
Alveolar Ridge Preservation with Autologous Platelet-Rich Fibrin (PRF): Case Reports and the Rationale

Abstract
:1. Introduction
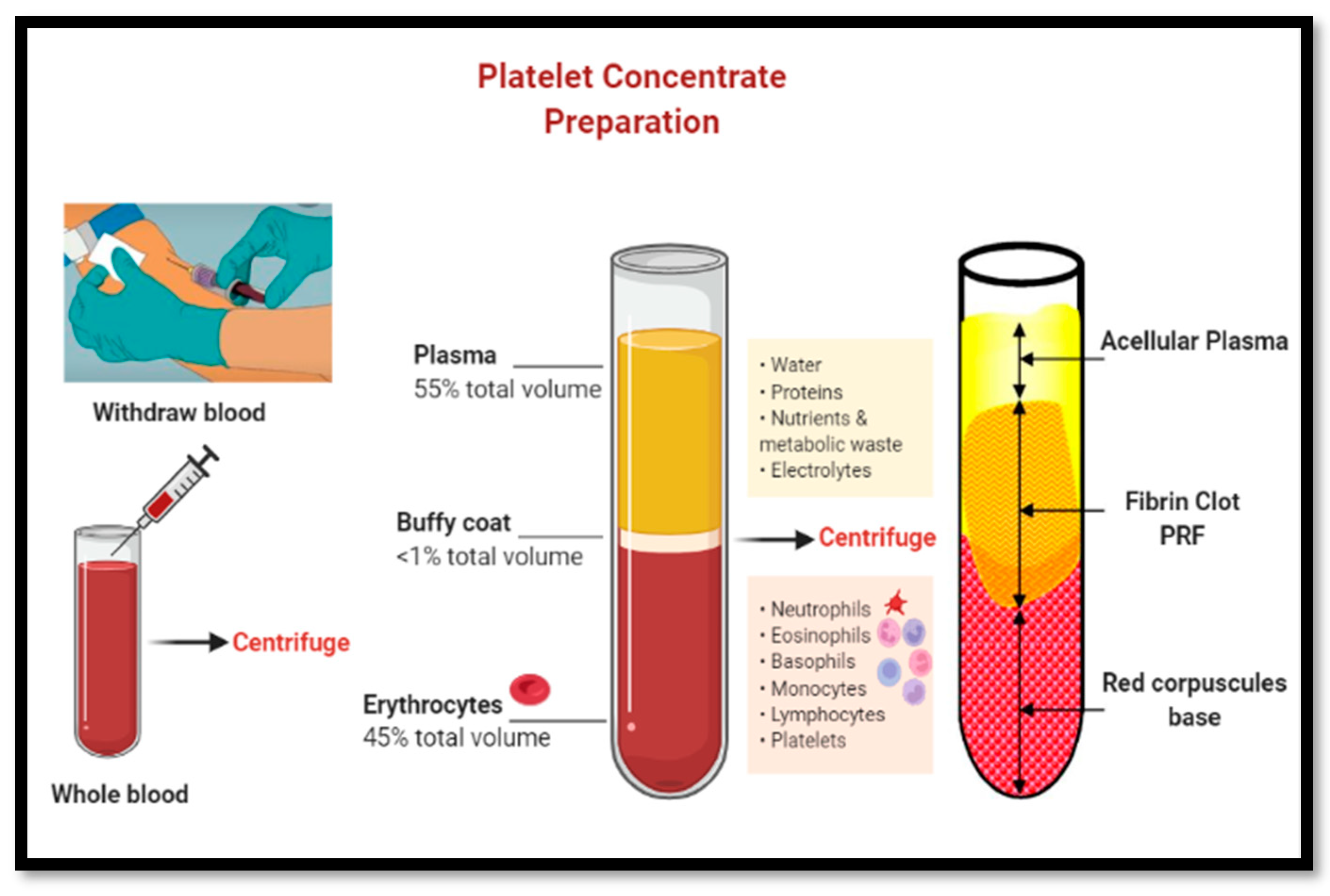
1.1. Use of Platelet-Rich Fibrin (PRF) in Dentistry
1.2. Improved PRF Protocols-A-PRF, A-PRF+ and i-PRF
2. Methodology
2.1. Materials and Methods
- Study Design:
- Step 1: Cases were selected for ARP and PRF according to established selection criteria (Ucer and Khan, 2023) [21]
- Step 2: Pre-treatment clinical and radiological assessments were undertaken to determine suitability for ARP
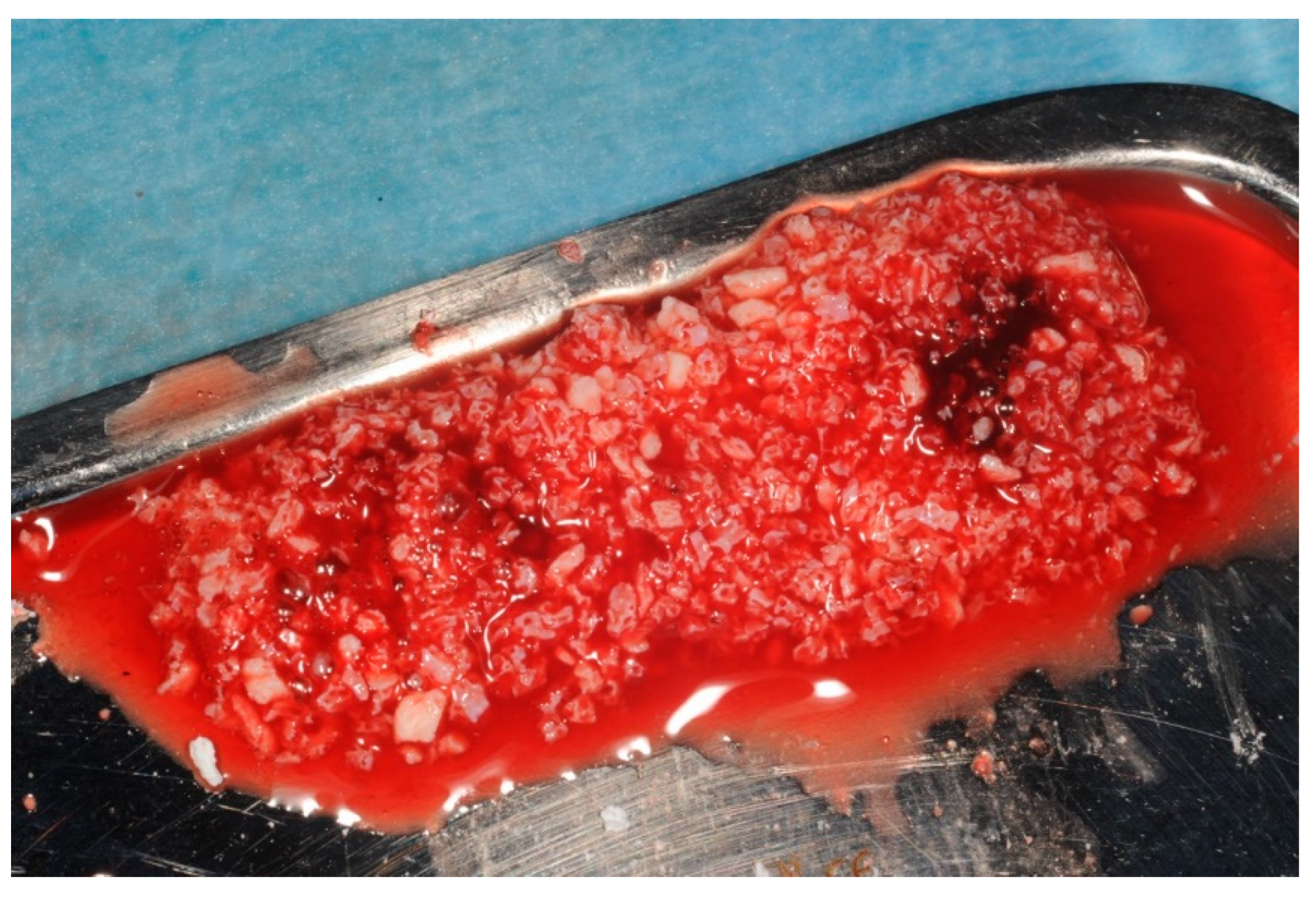
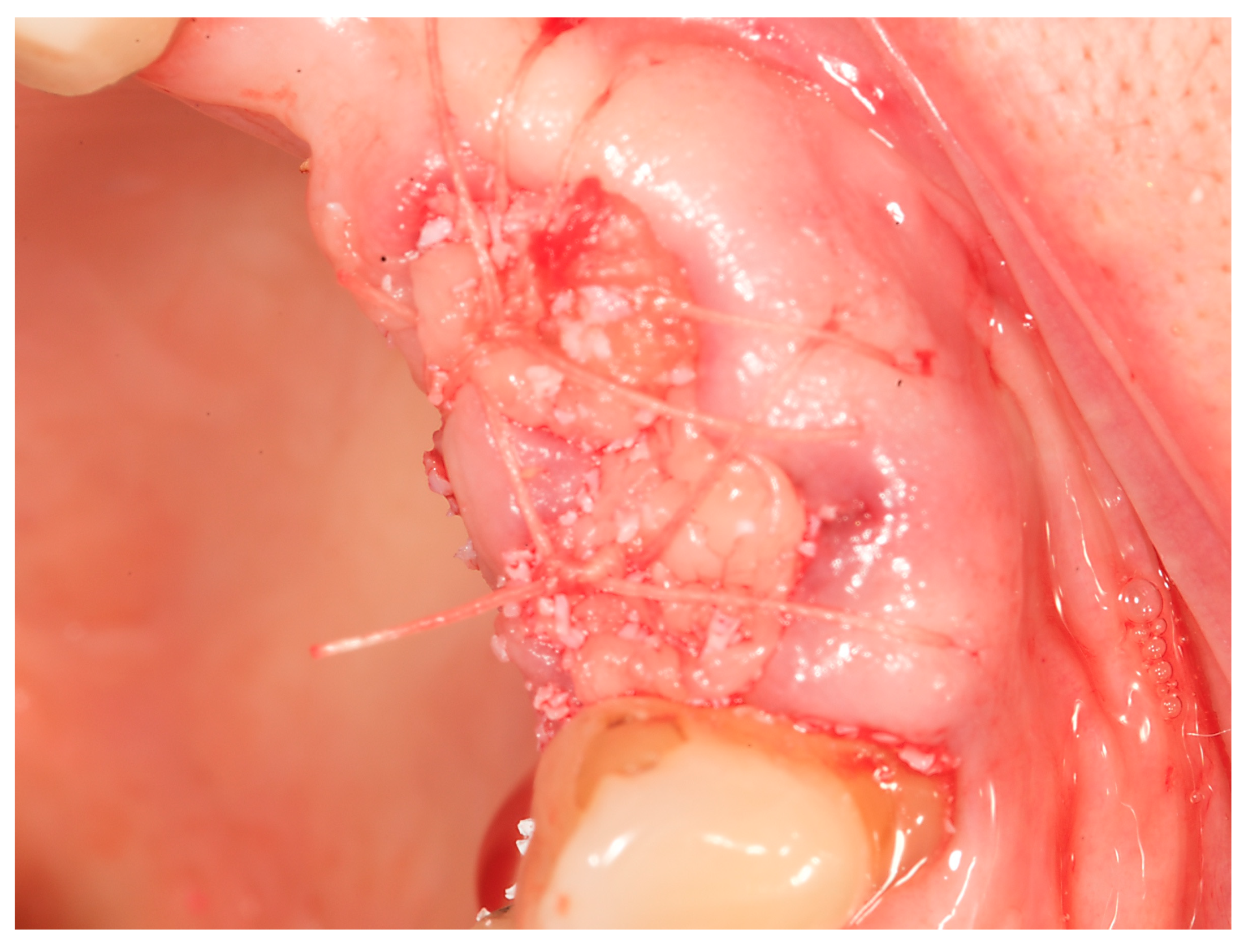
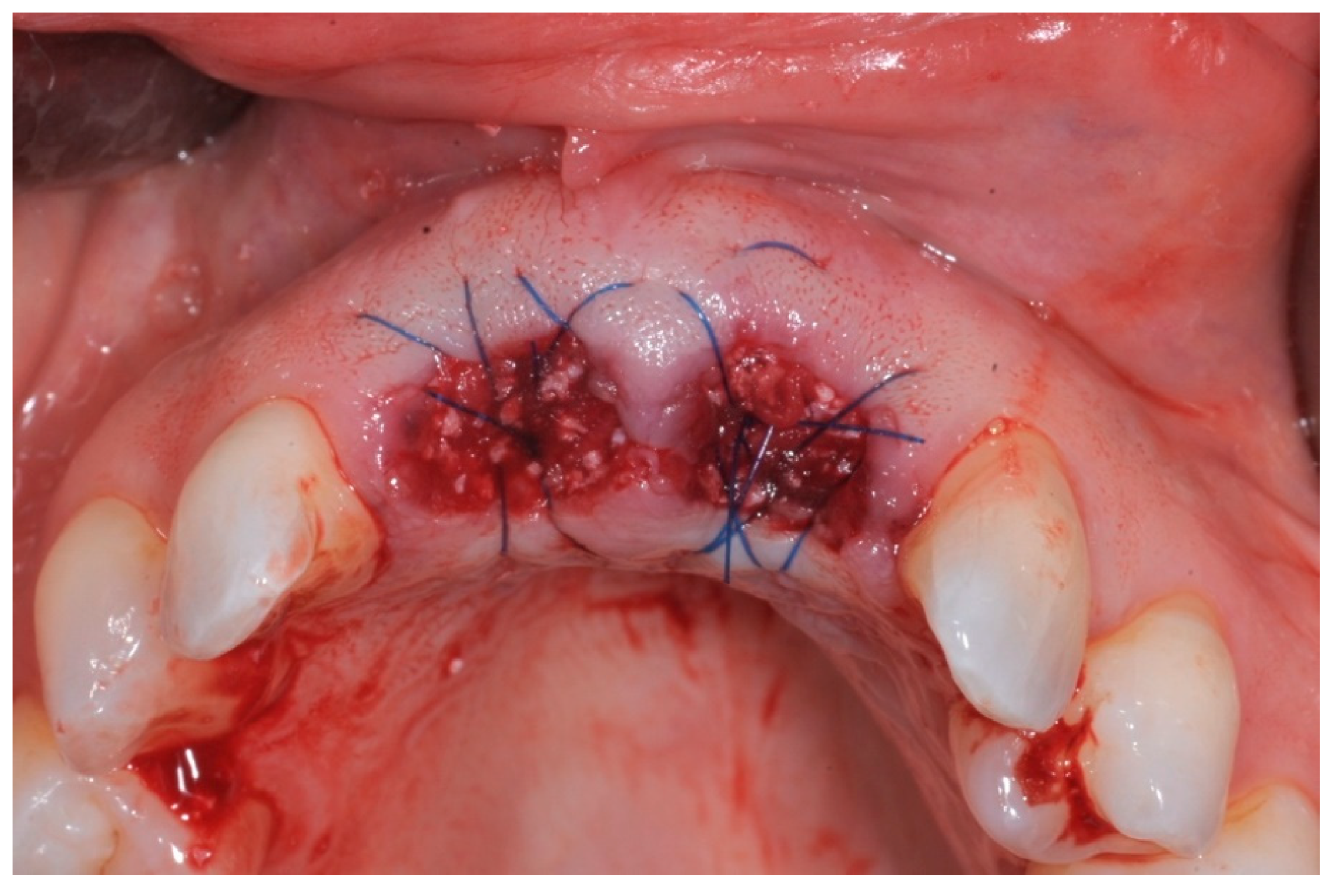
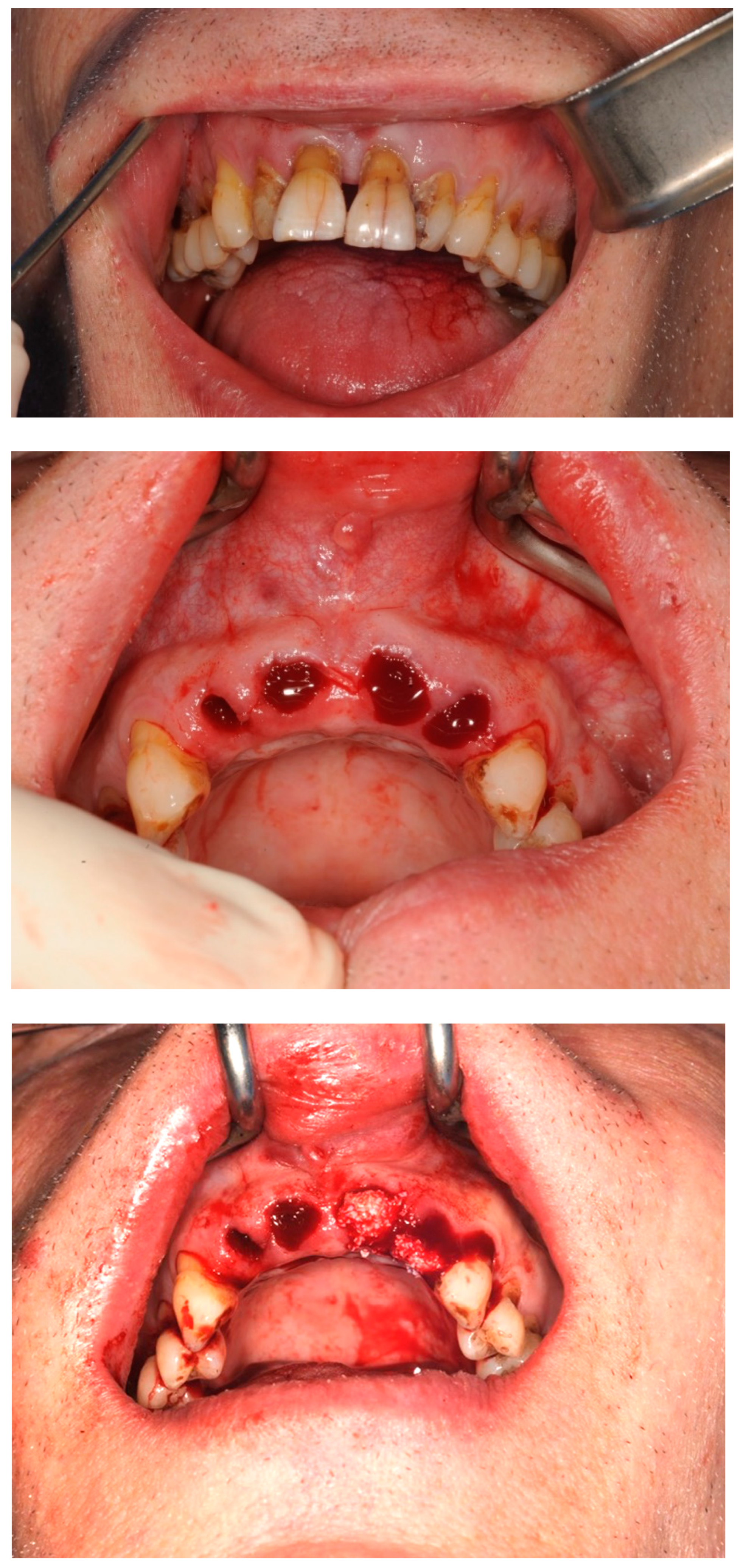
- Step 3: Teeth were removed using a minimally invasive extraction technique and the sockets were grafted with a xenograft and PRF
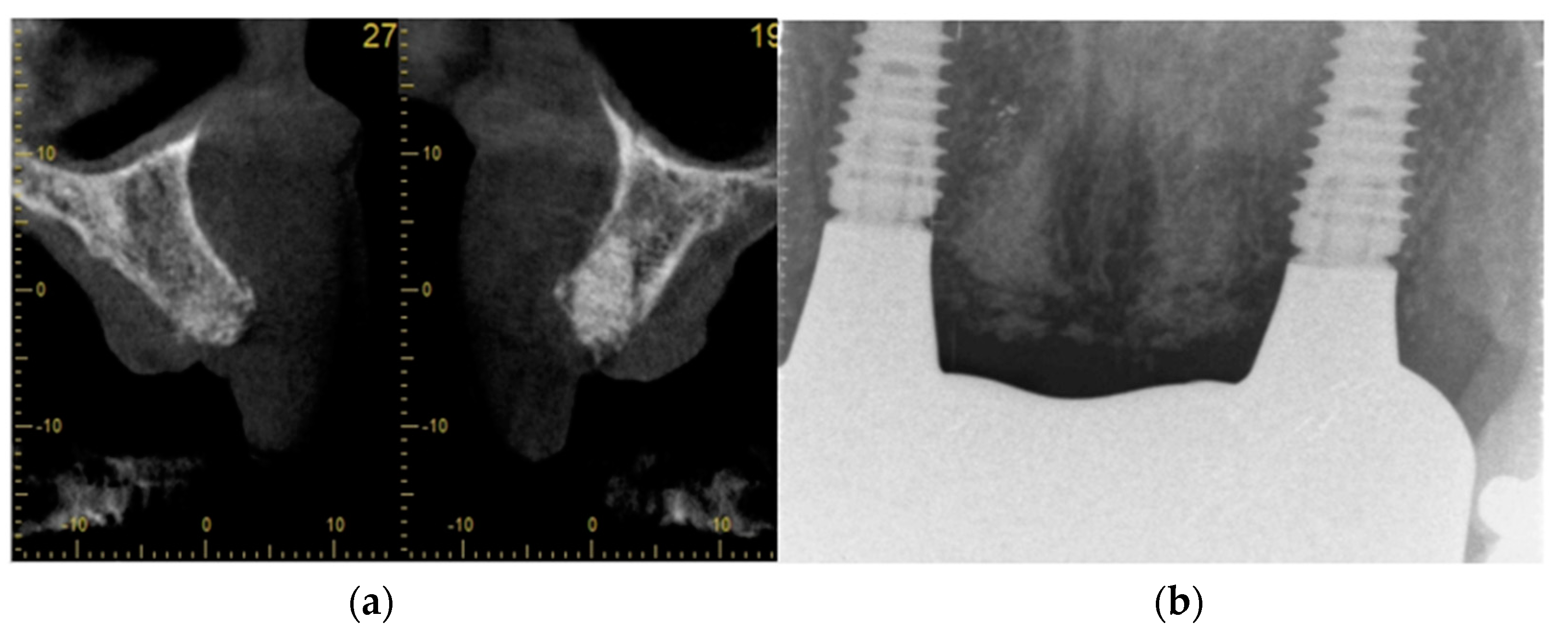
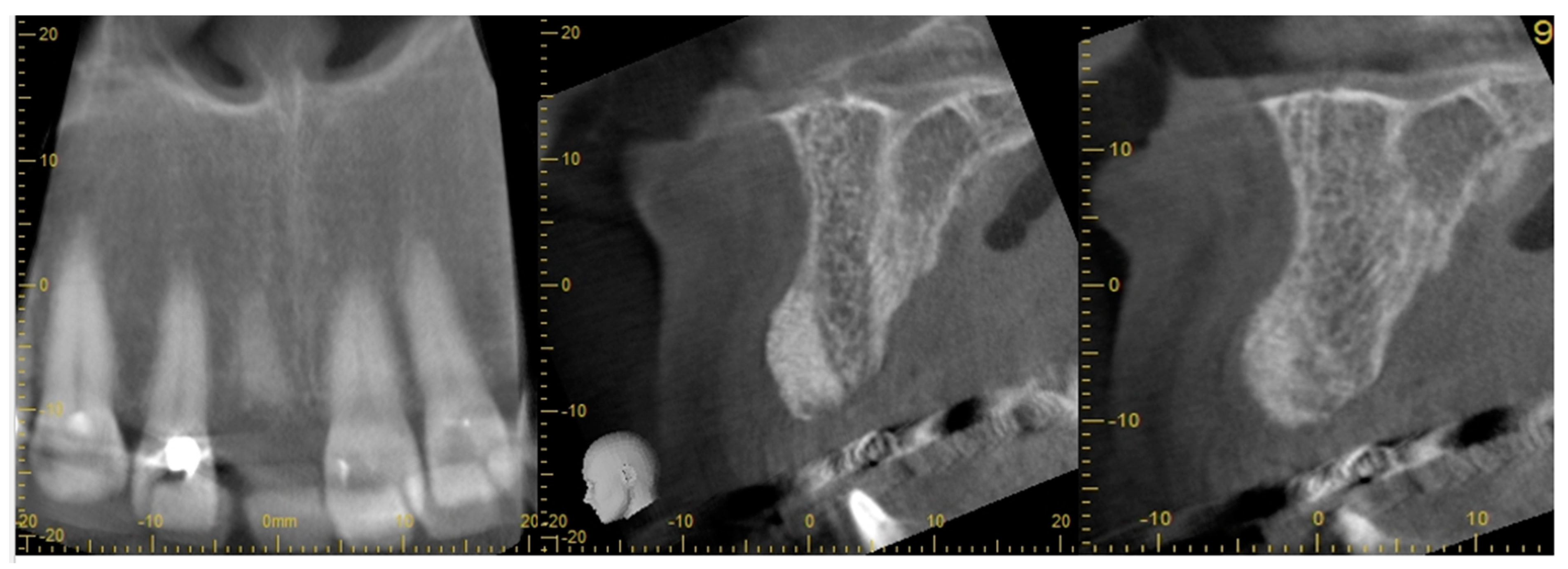
- Step 4: ARP graft healing was monitored radiologically. A CBCT was taken to plan for implant placement
- Step 5: Implant placement was carried out under LA
- Step 6: Implants were loaded early and monitored clinically and radiologically
2.2. Alveolar Ridge Preservation Technique
2.3. Outcome Measures
- (I)
- Primary outcome measures:
- (a)
- radiological assessment of bone quality and quantity after ARP using cone beam computerized tomography (CBCT)
- (b)
- Intra-operative assessment of bone quality, density, and primary implant stability during implant placement surgery
- (c)
- successful early placement and loading of implants
- (II)
- Secondary outcome measures:
- (a)
- presence or absence of implant mobility at the time of loading
- (b)
- need for additional grafting at the time of implantation
- (c)
- radiological assessment of implant integration and marginal bone integrity after loading.
2.4. The Radiological Protocol
- (a)
- Preoperative assessment of the tooth to be extracted using periapical radiographs
- (b)
- A CBCT scan of the sockets 8 weeks after ARP, before implant placement
- (c)
- Baseline radiographs at the restorative loading stage
- (d)
- Periapical radiographs at 6 months and 12 months after baseline
3. Results
3.1. Case Study 1
3.2. Case Study 2
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yu, H.Y.; Chang, Y.C. A Bibliometric Analysis of Platelet-Rich Fibrin in Dentistry. Int. J. Environ. Res. Public Health 2022, 19, 12545. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Zhang, Y.; Choukroun, J.; Ghanaati, S.; Miron, R.J. Effects of an injectable platelet-rich fibrin on osteoblast behavior and bone tissue formation in comparison to platelet-rich plasma. Platelets 2018, 29, 48–55. [Google Scholar] [CrossRef]
- Pavlovic, V.; Ciric, M.; Jovanovic, V.; Trandafilovic, M.; Stojanovic, P. Platelet-rich fibrin: Basics of biological actions and protocol modifications. Open Med. 2021, 16, 446–454. [Google Scholar] [CrossRef] [PubMed]
- Marx, R.E.; Carlson, E.R.; Eichstaedt, R.M.; Schimmele, S.R.; Strauss, J.E.; Georgeff, K.R. Platelet-rich plasma: Growth factor enhancement for bone grafts. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontology 1998, 85, 638–646. [Google Scholar] [CrossRef]
- Anitua, E.; Tejero, R.; Alkhraiarpt, M.H.; Orive, G. Platelet-rich plasma to improve the bio-functionality of biomaterials. BioDrugs 2013, 27, 97–111. [Google Scholar] [CrossRef]
- Miron, R.J.; Zucchelli, G.; Pikos, M.A.; ARPlama, M.; Lee, S.; Guillemette, V.; Fujioka-Kobayashi, M.; Bishara, M.; Zhang, Y.; Wang, H.L.; et al. Use of platelet-rich fibrin in regenerative dentistry: A systematic review. Clin. Oral Investig. 2017, 21, 1913–1927. [Google Scholar] [CrossRef]
- Choukroun, J.; Ghanaati, S. Reduction of relative centrifugation force within injectable platelet-rich-fibrin (PRF) concentrates advances patients’ own inflammatory cells, platelets and growth factors: The first introduction to the low speed centrifugation concept. Eur. J. Trauma Emerg. Surg. Off. Publ. Eur. Trauma Soc. 2018, 44, 87–95. [Google Scholar] [CrossRef]
- Fujioka-Kobayashi, M.; Miron, R.J.; Hernandez, M.; Kandalam, U.; Zhang, Y.; Choukroun, J. Optimized Platelet-Rich Fibrin With the Low-Speed Concept: Growth Factor Release, Biocompatibility, and Cellular Response. J. Periodontol. 2017, 88, 112–121. [Google Scholar] [CrossRef]
- Miron, R.J.; Fujioka-Kobayashi, M.; Hernandez, M.; Kandalam, U.; Zhang, Y.; Ghanaati, S.; Choukroun, J. Injectable platelet rich fibrin (i-PRF): Opportunities in regenerative dentistry? Clin. Oral Investig. 2017, 21, 2619–2627. [Google Scholar] [CrossRef]
- Miron, R.J.; Chai, J.; Zhang, P.; Li, Y.; Wang, Y.; Mourão, C.F.A.B.; Sculean, A.; Fujioka Kobayashi, M.; Zhang, Y. A novel method for harvesting concentrated platelet-rich fibrin (C-PRF) with a 10-fold increase in platelet and leukocyte yields. Clin. Oral Investig. 2020, 24, 2819–2828. [Google Scholar] [CrossRef]
- Quirynen, M.; Pinto, N.R. Leukocyte-and Platelet-Rich Fibrin in Oral Regenerative Procedures: Evidence-Based Clinical Guidelines; Quintessenz Verlag: Berlin, Germany, 2022; Available online: https://www.sigmaaldrich.com/deepweb/assets/sigmaaldrich/marketing/global/documents/232/100/rpm-converted-to-g-force-mk.pdf (accessed on 6 April 2023).
- Choukroun, J.; Diss, A.; Simonpieri, A.; Girard, M.O.; Schoeffler, C.; Dohan, S.L.; Dohan, A.J.; Mouhyi, J.; Dohan, D.M. Platelet-rich fibrin (PRF): A second-generation platelet concentrate. Part IV: Clinical effects on tissue healing. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontology 2006, 101, e56–e60. [Google Scholar] [CrossRef]
- Kobayashi, E.; Flückiger, L.; Fujioka-Kobayashi, M.; ARPwada, K.; Sculean, A.; Schaller, B.; Miron, R.J. Comparative release of growth factors from PRP, PRF, and advanced-PRF. Clin. Oral Investig. 2016, 20, 2353–2360. [Google Scholar] [CrossRef]
- Miron, R.J.; Dham, A.; Dham, U.; Zhang, Y.; Pikos, M.A.; Sculean, A. The effect of age, gender, and time between blood draw and start of centrifugation on the size outcomes of platelet-rich fibrin (PRF) membranes. Clin. Oral Investig. 2019, 23, 2179–2185. [Google Scholar] [CrossRef]
- Miron, R.J.; Chai, J.; Zheng, S.; Feng, M.; Sculean, A.; Zhang, Y. A novel method for evaluating and quantifying cell types in platelet rich fibrin and an introduction to horizontal centrifugation. J. Biomed. Mater. Research. Part A 2019, 107, 2257–2271. [Google Scholar] [CrossRef]
- Tunalı, M.; Özdemir, H.; Küçükodacı, Z.; Akman, S.; Yaprak, E.; Toker, H.; Fıratlı, E. A novel platelet concentrate: Titanium-prepared platelet-rich fibrin. Biomed Res. Int. 2014, 2014, 209548. [Google Scholar] [CrossRef]
- You, J.S.; Kim, S.G.; Oh, J.S.; Kim, J.S. Effects of Platelet-Derived Material (Platelet-Rich Fibrin) on Bone Regeneration. Implant. Dent. 2019, 28, 244–255. [Google Scholar] [CrossRef]
- Şimşek, S.; Özeç, İ.; Kürkçü, M.; Benlidayı, E. Histomorphometric Evaluation of Bone Formation in Peri-Implant Defects Treated with Different Regeneration Techniques: An Experimental Study in a Rabbit Model. J. Oral Maxillofac. Surg. 2016, 74, 1757–1764. [Google Scholar] [CrossRef]
- Oliveira, M.R.; Silva, A.D.; Ferreira, S.; Avelino, C.C.; Garcia, I.R., Jr.; Mariano, R.C. Influence of the association between platelet-rich fibrin and bovine bone on bone regeneration. A histomorphometric study in the calvaria of rats. Int. J. Oral. Maxillofac. Surg. 2015, 44, 649–655. [Google Scholar] [CrossRef]
- Phuong Tran, T.T.; Vu Pham, T.A. Effect of advanced and injectable platelet-rich fibrins against Aggregatibacter actinomycetemcomitans in subjects with or without periodontal diseases. J. Dent. Sci. 2023, 18, 491–496. [Google Scholar] [CrossRef]
- Ucer, C.; Khan, R.S. Extraction Socket Augmentation with Autologous Platelet-Rich Fibrin (PRF): The Rationale for Socket Augmentation. Dent. J. 2023, 11, 196. [Google Scholar] [CrossRef]
- Miron, R.J.; Fujioka-Kobayashi, M.; Sculean, A.; Zhang, Y. Optimization of platelet-rich fibrin. Periodontol 2000 2023. Epub ahead of print. [Google Scholar] [CrossRef]
- Zwittnig, K.; Kirnbauer, B.; Jakse, N.; Schlenke, P.; Mischak, I.; Ghanaati, S.; Al-Maawi, S.; Végh, D.; Payer, M.; Zrnc, T.A. Growth Factor Release within Liquid and Solid PRF. J. Clin. Med. 2022, 11, 5070. [Google Scholar] [CrossRef] [PubMed]
- ARPmmartino, G.; Dohan Ehrenfest, D.M.; Carile, F.; Tia, M.; Bucci, P. Prevention of hemorrhagic complications after dental extractions into open heart surgery patients under anticoagulant therapy: The use of leukocyte- and platelet-rich fibrin. J. Oral Implantol. 2011, 37, 681–690. [Google Scholar] [CrossRef]
- Yuan, S.; Li, Q.; Chen, K.; Mu, Z.; Chen, T.; Wang, H.; Ji, P. Ridge preservation applying a novel hydrogel for early angiogenesis and osteogenesis evaluation: An experimental study in canine. J. Biol. Eng. 2021, 15, 19. [Google Scholar] [CrossRef]
- Temmerman, A.; Vandessel, J.; Castro, A.; Jacobs, R.; Teughels, W.; Pinto, N.; Quirynen, M. The use of leucocyte and platelet-rich fibrin in socket management and ridge preservation: A split-mouth, randomized, controlled clinical trial. J. Clin. Periodontol. 2016, 43, 990–999. [Google Scholar] [CrossRef]
- Chenchev, I.L.; Ivanova, V.V.; Neychev, D.Z.; Cholakova, R.B. Application of platelet-rich fibrin and injectable platelet-rich fibrin in combination of bone substitute material for alveolar ridge augmentation-a case report. Folia Medica 2017, 59, 362–366. [Google Scholar] [CrossRef]
- Anitua, E.; Murias-Freijo, A.; AlkhraiARPt, M.H.; Orive, G. Clinical, radiographical, and histological outcomes of plasma rich in growth factors in extraction socket: A randomized controlled clinical trial. Clin. Oral Investig. 2015, 19, 589–600. [Google Scholar] [CrossRef]
- Chappuis, V.; Engel, O.; Reyes, M.; Shahim, K.; Nolte, L.P.; Buser, D. Ridge alterations post-extraction in the esthetic zone: A 3D analysis with CBCT. J. Dent. Res. 2013, 92, 195S–201S. [Google Scholar] [CrossRef]
- Castro, A.B.; Van Dessel, J.; Temmerman, A.; Jacobs, R.; Quirynen, M. Effect of different platelet-rich fibrin matrices for ridge preservation in multiple tooth extractions: A split-mouth randomized controlled clinical trial. J. Clin. Periodontol. 2021, 48, 984–995. [Google Scholar] [CrossRef]
- Wu, C.L.; Lee, S.S.; TARPi, C.H.; Lu, K.H.; Zhao, J.H.; Chang, Y.C. Platelet-rich fibrin increases cell attachment, proliferation and collagen-related protein expression of human osteoblasts. Aust. Dent. J. 2012, 57, 207–212. [Google Scholar] [CrossRef]
- Al-Maawi, S.; Becker, K.; Schwarz, F.; ARPder, R.; Ghanaati, S. Efficacy of platelet-rich fibrin in promoting the healing of extraction sockets: A systematic review. Int. J. Implant. Dent. 2021, 7, 117. [Google Scholar] [CrossRef] [PubMed]
- Clark, D.; Rajendran, Y.; Paydar, S.; Ho, S.; Cox, D.; Ryder, M.; Dollard, J.; Kao, R.T. Advanced platelet-rich fibrin and freeze-dried bone allograft for ridge preservation: A randomized controlled clinical trial. J. Periodontol. 2018, 89, 379–387. [Google Scholar] [CrossRef] [PubMed]
- Bennardo, F.; Gallelli, L.; Palleria, C.; Colosimo, M.; Fortunato, L.; De Sarro, G.; Giudice, A. Can platelet-rich fibrin act as a natural carrier for antibiotics delivery? A proof-of-concept study for oral surgical procedures. BMC Oral Health 2023, 23, 134. [Google Scholar] [CrossRef] [PubMed]
- Hauser, F.; Gaydarov, N.; Badoud, I.; Vazquez, L.; Bernard, J.P.; Ammann, P. Clinical and histological evaluation of postextraction platelet-rich fibrin socket filling: A prospective randomized controlled study. Implant. Dent. 2013, 22, 295–303. [Google Scholar] [CrossRef]
- Sisti, A.; Canullo, L.; Mottola, M.P.; Covani, U.; Barone, A.; Botticelli, D. Clinical evaluation of a ridge augmentation procedure for the severely resorbed alveolar socket: Multicenter randomized controlled trial, preliminary results. Clin. Oral Implants Res. 2012, 23, 526–535. [Google Scholar] [CrossRef] [PubMed]
- Mardas, N.; Trullenque-Eriksson, A.; MacBeth, N.; Petrie, A.; Donos, N. Does ridge preservation following tooth extraction improve implant treatment outcomes: A systematic review: Group 4: Therapeutic concepts & methods. Clin. Oral Implants Res. 2015, 26, 180–201. [Google Scholar] [CrossRef] [PubMed]
- Öncü, E.; Alaaddinoğlu, E.E. The effect of platelet-rich fibrin on implant stability. Int. J. Oral Maxillofac. Implant. 2015, 30, 578–582. [Google Scholar] [CrossRef] [PubMed]
- Öncü, E.; Erbeyoğlu, A.A. Enhancement of Immediate Implant Stability and Recovery Using Platelet-Rich Fibrin. Int. J. Periodontics Restor. Dent. 2019, 39, e58–e63. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PRF Preparation | Tube | RCF (g) | Time (min) | Speed (rpm) | Evidence |
|---|---|---|---|---|---|
| Solid Matrix | |||||
| L-PRF | Glass or Silica coated | 408 | 12 | 2700 | Choukroun, 2001 [12] |
| A-PRF | Glass or Silica coated | 194 | 14 | 1500 | Ghanaati et al., 2014 [7] |
| A-PRF+ | Glass or Silica coated | 145 | 8 | 1300 | Fujioka-Kobayashi et al., 2016 [13] |
| Liquid matrix | |||||
| i-PRF | Plastic (PET) | 60 | 3 | 700 | Miron et al., 2017 [8] |
| C-PRF | Plastic (PET) | 408 | 12 | 2700 | Miron et al., 2020 [10] |
| Radius (cm) | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 |
|---|---|---|---|---|---|---|---|---|---|---|
| Speed (rpm) | ||||||||||
| 1000 | 45 | 56 | 67 | 78 | 89 | 101 | 112 | 123 | 134 | 145 |
| 1500 | 101 | 126 | 151 | 176 | 201 | 226 | 252 | 277 | 302 | 327 |
| 2000 | 179 | 224 | 268 | 313 | 358 | 402 | 447 | 492 | 537 | 581 |
| 2500 | 280 | 349 | 419 | 489 | 559 | 629 | 699 | 769 | 839 | 908 |
| 3000 | 402 | 503 | 604 | 704 | 805 | 906 | 1006 | 1107 | 1207 | 1308 |
| Growth Factors | Functions |
|---|---|
| Transforming Growth Factor (TGF) | Growth of endothelial vascular cells, cell recruitment, and proliferation in wound healing. Inhibits osteoclast formation and bone resorption. Stimulates fibronectin and collagen production. |
| Epidermal Growth Factor (EGF) | Promotion of mesenchymal cell proliferation and differentiation, epithelial cell growth, and angiogenesis |
| Vascular Endothelial Growth Factor (VEGF) | Restores oxygen supply to the injured tissue. Promotes repair and growth of vascular endothelial cells, and angiogenesis |
| Platelet-Derived Growth Factors (PDGF) | Cell growth, proliferation of smooth muscle cells within vascular tissue, angiogenesis, and collagen production Provokes proliferation of mesenchymal cell lineage, and enables macrophage chemotaxis |
| Insulin-like Growth Factor (IGF) | Cell proliferation, cell-to-cell communications, stimulates chemotaxis and activation of osteoblasts and bone formation, and induces mitogenesis of mesenchymal cells |
| Fibroblast Growth Factor (FGF) | Tissue repair, cell growth, hyaluronic acid and collagen production |
| Case No: | Age, Gender, Medical History | ARP Technique | AR Volume | BQ after ARP | PS | BQ at Implant Placement | Secondary Grafting at Implant Placement | Time Since ARP | Early Loading | CBS |
|---|---|---|---|---|---|---|---|---|---|---|
| Case 1 | 60, male, prediabetes, non-smoker with no medication | open ARP | Full contour preserved | excellent | high | D2-3 | None | 8 weeks | 6 weeks | No crestal bone loss |
| Case 2 (implant 1) | 55, female, hay fever, non-smoker | open ARP | Full contour preserved | excellent | high | D2-4 | None | 9 weeks | 7 weeks | No crestal bone loss |
| Case 2 (implant 2) | 55, female, hay fever, non-smoker | open ARP | Full contour preserved | excellent | high | D2-4 | None | 9 weeks | 8 weeks | No crestal bone loss |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ucer, C.; Khan, R.S. Alveolar Ridge Preservation with Autologous Platelet-Rich Fibrin (PRF): Case Reports and the Rationale. Dent. J. 2023, 11, 244. https://doi.org/10.3390/dj11100244
Ucer C, Khan RS. Alveolar Ridge Preservation with Autologous Platelet-Rich Fibrin (PRF): Case Reports and the Rationale. Dentistry Journal. 2023; 11(10):244. https://doi.org/10.3390/dj11100244
Chicago/Turabian StyleUcer, Cemal, and Rabia S. Khan. 2023. "Alveolar Ridge Preservation with Autologous Platelet-Rich Fibrin (PRF): Case Reports and the Rationale" Dentistry Journal 11, no. 10: 244. https://doi.org/10.3390/dj11100244