
Are Allergy-Induced Implant Failures Actually Hypersensitivity Reactions to Titanium? A Literature Review

Abstract
:1. Introduction
2. Materials and Methods
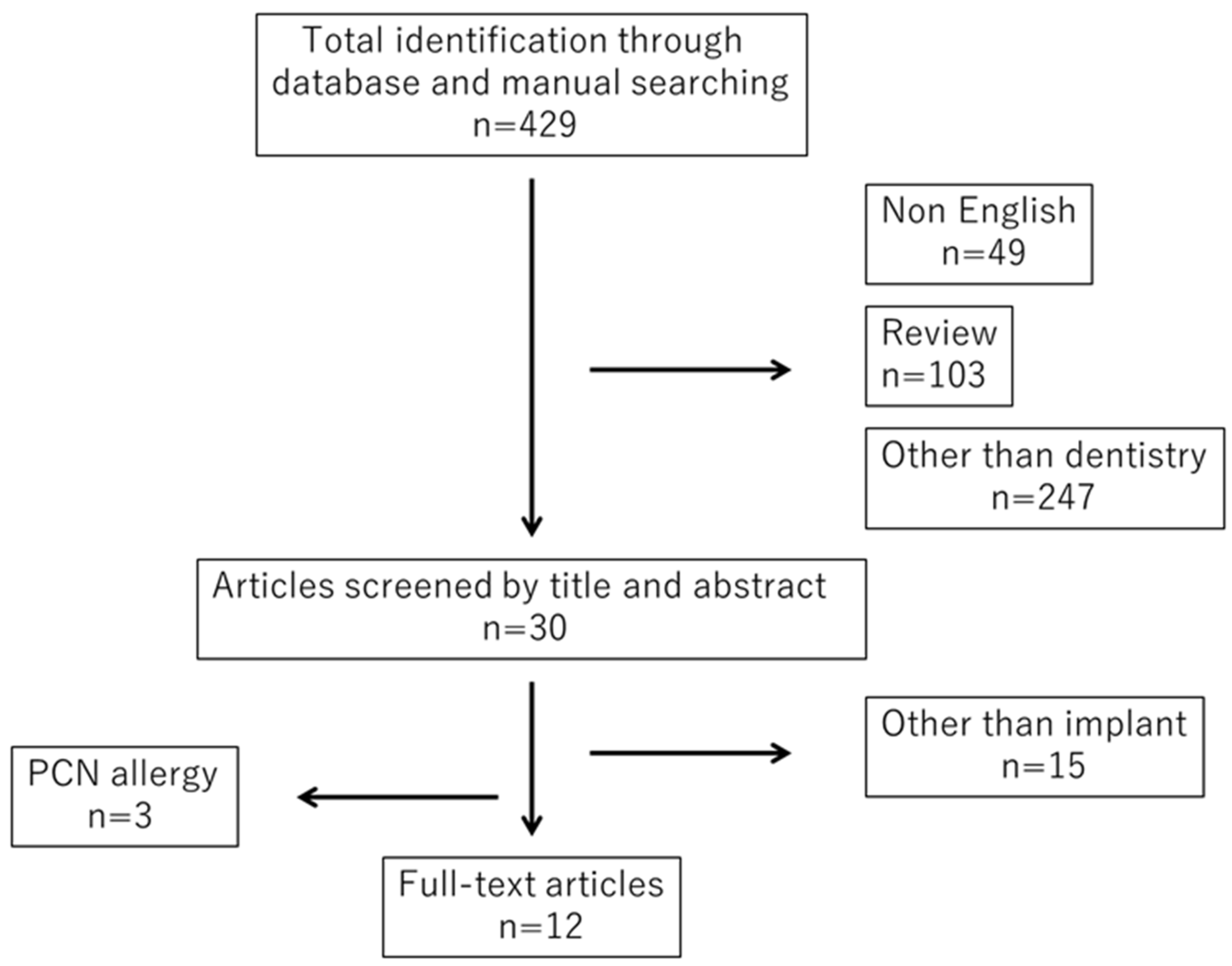
2.1. Search Strategy
2.2. Inclusion/Exclusion Criteria
2.3. Data Collection
3. Results
3.1. Characteristics of the Representative Articles
3.2. Positive Results for Allergies Other Than Titanium
3.3. Articles on Penicillin Allergy
4. Discussion
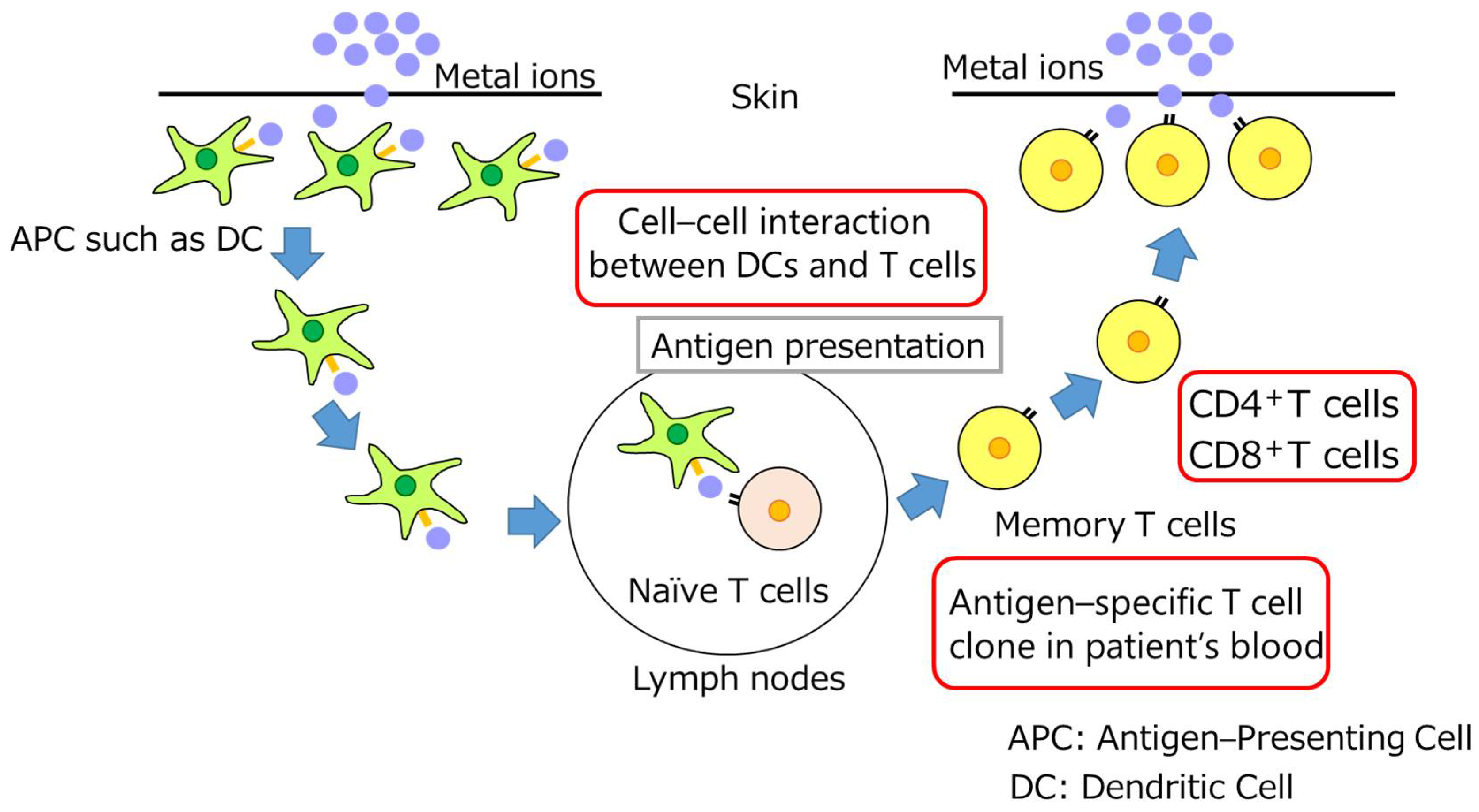
4.1. Mechanism of Dental Metal Allergy Development
4.2. Clinical Symptoms of Titanium Allergy
4.3. Immunological Mechanisms of Metal-Allergy-Testing Methodologies
4.4. Diagnostic Techniques Used in Titanium Allergy Detection and Their Limitations
4.5. The Effect of Non-Titanium Metal Materials Included in Dental Implants
4.6. Other Factors That May Contribute to the Development of Titanium Allergy
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Faschingbauer, M.; Renner, L.; Boettner, F. Allergy in total knee replacement. Does it exist?: Review article. HSS J. 2016, 13, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Dmochowski, J.M.; Royal, J.T.; Lourie, G.M. Could a titanium ulnar shortening plate trigger a metal allergy? A case report. J. Wrist Surg. 2019, 8, 503–507. [Google Scholar] [CrossRef]
- Razzante, M.C.; Ehredt, D.J.; Clougherty, C.O.; Kriger, S.J.; Menninger, B.A.; Dionisopoulos, S.B.; Bhakta, P.J.; Bruning, N.G. Type iv cell-mediated hypersensitivity reaction caused by titanium implant following double calcaneal osteotomy and first metatarsal-cuneiform arthrodesis: A case report and review of the literature. J. Foot Ankle Surg. 2019, 58, 974–979. [Google Scholar] [CrossRef]
- Tiwari, R.C.; Singh, R.; Lehl, G.; Hussain, A.; Abhang, T.; Kulkarni, M.; A Elagib, M. Prevalence of titanium hypersensitivity in patients with titanium implants: A systematic review and meta-analysis. J. Pharm. Bioallied Sci. 2021, 13, S1345–S1349. [Google Scholar] [CrossRef] [PubMed]
- Adell, R.; Lekholm, U.; Rockler, B.; Brånemark, P.I. A 15-year study of osseointegrated implants in the treatment of the edentulous jaw. Int. J. Oral Surg. 1981, 10, 387–416. [Google Scholar] [CrossRef] [PubMed]
- Alghamdi, H.S.; Jansen, J.A. The development and future of dental implants. Dent. Mater. J. 2020, 39, 167–172. [Google Scholar] [CrossRef] [PubMed]
- O’Mahony, A.; Spencer, P. Osseointegrated implant failures. J. Ir Dent. Assoc. 1999, 45, 44–51. [Google Scholar]
- Mitchell, D.L.; Synnott, S.A.; Dercreek, V.J.A. Tissue reaction involving an intraoral skin graft and CP titanium abutments: A clinical report. Int. J. Oral Maxillofac Implant. 1990, 5, 79–84. [Google Scholar]
- Müller, K.; Valentine-Thon, E. Hypersensitivity to titanium: Clinical and laboratory evidence. Neuro Endocrinol. Lett. 2006, 27, 31–35. [Google Scholar] [PubMed]
- Du Preez, L.A.; Bütow, K.W.; Swart, T.J.P. Implant failure due to titanium hypersensitivity/allergy?—Report of a case. S. Afr. Dent. J. 2007, 62, 24–25. [Google Scholar]
- Sicilia, A.; Cuesta, S.; Coma, G.; Arregui, I.; Guisasola, C.; Ruiz, E.; Maestro, A. Titanium allergy in dental implant patients: A clinical study on 1500 consecutive patients. Clin. Oral Implants Res. 2008, 19, 823–835. [Google Scholar] [CrossRef] [PubMed]
- Egusa, H.; Ko, N.; Shimazu, T.; Yatani, H. Suspected association of an allergic reaction with titanium dental implants: A clinical report. J. Prosthet. Dent. 2008, 100, 344–347. [Google Scholar] [CrossRef]
- Pigatto, P.D.; Berti, E.; Spadari, F.; Bombeccari, G.P.; Guzzi, G. Photoletter to the editor: Exfoliative cheilitis associated with titanium dental implants and mercury amalgam. J. Dermatol. Case Rep. 2011, 5, 89–90. [Google Scholar] [CrossRef]
- Hosoki, M.; Nishigawa, K.; Miyamoto, Y.; Ohe, G.; Matsuka, Y. Allergic contact dermatitis caused by titanium screws and dental implants. J. Prosthodont. Res. 2016, 60, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Hosoki, M.; Nishigawa, K.; Tajima, T.; Ueda, M.; Matsuka, Y. Cross-sectional observational study exploring clinical risk of titanium allergy caused by dental implants. J. Prosthodont. Res. 2018, 62, 426–431. [Google Scholar] [CrossRef] [PubMed]
- Andrei, O.C.; Tănăsescu, L.A.; Burlibaşa, M.; Bătăiosu, M.; Dăguci, L.; Burlibaşa, L.; Turcu, A.A.; Dăguci, C. Suspicions of titanium allergic reaction influencing the prosthetic solution in a rare case of implant “flowering”. Rom. J. Morphol. Embryol. 2019, 60, 233–241. [Google Scholar] [PubMed]
- Tawil, G.; Tawil, P.; Irani, C. Zirconium implant as an alternative to titanium implant in a case of type iv titanium allergy: Case report. Int. J. Oral Maxillofac. Implants 2020, 35, 639–644. [Google Scholar] [CrossRef]
- Borgonovo, A.E.; Censi, R.; Vavassori, V.; Savio, M.; Re, D. A possible relationship between peri-implantitis, titanium hypersensitivity, and external tooth resorption: Metal-free alternative to titanium implants. Case Rep. Dent. 2021, 2021, 8879988. [Google Scholar] [CrossRef]
- Alqahtani, A.R.; Gufran, K.; Silva, F.; Rocha, M.G.; Chang, J. A clinical case report of a potential acute allergic reaction with titanium dental implant. Case Rep. Dent. 2021, 2021, 1–7. [Google Scholar] [CrossRef]
- French, D.; Noroozi, M.; Shariati, B.; Larjava, H. Clinical retrospective study of self-reported penicillin allergy on dental implant failures and infections. Quintessence Int. 2016, 47, 861–870. [Google Scholar]
- Coll, S.O.; Carrascal, L.N.; Abdulkarim, L.A.; Alfaro, H.F.; Albiol, G.J.; Nieto, S.M. Do penicillin-allergic patients present a higher rate of implant failure? Int. J. Oral Maxillofac. Implants 2018, 33, 1390–1395. [Google Scholar] [CrossRef] [PubMed]
- Block, M.S.; Christensen, B.J.; Mercante, D.E.; Chapple, A.G. What factors are associated with implant failure? J. Oral Maxillofac. Surg. 2021, 79, 91–97. [Google Scholar] [CrossRef]
- Rajan, T.V. The Gell–Coombs classification of hypersensitivity reactions: A re-interpretation. Trends Immunol. 2003, 24, 376–379. [Google Scholar] [CrossRef] [PubMed]
- Brånemark, P.I.; Adell, R.; Breine, U.; Hansson, B.O.; Lindström, J.; Ohlsson, A. Intra-osseous anchorage of dental prostheses. I. Experimental studies. Scand. J. Plast. Reconstr. Surg. 1969, 3, 81–100. [Google Scholar] [CrossRef] [PubMed]
- The European Parliament and the Council of the European Union. Regulation of the European Parliament and of the Council on Cosmetic Products 2009; Official Journal of the European Union: Luxembourg, 2009. [Google Scholar]
- Wang, X.; Josefsson, L.; Meschnark, S.; Lind, M.L.; Emmer, Å.; Goessler, W.; Hedberg, Y.S. Analytical survey of tattoo inks—A chemical and legal perspective with focus on sensitizing substances. Contact Dermat. 2021, 85, 340–353. [Google Scholar] [CrossRef]
- Borowska, S.; Brzóska, M.M. Metals in cosmetics: Implications for human health. J. Appl. Toxicol. 2015, 35, 551–572. [Google Scholar] [CrossRef]
- Bocca, B.; Pino, A.; Alimonti, A.; Forte, G. Toxic metals contained in cosmetics: A status report. Regul. Toxicol. Pharmacol. 2014, 68, 447–467. [Google Scholar] [CrossRef]
- Wang, X.; Hedberg, Y.S.; Odnevall, I. Presence of impurities of nickel and cobalt in facial cosmetic pigments and their dissolution into artificial sweat. Contact Dermatitis. 2022, 87, 550–553. [Google Scholar] [CrossRef]
- Bezerra, S.F.; Rodrigues, B.D.S.; da Silva, A.C.G.; de Ávila, R.I.; Brito, H.R.G.; Cintra, E.R.; Veloso, D.F.M.C.; Lima, E.M.; Valadares, M.C. Application of the adverse outcome pathway framework for investigating skin sensitization potential of nanomaterials using new approach methods. Contact Dermat. 2021, 84, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Vallion, R.; Kerdine-Römer, S. Regulation of the immune response to contact sensitizers by Nrf2. Contact Dermat. 2022, 87, 13–19. [Google Scholar] [CrossRef]
- Liu, L.; Watanabe, M.; Minami, N.; Yunizar, M.F.; Ichikawa, T. Semaphorin 3A: A potential target for prevention and treatment of nickel allergy. Commun. Biol. 2022, 5, 671. [Google Scholar] [CrossRef]
- Hanawa, T. Biocompatibility of titanium from the viewpoint of its surface. Sci. Technol. Adv. Mater. 2022, 23, 457–472. [Google Scholar] [CrossRef] [PubMed]
- de Graaf, N.P.J.; Feilzer, A.J.; Kleverlaan, C.J.; Bontkes, H.; Gibbs, S.; Rustemeyer, T. A retrospective study on titanium sensitivity: Patch test materials and manifestations. Contact Dermat. 2018, 79, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Obtułowicz, A.; Ślusarczyk, M.N.; Pirowska, M.; Godlewska, S.L.; Pelc, A.W. The flare-up phenomenon: Recurrence of distant dermatitis during patch testing. Postepy Dermatol. Alergol. 2016, 33, 68–69. [Google Scholar] [CrossRef] [PubMed]
- Thomas, P. Clinical and diagnostic challenges of metal implant allergy using the example of orthopaedic surgical implants. Allergo J. Int. 2014, 23, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Basketter, D.A.; Whittle, E.; Monk, B. Possible allergy to complex titanium salt. Contact Dermat. 2000, 42, 310–311. [Google Scholar]
- Lalor, P.A.; Revell, P.A.; Gray, A.B.; Wright, S.; Railton, G.T.; Freeman, M.A. Sensitivity to titanium. A cause of implant failure? J. Bone Jt. Surg. Br. 1991, 73, 25–28. [Google Scholar] [CrossRef]
- Holgers, K.M.; Roupe, G.; Tjellström, A.; Bjursten, L.M. Clinical, immunological and bacteriological evaluation of adverse reactions to skin-penetrating titanium implants in the head and neck region. Contact Dermat. 1992, 27, 1–7. [Google Scholar] [CrossRef]
- Linauskienė, K.; Malinauskienė, L.; Blažienė, A. Metals are important contact sensitizers: An experience from Lithuania. Biomed Res. Int. 2017, 2017, 3964045. [Google Scholar] [CrossRef]
- Fage, S.W.; Muris, J.; Jakobsen, S.S.; Thyssen, J.P. Titanium: A review on exposure, release, penetration, allergy, epidemiology, and clinical reactivity. Contact Dermat. 2016, 74, 323–345. [Google Scholar] [CrossRef]
- Heupt, M.L.K.; Schiegnitz, E.; Kaya, S.; Gresser, J.E.; Kämmerer, P.W.; Nawas, A.B. Diagnostic tests for titanium hypersensitivity in implant dentistry: A systematic review of the literature. Int. J. Implant. Dent. 2022, 8, 29. [Google Scholar] [CrossRef] [PubMed]
- Bernard, S.; Baeck, M.; Tennstedt, D.; Haufroid, V.; Dekeuleneer, V. Chromate or titanium allergy—The role of impurities? Contact Dermat. 2013, 68, 191–192. [Google Scholar] [CrossRef]
- Harloff, T.; Hönle, W.; Holzwarth, U.; Bader, R.; Thomas, P.; Schuh, A. Titanium allergy or not? ‘Impurity’ of titanium implant materials. Health 2010, 2, 306–310. [Google Scholar] [CrossRef]
- Evrard, L.; Waroquier, D.; Parent, D. Allergies to dental metals. Titanium: A new allergen. Rev. Med. Brux. 2010, 31, 44–49. [Google Scholar] [PubMed]
- Pacheco, K.A. Allergy to surgical implants. Clin. Rev. Allergy Immunol. 2018, 56, 72–85. [Google Scholar] [CrossRef]
- Kim, K.T.; Eo, M.Y.; Nguyen, T.T.H.; Kim, S.M. General review of titanium toxicity. Int. J. Implant. Dent. 2019, 5, 10. [Google Scholar] [CrossRef] [PubMed]
- Chaturvedi, T. Allergy related to dental implant and its clinical significance. Clin. Cosmet. Investig. Dent. 2013, 5, 57–61. [Google Scholar] [CrossRef]
- Lugowski, S.J.; Smith, D.C.; McHugh, A.D.; Loon, V.J.C. Release of metal ions from dental implant materials in vivo: Determination of Al, Co, Cr, Mo, Ni, V, and Ti in organ tissue. J. Biomed. Mater. Res. 1991, 25, 1443–1458. [Google Scholar] [CrossRef]
- Peyron, R.N. Implants and prostheses (excluding dentistry) and metal allergies. Revue Française d’Allergologie 2010, 50, S23–S28. [Google Scholar]
- Thomas, P.; Bandl, W.D.; Maier, S.; Summer, B.; Przybilla, B. Hypersensitivity to titanium osteosynthesis with impaired fracture healing, eczema, and T-cell hyperresponsiveness in vitro: Case report and review of the literature. Contact Dermat. 2006, 55, 199–202. [Google Scholar] [CrossRef]
- Kohal, R.J.; Att, W.; Bächle, M.; Butz, F. Ceramic abutments and ceramic oral implants. An. Update Periodontol. 2000 2008, 47, 224–243. [Google Scholar] [CrossRef]
- Wenz, H.J.; Bartsch, J.; Wolfart, S.; Kern, M. Osseointegration and clinical success of zirconia dental implants: A systematic review. Int. J. Prosthodont. 2008, 21, 27–36. [Google Scholar] [PubMed]
- Andreiotelli, M.; Wenz, H.J.; Kohal, R.J. Are ceramic implants a viable alternative to titanium implants? A systematic literature review. Clin. Oral Implants Res. 2009, 20, 32–47. [Google Scholar] [CrossRef] [PubMed]
- Özkurt, Z.; Kazazoğlu, E. Zirconia dental implants: A literature review. J. Oral Implantol. 2011, 37, 367–376. [Google Scholar] [CrossRef] [PubMed]
- Osman, R.B.; Swain, M.V.; Atieh, M.; Ma, S.; Duncan, W. Ceramic implants (Y-tzp): Are they a viable alternative to titanium implants for the support of overdentures? A randomized clinical trial. Clin. Oral Implants Res. 2014, 25, 1366–1377. [Google Scholar] [CrossRef]
- Limones, A.; Mourelle, M.P.; Azevedo, L.; Rubio, R.M.; Correia, A.; Polo, G.M. Zirconia-ceramic versus metal-ceramic posterior multiunit tooth-supported fixed dental prostheses: A systematic review and meta-analysis of randomized controlled trials. J. Am. Dent. Assoc. 2020, 151, 230–238.e7. [Google Scholar] [CrossRef] [PubMed]
- Röhlig, G.B.; Saruhanoglu, A.; Cifter, E.D.; Evlioglu, G. Applicability of zirconia dental prostheses for metal allergy patients. Int. J. Prosthodont. 2010, 23, 562–565. [Google Scholar]
- Amoah, D.K.G.; Waddell, B.S.; Prakash, R.; Alexiades, M.M. Adverse Reaction to Zirconia in a Modern Total Hip Arthroplasty with Ceramic Head. Arthroplast Today 2020, 6, 612–616e1. [Google Scholar] [CrossRef]
- Kitagawa, M.; Murakami, S.; Akashi, Y.; Oka, H.; Shintani, T.; Ogawa, I.; Inoue, T.; Kurihara, H. Current status of dental metal allergy in Japan. J. Prosthodont. Res. 2019, 63, 309–312. [Google Scholar] [CrossRef] [PubMed]
- Modjtahedi, B.S.; Modjtahedi, S.P.; Maibach, H.I. The sex of the individual as a factor in allergic contact dermatitis. Contact Dermat. 2004, 50, 53–59. [Google Scholar] [CrossRef]
- Malm, M.O.; Jemt, T.; Stenport, V.F. Patient factors related to early implant failures in the edentulous jaw: A large retrospective case-control study. Clin. Implant. Dent. Relat Res. 2021, 23, 466–476. [Google Scholar] [CrossRef]
- Esposito, M.; Thomsen, P.; Ericson, L.E.; Lekholm, U. Histopathologic observations on early oral implant failures. Int. J. Oral Maxillofac. Implants 1999, 14, 798–810. [Google Scholar] [PubMed]
- Esposito, M.; Grusovin, M.G.; Worthington, H.V. Interventions for replacing missing teeth: Antibiotics at dental implant placement to prevent complications. Cochrane Database Syst. Rev. 2013, 2013, CD004152. [Google Scholar] [CrossRef] [PubMed]
- Dixon, W.G.; Bansback, N. Understanding the side effects of glucocorticoid therapy: Shining a light on a drug everyone thinks they know. Ann. Rheum Dis. 2012, 71, 1761–1764. [Google Scholar] [CrossRef] [PubMed]
- Ohnaka, K.; Tanabe, M.; Kawate, H.; Nawata, H.; Takayanagi, R. Glucocorticoid suppresses the canonical Wnt signal in cultured human osteoblasts. Biochem. Biophys. Res. Commun. 2005, 329, 77–181. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, R.S. Clinical practice. Glucocorticoid-induced bone disease. N. Engl. J. Med. 2011, 365, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Van Bever, H.P.; Samuel, S.T.; Lee, B.W. Halting the allergic march. World Allergy Organ. J. 2008, 1, 57–62. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Year | Authors and References | Research method | Number of Patients | Clinical Symptoms | Diagnostic Tests | Clinical Outcomes |
|---|---|---|---|---|---|---|
| 1990 | Mitchell DL [8] | Case-report | 2 | Gingival hyperplasia | NA | Removed implants→ Symptom improvement |
| 2006 | Müller K [9] | Clinical and Experimental | 56 | Dermatitis, Eczema | MELISA/Patch test | Removed implants→ Symptom improvement |
| 2007 | du Preez LA [10] | Case-report | 1 | Bone resorption, Flank pain, Giant cell reaction | IHC | Removed implants→ Symptom improvement |
| 2008 | Sicilia A [11] | Case-control | 1500 | Dermatitis, Eczema, Pruritis | Patch test | Removed implants/Follow-up |
| 2008 | Egusa H [12] | Case-report | 1 | Eczema | LTT | Removed implants→ Symptom improvement |
| 2011 | Pigatto PD [13] | Case-report | 1 | Cheilitis | Patch test | Removed implants→ Symptom improvement |
| 2016 | Hosoki M [14] | Case-report | 1 | Eczema | Patch test (non Ti) | Removed implants→ Symptom improvement |
| 2018 | Hosoki M [15] | Clinical retrospective | 16 implants | Eczema | Patch test | Removed implants and positive metals →Symptom improvement |
| 2019 | Anderei OC [16] | Case-report | 1 | Horizontal movement of an implant, Hyperplastic gingivitis | IHC | Removed implants→ Symptom improvement |
| 2020 | Tawil G [17] | Case-report | 1 | NA | LTT/MELISA | Removed Ti implants→ Replaced to Zr implants →Symptoms improvement |
| 2021 | Borgonovo AE [18] | Case-report | 1 | High mucosa sensitivity /Implant exposure | Biopsy/MELISA | Removed Ti implants→ Replaced to Zr implants →Symptoms improvement |
| 2021 | Alqahtani AR [19] | Case-report | 1 | Pain, Eczema, Swelling, Burning sensation | Medical history, Clinical symptoms after implantation | Removed implants/Follow-up |
| Year | Authors | Number of Patients | Onset of Allergy Symptoms | Time of Removal | Time of Recovery, Course of Symptoms |
|---|---|---|---|---|---|
| 1990 | Mitchell DL [8] | 2 | Within 2 weeks after abutment placement 3.5 months after implant placement | 16 months after abutment placement Not removed | Symptom resolution time unknown, no symptoms during 18 months of follow-up Symptom resolution time unknown, no symptoms during 11 months of follow-up |
| 2007 | du Preez LA [10] | 1 | 1 week after implant placement | Not described | Not described |
| 2008 | Egusa H [12] | 1 | 1 week after implant placement | 2 years after implant placement | Symptoms disappeared after 10 months from removal |
| 2011 | Pigatto PD [13] | 1 | 1 week after implant placement | Not removed | Not described |
| 2016 | Hosoki M [14] | 1 | 2 years after implant placement, 6 months after placement of Ti screws in lower limb fracture | 6 years after implant placement | Symptoms disappeared after 1 month from removal |
| 2019 | Anderei OC [16] | 1 | A few months | 1.5 years after placement | Not described |
| 2020 | Tawil G [17] | 1 | A few days after implant placement | 3 months after implant placement | Symptoms disappeared after 3 months from removal |
| 2021 | Borgonovo AE [18] | 1 | 6 months after implant placement | Not described | Symptom resolution time unknown, no symptoms during 18 months of follow-up |
| 2021 | Alqahtani AR [19] | 1 | 2 days after implant placement | Immediately | Symptoms disappeared after 3 weeks from removal |
| Positive Metals Other than Ti | Other Allergies | Sex | References |
|---|---|---|---|
| Ni, Hg | Female | [12] | |
| Ni, Hg, Pd, Au, Cu | Female | [13] | |
| Hg, Pd, Au, Cr, Co, Cu, Sn, Zn, Ir, Mo | Food | Male | [14] |
| Ni, Co | Female | [17] | |
| NA | Pollen, Dust | Female | [18] |
| Positive Metals Other than Ti | Patients or Implants | References | |
| Ni, Hg, Cd, Pd, Au, Pt, Sn | 56 patients | [9] | |
| Ni, Cr | 1500 patients | [11] | |
| Ni, Hg, Pd, Cr | 16 implants | [15] |
| Year | Authors and References | Research Method | Patients or Implants | Suggestions |
|---|---|---|---|---|
| 2016 | French D [20] | Retrospective cohort study | 5576 implants | Self-reported penicillin allergy is a risk factor for early implant failure due to high infection rates. |
| 2018 | Salomó-Coll O [21] | Cross-sectional study | 1210 patients | Penicillin allergy is one of the risk factors for early implant failure. |
| 2021 | Block MS [22] | Retrospective case-controlled study | 224 patients | Penicillin-allergic patients treated with other antibiotics showed four times the risk of suffering dental implant failure. |
| Classification | Immune Reactant | Timing of Reactions | Clinical Manifestations |
|---|---|---|---|
| Type I | IgE | Immediate Anaphylactic 15–20 min | Allergic rhinitis, Asthma, Food allergy Drug allergy, Anaphylactic shock |
| Type Ⅱ | IgG, IgM | Cytotoxic Various timings | Hemolytic transfusion reaction Autoimmune hemolytic anemia Immune thrombocytopenia |
| Type Ⅲ | IgG, IgM | Immune complex 3–12 h | Arthus reaction, Serum sickness SLE, Glomerulonephritis |
| Type Ⅳ | T cells | Delayed 24–72 h | Contact dermatitis Allograft rejection, Tuberculin reaction |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Watanabe, M.; Liu, L.; Ichikawa, T. Are Allergy-Induced Implant Failures Actually Hypersensitivity Reactions to Titanium? A Literature Review. Dent. J. 2023, 11, 263. https://doi.org/10.3390/dj11110263
Watanabe M, Liu L, Ichikawa T. Are Allergy-Induced Implant Failures Actually Hypersensitivity Reactions to Titanium? A Literature Review. Dentistry Journal. 2023; 11(11):263. https://doi.org/10.3390/dj11110263
Chicago/Turabian StyleWatanabe, Megumi, Lipei Liu, and Tetsuo Ichikawa. 2023. "Are Allergy-Induced Implant Failures Actually Hypersensitivity Reactions to Titanium? A Literature Review" Dentistry Journal 11, no. 11: 263. https://doi.org/10.3390/dj11110263