Implications for Immediate Implant Placement. Implant Dent. 2016, 25, 367–372. [Google Scholar] [CrossRef]
- Fry, R.R.; Patidar, D.C.; Goyal, S.; Malhotra, A. Proximity of Maxillary Posterior Teeth Roots to Maxillary Sinus and Adjacent Structures Using Denta Scan®. Indian J. Dent. 2016, 7, 126. [Google Scholar] [CrossRef] [PubMed]
- Didilescu, A.; Rusu, M.; Sandulescu, M.; Georgescu, C.; Ciuluvica, R. Morphometric Analysis of the Relationships between the Maxillary First Molar and Maxillary Sinus Floor. Open J. Stomatol. 2012, 2, 25726. [Google Scholar] [CrossRef]
- Maillet, M.; Bowles, W.R.; McClanahan, S.L.; John, M.T.; Ahmad, M. Cone-Beam Computed Tomography Evaluation of Maxillary Sinusitis. J. Endod. 2011, 37, 753–757. [Google Scholar] [CrossRef]
- Wehrbein, H.; Diedrich, P. The Initial Morphological State in the Basally Pneumatized Maxillary Sinus—A Radiological-Histological Study in Man. Fortschr. Kieferorthop. 1992, 53, 254–262. [Google Scholar] [CrossRef]
- Köse, E.; Canger, E.M.; Göller Bulut, D. Cone Beam Computed Tomographic Analysis of Paranasal Variations, Osteomeatal Complex Disease, Odontogenic Lesion and Their Effect on Maxillary Sinus. Meandros Med. Dent. J. 2018, 19, 310–316. [Google Scholar] [CrossRef]
- Zhang, B.; Wei, Y.; Cao, J.; Xu, T.; Zhen, M.; Yang, G.; Chung, K.; Hu, W. Association between the Dimensions of the Maxillary Sinus Membrane and Molar Periodontal Status: A Retrospective CBCT Study. J. Periodontol. 2020, 91, 1429–1435. [Google Scholar] [CrossRef]
- Nurbakhsh, B.; Friedman, S.; Kulkarni, G.V.; Basrani, B.; Lam, E. Resolution of Maxillary Sinus Mucositis after Endodontic Treatment of Maxillary Teeth with Apical Periodontitis: A Cone-Beam Computed Tomography Pilot Study. J. Endod. 2011, 37, 1504–1511. [Google Scholar] [CrossRef]
- Kapusuz Gencer, Z.; Özkırış, M.; Okur, A.; Karaçavuş, S.; Saydam, L. The Effect of Nasal Septal Deviation on Maxillary Sinus Volumes and Development of Maxillary Sinusitis. Eur. Arch. Oto-Rhino-Laryngol. 2013, 270, 3069–3073. [Google Scholar] [CrossRef]
- Moorthy, P.N.S.; Kolloju, S.; Madhira, S.; Jowkar, A.B. Clinical Study on Deviated Nasal Septum and Its Associated Pathology. Int. J. Otolaryngol. Head Neck Surg. 2014, 3, 75–81. [Google Scholar] [CrossRef]
- Rehman, A.; Hamid, S.; Ahmad, M.; Rashid, A.F. A Prospective Study of Nasal Septal Deformities in Kashmiri Population Attending a Tertiary Care Hospital. Int. J. Otolaryngol. Head Neck Surg. 2012, 1, 24807. [Google Scholar] [CrossRef]
- Smith, K.D.; Edwards, P.C.; Saini, T.S.; Norton, N.S. The Prevalence of Concha Bullosa and Nasal Septal Deviation and Their Relationship to Maxillary Sinusitis by Volumetric Tomography. Int. J. Dent. 2010, 2010, 404982. [Google Scholar] [CrossRef]
- Mohebbi, A.; Ahmadi, A.; Etemadi, M.; Safdarian, M.; Ghourchian, S. An Epidemiologic Study of Factors Associated with Nasal Septum Deviation by Computed Tomography Scan: A Cross Sectional Study. BMC Ear Nose Throat Disord. 2012, 12, 15. [Google Scholar] [CrossRef] [PubMed]
- Shoib, S.M.; Viswanatha, B. Association between Symptomatic Deviated Nasal Septum and Sinusitis: A Prospective Study. Res. Otolaryngol. 2016, 5, 1–8. [Google Scholar]
- Tassoker, M.; Magat, G.; Lale, B.; Gulec, M.; Ozcan, S.; Orhan, K. Is the Maxillary Sinus Volume Affected by Concha Bullosa, Nasal Septal Deviation, and Impacted Teeth? A CBCT Study. Eur. Arch. Oto-Rhino-Laryngol. 2020, 277, 227–233. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| n | % | |||
|---|---|---|---|---|
| Gender (n = 164 patients) | Male | 85 | 51.8 | |
| Female | 79 | 48.2 | ||
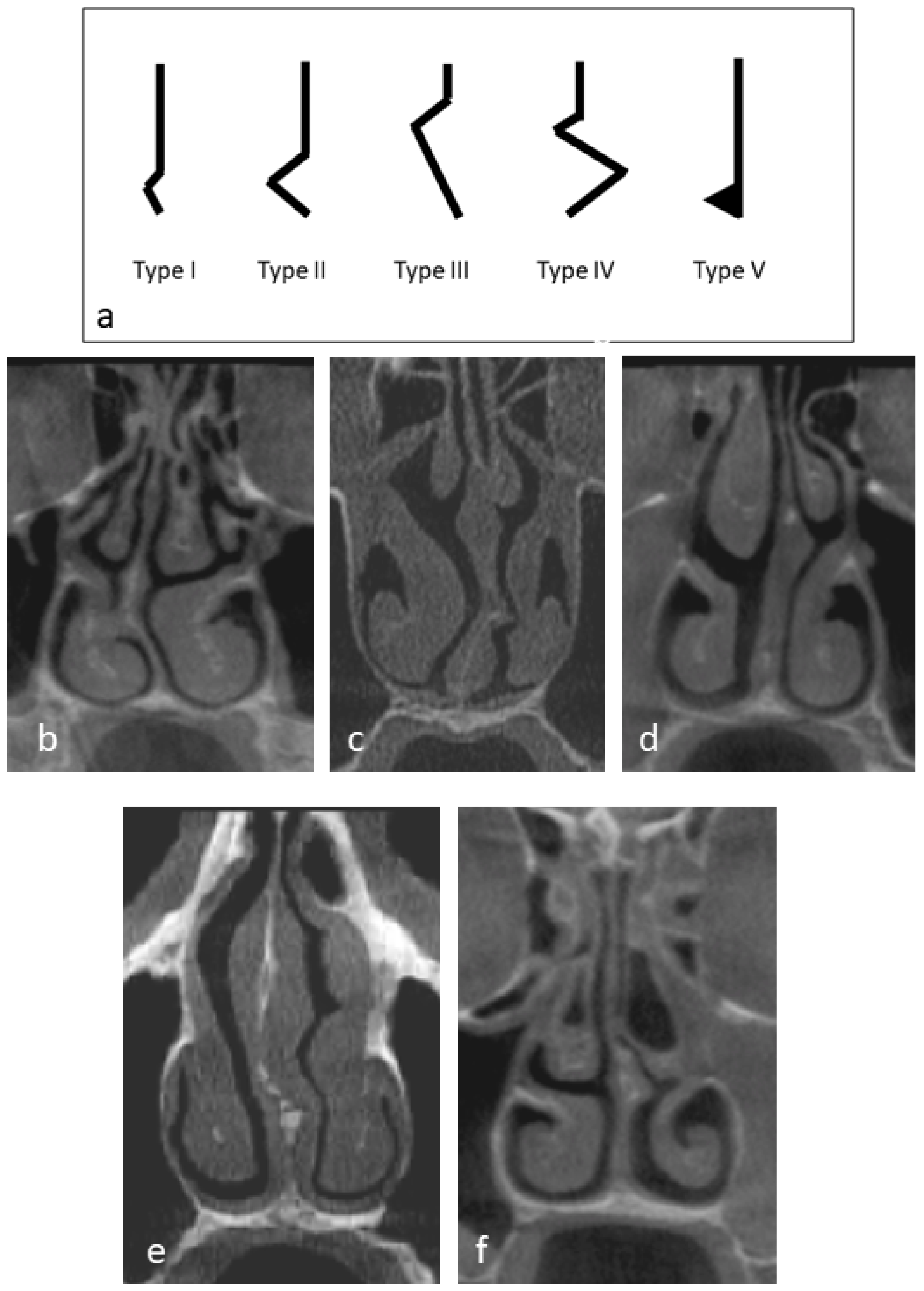
| Nasal septum classification (n = 164) | No nasal septum deviation | 84 | 51.2 | |
| Type I | 15 | 9.1 | ||
| Type II | 16 | 9.8 | ||
| Type III | 34 | 20.7 | ||
| Type IV | 3 | 1.8 | ||
| Type V | 12 | 7.3 | ||
| Prevalence of MT (n = 164 patients) | Yes | 131 | 79.9 | |
| No | 33 | 20.1 | ||
| Distribution of MT (n = 131 patients) | Unilateral | Right | 21 | 12.8 |
| Left | 34 | 20.7 | ||
| Bilateral | 76 | 46.3 | ||
| Teeth classification (n = 1269 teeth) | #18 and 28 | 149 | 11.7 | |
| #17 and 27 | 289 | 22.8 | ||
| #16 and 26 | 279 | 22.0 | ||
| #15 and 25 | 278 | 21.9 | ||
| #14 and 24 | 274 | 21.6 | ||
| Classification of MT (n = 1269 teeth) | 0–2 | 770 | 60.7 | |
| 2–10 | 313 | 24.7 | ||
| >10 | 186 | 14.7 | ||
| n | % | ||
|---|---|---|---|
| The relation of roots of posterior maxillary teeth to the sinus floor (RPMT) | Type 0 | 583 | 45.9 |
| Type 1 | 403 | 31.8 | |
| Type 2 | 183 | 14.4 | |
| Type 3 | 77 | 6.1 | |
| Type 4 | 23 | 1.8 | |
| Radiographic bone loss | <25% | 1148 | 90.5 |
| 25–50% | 68 | 5.4 | |
| >50% | 53 | 4.2 | |
| Teeth condition | Vital | 717 | 56.5 |
| Restoration | 317 | 25.0 | |
| Failed RCT | 156 | 12.3 | |
| RCT | 51 | 4.0 | |
| Remaining root | 15 | 1.2 | |
| Implant | 13 | 1.0 | |
| Root length (mean ± SD) | 13.1 ± 2.4 | ||
| Unconditional Model | Model with Level 1 Fixed-Effect Factors | Model with Level 2 Fixed-Effect Factors | Model with Level 1 and Level 2 Fixed-Effect Factors Combined | |
|---|---|---|---|---|
| ICC | 0.32 | 0.36 | 0.32 | 0.33 |
| Pseudo R2 | 0.27 | 0.34 | 0.27 | 0.35 |
| Percentage correctly classified | 76.4 | 79.3 | 76.4 | 79.6 |
| Mucosal Thickness of Maxillary Sinus Presence | ||||
|---|---|---|---|---|
| AOR | 95% CI | p Value | ||
| Patient-level factors | ||||
| Gender | Male | 1.46 | 0.92, 2.33 | 0.13 |
| Female | Reference | |||
| Nasal septum deviation | Yes | 0.74 | 0.46, 1.20 | 0.24 |
| No | Reference | |||
| Tooth-level factors | ||||
| The relation of roots of posterior maxillary teeth to the sinus floor (RPMT) | Type 1 | 2.80 | 1.98, 13.26 | <0.001 * |
| Type 2 | 3.43 | 1.43, 4.08 | <0.001 * | |
| Type 3 | 3.15 | 1.52, 3.26 | <0.001 * | |
| Type 4 | 4.04 | 1.57, 2.86 | <0.018 * | |
| Type 0 | Reference | |||
| Periodontal bone loss | >50% | 2.29 | 1.36, 4.82 | 0.07 |
| 25–50% | 1.34 | 1.02, 2.94 | 0.38 | |
| <25% | Reference | |||
| Tooth condition | RCT | 1.43 | 0.68, 2.98 | 0.34 |
| Failed RCT | 2.87 | 1.65, 4.42 | <0.001 * | |
| Restoration | 1.64 | 1.14, 2.36 | 0.008 * | |
| Implant | 0.25 | 0.05, 1.35 | 1.12 | |
| Remaining root | 1.78 | 0.44, 7.01 | 0.42 | |
| Vital | Reference | |||
| Root length | 0.96 | 0.91, 1.04 | 0.18 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Madi, M.; Alsaad, S.S.; AlAssiry, N.; Attia, D.; AlAssiry, M.; Zakaria, O. Multilevel Modeling Analysis of Odontogenic Risk Factors and Nasal Septum Deviation Associated with Maxillary Sinus Mucosal Thickening: A Cone-Beam Computed Tomography Study. Dent. J. 2024, 12, 74. https://doi.org/10.3390/dj12030074
Madi M, Alsaad SS, AlAssiry N, Attia D, AlAssiry M, Zakaria O. Multilevel Modeling Analysis of Odontogenic Risk Factors and Nasal Septum Deviation Associated with Maxillary Sinus Mucosal Thickening: A Cone-Beam Computed Tomography Study. Dentistry Journal. 2024; 12(3):74. https://doi.org/10.3390/dj12030074
Chicago/Turabian StyleMadi, Marwa, Sara S. Alsaad, Nada AlAssiry, Dina Attia, Mansour AlAssiry, and Osama Zakaria. 2024. "Multilevel Modeling Analysis of Odontogenic Risk Factors and Nasal Septum Deviation Associated with Maxillary Sinus Mucosal Thickening: A Cone-Beam Computed Tomography Study" Dentistry Journal 12, no. 3: 74. https://doi.org/10.3390/dj12030074