
Extraction Socket Augmentation with Autologous Platelet-Rich Fibrin (PRF): The Rationale for Socket Augmentation

Abstract
:1. Introduction
1.1. Post-Extraction Alveolar Bone Resorption
1.1.1. Stages of Post-Extraction Changes
1.1.2. Post-Extraction Socket Augmentation
1.2. Decision Tree for timing of Implant Placement
1.3. Extraction Socket Healing and Dimensional Changes
1.4. Stages of Extraction Socket Healing
1.4.1. Haemostasias and Inflammation Phase
1.4.2. Cell Proliferation Phase
2. Indications for Socket Augmentation
2.1. Indications for Socket Augmentation at the Time of Tooth Loss
- To preserve and augment hard and soft tissues to mitigate against post-extraction socket remodelling when future implant placement is being planned, see Table 4;
- To optimise the future implant site for prosthodontically guided, 3D placement of an implant to fulfil aesthetic, functional, and biomechanical requirements and patient expectations;
- To regenerate bone within the socket to facilitate future implant placement with improved primary stability;
- To prevent gross post-extraction alveolar ridge reduction in sites:
- ◦
- With damaged socket walls;
- ◦
- With thin gingival biotype or thin buccal wall thickness <2 mm;
- ◦
- In close proximity to apically related anatomical structures such as the maxillary sinus or inferior alveolar nerve.
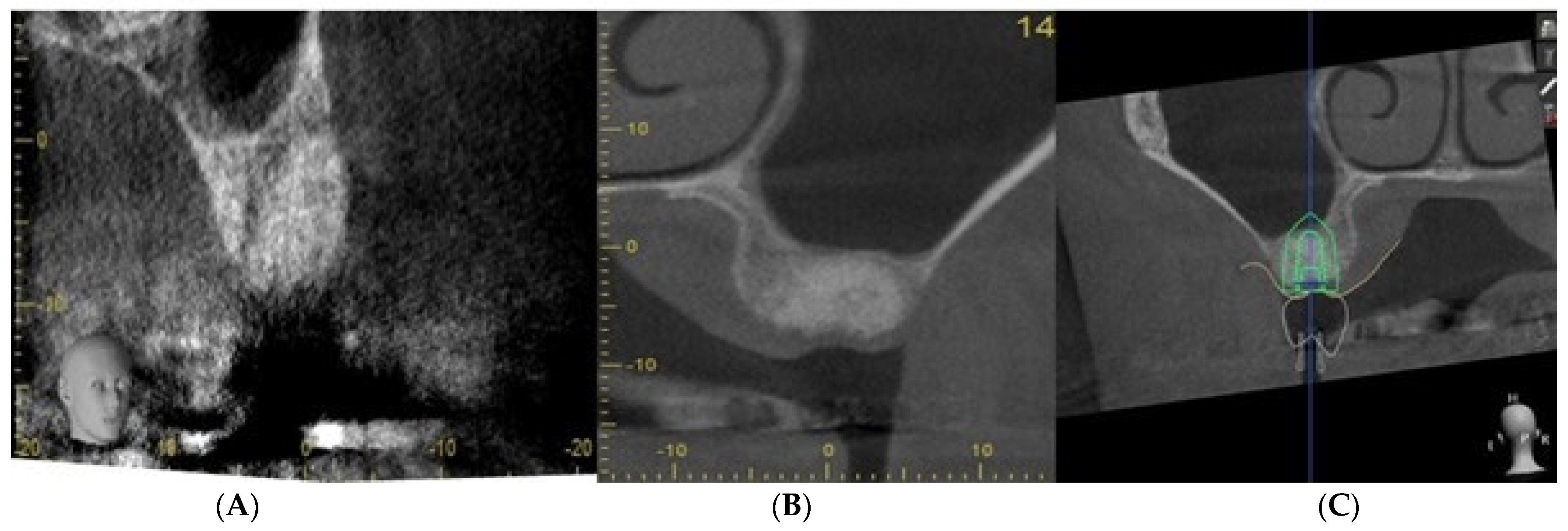
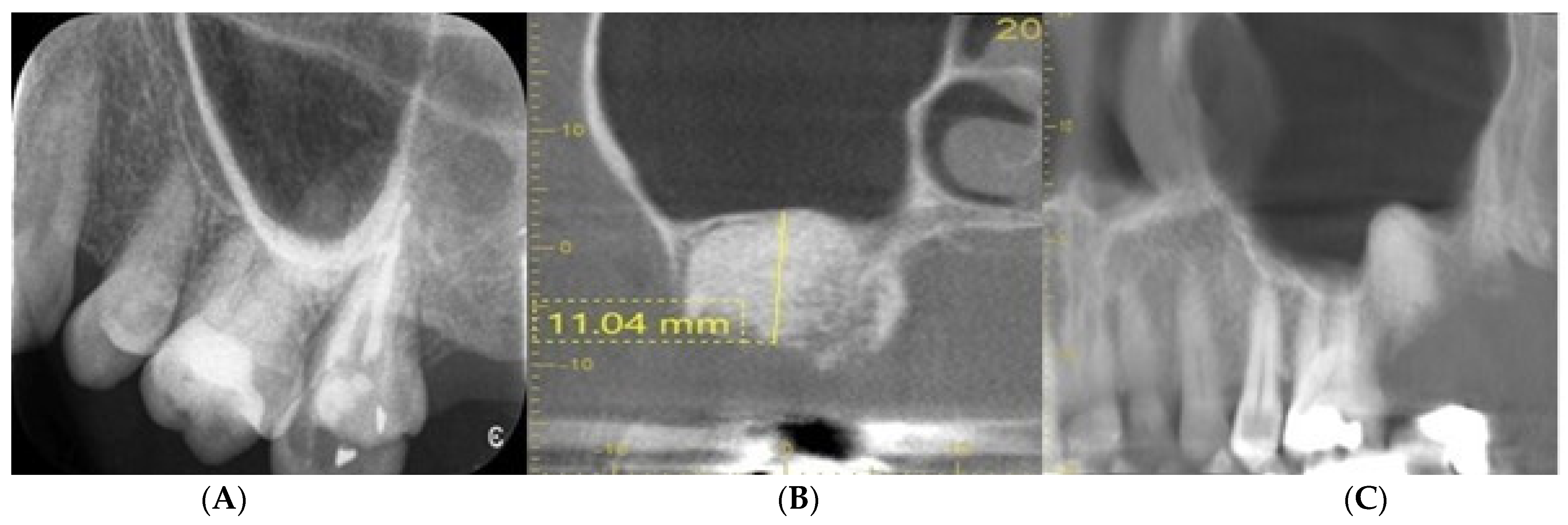
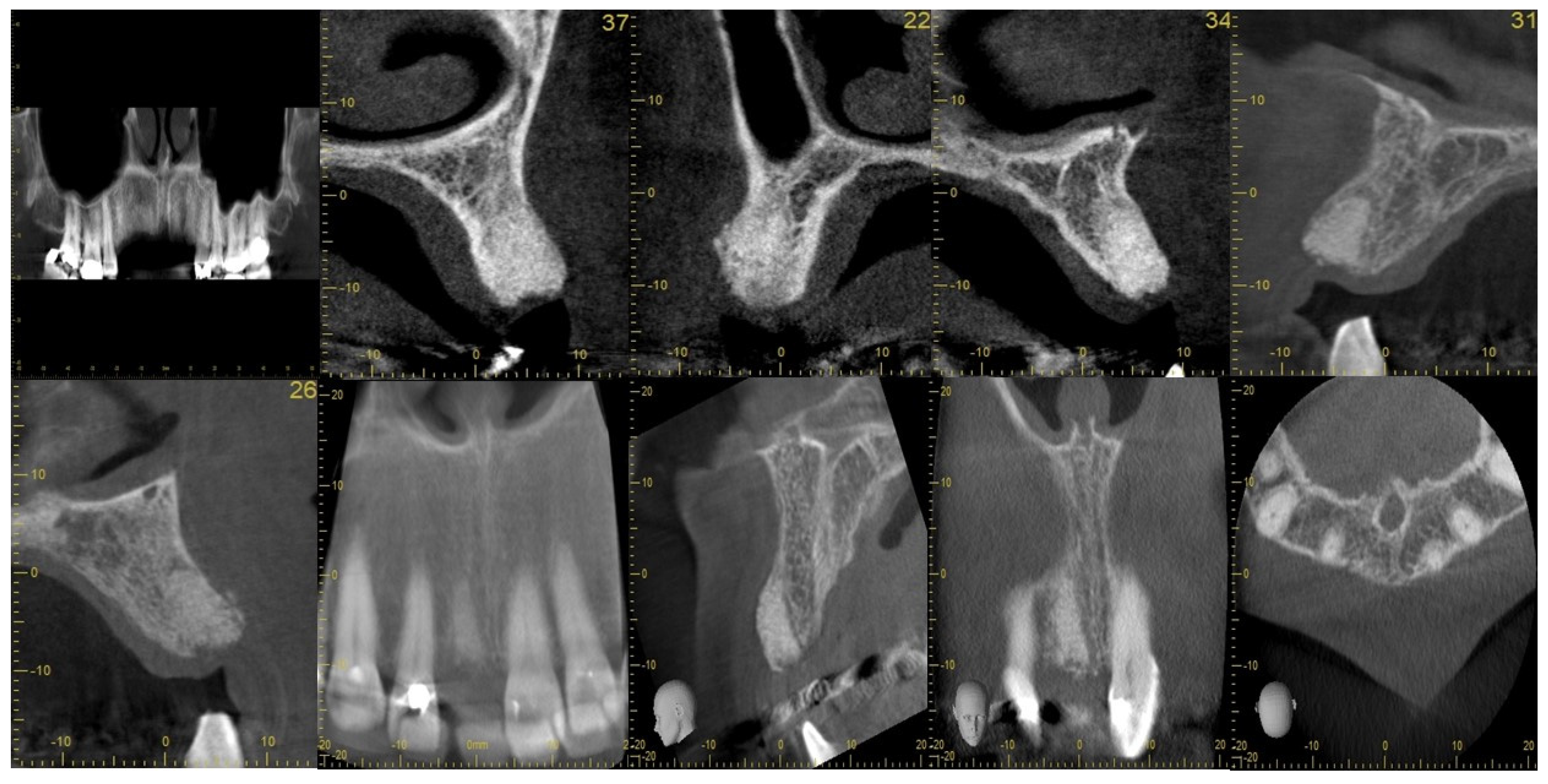
2.2. Case Study
2.3. Evidence for Socket Augmentation
2.4. Clinical, Radiological, and Histological Investigations Validating the Technique of Socket Augmentation
2.5. Comparative Study Analysis of Socket Augmentation
3. Bone Grafting and Guided Bone Regeneration
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Johnson, K. A study of the dimensional changes occurring in the maxilla following tooth extraction. Aust. Dent. J. 1969, 14, 241–244. [Google Scholar] [CrossRef] [PubMed]
- Marrelli, M.; Tatullo, M. Influence of PRF in the healing of bone and gingival tissues. Clin. Histol. Eval. Eur. Rev. Med. Pharmacol. Sci. 2013, 17, 1958–1962. [Google Scholar]
- Isalla, J.M.; Greenwell, H. Ridge preservation with freeze dried bone allograft and a membrane compared to extraction alone for implant site preparation: A clinical and histological study in humans. J. Periodontol. 2003, 74, 990–999. [Google Scholar] [CrossRef] [Green Version]
- Maia, L.P.; Reino, D.M.; Novaes Junior, A.B.; Muglia, V.A.; Taba Junior, M.; Grisi, M.F.; Souza, S.L.; Palioto, D.B. Influence of periodontal biotype on buccal bone remodeling after tooth extraction using the flapless approach with a xenograft: A histomorphometric and fluorescence study in small dogs. Clin. Implant Dent. Relat. Res. 2015, 17 (Suppl. S1), e221–e235. [Google Scholar] [CrossRef]
- Chappuis, V.; Araújo, M.G.; Buser, D. Clinical relevance of dimensional bone and soft tissue alterations post-extraction in esthetic sites. Periodontology 2000 2017, 73, 73–83. [Google Scholar] [CrossRef]
- Chen, S.T.; Wilson, T.G., Jr.; Hämmerle, C.H. Immediate or early placement of implants following tooth extraction: Review of biologic basis, clinical procedures, and outcomes. Int. J. Oral Maxillofac. Implant. 2004, 19, 12–25. [Google Scholar]
- Atieh, M.A.; Alsabeeha, N.H.; Payne, A.G.; Ali, S.; Faggion, C.M.J.; Esposito, M. Interventions for replacing missing teeth: Alveolar ridge preservation techniques for dental implant site development. Cochrane Database Syst. Rev. 2021, 4, CD010176. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Jung, R.E.; Avila-Ortiz, G.; Blanco, J.; Cosyn, J.; Fickl, S.; Figuero, E.; Goldstein, M.; Graziani, F.; Madianos, P.; et al. Management of the extraction socket and timing of implant placement: Consensus report and clinical recommendations of group 3 of the XV European Workshop in Periodontology. J. Clin. Periodontol. 2019, 46 (Suppl. S21), 183–194. [Google Scholar] [CrossRef] [Green Version]
- Lombardi, T.; Bernardello, F.; Berton, F.; Porrelli, D.; Rapani, A.; Camurri Piloni, A.; Fiorillo, L.; Di Lenarda, R.; Stacchi, C. Efficacy of Alveolar Ridge Preservation after Maxillary Molar Extraction in Reducing Crestal Bone Resorption and Sinus Pneumatization: A Multicenter Prospective Case-Control Study. BioMed Res. Int. 2018, 2018, 9352130. [Google Scholar] [CrossRef] [Green Version]
- Schropp, L.; Wenzel, A.; Kostopoulos, L.; Karring, T. Bone healing and soft tissue contour changes following single-tooth extraction: A clinical and radiographic 12-month prospective study. Int. J. Periodontics Restor. Dent. 2003, 23, 313–323. [Google Scholar]
- Li, B.; Wang, Y. Contour changes in human alveolar bone following tooth extraction of the maxillary central incisor. J. Zhejiang Univ. Sci. B 2014, 15, 1064–1071. [Google Scholar] [CrossRef] [PubMed]
- Araújo, M.G.; Lindhe, J. Dimensional ridge alterations following tooth extraction. Exp. Study Dog. J. Clin. Periodontol. 2005, 32, 212–218. [Google Scholar] [CrossRef] [PubMed]
- Farshidfar, N.; Jafarpour, D.; Firoozi, P.; Sahmeddini, S.; Hamedani, S.; de Souza, R.F.; Tayebi, L. The application of injectable platelet-rich fibrin in regenerative dentistry: A systematic scoping review of In vitro and In vivo studies. Jpn. Dent. Sci. Rev. 2022, 58, 89–123. [Google Scholar] [CrossRef] [PubMed]
- Temmerman, A.; Vandessel, J.; Castro, A.; Jacobs, R.; Teughels, W.; Pinto, N.; Quirynen, M. The use of leucocyte and platelet-rich fibrin in socket management and ridge preservation: A split-mouth, randomized, controlled clinical trial. J. Clin. Periodontol. 2016, 43, 990–999. [Google Scholar] [CrossRef]
- Castro, A.B.; Van Dessel, J.; Temmerman, A.; Jacobs, R.; Quirynen, M. Effect of different platelet-rich fibrin matrices for ridge preservation in multiple tooth extractions: A split-mouth randomized controlled clinical trial. J. Clin. Periodontol. 2021, 48, 984–995. [Google Scholar] [CrossRef]
- Al-Maawi, S.; Becker, K.; Schwarz, F.; Sader, R.; Ghanaati, S. Efficacy of platelet-rich fibrin in promoting the healing of extraction sockets: A systematic review. Int. J. Implant Dent. 2021, 7, 117. [Google Scholar] [CrossRef]
- Chappuis, V.; Engel, O.; Reyes, M.; Shahim, K.; Nolte, L.P.; Buser, D. Ridge alterations post-extraction in the esthetic zone: A 3D analysis with CBCT. J. Dent. Res. 2013, 92 (Suppl. S12), 195S–201S. [Google Scholar] [CrossRef] [Green Version]
- Avila-Ortiz, G.; Elangovan, S.; Kramer, K.W.; Blanchette, D.; Dawson, D.V. Effect of alveolar ridge preservation after tooth extraction: A systematic review and meta-analysis. J. Dent. Res. 2014, 93, 950–958. [Google Scholar] [CrossRef] [Green Version]
- Avila-Ortiz, G.; Gubler, M.; Romero-Bustillos, M.; Nicholas, C.L.; Zimmerman, M.B.; Barwacz, C.A. Efficacy of Alveolar Ridge Preservation: A Randomized Controlled Trial. J. Dent. Res. 2020, 99, 402–409. [Google Scholar] [CrossRef]
- Mardas, N.; Trullenque-Eriksson, A.; MacBeth, N.; Petrie, A.; Donos, N. Does ridge preservation following tooth extraction improve implant treatment outcomes: A systematic review: Group 4: Therapeutic concepts & methods. Clin. Oral Implant. Res. 2015, 26 (Suppl. S11), 180–201. [Google Scholar]
- Mardas, N.; Chadha, V.; Donos, N. Alveolar ridge preservation with guided bone regeneration and a synthetic bone substitute or a bovine-derived xenograft: A randomized, controlled clinical trial. Clin. Oral Implant. Res. 2010, 21, 688–698. [Google Scholar] [CrossRef] [PubMed]
- De Risi, V.; Clementini, M.; Vittorini, G.; Mannocci, A.; De Sanctis, M. Alveolar ridge preservation techniques: A systematic review and meta-analysis of histological and histomorphometrical data. Clin. Oral Implant. Res. 2015, 26, 50–68. [Google Scholar] [CrossRef] [PubMed]
- Bornstein, M.M.; Halbritter, S.; Harnisch, H.; Weber, H.P.; Buser, D. A retrospective analysis of patients referred for implant placement to a specialty clinic: Indications, surgical procedures, and early failures. Int. J. Oral Maxillofac. Implant. 2008, 23, 1109–1116. [Google Scholar]
- Borg, T.D.; Mealey, B.L. Histologic healing following tooth extraction with ridge preservation using mineralized versus combined mineralized-demineralized freeze-dried bone allograft: A randomized controlled clinical trial. J. Periodontol. 2015, 86, 348–355. [Google Scholar] [CrossRef] [PubMed]
- Méndez, C.A.; Lang, N.P.; Caneva, M.; Ramírez Lemus, G.; Mora Solano, G.; Botticelli, D. Comparison of allografts and xenografts used for alveolar ridge preservation. A clinical and histomorphometric RCT in humans. Clin. Implant Dent. Relat. Res. 2017, 19, 608–615. [Google Scholar] [CrossRef] [PubMed]
- Wilson, T.G., Jr.; Roccuzzo, M.; Ucer, C.; Beagle, J.R. Immediate placement of tapered effect (TE) implants: 5-year results of a prospective, multicenter study. Int. J. Oral Maxillofac. Implant. 2013, 28, 261–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Kesteren, C.J.; Schoolfield, J.; West, J.; Oates, T. A prospective randomized clinical study of changes in soft tissue position following immediate and delayed implant placement. Int. J. Oral Maxillofac. Implant. 2010, 25, 562–570. [Google Scholar]
- Jonker, B.P.; Strauss, F.J.; Naenni, N.; Jung, R.E.; Wolvius, E.B.; Pijpe, J. Early implant placement with or without alveolar ridge preservation in single tooth gaps renders similar esthetic, clinical and patient-reported outcome measures: One-year results of a randomized clinical trial. Clin. Oral Implant. Res. 2021, 32, 1041–1051. [Google Scholar] [CrossRef]
- Margetic, S. Inflammation and haemostasis. Biochem. Med. 2012, 22, 49–62. [Google Scholar] [CrossRef]
- Ahmed, N.; Gopalakrishna, V.; Shetty, A.; Nagraj, V.; Imran, M.; Kumar, P. Efficacy of PRF vs PRF + biodegradable collagen plug in post-extraction preservation of socket. J. Contemp. Dent. Pract. 2019, 20, 1323–1328. [Google Scholar]
- Yu, H.-C.; Huang, F.-M.; Lee, S.-S.; Yu, C.-C.; Chang, Y.-C. Effects of fibroblast growth factor-2 on cell proliferation of cementoblasts. J. Dent. Sci. 2016, 11, 463–467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zwittnig, K.; Kirnbauer, B.; Jakse, N.; Schlenke, P.; Mischak, I.; Ghanaati, S.; Al-Maawi, S.; Végh, D.; Payer, M.; Zrnc, T.A. Growth Factor Release within Liquid and Solid PRF. J. Clin. Med. 2022, 11, 5070. [Google Scholar] [CrossRef] [PubMed]
- Berglundh, T.; Lindhe, J. Healing around implants placed in bone defects treated with Bio-Oss. Exp. Study Dog. Clin. Oral Implant. Res. 1997, 8, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Hockers, T.; Abensur, D.; Valentini, P.; Legrand, R.; Hammerle, C.H. The combined use of bioresorbable membranes and xenografts or autografts in the treatment of bone defects around implants. A study in beagle dogs. Clin. Oral Implant. Res. 1999, 10, 487–498. [Google Scholar] [CrossRef] [PubMed]
- Buser, D.; Brägger, U.; Lang, N.P.; Nyman, S. Regeneration and enlargement of jaw bone using guided tissue regeneration. Clin. Oral Implant. Res. 1990, 1, 22–32. [Google Scholar] [CrossRef] [PubMed]
- Jung, R.E.; Ioannidis, A.; Hämmerle, C.H.F.; Thoma, D.S. Alveolar ridge preservation in the esthetic zone. Periodontology 2000 2018, 77, 165–175. [Google Scholar] [CrossRef] [PubMed]
- Fairbairn, P.; Leventis, M.; Mangham, C.; Horowitz, R. Alveolar Ridge Preservation Using a Novel Synthetic Grafting Material: A Case with Two-Year Follow-Up. Case Rep. Dent. 2018, 2018, 6412806. [Google Scholar] [CrossRef] [Green Version]
- Leventis, M.; Tsetsenekou, E.; Kalyvas, D. Treatment of Osseous Defects after Mandibular Third Molar Removal with a Resorbable Alloplastic Grafting Material: A Case Series with 1- to 2-Year Follow-Up. Materials 2020, 13, 4688. [Google Scholar] [CrossRef]
- Chen, S.T.; Buser, D. Clinical and esthetic outcomes of implants placed in postextraction sites. Int. J. Oral Maxillofac. Implant. 2009, 24, 186–217. [Google Scholar]
- Giudice, A.; Esposito, M.; Bennardo, F.; Brancaccio, Y.; Buti, J.; Fortunato, L. Dental extractions for patients on oral antiplatelet: A within-person randomised controlled trial comparing haemostatic plugs, advanced-platelet-rich fibrin (A-PRF+) plugs, leukocyte- and platelet-rich fibrin (L-PRF) plugs and suturing alone. Int. J. Oral Implantol. 2019, 12, 77–87. [Google Scholar]
- De Mourão, A.B.C.F.; de Mello-Machado, R.C.; Javid, K.; Moraschini, V. The use of leukocyte- and platelet-rich fibrin in the management of soft tissue healing and pain in post-extraction sockets: A randomized clinical trial. J. Cranio-Maxillofac. Surg. 2020, 48, 452–457. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Ingole, S.; Deshpande, M.; Ranadive, P.; Sharma, S.; Kazi, N.; Rajurkar, S. Influence of platelet-rich fibrin on wound healing and bone regeneration. J. Oral Biol. Craniofacial Res. 2020, 10, 385–390. [Google Scholar] [CrossRef] [PubMed]
- Srinivas, B.; Das, P.; Rana, M.M.; Qureshi, A.Q.; Vaidya, K.C.; Raziuddin, S.J.A. Wound healing and bone regeneration in postextraction sockets with and with- out platelet-rich fibrin. Ann. Maxillofac. Surg. 2018, 8, 28–34. [Google Scholar] [PubMed]
- Ustaoğlu, G.; Göller Bulut, D.; Gümüş, K. Evaluation of diferent platelet-rich concentrates effects on early soft tissue healing and socket preservation after tooth extraction. J. Stomatol. Oral Maxillofac. Surg. 2019, 121, 539–544. [Google Scholar] [CrossRef] [PubMed]
- Marenzi, G.; Riccitiello, F.; Tia, M.; di Lauro, A.; Sammartino, G. Influence of leukocyte- and platelet-rich fibrin (L-PRF) in the healing of simple postextraction sockets: A split-mouth study. BioMed Res. Int. 2015, 2015, 369273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asmael, H.M.; Jamil, F.A.; Hasan, A.M. Novel application of platelet-rich fibrin as a wound healing enhancement in extraction sockets of patients who smoke. J. Craniofac. Surg. 2018, 29, E794–E797. [Google Scholar] [CrossRef] [PubMed]
- Rutkowski, J.L.; Johnson, D.A.; Radio, N.M.; Fennell, J.W. Platelet rich plasma to facilitate wound healing following tooth extraction. J. Oral Implantol. 2010, 36, 11–23. [Google Scholar] [CrossRef]
- Thoma, D.S.; Cosyn, J.; Fickl, S.; Jensen, S.S.; Jung, R.E.; Raghoebar, G.M.; Rocchietta, I.; Roccuzzo, M.; Sanz, M.; Sanz-Sánchez, I.; et al. Soft tissue management at implants: Summary and consensus statements of group 2. The 6th EAO Consensus Conference 2021. Clin. Oral Implant. Res. 2021, 32 (Suppl. S21), 174–180. [Google Scholar] [CrossRef]
- Kalsi, A.S.; Bomfim, D.I.; Hussain, Z. Factors affecting decision making at reassessment of periodontitis. Part 4: Treatment options for residual periodontal pockets. Br. Dent. J. 2019, 227, 967–974. [Google Scholar] [CrossRef]
- Fernandes, G.; Yang, S. Application of platelet-rich plasma with stem cells in bone and periodontal tissue engineering. Bone Res. 2016, 4, 16036. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.J.; Ben Amara, H.; Chung, I.; Koo, K.T. Compromised extraction sockets: A new classification and prevalence involving both soft and hard tissue loss. J. Periodontal Implant Sci. 2021, 51, 100–113. [Google Scholar] [CrossRef] [PubMed]
- Pesce, P.; Mijiritsky, E.; Canullo, L.; Menini, M.; Caponio, V.C.A.; Grassi, A.; Gobbato, L.; Baldi, D. An Analysis of Different Techniques Used to Seal Post-Extractive Sites—A Preliminary Report. Dent. J. 2022, 10, 189. [Google Scholar] [CrossRef]
- Darby, I.; Chen, S.T.; Buser, D. Ridge preservation techniques for implant therapy. Int. J. Oral Maxillofac. Implant. 2009, 24, 260–271. [Google Scholar]
- Pesce, P.; Menini, M.; Canullo, L.; Khijmatgar, S.; Modenese, L.; Gallifante, G.; Del Fabbro, M. Radiographic and Histomorphometric Evaluation of Biomaterials Used for Lateral Sinus Augmentation: A Systematic Review on the Effect of Residual Bone Height and Vertical Graft Size on New Bone Formation and Graft Shrinkage. J. Clin. Med. 2021, 10, 4996. [Google Scholar] [CrossRef] [PubMed]
- Canullo, L.; Rossi-Fedele, G.; Camodeca, F.; Menini, M.; Pesce, P. A Pilot Retrospective Study on the Effect of Bone Grafting after Wisdom Teeth Extraction. Materials 2021, 14, 2844. [Google Scholar] [CrossRef] [PubMed]
- Baldi, D.; Menini, M.; Pera, F.; Ravera, G.; Pera, P. Sinus floor elevation using osteotomes or piezoelectric surgery. Int. J. Oral Maxillofac. Surg. 2011, 40, 497–503. [Google Scholar] [CrossRef] [PubMed]
- Barootchi, S.; Wang, H.L.; Ravida, A.; Ben Amor, F.; Riccitiello, F.; Rengo, C.; Paz, A.; Laino, L.; Marenzi, G.; Gasparro, R.; et al. Ridge preservation techniques to avoid invasive bone reconstruction: A systematic review and meta-analysis: Naples Consensus Report Working Group C. Int. J. Oral Implantol. 2019, 12, 399–416. [Google Scholar]
- Horváth, A.; Mardas, N.; Mezzomo, L.A.; Needleman, I.G.; Donos, N. Alveolar ridge preservation. Syst. Rev. Clin. Oral Investig. 2013, 17, 341–363. [Google Scholar] [CrossRef]
- Baldi, D.; Pesce, P.; Musante, B.; Pera, F.; Fulcheri, E.; Romano, F.; Menini, M. Radiological and Histomorphometric Outcomes of Homologous Bone Graft in Postextractive Implant Sites: A 6-Year Retrospective Analysis. Implant Dent. 2019, 28, 472–477. [Google Scholar] [CrossRef]
- Ghanaati, S.; Herrera-Vizcaino, C.; Al-Maawi, S.; Lorenz, J.; Miron, R.J.; Nelson, K.; Schwarz, F.; Choukroun, J.; Sader, R. Fifteen Years of Platelet Rich Fibrin in Dentistry and Oromaxillofacial Surgery: How High is the Level of Scientific Evidence? J. Oral Implantol. 2018, 44, 471–492. [Google Scholar] [CrossRef]
- Tischler, M.; Misch, C.E. Extraction site bone grafting in general dentistry. Review of applications and principles. Dent. Today 2004, 23, 108–113. [Google Scholar] [PubMed]
- Miron, R.J.; Zucchelli, G.; Pikos, M.A.; Salama, M.; Lee, S.; Guillemette, V.; Fujioka-Kobayashi, M.; Bishara, M.; Zhang, Y.; Wang, H.L.; et al. Use of platelet-rich fibrin in regenerative dentistry: A systematic review. Clin. Oral Investig. 2017, 21, 1913–1927. [Google Scholar] [CrossRef] [PubMed]
- Becker, W.; Clokie, C.; Sennerby, L.; Urist, M.R.; Becker, B.E. Histologic findings after implantation and evaluation of different grafting materials and titanium micro screws into extraction sockets: Case reports. J. Periodontol. 1998, 69, 414–421. [Google Scholar] [CrossRef]
- Nevins, M.; Camelo, M.; De Paoli, S.; Friedland, B.; Schenk, R.K.; Parma-Benfenati, S.; Simion, M.; Tinti, C.; Wagenberg, B. A study of the fate of the buccal wall of extraction sockets of teeth with prominent roots. Int. J. Periodontics Restor. Dent. 2006, 26, 19–29. [Google Scholar] [CrossRef]
- Araújo, M.G.; da Silva, J.C.C.; de Mendonça, A.F.; Lindhe, J. Ridge alterations following grafting of fresh extraction sockets in man. Randomized Clin. Trial. Clin. Oral Implant. Res. 2015, 26, 407–412. [Google Scholar] [CrossRef] [PubMed]
- Adams, R.J. Is there clinical evidence to support alveolar ridge preservation over extraction alone? A review of recent literature and case reports of late graft failure. Br. Dent. J. 2022, 233, 469–474. [Google Scholar] [CrossRef] [PubMed]
- Ranganathan, M.; Balaji, M.; Krishnaraj, R.; Narayanan, V.; Thangavelu, A. Assessment of Regeneration of Bone in the Extracted Third Molar Sockets Augmented Using Xenograft (CollaPlugTN Zimmer) in Comparison with the Normal Healing on the Contralateral Side. J. Pharm. Bioallied Sci. 2017, 9 (Suppl. 1), S180–S186. [Google Scholar] [CrossRef] [PubMed]
- Cornelini, R.; Cangini, F.; Martuscelli, G.; Wennström, J. Deproteinized bovine bone and biodegradable barrier membranes to support healing following immediate placement of transmucosal implants: A short-term controlled clinical trial. Int. J. Periodontics Restor. Dent. 2004, 24, 555–563. [Google Scholar]
- Chen, S.T.; Darby, I.B.; Reynolds, E.C. A prospective clinical study of non-submerged immediate implants: Clinical outcomes and esthetic results. Clin. Oral Implant. Res. 2007, 18, 552–562. [Google Scholar] [CrossRef]
- Kalsi, A.S.; Kalsi, J.S.; Bassi, S. Alveolar ridge preservation: Why, when and how. Br. Dent. J. 2019, 227, 264–274. [Google Scholar] [CrossRef]
- Sisti, A.; Canullo, L.; Mottola, M.P.; Covani, U.; Barone, A.; Botticelli, D. Clinical evaluation of a ridge augmentation procedure for the severely resorbed alveolar socket: Multicenter randomized controlled trial, preliminary results. Clin. Oral Implant. Res. 2012, 23, 526–535. [Google Scholar] [CrossRef] [PubMed]
- Amin, V.; Kumar, S.; Joshi, S.; Hirani, T.; Shishoo, D. A clinical and radiographical comparison of buccolingual crestal bone changes after immediate and delayed implant placement. Med. Pharm. Rep. 2019, 92, 401–407. [Google Scholar] [CrossRef]
- Tabrizi, R.; Mohajerani, H.; Ardalani, B.; Khiabani, K. Does preservation of the socket decrease marginal bone loss in the mandible after extraction of first molars? Br. J. Oral Maxillofac. Surg. 2019, 57, 886–890. [Google Scholar] [CrossRef] [PubMed]
- Vittorini Orgeas, G.; Clementini, M.; De Risi, V.; de Sanctis, M. Surgical techniques for alveolar socket preservation: A systematic review. Int. J. Oral Maxillofac. Implant. 2013, 28, 1049–1061. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leventis, M.D.; Fairbairn, P.; Kakar, A.; Leventis, A.D.; Margaritis, V.; Lückerath, W.; Horowitz, R.A.; Rao, B.H.; Lindner, A.; Nagursky, H. Minimally Invasive Alveolar Ridge Preservation Utilizing an In Situ Hardening β-Tricalcium Phosphate Bone Substitute: A Multicenter Case Series. Int. J. Dent. 2016, 2016, 5406736. [Google Scholar] [CrossRef] [Green Version]
- Avila-Ortiz, G.; Chambrone, L.; Vignoletti, F. Effect of alveolar ridge preservation interventions following tooth extraction: A systematic review and meta-analysis. J. Clin. Periodontol. 2019, 46 (Suppl. S21), 195–223, Erratum in J. Clin. Periodontol. 2020, 47, 129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barone, A.; Ricci, M.; Tonelli, P.; Santini, S.; Covani, U. Tissue changes of extraction sockets in humans: A comparison of spontaneous healing vs. ridge preservation with secondary soft tissue healing. Clin. Oral Implant. Res. 2013, 24, 1231–1237. [Google Scholar] [CrossRef]
- Vignoletti, F.; Matesanz, P.; Rodrigo, D.; Figuero, E.; Martin, C.; Sanz, M. Surgical protocols for ridge preservation after tooth extraction. A systematic review. Clin. Oral Implants Res. 2012, 23 (Suppl. S5), 22–38. [Google Scholar] [CrossRef]
- Leventis, M.D.; Fairbairn, P.; Horowitz, R.A. Extraction site preservation using an in-situ hardening alloplastic bone graft substitute. Compend. Contin. Educ. Dent. 2014, 35 (Suppl. S4), 11–13. [Google Scholar]
- Schwarz, F.; Herten, M.; Sager, M.; Bieling, K.; Sculean, A.; Becker, J. Comparison of naturally occurring and ligature-induced peri-implantitis bone defects in humans and dogs. Clin. Oral Implant. Res. 2007, 18, 161–170. [Google Scholar] [CrossRef]
- Keith, J.D., Jr.; Salama, M.A. Ridge preservation and augmentation using regenerative materials to enhance implant predictability and esthetics. Compend. Contin. Educ. Dent. 2007, 28, 614–624. [Google Scholar]
- Yu, H.Y.; Chang, Y.C. A Bibliometric Analysis of Platelet-Rich Fibrin in Dentistry. Int. J. Environ. Res. Public Health 2022, 19, 12545. [Google Scholar] [CrossRef]
- Wang, X.; Zhang, Y.; Choukroun, J.; Ghanaati, S.; Miron, R.J. Effects of an injectable platelet-rich fibrin on osteoblast behavior and bone tissue formation in comparison to platelet-rich plasma. Platelets 2018, 29, 48–55. [Google Scholar] [CrossRef]
- Jambhekar, S.; Kernen, F.; Bidra, A.S. Clinical and histologic outcomes of socket grafting after flapless tooth extraction: A systematic review of randomized controlled clinical trials. J. Prosthet. Dent. 2015, 113, 371–382. [Google Scholar] [CrossRef]
- Quirynen, M.; Pinto, N.R. Leukocyte- and Platelet-Rich Fibrin in Oral Regenerative Procedures: Evidence-Based Clinical Guidelines; Quintessenz Verlag: München, Germany, 2022. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Strategy for Management of Tooth Loss | Immediate Implant Placement in Fresh Extraction Sites | Socket Augmentation (with or without PRF) (+/−Connective Tissue Graft) |
|---|---|---|
| Criteria 1 | Tooth socket intact with >2 mm labial wall thickness | Tooth socket with >50% missing labial wall height |
| Criteria 2 | Primary stability is possible in optimum 3D prosthodontically driven implant trajectory | Tooth socket with <1 mm labial wall thickness |
| Criteria 3 | Thick soft tissue biotype | Poor soft tissue biotype (e.g., thin/non-keratinised/mobile mucosa), unfavourable smile line |
| Factors That Affect Socket Augmentation Treatment | |
|---|---|
| 1 | Presence of infection (e.g., large cystic lesion) |
| 2 | Inability to achieve primary stability in the restoratively driven position |
| 3 | Presence of a damaged alveolus (including thin buccal socket wall) |
| 4 | Periodontal phenotype |
| 5 | Aesthetic demands |
| 6 | Systemic conditions |
| Study | Design | Patient Numbers | Teeth Extracted/Region | PRF Type | RPM (RCF [xg]) and Centrifuge Time | Bone Regeneration | Soft Tissue Healing |
|---|---|---|---|---|---|---|---|
| Ahmed et al. [30] | Parallel RCT | 54 | Not reported | L-PRF | 3000 rpm for 10 min | Radiographic analysis (bone height reduction, crest to tip of root taking adjoining tooth as a guide) after 16 weeks | Wound healing index, resulted in spontaneous healing |
| Asmael et al. [46] | Split mouth RCT | 20 | All regions | PRF | 3000 rpm for 10 min | Not reported | Percentage of epithelization after 1 week 52.7% and 51.3%, the Landry wound healing index, resulted in spontaneous healing |
| Giudice et al. [40] | Split mouth RCT | 40 | All regions | A-PRF+ | 2700 rpm for 18 min | Not reported | Wound healing index, resulted in spontaneous healing |
| Marenzi et al. [45] | Split mouth RCT | 26 | Canines, premolars, and molars | L-PRF | 2700 rpm for 12 min | Not reported | Wound healing index, resulted in spontaneous healing |
| Mourão et al. [41] | Parallel RCT | 32 | Molars and premolars | L-PRF | 3000 rpm for 12 min | Not reported | Wound healing index, resulted in spontaneous healing |
| Sharma et al. [42] | Split mouth RCT | 30 | Not reported | PRF | 3000 rpm for 10 min | Digital panoramic radiographs after 16 weeks | The Landry healing index, resulted in spontaneous healing |
| Srinivas et al. [43] | CCT split mouth | 30 | Maxilla and mandible | L-PRF | 3000 rpm for 10 min | CBCT(bone density 24 h, p < 0.001 | Wound healing index, resulted in spontaneous healing |
| Ustaoğlu et al. [44] | Parallel RCT | 57 | Single rooted tooth | L-PRF | 2700 rpm for 12 min | Not reported | The Landry healing index, resulted in spontaneous healing |
| Step 1 | Assess alveolar ridge condition and morphology clinically and radiologically
|
| Step 2 | Extract using minimally invasive technique and clean and irrigate the extraction socket
|
| Step 3 | Augment and suture
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ucer, C.; Khan, R.S. Extraction Socket Augmentation with Autologous Platelet-Rich Fibrin (PRF): The Rationale for Socket Augmentation. Dent. J. 2023, 11, 196. https://doi.org/10.3390/dj11080196
Ucer C, Khan RS. Extraction Socket Augmentation with Autologous Platelet-Rich Fibrin (PRF): The Rationale for Socket Augmentation. Dentistry Journal. 2023; 11(8):196. https://doi.org/10.3390/dj11080196
Chicago/Turabian StyleUcer, Cemal, and Rabia S. Khan. 2023. "Extraction Socket Augmentation with Autologous Platelet-Rich Fibrin (PRF): The Rationale for Socket Augmentation" Dentistry Journal 11, no. 8: 196. https://doi.org/10.3390/dj11080196