
Coronal Repercussions of the Maxillary Central Incisor Torque in the First Set of Aligners: A Retrospective Study


Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Materials: Participants of the Clinical Study and Selection Criteria
- -
- Individuals with definitive dentition undergoing orthodontic treatment with clear aligners;
- -
- Individuals who had already completed, in full, the first series of orthodontic treatment with aesthetic aligners without misfits;
- -
- Individuals with available and complete cephalometric analysis;
- -
- Patients who presented, in the programmed table of movements taken from the Invisalign Doctor Site®, coronal inclination movements of maxillary central incisors above 5°.
- -
- Individuals who had temporary teeth;
- -
- Individuals whose records were incomplete;
- -
- Individuals with cognitive or neurological disorders, with identified syndromes, history of trauma and/or tumors in the head and neck and metabolic diseases that affect the joints and/or muscles;
- -
- Individuals who were being treated with anti-inflammatory drugs, analgesics or psychiatric medication.
- -
- Intra-oral scanner (Itero® Element 5D Plus, Align Technology, Tempe, AZ, USA);
- -
- Itero® software version 1.34.0.3 (Align Technology, Tempe, AZ, USA);
- -
- Tables and Clincheck Pro® 6.0 software (AlignTech, Santa Monica, CA, USA);
- -
- Orthodontic and clinical patient reports;
- -
- Geomagic® Control X TM version 2022.1.0 (OQTON, X3D).
- -
- Microsoft Excel version 16.75.2;
- -
- IBM® SPSS® version 29.0.
2.3. Ethical Principals
2.4. Methods
- -
- For pro-inclination ⇒ TP = T0 + Tooth movement planned value on platform.
- -
- For retro-inclination ⇒ TP = T0 − Tooth movement planned value on platform.
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Clinical Study Sample
3.2. Efficacy and Predictability of Coronal Repercussions of Maxillary Central Incisor Torque
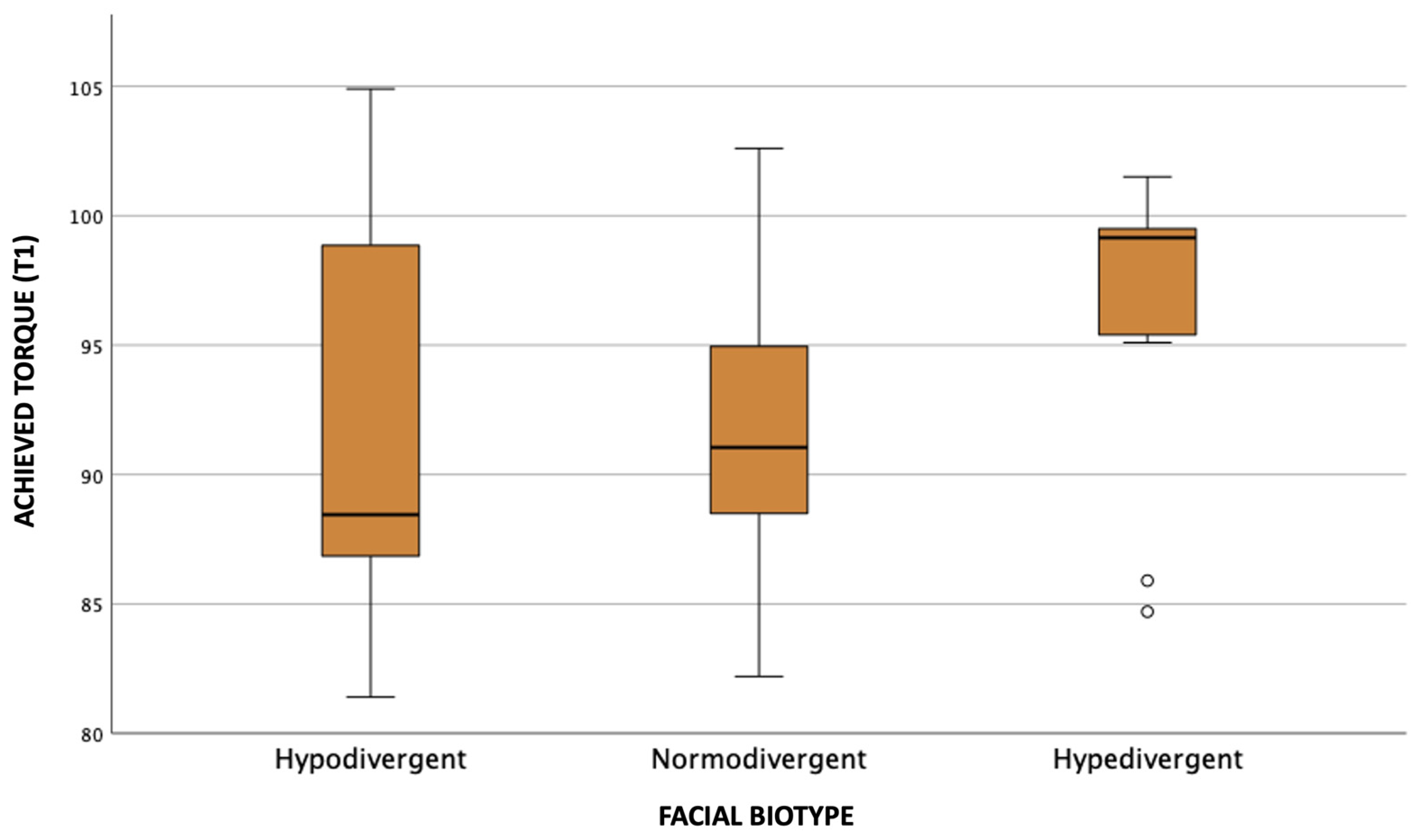
3.3. Influence of Different Facial Biotypes on Coronal Repercussions of the Maxillary Central Incisor Torque
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Grünheid, T.; Loh, C.; Larson, B.E. How accurate is Invisalign in nonextraction cases? Are predicted tooth positions achieved? Angle Orthod. 2017, 87, 809–815. [Google Scholar] [CrossRef] [PubMed]
- Gaddam, R.; Freer, E.; Kerr, B.; Weir, T. Reliability of torque expression by the invisalign® appliance: A retrospective study. Australas. Orthod. J. 2021, 37, 3–13. [Google Scholar] [CrossRef]
- Sabbagh, H.; Heger, S.M.; Stocker, T.; Baumert, U.; Wichelhaus, A.; Hoffmann, L. Accuracy of 3D Tooth Movements in the Fabrication of Manual Setup Models for Aligner Therapy. Materials 2022, 15, 3853. [Google Scholar] [CrossRef] [PubMed]
- Bichu, Y.M.; Alwafi, A.; Liu, X.; Andrews, J.; Ludwig, B.; Bichu, A.Y.; Zou, B. Advances in orthodontic clear aligner materials. Bioact. Mater. 2023, 22, 384–403. [Google Scholar] [CrossRef] [PubMed]
- Al-Nadawi, M.; Kravitz, N.D.; Hansa, I.; Makki, L.; Ferguson, D.J.; Vaid, N.R. Effect of clear aligner wear protocol on the efficacy of tooth movement: A randomized clinical trial. Angle Orthod. 2021, 91, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Long, H.; Wu, Z.; Yan, X.; Wang, Q.; Liu, L.; Wang, Y.; Jian, F.; Liao, L.; Li, X.; Lai, W. An objective system for appraising clear aligner treatment difficulty: Clear aligner treatment complexity assessment tool (CAT–CAT). BMC Oral Health 2020, 20, 312. [Google Scholar] [CrossRef]
- Bilello, G.; Fazio, M.; Amato, E.; Crivello, L.; Galvano, A.; Currò, G. Accuracy evaluation of orthodontic movements with aligners: A prospective observational study. Prog. Orthod. 2022, 23, 12. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Liu, X.; Chen, X.; Li, X.; Fang, S.; Wang, W.; Ma, Y.; Jin, Z. The three-dimensional displacement tendency of teeth depending on incisor torque compensation with clear aligners of different thicknesses in cases of extraction: A finite element study. BMC Oral Health 2022, 22, 499. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Zhan, Q.; Zhou, J.; Kuang, Q.; Yan, X.; Zhang, X.; Shan, Y.; Li, X.; Lai, W.; Long, H. Effectiveness of an anterior mini-screw in achieving incisor intrusion and palatal root torque for anterior retraction with clear aligners. Angle Orthod. 2021, 91, 794–803. [Google Scholar] [CrossRef] [PubMed]
- Ke, Y.; Zhu, Y.; Zhu, M. A comparison of treatment effectiveness between clear aligner and fixed appliance therapies. BMC Oral Health. 2019, 19, 24. [Google Scholar] [CrossRef] [PubMed]
- Tepedino, M.; Paoloni, V.; Cozza, P.; Chimenti, C. Movement of anterior teeth using clear aligners: A three-dimensional, retrospective evaluation. Prog. Orthod. 2018, 19, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonçalves, A.; Collard, A.; Monteiro, F.; Matos, D.; Carvalho, Ó.; Azevedo, R.; Silva, F.S.; Pinho, T. Accuracy of Invisalign® on Upper Incisors: A Systematic Review. Turkish J. Orthod. 2023, 36, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Pithon, M.M.; Baião, F.C.S.; Anna, L.I.D.d.A.S.; Paranhos, L.R.; Maia, L.C. Assessment of the effectiveness of invisible aligners compared with conventional appliance in aesthetic and functional orthodontic treatment: A systematic review. J. Investig. Clin. Dent. 2019, 10, e12455. [Google Scholar] [CrossRef] [PubMed]
- Bowman, E.; Bowman, P.; Weir, T.; Dreyer, C.W.; Meade, M.J. Evaluation of the predicted vs. achieved occlusal outcomes with the Invisalign® appliance: A retrospective investigation of adult patients. Int. Orthod. 2023, 21, 100746. [Google Scholar] [CrossRef] [PubMed]
- Bou Assi, S.; Macari, A.; Hanna, A.; Tarabay, R.; Salameh, Z. Cephalometric evaluation of maxillary incisors inclination, facial, and growth axes in different vertical and sagittal patterns: An original study. J. Int. Soc. Prevent. Communit. Dent. 2020, 10, 292–299. [Google Scholar] [CrossRef] [PubMed]
- Castroflorio, T.; Garino, F.; Lazzaro, A.; Debernardi, C. Upper-incisor root control with Invisalign appliances. J. Clin. Orthod. 2013, 47, 346–351. [Google Scholar] [PubMed]
- Dai, F.F.; Xu, T.M.; Shu, G. Comparison of achieved and predicted tooth movement of maxillary first molars and central incisors: First premolar extraction treatment with Invisalign. Angle Orthod. 2019, 89, 679–687. [Google Scholar] [CrossRef] [PubMed]
- Simon, M.; Keilig, L.; Schwarze, J.; Jung, B.A.; Bourauel, C. Treatment outcome and efficacy of an aligner technique—Regarding incisor torque, premolar derotation and molar distalization. BMC Oral Health 2014, 14, 68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chisari, J.R.; McGorray, S.P.; Nair, M.; Wheeler, T.T. Variables affecting orthodontic tooth movement with clear aligners. Am. J. Orthod. Dentofac. Orthop. 2014, 145 (Suppl. S4), S82–S91. [Google Scholar] [CrossRef] [PubMed]
- Alwafi, A.A.; Hannam, A.G.; Yen, E.H.; Zou, B. A new method assessing predicted and achieved mandibular tooth movement in adults treated with clear aligners using CBCT and individual crown superimposition. Sci. Rep. 2023, 13, 4084. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Definition | Frequency (Number) | Percentage (%) |
|---|---|---|---|
| Overjet | Decreased (<0 mm) | 2 | 7.4 |
| Normal (2.5 ± 2.5 mm) | 21 | 77.8 | |
| Increased (>5 mm) | 4 | 14.8 | |
| Overbite | Decreased (<0.5 mm) | 2 | 7.4 |
| Normal (2.5 ± 2 mm) | 9 | 33.3 | |
| Increased (>4.5 mm) | 16 | 59.3 |
| Variable | Definition | Frequency (Number) | Percentage (%) |
|---|---|---|---|
| Complexity of the case | Simple | 0 | 0 |
| Moderate | 19 | 70 | |
| Complex | 8 | 30 |
| Sample | Moment | Mean ± SD | z | p-Value |
|---|---|---|---|---|
| Proinclination | T0 | 83.6 ± 7.3 | −5.571 | <0.001 * |
| T1 | 91.9 ± 6.4 | |||
| Retroinclination | T0 | 101.0 ± 3.9 | −2.903 | 0.004 * |
| T1 | 96.4 ± 3.6 |
| Sample | Moment | Mean ± SD | z | p-Value |
|---|---|---|---|---|
| Pro-inclination | T1 | 91.9 ± 6.4 | −2.707 | 0.007 * |
| TP | 95.4 ± 5.3 | |||
| Retro-inclination | T1 | 96.4 ± 3.6 | −1.295 | 0.195 |
| TP | 94.3 ± 3.8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oliveira, A.C.; Rocha, A.S.; Leitão, R.; Maia, M.; Pinho, T. Coronal Repercussions of the Maxillary Central Incisor Torque in the First Set of Aligners: A Retrospective Study. Dent. J. 2023, 11, 186. https://doi.org/10.3390/dj11080186
Oliveira AC, Rocha AS, Leitão R, Maia M, Pinho T. Coronal Repercussions of the Maxillary Central Incisor Torque in the First Set of Aligners: A Retrospective Study. Dentistry Journal. 2023; 11(8):186. https://doi.org/10.3390/dj11080186
Chicago/Turabian StyleOliveira, Ana Catarina, Ana Sofia Rocha, Rita Leitão, Manuela Maia, and Teresa Pinho. 2023. "Coronal Repercussions of the Maxillary Central Incisor Torque in the First Set of Aligners: A Retrospective Study" Dentistry Journal 11, no. 8: 186. https://doi.org/10.3390/dj11080186