

Dental Pulp Response to Silver-Containing Solutions: A Scoping Review



Abstract
:1. Introduction
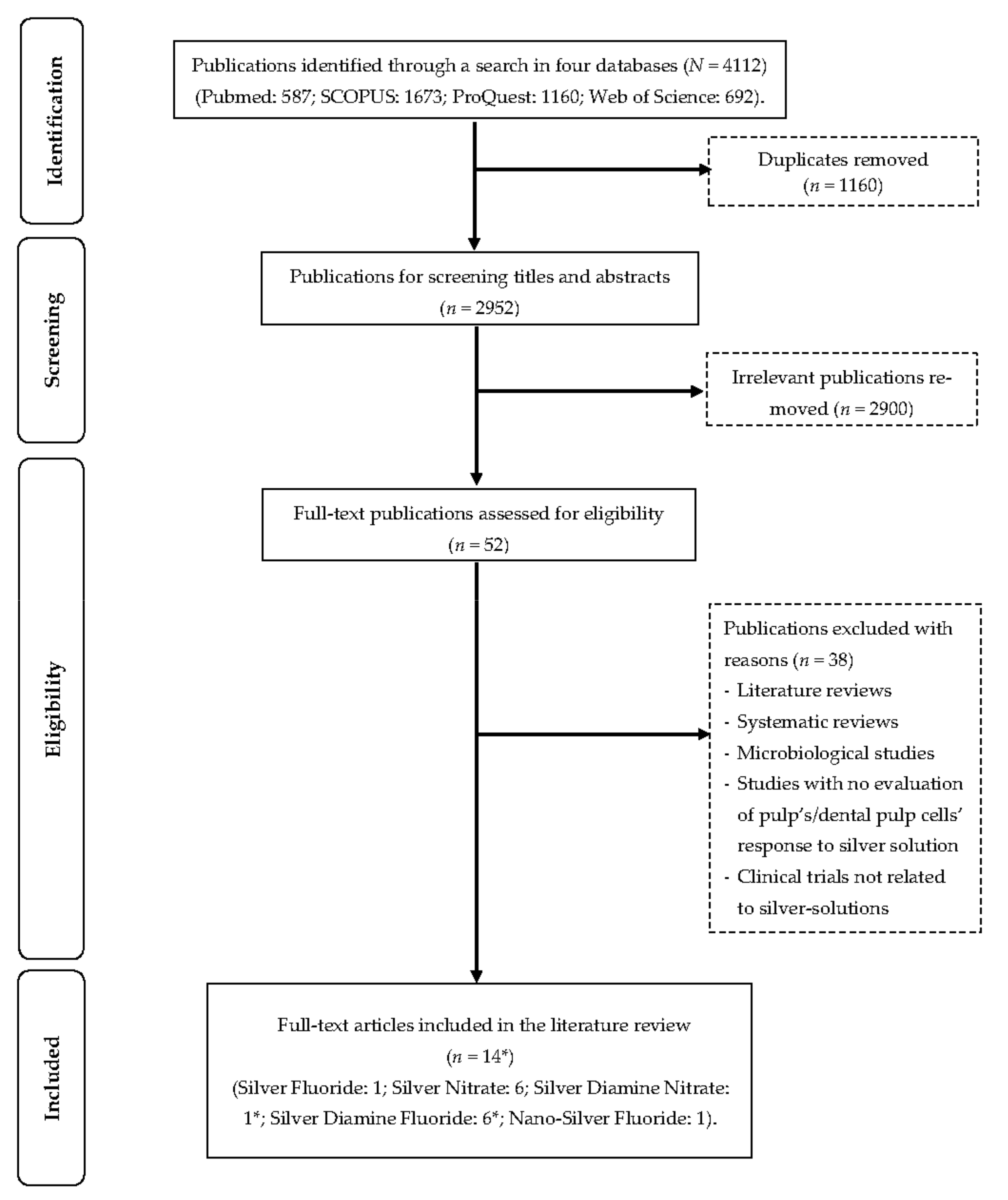
2. Materials and Methods
3. Silver-Containing Solutions for Deep Caries Management
3.1. Silver Fluoride
3.2. Silver Nitrate
3.3. Silver Diamine Nitrate
3.4. Silver Diamine Fluoride
3.5. Nano Silver Fluoride

{kind=link}
| Solution [Ref.] | Wt.% (Concentration According to Manufacturer(s)) | Anticaries Properties |
|---|---|---|
| Silver fluoride [40,42] | 40% (Ag: 340,000 ppm; F: 60,000 ppm) |
|
| Silver nitrate [77] | 25% (Ag: 151,130 ppm) |
|
| Silver diamine nitrate [33] | 48% (Ag: 319,914 ppm *) |
|
| Silver diamine fluoride [78] | 12% (Ag: 80,170 ppm; F: 14,150 ppm) |
|
| 30% (Ag: 200,400 ppm; F: 35,400 ppm) | ||
| 38% (Ag: 253,900 ppm; F: 44,800 ppm) | ||
| Nano-silver fluoride [39] | 1.05% * (Ag: 399.33 ppm; F: 10,147 ppm) |
|
4. Dental Pulpal Response to Silver-Containing Solutions
4.1. Silver Fluoride
4.2. Silver Nitrate
4.3. Silver Diamine Nitrate
4.4. Silver Diamine Fluoride
4.5. Nano Silver Fluoride
5. Limitation
6. Summary
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zaeneldin, A.; Yu, O.Y.; Chu, C.-H. Effect of silver diamine fluoride on vital dental pulp: A systematic review. J. Dent. 2022, 119, 104066. [Google Scholar] [CrossRef]
- Nyvad, B.; Fejerskov, O. Assessing the stage of caries lesion activity on the basis of clinical and microbiological examination. Community Dent. Oral Epidemiol. 1997, 25, 69–75. [Google Scholar] [CrossRef]
- Bjørndal, L.; Fransson, H.; Bruun, G.; Markvart, M.; Kjældgaard, M.; Näsman, P.; Hedenbjörk-Lager, A.; Dige, I.; Thordrup, M. Randomized Clinical Trials on Deep Carious Lesions: 5-Year Follow-up. J. Dent. Res. 2017, 96, 747–753. [Google Scholar] [CrossRef]
- Ricketts, D.; Innes, N.; Schwendicke, F. Selective Removal of Carious Tissue. Monogr. Oral Sci. 2018, 27, 82–91. [Google Scholar] [CrossRef] [PubMed]
- Schwendicke, F.; Göstemeyer, G. Understanding dentists’ management of deep carious lesions in permanent teeth: A systematic review and meta-analysis. Implement. Sci. 2016, 11, 142. [Google Scholar] [CrossRef]
- Jurasic, M.M.; Gillespie, S.; Sorbara, P.; Clarkson, J.; Ramsay, C.; Nyongesa, D.; McEdward, D.; Gilbert, G.H.; Vollmer, W.M.; National Dental PBRN Collaborative Group. Deep caries removal strategies: Findings from The National Dental Practice-Based Research Network. JADA J. Am. Dent. Assoc. 2022, 153, 1078–1088.e7. [Google Scholar] [CrossRef] [PubMed]
- Osborne, J.; Summitt, J. Extension for prevention: Is it relevant today? Am. J. Dent. 1998, 11, 189–196. [Google Scholar] [PubMed]
- Banerjee, A.; Watson, T.; Kidd, E. Dentine Caries: Take It or Leave It? Dent. Update 2000, 27, 272–276. [Google Scholar] [CrossRef] [PubMed]
- Fusayama, T. Two layers of carious dentin; diagnosis and treatment. Oper. Dent. 1979, 4, 63–70. [Google Scholar]
- Takahashi, N.; Nyvad, B. Ecological Hypothesis of Dentin and Root Caries. Caries Res. 2016, 50, 422–431. [Google Scholar] [CrossRef]
- Cate, J.M.T. Remineralization of Caries Lesions Extending into Dentin. J. Dent. Res. 2001, 80, 1407–1411. [Google Scholar] [CrossRef] [PubMed]
- Silva, N.; Carvalho, R.; Pegoraro, L.; Tay, F.; Thompson, V.P. Evaluation of a Self-limiting Concept in Dentinal Caries Removal. J. Dent. Res. 2006, 85, 282–286. [Google Scholar] [CrossRef] [PubMed]
- Hesse, D.; Bonifácio, C.C.; Mendes, F.M.; Braga, M.M.; Imparato, J.C.P.; Raggio, D.P. Sealing versus partial caries removal in primary molars: A randomized clinical trial. BMC Oral Health 2014, 14, 58. [Google Scholar] [CrossRef]
- Spadaro, J.A.; Webster, D.A.; Becker, R.O. Silver polymethyl methacrylate antibacterial bone cement. Clin. Orthop. Relat. Res. 1979, 143, 266–270. [Google Scholar] [CrossRef]
- Barillo, D.J.; Marx, D.E. Silver in medicine: A brief history BC 335 to present. Burns 2014, 40 (Suppl. 1), S3–S8. [Google Scholar] [CrossRef] [PubMed]
- Moyer, C.; Brentano, L.; Gravens, D.; Margraf, H.; Monafo, W. Treatment of large human burns with 0.5% silver nitrate solution. Arch. Surg. 1965, 90, 812–867. [Google Scholar] [CrossRef]
- Rosenblatt, A.; Stamford, T.; Niederman, R. Silver Diamine Fluoride: A Caries “Silver-Fluoride Bullet”. J. Dent. Res. 2009, 88, 116–125. [Google Scholar] [CrossRef]
- Sorkhdini, P.; Crystal, Y.O.; Tang, Q.; Lippert, F. The effect of silver diamine fluoride in preventing in vitro primary coronal caries under pH-cycling conditions. Arch. Oral Biol. 2020, 121, 104950. [Google Scholar] [CrossRef]
- Sorkhdini, P.; Crystal, Y.O.; Tang, Q.; Lippert, F. The effect of silver diamine fluoride on the remineralization of early enamel carious lesions under pH-cycling conditions. JADA Found. Sci. 2022, 1, 100006. [Google Scholar] [CrossRef]
- Jung, W.K.; Koo, H.C.; Kim, K.W.; Shin, S.; Kim, S.H.; Park, Y.H. Antibacterial Activity and Mechanism of Action of the Silver Ion in Staphylococcus aureus and Escherichia coli. Appl. Environ. Microbiol. 2008, 74, 2171–2178. [Google Scholar] [CrossRef]
- Furr, J.; Russell, A.; Turner, T.; Andrews, A. Antibacterial activity of Actisorb Plus, Actisorb and silver nitrate. J. Hosp. Infect. 1994, 27, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Richards, R.M.; Odelola, H.A.; Anderson, B. Effect of silver on whole cells and spheroplasts of a silver resistant Pseudomonas aeruginosa. Microbios 1984, 39, 151–157. [Google Scholar] [PubMed]
- Thurman, R.B.; Gerba, C.P.; Bitton, G. The molecular mechanisms of copper and silver ion disinfection of bacteria and viruses. Crit. Rev. Environ. Control 1989, 18, 295–315. [Google Scholar] [CrossRef]
- Seifo, N.; Robertson, M.; MacLean, J.; Blain, K.; Grosse, S.; Milne, R.; Seeballuck, C.; Innes, N. The use of silver diamine fluoride (SDF) in dental practice. Br. Dent. J. 2020, 228, 75–81. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Gotjamanos, T. Pulp response in primary teeth with deep residual caries treated with silver fluoride and glass ionomer cement (‘atraumatic’ technique). Aust. Dent. J. 1996, 41, 328–334. [Google Scholar] [CrossRef]
- Zander, H.; Burrill, D.Y. The Penetration of Silver Nitrate Solution into Dentin. J. Dent. Res. 1943, 22, 85–89. [Google Scholar] [CrossRef]
- Zander, H.; Smith, H. Penetration of Silver Nitrate Into Dentin II. J. Dent. Res. 1945, 24, 121–128. [Google Scholar] [CrossRef]
- Perreault, J.G.; Massler, M.; Schour, I. Reaction of odontoblasts to medicaments placed in cavity preparations in rat incisors. J. Am. Dent. Assoc. 1956, 52, 533–554. [Google Scholar] [CrossRef]
- Englander, H.R.; James, V.E.; Massler, M. Histologic effects of silver nitrate on human dentin and pulp. J. Am. Dent. Assoc. 1958, 57, 621–630. [Google Scholar] [CrossRef]
- Seltzer, S.; Bender, I.; Kaufman, I.J. Histologic changes in dental pulps of dogs and monkeys following application of pressure, drugs, and microorganisms on prepared cavities. Oral Surg. Oral Med. Oral Pathol. 1961, 14, 327–346. [Google Scholar] [CrossRef] [PubMed]
- Seltzer, S.; Bender, I.; Kaufman, I.J. Histologic changes in dental pulps of dogs and monkeys following application of pressure, drugs, and microorganisms on prepared cavities: Part II. Changes observable more than one month after Application of Traumatic Agents. Oral Surg. Oral Med. Oral Pathol. 1961, 14, 856–867. [Google Scholar] [CrossRef] [PubMed]
- Srisomboon, S.; Kettratad, M.; Stray, A.; Pakawanit, P.; Rojviriya, C.; Patntirapong, S.; Panpisut, P. Effects of Silver Diamine Nitrate and Silver Diamine Fluoride on Dentin Remineralization and Cytotoxicity to Dental Pulp Cells: An In Vitro Study. J. Funct. Biomater. 2022, 13, 16. [Google Scholar] [CrossRef] [PubMed]
- Hosoya, Y.; Aritomi, K.; Goto, G. Pulpal response to diammine silver fluoride. (2). Application on exposed pulps. Shoni Shikagaku Zasshi 1990, 28, 327–337. [Google Scholar] [PubMed]
- Shah, N.; Korwar, A.; Sharma, S.; Logani, A. Pulp response to high fluoride releasing glass ionomer, silver diamine fluoride, and calcium hydroxide used for indirect pulp treatment: An in-vivo comparative study. Contemp. Clin. Dent. 2015, 6, 288–292. [Google Scholar] [CrossRef]
- Rossi, G.; Squassi, A.; Mandalunis, P.; Kaplan, A. Effect of silver diamine fluoride (SDF) on the dentin-pulp complex: Ex vivo histological analysis on human primary teeth and rat molars. Acta Odontol. Latinoam. 2017, 30, 5–12. [Google Scholar]
- Bimstein, E.; Damm, D. Human Primary Tooth Histology Six Months after Treatment with Silver Diamine Fluoride. J. Clin. Pediatr. Dent. 2018, 42, 442–444. [Google Scholar] [CrossRef]
- Hu, S.; Muniraj, G.; Mishra, A.; Hong, K.; Lum, J.L.; Hong, C.H.L.; Rosa, V.; Sriram, G. Characterization of silver diamine fluoride cytotoxicity using microfluidic tooth-on-a-chip and gingival equivalents. Dent. Mater. 2022, 38, 1385–1394. [Google Scholar] [CrossRef]
- Targino, A.G.R.; Flores, M.A.P.; Junior, V.E.D.S.; Bezerra, F.D.G.B.; Freire, H.D.L.; Galembeck, A.; Rosenblatt, A. An innovative approach to treating dental decay in children. A new anti-caries agent. J. Mater. Sci. Mater. Med. 2014, 25, 2041–2047. [Google Scholar] [CrossRef]
- Gotjamanos, T.; Afonso, F. Unacceptably high levels of fluoride in commercial preparations of silver fluoride. Aust. Dent. J. 1997, 42, 52–53. [Google Scholar] [CrossRef]
- Gardner, A.F.; Higel, R.W. An evaluation of agents used in cavity sterilization. Aust. Dent. J. 1962, 7, 53–61. [Google Scholar] [CrossRef]
- Gotjamanos, T.; Orton, V. Fluorideion concentration in 40 per cent silver fluoride solutions determined by ion selective electrode and ion chromatography techniques. Aust. Dent. J. 1998, 43, 55–56. [Google Scholar] [CrossRef] [PubMed]
- Stebbins, E. What value has argenti nitras as a therapeutic agent in dentistry? Int. Dent. J. 1891, 12, 661–670. [Google Scholar]
- Bauer, M.; Balogh, D.; Kompatscher, P. 10% Silver nitrate solution for topical treatment in scalding. Chir. Plast. 1984, 8, 25–36. [Google Scholar] [CrossRef]
- Howe, P.R. A method of sterilizing and at the same time impregnating with a metal affected dentinal tissue. Dent. Cosm. 1917, 59, 891–904. [Google Scholar]
- Klein, H.; Knutson, J.W. XIII. Effect of Ammoniacal Silver Nitrate on Caries in the First Permanent Molar. J. Am. Dent. Assoc. 1942, 29, 1420–1426. [Google Scholar] [CrossRef]
- James, P.; Parfitt, G. A clinical note on the use of silver nitrate in the prevention of fissure caries in newly erupted first permanant molars. Br. Dent. J. 1954, 96, 35–36. [Google Scholar]
- Schultz-Haudt, S.; Taylor, R.; Brudevold, F. Silver nitrate treatment of proximal caries in primary molars. J. Dent. Child. 1956, 23, 184–186. [Google Scholar]
- Hyde, E.J. Caries-inhibiting action of three different topically-applied agents on incipient lesions in newly erupted teeth: Results after 24 months. J. Can. Dent. Assoc. 1973, 39, 189–193. [Google Scholar]
- Chu, C.-H.; Gao, S.S.; Li, S.K.; Wong, M.C.; Lo, E.C. The effectiveness of the biannual application of silver nitrate solution followed by sodium fluoride varnish in arresting early childhood caries in preschool children: Study protocol for a randomised controlled trial. Trials 2015, 16, 426. [Google Scholar] [CrossRef]
- Saito, T.; Toyooka, H.; Ito, S.; Crenshaw, M.A. In vitro Study of Remineralization of Dentin: Effects of Ions on Mineral Induction by Decalcified Dentin Matrix. Caries Res. 2003, 37, 445–449. [Google Scholar] [CrossRef] [PubMed]
- Mei, M.L.; Nudelman, F.; Marzec, B.; Walker, J.; Lo, E.; Walls, A.; Chu, C. Formation of Fluorohydroxyapatite with Silver Diamine Fluoride. J. Dent. Res. 2017, 96, 1122–1128. [Google Scholar] [CrossRef] [PubMed]
- Mei, M.L.; Ito, L.; Cao, Y.; Li, Q.; Lo, E.C.; Chu, C. Inhibitory effect of silver diamine fluoride on dentine demineralisation and collagen degradation. J. Dent. 2013, 41, 809–817. [Google Scholar] [CrossRef]
- Nishino, M.; Yoshida, S.; Sobue, S.; Kato, J.; Nishida, M. Effect of topically applied ammoniacal silver fluoride on dental caries in children. J. Osaka Univ. Dent. Sch. 1969, 9, 149–155. [Google Scholar] [PubMed]
- Mitwalli, H.; Mourao, M.D.; Dennison, J.; Yaman, P.; Paster, B.J.; Fontana, M. Effect of Silver Diamine Fluoride Treatment on Microbial Profiles of Plaque Biofilms from Root/Cervical Caries Lesions. Caries Res. 2019, 53, 555–566. [Google Scholar] [CrossRef]
- Chopra, I. The increasing use of silver-based products as antimicrobial agents: A useful development or a cause for concern? J. Antimicrob. Chemother. 2007, 59, 587–590. [Google Scholar] [CrossRef]
- Natarajan, D. Silver Modified Atraumatic Restorative Technique: A Way Towards “SMART” Pediatric Dentistry During the COVID-19 Pandemic. Front. Dent. 2022, 19, 12. [Google Scholar] [CrossRef]
- Benzian, H.; Niederman, R. A Dental Response to the COVID-19 Pandemic—Safer Aerosol-Free Emergent (SAFER) Dentistry. Front. Med. 2020, 7, 520. [Google Scholar] [CrossRef]
- Oliveira, B.H.; Rajendra, A.; Veitz-Keenan, A.; Niederman, R. The Effect of Silver Diamine Fluoride in Preventing Caries in the Primary Dentition: A Systematic Review and Meta-Analysis. Caries Res. 2018, 53, 24–32. [Google Scholar] [CrossRef]
- Tirupathi, S.P.; Svsg, N.; Rajasekhar, S.; Nuvvula, S. Comparative cariostatic efficacy of a novel Nano-silver fluoride varnish with 38% silver diamine fluoride varnish a double-blind randomized clinical trial. J. Clin. Exp. Dent. 2019, 11, e105–e112. [Google Scholar] [CrossRef]
- Seifo, N.; Cassie, H.; Radford, J.R.; Innes, N.P.T. Silver diamine fluoride for managing carious lesions: An umbrella review. BMC Oral Health 2019, 19, 145. [Google Scholar] [CrossRef] [PubMed]
- Noronha, V.T.; Paula, A.J.; Durán, G.; Galembeck, A.; Cogo-Müller, K.; Franz-Montan, M.; Durán, N. Silver nanoparticles in dentistry. Dent. Mater. 2017, 33, 1110–1126. [Google Scholar] [CrossRef]
- Lung, C.Y.K.; Abdalla, M.M.; Chu, C.H.; Yin, I.; Got, S.-R.; Matinlinna, J.P. A Multi-Element-Doped Porous Bioactive Glass Coating for Implant Applications. Materials 2021, 14, 961. [Google Scholar] [CrossRef] [PubMed]
- Kittler, S.; Greulich, C.; Diendorf, J.; Köller, M.; Epple, M. Toxicity of Silver Nanoparticles Increases during Storage Because of Slow Dissolution under Release of Silver Ions. Chem. Mater. 2010, 22, 4548–4554. [Google Scholar] [CrossRef]
- Khorrami, S.; Zarrabi, A.; Khaleghi, M.; Danaei, M.; Mozafari, M.R. Selective cytotoxicity of green synthesized silver nanoparticles against the MCF-7 tumor cell line and their enhanced antioxidant and antimicrobial properties. Int. J. Nanomed. 2018, 13, 8013–8024. [Google Scholar] [CrossRef] [PubMed]
- Bapat, R.A.; Chaubal, T.V.; Joshi, C.P.; Bapat, P.R.; Choudhury, H.; Pandey, M.; Gorain, B.; Kesharwani, P. An overview of application of silver nanoparticles for biomaterials in dentistry. Mater. Sci. Eng. C 2018, 91, 881–898. [Google Scholar] [CrossRef]
- Ramkumar, V.S.; Pugazhendhi, A.; Gopalakrishnan, K.; Sivagurunathan, P.; Saratale, G.D.; Dung, T.N.B.; Kannapiran, E. Biofabrication and characterization of silver nanoparticles using aqueous extract of seaweed Enteromorpha compressa and its biomedical properties. Biotechnol. Rep. 2017, 14, 1–7. [Google Scholar] [CrossRef]
- Hackenberg, S.; Scherzed, A.; Kessler, M.; Hummel, S.; Technau, A.; Froelich, K.; Ginzkey, C.; Koehler, C.; Hagen, R.; Kleinsasser, N. Silver nanoparticles: Evaluation of DNA damage, toxicity and functional impairment in human mesenchymal stem cells. Toxicol. Lett. 2011, 201, 27–33. [Google Scholar] [CrossRef]
- Quinzii, C.M.; Lopez, L.C.; Gilkerson, R.W.; Dorado, B.; Coku, J.; Naini, A.B.; Lagier-Tourenne, C.; Schuelke, M.; Salviati, L.; Carrozzo, R.; et al. Reactive oxygen species, oxidative stress, and cell death correlate with level of CoQ10 deficiency. FASEB J. 2010, 24, 3733–3743. [Google Scholar] [CrossRef]
- Durán, N.; Nakazato, G.; Seabra, A.B. Antimicrobial activity of biogenic silver nanoparticles, and silver chloride nanoparticles: An overview and comments. Appl. Microbiol. Biotechnol. 2016, 100, 6555–6570. [Google Scholar] [CrossRef]
- Liao, C.; Li, Y.; Tjong, S.C. Bactericidal and Cytotoxic Properties of Silver Nanoparticles. Int. J. Mol. Sci. 2019, 20, 449. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Li, L.; Zhou, X.; Yu, Y.; Li, Z.; Zuo, D.; Wu, Y. Silver nanoparticles induce protective autophagy via Ca2+/CaMKKβ/AMPK/mTOR pathway in SH-SY5Y cells and rat brains. Nanotoxicology 2019, 13, 369–391. [Google Scholar] [CrossRef] [PubMed]
- García-Contreras, R.; Argueta-Figueroa, L.; Mejía-Rubalcava, C.; Jiménez-Martínez, R.; Cuevas-Guajardo, S.; Sánchez-Reyna, P.A.; Zeron, H.M. Perspectives for the use of silver nanoparticles in dental practice. Int. Dent. J. 2011, 61, 297–301. [Google Scholar] [CrossRef]
- E Silva, A.V.C.; Teixeira, J.A.; Mota, C.C.; Lins, E.C.C.C.; Correia de Melo Júnior, P.; de Souza Lima, M.G.; Arnaud, M.; Galembeck, A.; Gadelha, A.T.; Pereira, J.R.D.; et al. In Vitro morphological, optical and microbiological evaluation of nanosilver fluoride in the remineralization of deciduous teeth enamel. Nanotechnol. Rev. 2018, 7, 509–520. [Google Scholar] [CrossRef]
- Dos Santos, V., Jr.; Vasconcelos Filho, A.; Targino, A.; Flores, M.; Galembeck, A.; Caldas, A.F., Jr.; Rosenblatt, A. A new “silver-bullet” to treat caries in children–nano silver fluoride: A randomised clinical trial. J. Dent. 2014, 42, 945–951. [Google Scholar] [CrossRef] [PubMed]
- Puppala, N.; Nagireddy, V.R.; Reddy, D.; Kondamadugu, S.; Mareddy, A.; Chris, A. Nanosilver Fluoride—A Paradigm Shift for Arrest in Dental Caries in Primary Teeth of Schoolchildren: A Randomized Controlled Clinical Trial. Int. J. Clin. Pediatr. Dent. 2019, 12, 484–490. [Google Scholar] [CrossRef]
- Zhao, I.S.; Mei, M.L.; Li, Q.-L.; Lo, E.C.M.; Chu, C.-H. Arresting simulated dentine caries with adjunctive application of silver nitrate solution and sodium fluoride varnish: An In Vitro study. Int. Dent. J. 2017, 67, 206–214. [Google Scholar] [CrossRef]
- Mei, M.L.; Chu, C.H.; Lo, E.C.M.; Samaranayake, L.P. Fluoride and silver concentrations of silver diammine fluoride solutions for dental use. Int. J. Paediatr. Dent. 2012, 23, 279–285. [Google Scholar] [CrossRef]
- Seltzer, S.; Werther, L. Conservative Silver Nitrate Treatment of Borderline Cases of Deep Dental Caries. J. Am. Dent. Assoc. 1941, 28, 1586–1594. [Google Scholar] [CrossRef]
- ISO 10993-5: 2009; Biological Evaluation of Medical Devices—Part 5: Tests for In Vitro Cytotoxicity. ISO: Geneva, Switzerland, 2009.
- Luong, M.; Sadr, A.; Chan, D.C.N. Dentin Discoloration and Pulpal Ion Concentrations Following Silver Diamine Fluoride and Potassium Iodide Treatment. Oper. Dent. 2022, 47, 640–647. [Google Scholar] [CrossRef]

| Solution | Author, Date | Study Type/Evaluation Method | Main Findings |
|---|---|---|---|
| Silver fluoride | Gotjamanos, T., 1996 [26] | In-vivo study/Histopathology | Favourable pulpal response, including the presence of abundant reparative dentine and a wide odontoblast layer in most teeth. |
| Silver nitrate | Zander, H., 1943 [27] | In-vivo & ex-vivo/Histology | Slight haemorrhage opposite to the cavity and silver particles within the pulp. |
| Zander, H., 1945 [28] | In-vivo & ex-vivo/Histology | Odontoblast injury, silver particles within the pulp, and dentine formation. | |
| Perreault, J., 1956 [29] | In-vivo/Histopathology | Hypoplasia in shallow cavities, aplasia, and pulpal necrosis in deeper cavities. | |
| Englander, H., 1956 [30] | Ex-vivo/Histopathology | Silver particles penetrated through dentine into the pulp. | |
| Seltzer, S., 1961 [31] | In-vivo/Histopathology | Morphologic changes of the odontoblasts after 1 month (Monkeys). No pulpal effect after 1 month (Dogs). | |
| Seltzer, S., 1961 [32] | In-vivo/Histopathology | Pulp healed in shallow cavities but not in deep cavities after 6 months (Monkeys). Pulp healed in shallow cavities but inflammation in deep cavities after 6 months (Dogs). | |
| Silver diamine nitrate | Srisomboon, S., 2022 [33] | In-vitro/Cytotoxicity | Cellular vitality was 88%. |
| Silver diamine fluoride | Hosoya, Y., 1990 [34] | In-vivo/Histopathology | Inflammation, hyperaemia, necrosis after 3 days. Hyperaemia, partial necrosis after 7 days. A decrease in inflammation, but an increase in pulp necrosis after 30 days. |
| Korwar, A., 2015 [35] | Ex-vivo/Histopathology | Tertiary dentine formation with no inflammation or necrosis After 6 weeks. | |
| Rossi, G., 2017 [36] | Ex-vivo & in-vivo/Histopathology | Ex-vivo: Limited penetration of silver diamine fluoride into the dentinal tubules, chronic inflammatory infiltrate in the pulp tissue, and tertiary dentine formation. In-vivo: Well-organized dental pulp with mild inflammatory infiltrate. | |
| Bimstein, E., 2018 [37] | Case report/Histopathology | Tertiary dentine formation, minimal pulpal inflammation, and silver particles within dentinal tubules after 6 months. | |
| Hu, S., 2022 [38] | In-vitro/Cytotoxicity | Direct contact: Cellular viability was less than 50% above 0.001% silver diamine fluoride. Indirect contact: No vital cells for dentine 1 mm thick and 30% cell viability for dentine of 1.5 mm thick. | |
| Srisomboon, S., 2022 [33] | In-vitro/Cytotoxicity | Cellular vitality was 92%. | |
| Nano-silver fluoride | Targino, A., 2014 [39] | In-vitro/Cytotoxicity | Non-toxic to human erythrocytes at any concentration. |
| Solution | Pulpal Response to Direct Contact | Pulpal Response to Indirect Contact |
|---|---|---|
| Silver fluoride |
|
|
| Silver nitrate |
|
|
| Silver diamine nitrate |
|
|
| Silver diamine fluoride |
|
|
| Nano-silver fluoride |
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zaeneldin, A.; Chu, C.-H.; Yu, O.Y. Dental Pulp Response to Silver-Containing Solutions: A Scoping Review. Dent. J. 2023, 11, 114. https://doi.org/10.3390/dj11050114
Zaeneldin A, Chu C-H, Yu OY. Dental Pulp Response to Silver-Containing Solutions: A Scoping Review. Dentistry Journal. 2023; 11(5):114. https://doi.org/10.3390/dj11050114
Chicago/Turabian StyleZaeneldin, Ahmed, Chun-Hung Chu, and Ollie Yiru Yu. 2023. "Dental Pulp Response to Silver-Containing Solutions: A Scoping Review" Dentistry Journal 11, no. 5: 114. https://doi.org/10.3390/dj11050114