
Endodontic Outcome of Root Canal Treatment Using Different Obturation Techniques: A Clinical Study
 , , , and
, , , and
Abstract
:1. Introduction
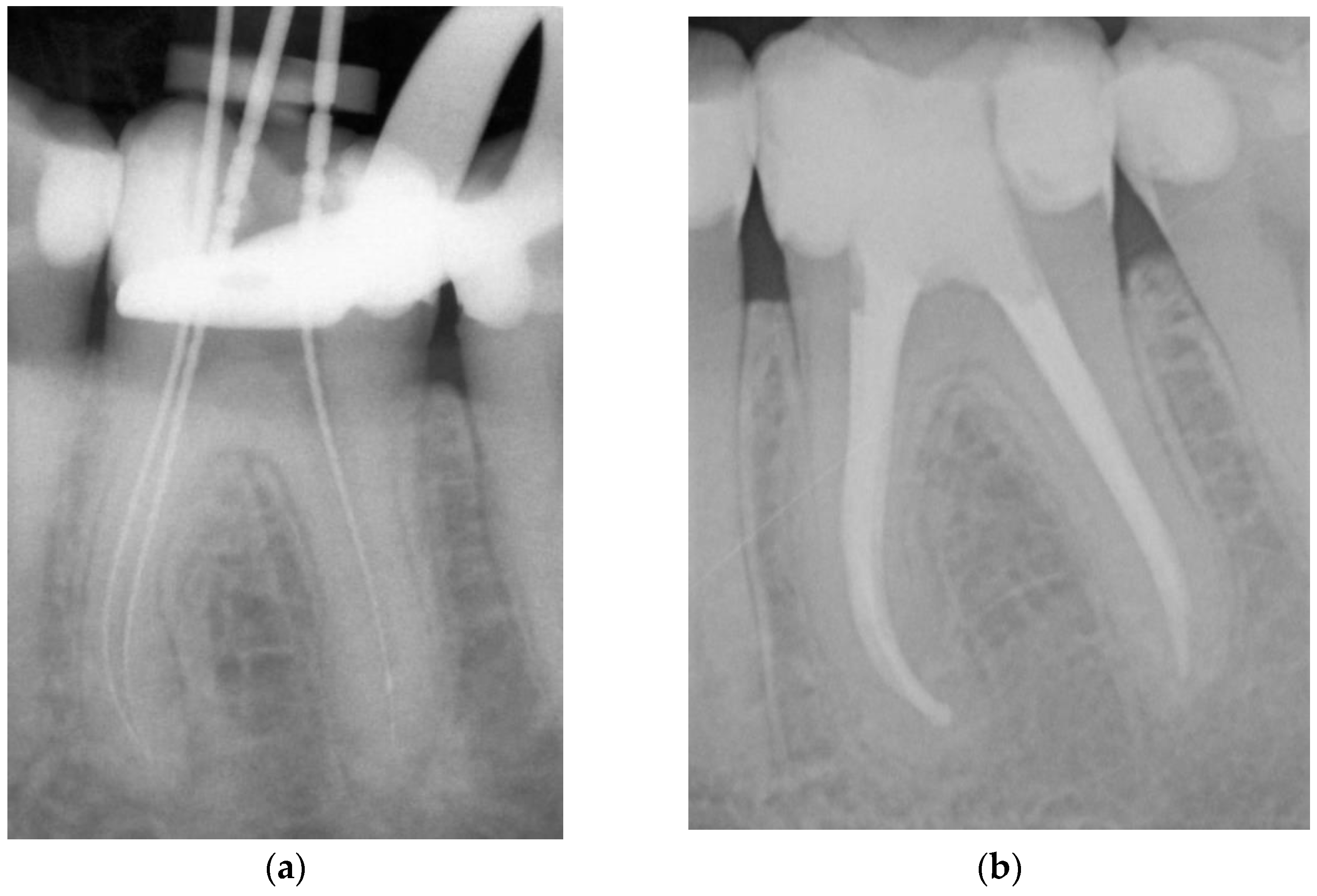
- Adhesive obturation using the continuous wave of condensation technique with Resilon® (CWR).
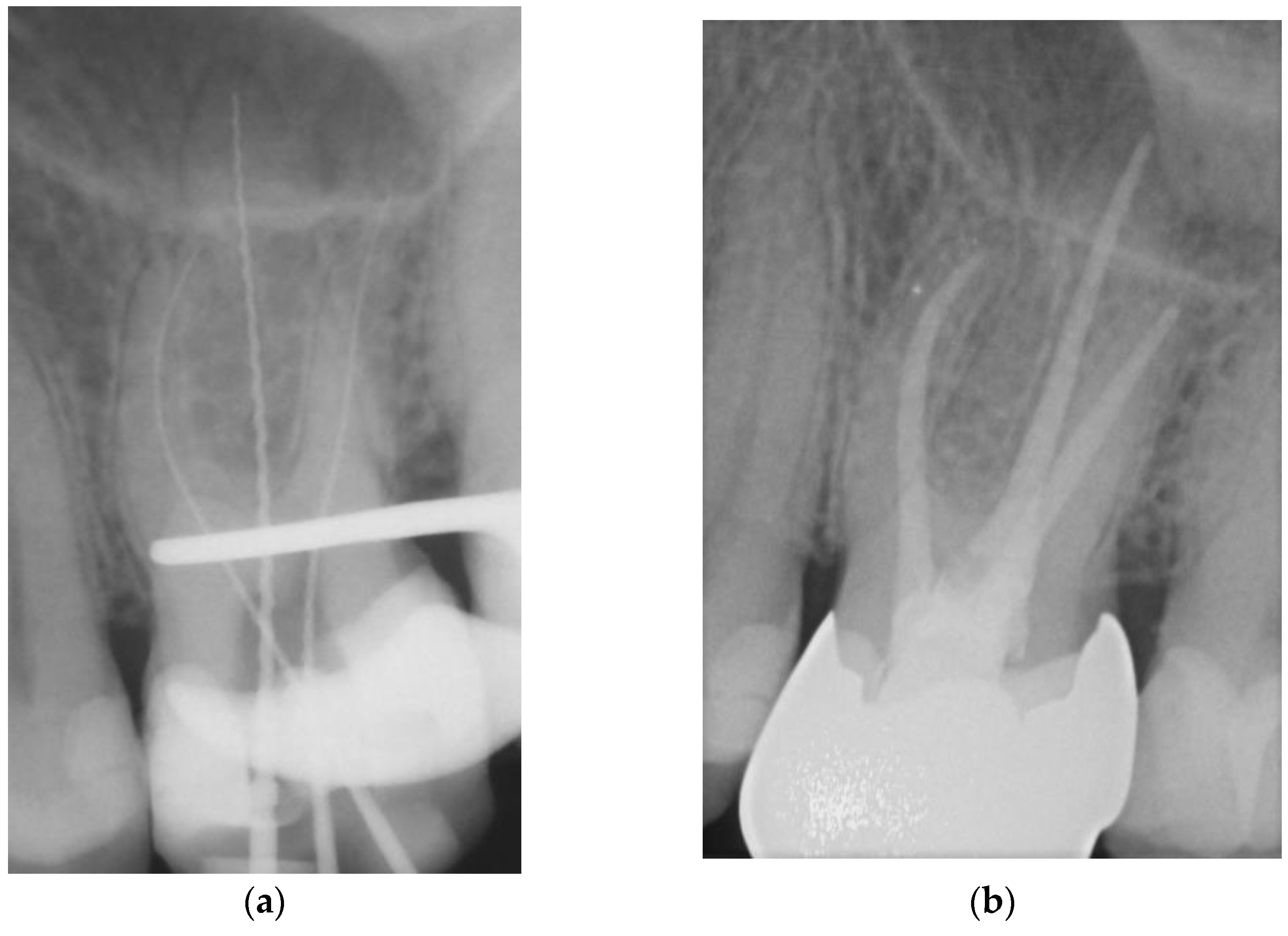
- Matching-taper single-cone obturation with gutta-percha and the epoxy-resin-based sealer AH Plus® (SCGP).
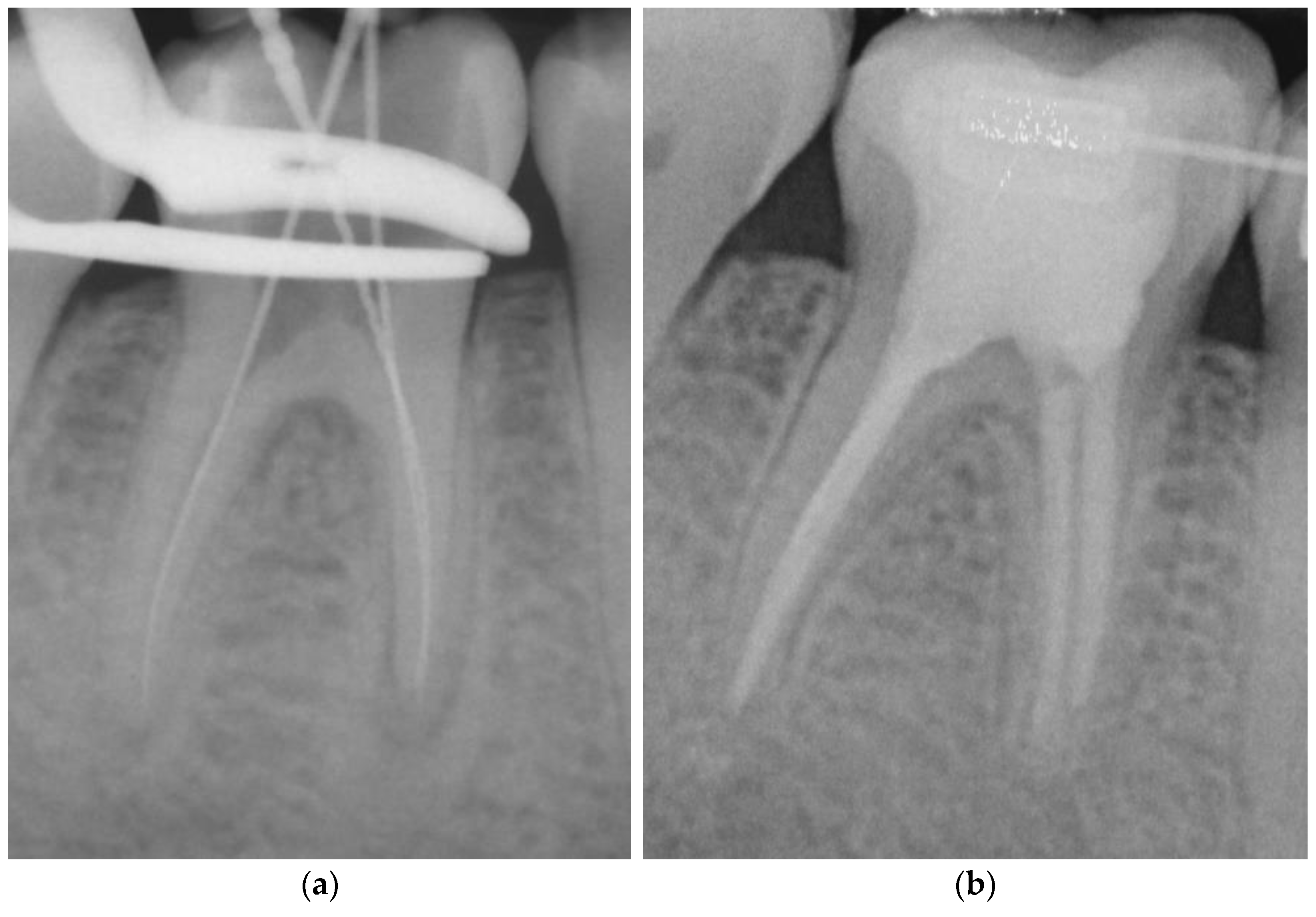
- Matching-taper single-cone obturation with gutta-percha and the silicon-based sealer GuttaFlow® (SCGF).
2. Materials and Methods
- Adhesive obturation using the continuous wave of condensation technique with Resilon® (CWR) (Figure 1).
- Matching-taper single-cone obturation with gutta-percha and the epoxy-resin-based sealer AH Plus® (SCGP) (Figure 2).
- Matching-taper single-cone obturation with gutta-percha and the silicon-based sealer GuttaFlow® (SCGF) (Figure 3).
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Connert, T.; Truckenmüller, M.; ElAyouti, A.; Eggmann, F.; Krastl, G.; Löst, C.; Weiger, R. Changes in periapical status, quality of root fillings and estimated endodontic treatment need in a similar urban German population 20 years later. Clin. Oral Investig. 2019, 23, 1373–1382. [Google Scholar] [CrossRef] [PubMed]
- Laukkanen, E.; Vehkalahti, M.M.; Kotiranta, A.K. Radiographic outcome of root canal treatment in general dental practice: Tooth type and quality of root filling as prognostic factors. Acta Odontol. Scand. 2021, 79, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Ng, Y.L.; Mann, V.; Rahbaran, S.; Lewsey, J.; Gulabivala, K. Outcome of primary root canal treatment: Systematic review of the literature—Part 2. Influence of clinical factors. Int. Endod. J. 2008, 41, 6–31. [Google Scholar] [CrossRef] [PubMed]
- Wesselink, P. Root filling techniques. In Textbook of Endodontology, 2nd ed.; Bergenholtz, G., Hørsted-Bindslev, P., Reit, C., Eds.; Wiley-Blackwell, John Wiley & Sons Ltd: Oxford, UK, 2010; pp. 219–232. [Google Scholar]
- Ørstavik, D. Materials used for root canal obturation: Technical, biological and clinical testing. Endod. Top. 2005, 12, 25–38. [Google Scholar] [CrossRef]
- Ørstavik, D.; Nordahl, I.; Tibballs, J.E. Dimensional change following setting of root canal sealer materials. Dent. Mater. 2001, 17, 512–519. [Google Scholar] [CrossRef] [PubMed]
- Qualtrough, A.J.E.; Whitworth, J.M.; Dummer, P.M.H. Preclinical endodontology: An international comparison. Int. Endod. J. 1999, 32, 406–414. [Google Scholar] [CrossRef] [PubMed]
- Whitworth, J.M. Methods of filling root canals: Principles and practices. Endod. Top. 2005, 12, 2–24. [Google Scholar] [CrossRef]
- Pirani, C.; Camilleri, J. Effectiveness of root canal filling materials and techniques for treatment of apical periodontitis: A systematic review. Int. Endod. J. 2022. [Google Scholar] [CrossRef]
- Schäfer, E.; Schrenker, C.; Zupanc, J.; Bürklein, S. Percentage of Gutta-percha Filled Areas in Canals Obturated with Cross-linked Gutta-percha Core-carrier Systems, Single-Cone and Lateral Compaction Technique. J. Endod. 2016, 42, 294–298. [Google Scholar] [CrossRef]
- Krug, R.; Krastl, G.; Jahreis, M. Technical quality of a matching-taper single-cone filling technique following rotary instrumentation compared with lateral compaction after manual preparation: A retrospective study. Clin. Oral Investig. 2017, 21, 643–652. [Google Scholar] [CrossRef]
- Brosh, T.; Metzger, Z.; Pilo, R. Circumferential root strains generated during lateral compaction with stainless steel vs. nickel-titanium finger spreaders. Eur. J. Oral Sci. 2018, 126, 518–525. [Google Scholar] [CrossRef] [PubMed]
- Koçak, M.M.; Darendeliler-Yaman, S. Sealing ability of lateral compaction and tapered single cone gutta-percha techniques in root canals prepared with stainless steel and rotary nickel titanium instruments. J. Clin. Exp. Dent. 2012, 4, e156–e159. [Google Scholar] [CrossRef]
- Wu, M.K.; Bud, M.G.; Wesselink, P.R. The quality of single cone and laterally compacted gutta-percha fillings in small and curved root canals as evidenced by bidirectional radiographs and fluid transport measurements. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2009, 108, 946–951. [Google Scholar] [CrossRef] [PubMed]
- Schäfer, E.; Nelius, B.; Bürklein, S. A comparative evaluation of gutta-percha filled areas in curved root canals obturated with different techniques. Clin. Oral Investig. 2012, 16, 225–230. [Google Scholar] [CrossRef] [PubMed]
- McMichen, F.R.; Pearson, G.; Rahbaran, S.; Gulabivala, K. A comparative study of selected physical properties of five root-canal sealers. Int. Endod. J. 2003, 36, 629–635. [Google Scholar] [CrossRef] [PubMed]
- Silva, E.J.N.L.; Cardoso, M.L.; Rodrigues, J.P.; De-Deus, G.; Fidalgo, T.K.d.S. Solubility of bioceramic- and epoxy resin-based root canal sealers: A systematic review and meta-analysis. Aust. Endod. J. 2021, 47, 690–702. [Google Scholar] [CrossRef] [PubMed]
- Wu, D.; Tang, Z.; Zhang, G.; Liu, W. The sealing ability of a new silicone-based root canal filling material (GuttaFlow): An in vitro study using the percentage of gutta-percha-filled area. Dent. Mater. J. 2011, 30, 569–575. [Google Scholar] [CrossRef] [PubMed]
- Zielinski, T.M.; Baumgartner, J.C.; Marshall, J.G. An evaluation of Guttaflow and gutta-percha in the filling of lateral grooves and depressions. J. Endod. 2008, 34, 295–298. [Google Scholar] [CrossRef]
- Donnelly, A.; Sword, J.; Nishitani, Y.; Yoshiyama, M.; Agee, K.; Tay, F.R.; Pashley, D.H. Water sorption and solubility of methacrylate resin-based root canal sealers. J. Endod. 2007, 33, 990–994. [Google Scholar] [CrossRef]
- Patil, P.; Rathore, V.P.; Hotkar, C.; Savgave, S.S.; Raghavendra, K.; Ingale, P. A comparison of apical sealing ability between GuttaFlow and AH plus: An in vitro study. J. Int. Soc. Prev. Community Dent. 2016, 6, 377–382. [Google Scholar] [CrossRef]
- Savariz, A.; González-Rodríguez, M.P.; Ferrer-Luque, C.M. Long-term sealing ability of GuttaFlow versus Ah Plus using different obturation techniques. Med. Oral Patol. Oral Cir. Bucal 2010, 15, e936–e941. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, F.B.; Teixeira, E.C.; Thompson, J.; Leinfelder, K.F.; Trope, M. Dentinal bonding reaches the root canal system. J. Esthet. Restor. Dent. 2004, 16, 348–354, discussion 354. [Google Scholar] [CrossRef] [PubMed]
- Shipper, G.; Ørstavik, D.; Teixeira, F.B.; Trope, M. An evaluation of microbial leakage in roots filled with a thermoplastic synthetic polymer-based root canal filling material (Resilon). J. Endod. 2004, 30, 342–347. [Google Scholar] [CrossRef] [PubMed]
- Tay, F.R.; Pashley, D.H. Monoblocks in root canals: A hypothetical or a tangible goal. J. Endod. 2007, 33, 391–398. [Google Scholar] [CrossRef] [PubMed]
- Tay, F.R.; Loushine, R.J.; Lambrechts, P.; Weller, R.N.; Pashley, D.H. Geometric factors affecting dentin bonding in root canals: A theoretical modeling approach. J. Endod. 2005, 31, 584–589. [Google Scholar] [CrossRef] [PubMed]
- De Munck, J.; Van Landuyt, K.; Peumans, M.; Poitevin, A.; Lambrechts, P.; Braem, M.; Van Meerbeek, B. A critical review of the durability of adhesion to tooth tissue: Methods and results. J. Dent. Res. 2005, 84, 118–132. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.K.; Grandini, S.; Ames, J.M.; Gu, L.S.; Kim, S.K.; Pashley, D.H.; Gutmann, J.L.; Tay, F.R. Critical review on methacrylate resin-based root canal sealers. J. Endod. 2010, 36, 383–399. [Google Scholar] [CrossRef] [PubMed]
- Kqiku, L.; Miletic, I.; Gruber, H.J.; Anic, I.; Städtler, P. Microleakage of root canal fillings with GuttaFlow and Resilon compared with lateral condensation. Wien. Med. Wochenschr. 2010, 160, 230–234. [Google Scholar] [CrossRef]
- Prithviraj, K.J.; Manjunatha, R.K.; Horatti, P.; Rao, N.; Gokul, S. In Vitro comparison of the microbial leakage of obturation systems: Epiphany with resilon, guttaflow, and ah plus with gutta percha. Indian J. Dent. Res. Off. Publ. Indian Soc. Dent. Res. 2020, 31, 37–41. [Google Scholar] [CrossRef]
- Barborka, B.J.; Woodmansey, K.F.; Glickman, G.N.; Schneiderman, E.; He, J. Long-term Clinical Outcome of Teeth Obturated with Resilon. J. Endod. 2017, 43, 556–560. [Google Scholar] [CrossRef]
- Strange, K.A.; Tawil, P.Z.; Phillips, C.; Walia, H.D.; Fouad, A.F. Long-term Outcomes of Endodontic Treatment Performed with Resilon/Epiphany. J. Endod. 2019, 45, 507–512. [Google Scholar] [CrossRef] [PubMed]
- Payne, L.A.; Tawil, P.Z.; Phillips, C.; Fouad, A.F. Resilon: Assessment of Degraded Filling Material in Nonhealed Cases. J. Endod. 2019, 45, 691–695. [Google Scholar] [CrossRef] [PubMed]
- Ørstavik, D. Reliability of the periapical index scoring system. Scand. J. Dent. Res. 1988, 96, 108–111. [Google Scholar] [CrossRef] [PubMed]
- Kirkevang, L.L.; Ørstavik, D.; Wenzel, A.; Vaeth, M. Prognostic value of the full-scale Periapical Index. Int. Endod. J. 2015, 48, 1051–1058. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. A Coefficient of Agreement for Nominal Scales. Educ. Psychol. Meas. 1960, 20, 37–46. [Google Scholar] [CrossRef]
- Ng, Y.L.; Mann, V.; Rahbaran, S.; Lewsey, J.; Gulabivala, K. Outcome of primary root canal treatment: Systematic review of the literature—Part 1. Effects of study characteristics on probability of success. Int. Endod. J. 2007, 40, 921–939. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.K.; Shemesh, H.; Wesselink, P.R. Limitations of previously published systematic reviews evaluating the outcome of endodontic treatment. Int. Endod. J. 2009, 42, 656–666. [Google Scholar] [CrossRef]
- Cotton, T.P.; Schindler, W.G.; Schwartz, S.A.; Watson, W.R.; Hargreaves, K.M. A retrospective study comparing clinical outcomes after obturation with Resilon/Epiphany or Gutta-Percha/Kerr sealer. J. Endod. 2008, 34, 789–797. [Google Scholar] [CrossRef]
- Hiraishi, N.; Sadek, F.T.; King, N.M.; Ferrari, M.; Pashley, D.H.; Tay, F.R. Susceptibility of a polycaprolactone-based root canal filling material to degradation using an agar-well diffusion assay. Am. J. Dent. 2008, 21, 119–123. [Google Scholar]
- Hwang, J.H.; Chung, J.; Na, H.S.; Park, E.; Kwak, S.; Kim, H.C. Comparison of bacterial leakage resistance of various root canal filling materials and methods: Confocal laser-scanning microscope study. Scanning 2015, 37, 422–428. [Google Scholar] [CrossRef]
- Adhikari, H.D.; Jain, S. Scanning electron microscopic evaluation of marginal adaptation of AH-Plus, GuttaFlow, and RealSeal at apical one-third of root canals—Part II: Core-sealer interface. J. Conserv. Dent. 2018, 21, 90–94. [Google Scholar] [CrossRef] [PubMed]
- Herbert, J.; Bruder, M.; Braunsteiner, J.; Altenburger, M.J.; Wrbas, K.T. Apical quality and adaptation of Resilon, EndoREZ, and Guttaflow root canal fillings in combination with a noncompaction technique. J. Endod. 2009, 35, 261–264. [Google Scholar] [CrossRef] [PubMed]
- Khandelwal, A.; Janani, K.; Teja, K.; Jose, J.; Battineni, G.; Riccitiello, F.; Valletta, A.; Palanivelu, A.; Spagnuolo, G. Periapical Healing following Root Canal Treatment Using Different Endodontic Sealers: A Systematic Review. BioMed Res. Int. 2022, 2022, 3569281. [Google Scholar] [CrossRef] [PubMed]
- Aqrabawi, J.A. Outcome of endodontic treatment of teeth filled using lateral condensation versus vertical compaction (Schilder’s technique). J. Contemp. Dent. Pract. 2006, 7, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Peng, L.; Ye, L.; Tan, H.; Zhou, X. Outcome of root canal obturation by warm gutta-percha versus cold lateral condensation: A meta-analysis. J. Endod. 2007, 33, 106–109. [Google Scholar] [CrossRef] [PubMed]
- Sjogren, U.; Hagglund, B.; Sundqvist, G.; Wing, K. Factors affecting the long-term results of endodontic treatment. J. Endod. 1990, 16, 498–504. [Google Scholar] [CrossRef] [PubMed]
- Jahreis, M.; Soliman, S.; Schubert, A.; Connert, T.; Schlagenhauf, U.; Krastl, G.; Krug, R. Outcome of non-surgical root canal treatment related to periodontitis and chronic disease medication among adults in age group of 60 years or more. Gerodontology 2019, 36, 267–275. [Google Scholar] [CrossRef] [PubMed]
- Ng, Y.L.; Mann, V.; Gulabivala, K. A prospective study of the factors affecting outcomes of non-surgical root canal treatment: Part 2: Tooth survival. Int. Endod. J. 2011, 44, 610–625. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Records data | Anamnesis, type and progress of endodontic treatment, obturation material and technique, periapical radiographs |
| Radiographic data | Preoperative, working length, and postoperative radiographs of high quality using a digital imaging assessment (VistaScan Mini View, Dürr Dental SE) with a high resolution of 22 line pairs each millimeter |
| Demographic data | Age and gender of the participants in this study at the time of the follow-up examination |
| Time of treatment, operator | Endodontic treatment at the University of Würzburg, Department of Conservative Dentistry (Würzburg, Germany), between 2009 and 2012 |
| Obturation technique |
|
| PAI | 1 | Sound periapical status |
| 2 | Minor changes in bone structure | |
| 3 | Changes in bone structure with mineral loss | |
| 4 | Apical periodontitis with defined lesion | |
| 5 | Severe apical periodontitis with signs of exacerbation | |
| Length of RCF | Adequate | RCF ending ≤ 2 mm from the radiographic apex |
| Overfilled | RCF ending beyond the radiographic apex | |
| Underfilled | RCF ending > 2 mm from the radiographic apex | |
| Homogeneity of RCF | Homogeneous | Absence of voids within or between fillings and root canal walls |
| Inhomogeneous | Presence of voids within or between fillings and root canal walls |
| Total [n] | Sound [n] (%) | Diseased [n] (%) | |
|---|---|---|---|
| Before intervention | 114 | 43 (37.7%) | 71 (62.3%) |
| After intervention | 114 | 86 (75.4%) | 28 (24.6%) |
| Obturation Technique | Total [n] (%) | Success [n] (%) | Failure [n] (%) |
|---|---|---|---|
| CWR | 64 (56.1%) | 44 (68.7%) | 20 (31.3%) |
| SCGP | 40 (35.1%) | 34 (85.0%) | 6 (15.0%) |
| SCGF | 10 (8.8%) | 8 (80.0%) | 2 (20.0%) |
| Total [n] | 114 (100%) | 86 (75.4%) | 28 (24.6%) |
| Quality Criteria | CWR (n = 64) | SCGP (n = 40) | SCGF (n = 10) | p | Effect Size | |
|---|---|---|---|---|---|---|
| Homogeneity | Homogeneous | 51 (79.7%) | 27 (67.5%) | 9 (90.0%) | 0.20 | |
| Inhomogeneous | 13 (20.3%) | 13 (32.5%) | 1 (10.0%) | |||
| Extrusion of RCF | No extrusion | 54 (84.4%) | 33 (82.5%) | 8 (80.0%) | 0.93 | |
| Extrusion | 10 (15.6%) | 7 (17.5%) | 2 (20.0%) | |||
| Length of RCF | Adequate | 46 (71.9%) | 37 (92.5%) | 8 (80.0%) | 0.04 * | 0.24 (Cramer’s V) |
| Underfilled | 12 (18.7%) | 3 (7.5%) | 0 (0.0%) | |||
| Overfilled | 6 (9.4%) | 0 (0.0%) | 2 (20.0%) |
| Total [n] (%) | Success [n] (%) | Failure [n] (%) | p | Effect Size | ||
|---|---|---|---|---|---|---|
| Preoperative periapical status | Sound | 43 (37.7%) | 39 (90.7%) | 4 (9.3%) | 0.007 * | 0.28 (Phi) |
| Diseased | 71 (62.3%) | 47 (66.2%) | 24 (33.8%) | |||
| Total | 114 (100%) | 86 (75.4%) | 28 (24.6%) | |||
| Type of treatment | Primary treatment | 70 (61.4%) | 55 (78.6%) | 15 (21.4%) | 0.45 | |
| Retreatment | 44 (38.6%) | 31 (70.4%) | 13 (29.6%) | |||
| Total | 114 (100%) | 86 (75.4%) | 28 (24.6%) | |||
| Periodontitis | Present | 81 (73.0%) | 58 (71.6%) | 23 (28.4%) | 0.08 | |
| Absent | 30 (27.0%) | 27 (90.0%) | 3 (10.0%) | |||
| Total | 111 (100%) | 85 (76.6%) | 26 (23.4%) | |||
| Quality of coronal restoration | Adequate | 107 (93.9%) | 82 (76.6%) | 25 (23.3%) | 0.36 | |
| Inadequate | 7 (6.1%) | 4 (57.1%) | 3 (42.9%) | |||
| Total | 114 (100%) | 86 (75.4%) | 28 (24.6%) | |||
| Tooth type | Incisors | 25 (21.9%) | 23 (92.0%) | 2 (8.0%) | 0.07 | |
| Premolars | 25 (21.9%) | 19 (76.0%) | 6 (24.0%) | |||
| Molars | 64 (56.2%) | 44 (68.7%) | 20 (31.3%) | |||
| Gender | Male | 45 (39.5%) | 33 (73.3%) | 12 (26.7%) | 0.67 | |
| Female | 69 (60.5%) | 53 (76.8%) | 16 (23.2%) | |||
| Total | 114 (100%) | 86 (75.4%) | 28 (24.6%) | |||
| Chronic disease medication | Present | 47 (42.3%) | 39 (83.0%) | 8 (17.0%) | 0.19 | |
| Absent | 64 (57.7%) | 45 (70.3%) | 19 (29.7%) | |||
| Total | 111 (100%) | 84 (75.7%) | 27 (24.3%) | |||
| Smoking | Present | 27 (23.7%) | 18 (66.7%) | 9 (33.3%) | 0.34 | |
| Absent | 87 (76.3%) | 68 (78.2%) | 19 (21.8%) | |||
| Total | 114 (100%) | 86 (75.4%) | 28 (24.6%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Winkler, A.; Adler, P.; Ludwig, J.; Hofmann, N.; Soliman, S.; Krastl, G.; Krug, R. Endodontic Outcome of Root Canal Treatment Using Different Obturation Techniques: A Clinical Study. Dent. J. 2023, 11, 200. https://doi.org/10.3390/dj11080200
Winkler A, Adler P, Ludwig J, Hofmann N, Soliman S, Krastl G, Krug R. Endodontic Outcome of Root Canal Treatment Using Different Obturation Techniques: A Clinical Study. Dentistry Journal. 2023; 11(8):200. https://doi.org/10.3390/dj11080200
Chicago/Turabian StyleWinkler, Alexander, Philipp Adler, Julia Ludwig, Norbert Hofmann, Sebastian Soliman, Gabriel Krastl, and Ralf Krug. 2023. "Endodontic Outcome of Root Canal Treatment Using Different Obturation Techniques: A Clinical Study" Dentistry Journal 11, no. 8: 200. https://doi.org/10.3390/dj11080200