
Resin Cement Residue Removal Techniques: In Vitro Analysis of Marginal Defects and Discoloration Intensity Using Micro-CT and Stereomicroscopy


Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion of Samples
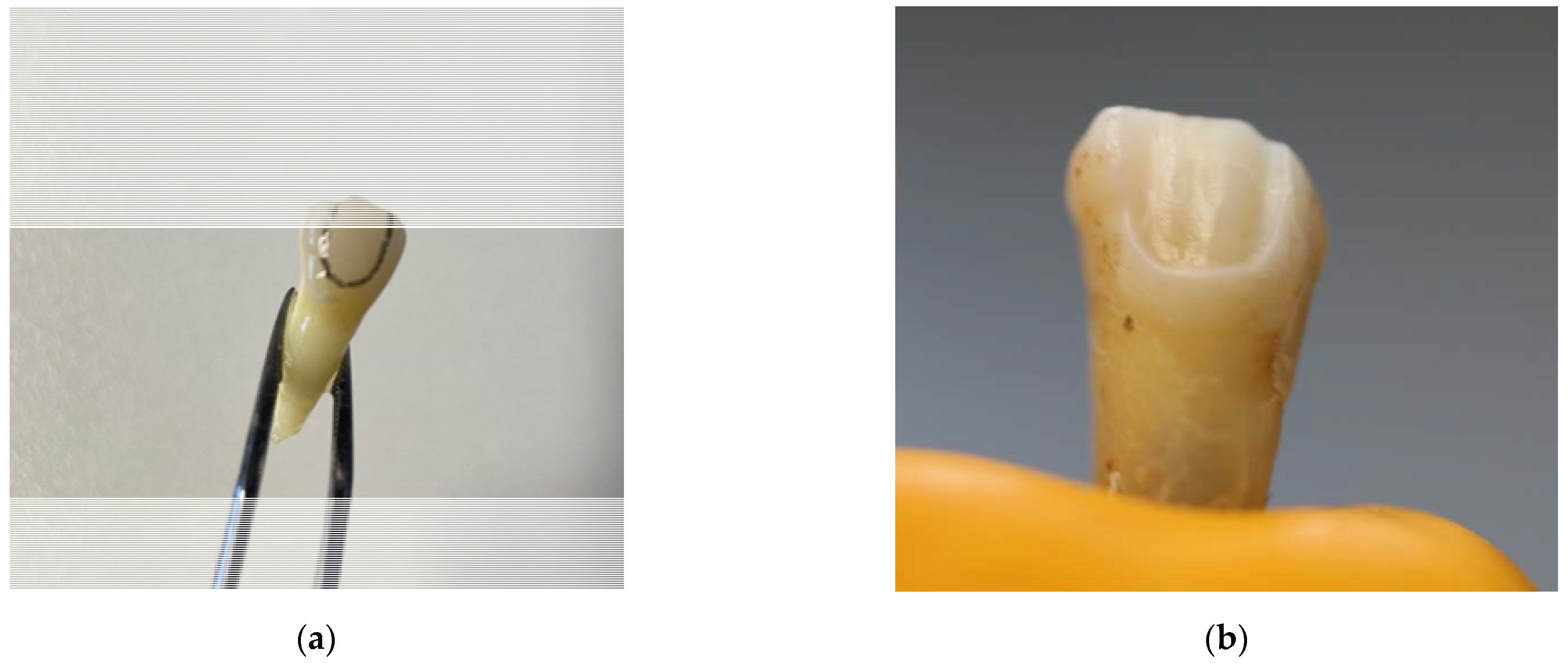
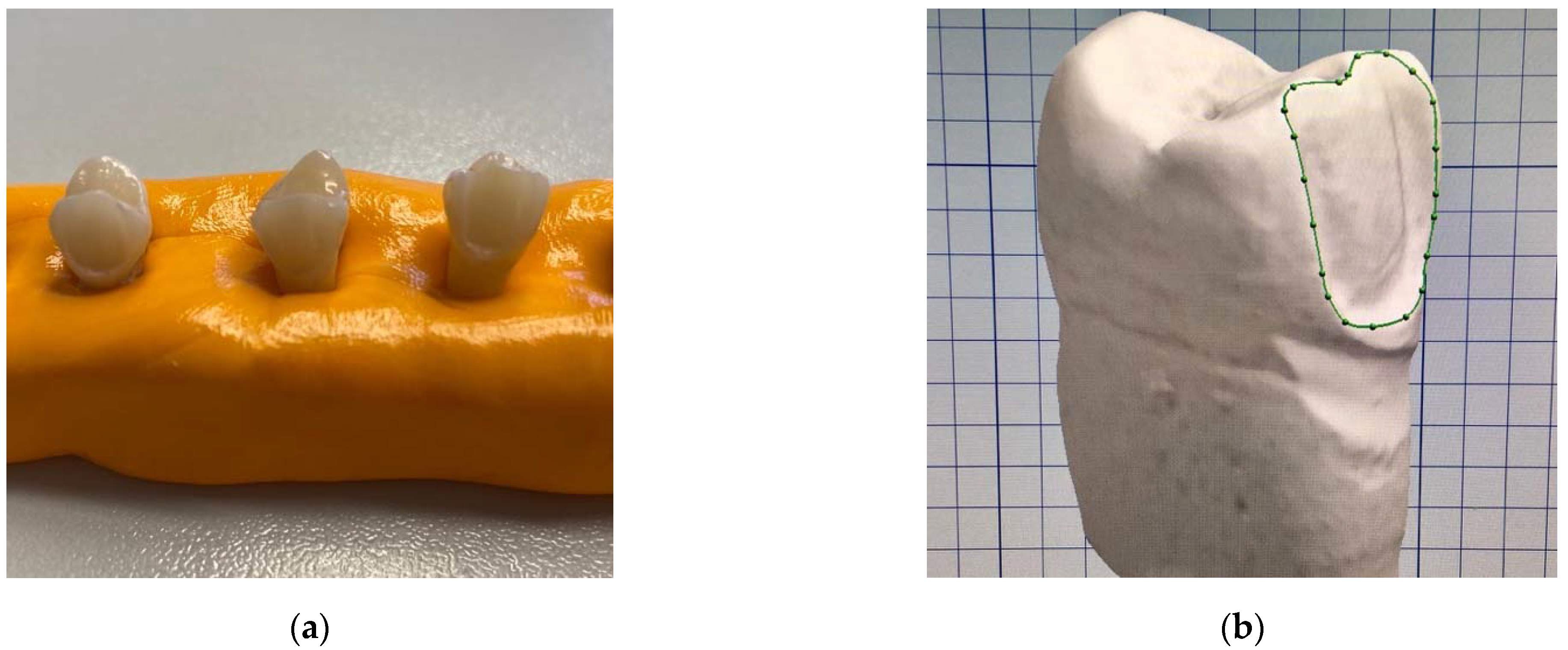
2.2. Tooth Preparation
2.3. Veneer Fabrication
2.4. Cementation
2.5. Thermocycling
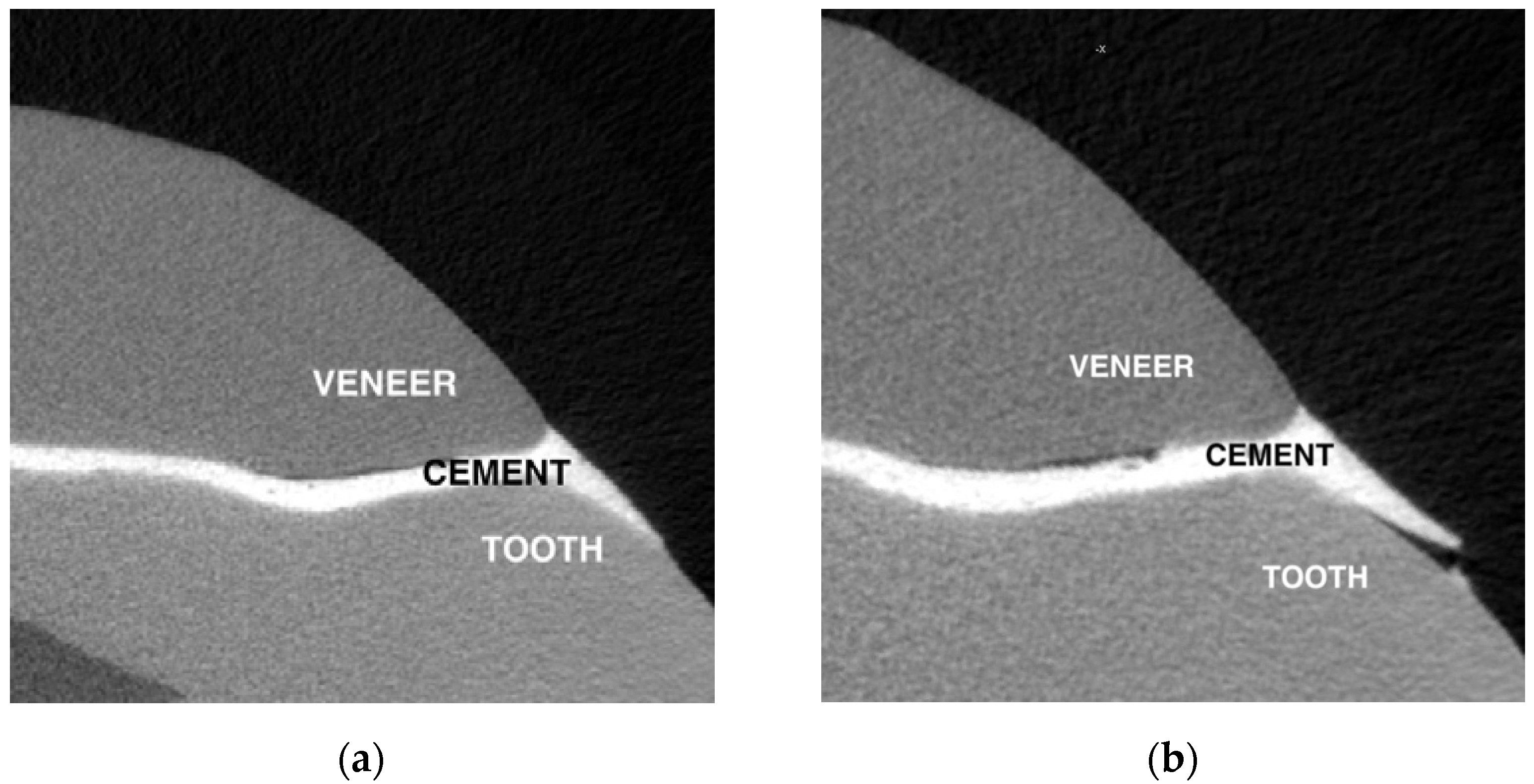
2.6. Micro-Computed Tomography (Micro-CT) Evaluation
- Number of structural defects next to enamel, next to the veneer, and in the cement layer;
- Sum of overall structural defects;
- Number of slices with cement layer underfill/irrelevant overfill/wide overfill.
2.7. Coloring
2.8. Statistical Analysis
3. Results
3.1. Size and Character of Defects
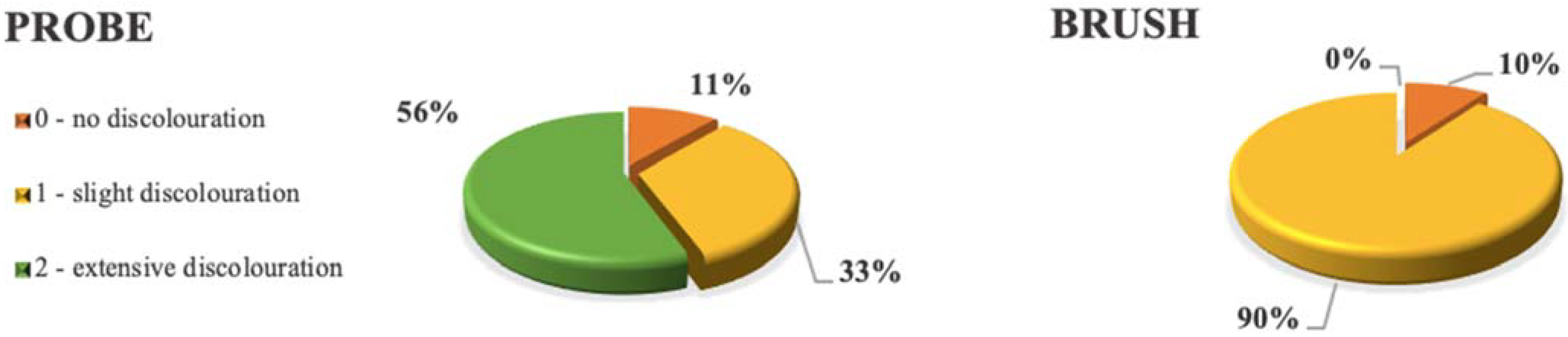
3.2. Comparison of Discoloration
3.2.1. Intensity of Discoloration
3.2.2. Depth of Dye Penetration
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Peumans, M.; Van Meerbeek, B.; Lambrechts, P.; Vanherle, G. Porcelain veneers: A review of the literature. J. Dent. 2000, 28, 163–177. [Google Scholar] [CrossRef]
- Morimoto, S.; Albanesi, R.B.; Sesma, N.; Agra, C.M.; Braga, M.M. Main Clinical Outcomes of Feldspathic Porcelain and Glass-Ceramic Laminate Veneers: A Systematic Review and Meta-Analysis of Survival and Complication Rates. Int. J. Prosthodont. 2016, 29, 38–49. [Google Scholar] [CrossRef] [PubMed]
- Alenezi, A.; Alsweed, M.; Alsidrani, S.; Chrcanovic, B.R. Long-Term Survival and Complication Rates of Porcelain Laminate Veneers in Clinical Studies: A Systematic Review. J. Clin. Med. 2021, 10, 1074. [Google Scholar] [CrossRef]
- Addison, O.; Marquis, P.M.; Fleming, G.J.P. Adhesive luting of all-ceramic restorations—The impact of cementation variables and short-term water storage on the strength of a feldspathic dental ceramic. J. Adhes. Dent. 2008, 10, 285–293. [Google Scholar]
- Stangel, I.; Nathanson, D.; Hsu, C.S. Shear Strength of the Composite Bond to Etched Porcelain. J. Dent. Res. 1987, 66, 1460–1465. [Google Scholar] [CrossRef]
- Kursoglu, P.; Motro, P.F.K.; Yurdaguven, H. Shear bond strength of resin cement to an acid etched and a laser irradiated ceramic surface. J. Adv. Prosthodont. 2013, 5, 98–103. [Google Scholar] [CrossRef] [Green Version]
- Valian, A.; Moravej-Salehi, E. Surface treatment of feldspathic porcelain: Scanning electron microscopy analysis. J. Adv. Prosthodont. 2014, 6, 387–394. [Google Scholar] [CrossRef] [Green Version]
- Aida, M.; Hayakawa, T.; Mizukawa, K. Adhesion of composite to porcelain with various surface conditions. J. Prosthet. Dent. 1995, 73, 464–470. [Google Scholar] [CrossRef]
- Blatz, M.B.; Sadan, A.; Kern, M. Resin-ceramic bonding: A review of the literature. J. Prosthet. Dent. 2003, 89, 268–274. [Google Scholar] [CrossRef] [Green Version]
- Tay, W.M.; Lynch, E.; Auger, D. Effects of some finishing techniques on cervical margins of porcelain laminates. Quintessence Int. 1987, 18, 599–602. [Google Scholar]
- Calamia, J.R.; Calamia, C.S. Porcelain Laminate Veneers: Reasons for 25 Years of Success. Dent. Clin. N. Am. 2007, 51, 399–417. [Google Scholar] [CrossRef]
- Stegall, D.; Tantbirojn, D.; Perdigão, J.; Versluis, A. Does Tack Curing Luting Cements Affect the Final Cure? J. Adhes. Dent. 2017, 19, 239. [Google Scholar] [CrossRef] [PubMed]
- Hamlett, K. The art of veneer cementation. Alpha Omegan 2009, 102, 128–132. [Google Scholar] [CrossRef] [PubMed]
- IPS e.max CAD Instructions for Use. Available online: https://downloadcenter.ivoclarvivadent.com/#search-info-211=279006%2C1&details=13022 (accessed on 4 December 2021).
- Panavia V5 Instructions for Use. Available online: https://kuraraydental.com/wp-content/uploads/2018/05/panavia-v5-ifu.pdf (accessed on 4 December 2021).
- Haralur, S.B. Microleakage of porcelain laminate veneers cemented with different bonding techniques. J. Clin. Exp. Dent. 2018, 10, 166–171. [Google Scholar]
- Aldhafyan, M.; Silikas, N.; Watts, D.C. Influence of curing modes on conversion and shrinkage of dual-cure resin-cements. Dent. Mater. 2021, 38, 194–203. [Google Scholar] [CrossRef] [PubMed]
- Braga, R.R.; Ferracane, J.L.; Condon, J.R. Polymerization contraction stress in dual-cure cements and its effect on interfacial integrity of bonded inlays. J. Dent. 2002, 30, 333–340. [Google Scholar] [CrossRef]
- Chen, L.; Suh, B.I.; Gleave, C.; Choi, W.J.; Hyun, J.; Nam, J. Effects of light-, self-, and tack-curing on degree of conversion and physical strength of dual-cure resin cements. Am. J. Dent. 2016, 29, 67–70. [Google Scholar] [PubMed]
- De Souza, G.; Braga, R.R.; Cesar, P.F.; Lopes, G.C. Correlation between clinical performance and degree of conversion of resin cements: A literature review. J. Appl. Oral Sci. 2015, 23, 358–368. [Google Scholar] [CrossRef] [Green Version]
- Magalhães, A.P.R.; Cardoso, P.d.C.; de Souza, J.B.; Fonseca, R.B.; Pires-de-Souza, F.d.C.P.; Lopez, L.G. Influence of Activation Mode of Resin Cement on the Shade of Porcelain Veneers: Influence of Cement Activation Mode on the Color of Veneers. J. Prosthodont. 2014, 23, 291–295. [Google Scholar] [CrossRef]
- Marchionatti, A.M.E.; Wandscher, V.F.; May, M.M.; Bottino, M.A.; May, L.G. Color stability of ceramic laminate veneers cemented with light-polymerizing and dual-polymerizing luting agent: A split-mouth randomized clinical trial. J. Prosthet. Dent. 2017, 118, 604–610. [Google Scholar] [CrossRef] [Green Version]
- Kilinc, E.; Antonson, S.A.; Hardigan, P.C.; Kesercioglu, A. Resin cement color stability and its influence on the final shade of all-ceramics. J. Dent. 2011, 39 (Suppl. 1), e30–e36. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, M. Adhesive Dentistry: Understanding the Science and Achieving Clinical Success. Dent. Clin. N. Am. 2020, 64, 633–643. [Google Scholar] [CrossRef]
- Tabatabaei, M.H.; Matinfard, F.; Ahmadi, E.; Ranjbar Omrani, L.; Sadeghi Mahounak, F. Color Stability of Ceramic Veneers Cemented with Self-Adhesive Cements after Accelerated Aging. Front. Dent. 2019, 16, 393–401. [Google Scholar] [CrossRef]
- Ibarra, G.; Johnson, G.H.; Geurtsen, W.; Vargas, M.A. Microleakage of porcelain veneer restorations bonded to enamel and dentin with a new self-adhesive resin-based dental cement. Dent. Mater. 2007, 23, 218–225. [Google Scholar] [CrossRef] [PubMed]
- Sinjari, B.; Santilli, M.; D’Addazio, G.; Rexhepi, I.; Gigante, A.; Caputi, S.; Traini, T. Influence of Dentine Pre-Treatment by Sandblasting with Aluminum Oxide in Adhesive Restorations. An In Vitro Study. Materials 2020, 13, 3026. [Google Scholar] [CrossRef] [PubMed]
- Rohr, N.; Fischer, J. Tooth surface treatment strategies for adhesive cementation. J. Adv. Prosthodont. 2017, 9, 85–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Straface, A.; Rupp, L.; Gintaute, A.; Fischer, J.; Zitzmann, N.U.; Rohr, N. HF etching of CAD/CAM materials: Influence of HF concentration and etching time on shear bond strength. Head Face Med. 2019, 15, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Małysa, A.; Weżgowiec, J.; Danel, D.; Boening, K.; Walczak, K.; Więckiewicz, M. Bond strength of modern self-adhesive resin cements to human dentin and different CAD/CAM ceramics. Acta Bioeng. Biomech. 2020, 22, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Ghajghouj, O.; Taşar-Faruk, S. Evaluation of Fracture Resistance and Microleakage of Endocrowns with Different Intracoronal Depths and Restorative Materials Luted with Various Resin Cements. Materials 2019, 12, 2528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aboushelib, M.N.; Elmahy, W.A.; Ghazy, M.H. Internal adaptation, marginal accuracy and microleakage of a pressable versus a machinable ceramic laminate veneers. J. Dent. 2012, 40, 670–677. [Google Scholar] [CrossRef] [PubMed]
- Yuce, M.; Ulusoy, M.; Turk, A.G. Comparison of Marginal and Internal Adaptation of Heat-Pressed and CAD/CAM Porcelain Laminate Veneers and a 2-Year Follow-up. J. Prosthodont. 2019, 28, 504–510. [Google Scholar] [CrossRef]
- Qahtani, W.M.S.A.L. Assessment of Marginal Opening for Different Cementation Techniques for Heat-Pressed Ceramic Veneers. Niger. J. Clin. Pract. 2020, 23, 1643–1647. [Google Scholar] [CrossRef] [PubMed]
- Chieffi, N.; Chersoni, S.; Papacchini, F.; Vano, M.; Goracci, C.; Davidson, C.L.; Tay, F.R.; Ferrari, M. The effect of application sustained seating pressure on adhesive luting procedure. Dent. Mater. 2006, 23, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Harasani, M.H.; Isidor, F.; Kaaber, S. Marginal fit of porcelain and indirect composite laminate veneers under in vitro conditions. Eur. J. Oral Sci. 1991, 99, 262–268. [Google Scholar] [CrossRef]
- Lee, J.J.; Nettey-Marbell, A.; Cook, A., Jr.; Pimenta, L.A.; Leonard, R.; Ritter, A.V. Using extracted teeth for research: The effect of storage medium and sterilization on dentin bond strengths. J. Am. Dent. Assoc. 2007, 138, 1599–1603. [Google Scholar] [CrossRef] [PubMed]
- Mobarak, E.H.; El-Badrawy, W.; Pashley, D.H.; Jamjoom, H. Effect of pretest storage conditions of extracted teeth on their dentin bond strengths. J. Prosthet. Dent. 2010, 104, 92–97. [Google Scholar] [CrossRef]
- Armstrong, S.; Breschi, L.; Özcan, M.; Pfefferkorn, F.; Ferrari, M.; Van Meerbeek, B. Academy of Dental Materials guidance on in vitro testing of dental composite bonding effectiveness to dentin/enamel using micro-tensile bond strength (μTBS) approach. Dent. Mater. 2017, 33, 133–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, K.Y.; Mooney, D.J. Alginate: Properties and biomedical applications. Prog. Polym. Sci. 2012, 37, 106–126. [Google Scholar] [CrossRef] [Green Version]
- Turgut, S.; Bagis, B. Colour stability of laminate veneers: An in vitro study. J. Dent. 2011, 39, e57–e64. [Google Scholar] [CrossRef] [PubMed]
- McKinney, J.E.; Wu, W. Chemical Softening and Wear of Dental Composites. J. Dent. Res. 1985, 64, 1326–1331. [Google Scholar] [CrossRef]
- Roulet, J.-F.; Wälti, C. Influence of oral fluid on composite resin and glass-ionomer cement. J. Prosthet. Dent. 1984, 52, 182–189. [Google Scholar] [CrossRef]
- Vrijhoef, M.M.A.; Hendriks, F.H.J.; Letzel, H. Loss of substance of dental composite restorations. Dent. Mater. 1985, 1, 101–105. [Google Scholar] [CrossRef]
- Barclay, C.W.; Spence, D.; Laird, W.R.E. Intra-oral temperatures during function. J. Oral Rehabil. 2005, 32, 886–894. [Google Scholar] [CrossRef]
- Ernst, C.-P.; Canbek, K.; Euler, T.; Willershausen, B. In vivo validation of the historical in vitro thermocycling temperature range for dental materials testing. Clin. Oral. Investig. 2004, 8, 130–138. [Google Scholar] [CrossRef] [PubMed]
- Mathew, M.; Parameswaran Nair, E.K.; Krishnan, V.K. Bonding agent is a decisive factor in determining the marginal leakage of dental composites subjected to thermal cycling: An in vitro study. J. Oral Rehabil. 2001, 28, 68–77. [Google Scholar] [CrossRef] [PubMed]
- Hahnel, S.; Henrich, A.; Bürgers, R.; Handel, G.; Rosentritt, M. Investigation of mechanical properties of modern dental composites after artificial aging for one year. Oper. Dent. 2010, 35, 412–419. [Google Scholar] [CrossRef] [PubMed]
- Assunção, W.G.; Gomes, E.A.; Barão, V.A.; Barbosa, D.B.; Delben, J.A.; Tabata, L.F. Effect of storage in artificial saliva and thermal cycling on Knoop hardness of resin denture teeth. J. Prosthodont. Res. 2010, 54, 123–127. [Google Scholar] [CrossRef] [PubMed]
- Weir, M.D.; Moreau, J.L.; Levine, E.D.; Strassler, H.E.; Chow, L.C.; Xu, H.H. Nanocomposite containing CaF(2) nanoparticles: Thermal cycling, wear and long-term water-aging. Dent. Mater. 2012, 28, 642–652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreau, J.L.; Weir, M.D.; Giuseppetti, A.A.; Chow, L.C.; Antonucci, J.M.; Xu, H.H.K. Long-term mechanical durability of dental nanocomposites containing amorphous calcium phosphate nanoparticles. J. Biomed. Mater. Res. 2012, 100, 1264–1273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawano, F.; Ohguri, T.; Ichikawa, T.; Matsumoto, N. Influence of thermal cycles in water on flexural strength of laboratory-processed composite resin. J. Oral Rehabil. 2001, 28, 703–707. [Google Scholar] [CrossRef]
- Morresi, A.L.; D’Amario, M.; Capogreco, M.; Gatto, R.; Marzo, G.; D’Arcangelo, C.; Monaco, A. Thermal cycling for restorative materials: Does a standardized protocol exist in laboratory testing? A literature review. J. Mech. Behav. Biomed. Mater. 2014, 29, 295–308. [Google Scholar] [CrossRef]
- Celebi, A.T.; Icer, E.; Eren, M.M.; Baykasoglu, C.; Mugan, A.; Yildiz, E. Thermal-stress analysis of ceramic laminate veneer restorations with different incisal preparations using micro-computed tomography-based 3D finite element models. J. Mech. Behav. Biomed. Mater. 2017, 75, 302–313. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.; Lu, C.; Wu, Y.; Zhang, X.; Arola, D.; Zhang, D. The Effects of Adhesive Type and Thickness on Stress Distribution in Molars Restored with All-Ceramic Crowns. J. Prosthodont. 2011, 20, 35–44. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.-H.; Wang, H.-W.; Lin, P.-H.; Lin, C.-L. Evaluation of early resin luting cement damage induced by voids around a circular fiber post in a root canal treated premolar by integrating micro-CT, finite element analysis and fatigue testing. Dent. Mater. 2018, 34, 1082–1088. [Google Scholar] [CrossRef]
- Uzun, I.; Keleş, A.; Arslan, H.; Güler, B.; Keskin, C.; Gündüz, K. Influence of oval and circular post placement using different resin cements on push-out bond strength and void volume analysed by micro-CT. Int. Endod. J. 2016, 49, 1175–1182. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.-H.; Lee, H.; Lin, C.-L. Early resin luting material damage around a circular fiber post in a root canal treated premolar by using micro-computerized tomographic and finite element sub-modeling analyses. J. Mech. Behav. Biomed. Mater. 2015, 51, 184–193. [Google Scholar] [CrossRef] [PubMed]
- Scotti, N.; Baldi, A.; Vergano, E.A.; Tempesta, R.M.; Alovisi, M.; Pasqualini, D.; Carpegna, G.C.; Comba, A. Tridimensional Evaluation of the Interfacial Gap in Deep Cervical Margin Restorations: A Micro-CT Study. Oper. Dent. 2020, 45, E227–E236. [Google Scholar] [CrossRef]
- Hsu, P.; Ramos, V.; Sadr, A. Microcomputed tomography evaluation of cement shrinkage under zirconia versus lithium disilicate veneers. J. Prosthet. Dent. 2021, 125, 307–315. [Google Scholar] [CrossRef] [PubMed]
- Măroiu, A.C.; Sinescu, C.; Duma, V.F.; Topală, F.; Jivănescu, A.; Popovici, P.M.; Tudor, A.; Romînu, M. Micro-CT and Microscopy Study of Internal and Marginal Gap to Tooth Surface of Crenelated versus Conventional Dental Indirect Veneers. Medicina 2021, 57, 772. [Google Scholar] [CrossRef] [PubMed]
- Sampaio, C.S.; Niemann, K.D.; Schweitzer, D.D.; Hirata, R.; Atria, P.J. Microcomputed tomography evaluation of cement film thickness of veneers and crowns made with conventional and 3D printed provisional materials. J. Esthet. Restor. Dent. 2021, 33, 487–495. [Google Scholar] [CrossRef]
- Coyne, B.M.; Wilson, N.H. A clinical evaluation of the marginal adaptation of porcelain laminate veneers. Eur. J. Prosthodont. Restor Dent 1994, 3, 87–90. [Google Scholar] [PubMed]
- Pereira, D.D.; Marquezan, M.; Grossi, M.L.; Silva Oshima, H.M. Analysis of Marginal Adaptation of Porcelain Laminate Veneers Produced by Computer-Aided Design/Computer-Assisted Manufacturing Technology: A Preliminary In Vitro Study. Int. J. Prosthodont. 2018, 31, 346–348. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Energy | 90 kVp |
|---|---|
| Intensity | 66 µA |
| Filter | Al 0.5 mm |
| Resolution | High |
| Voxel size | 7.4 µm |
| Integration time | 1000 ms |
| Data Average | 3 |
| Type of Defect | PROBE | BRUSH | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Before TC | After TC | p Value | Before TC | After TC | p Value | |||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | |||
| Overall count | 4.7 | 1.83 | 11.1 | 5.99 | 0.0123 | 8.5 | 4.22 | 10.7 | 3.89 | 0.0453 |
| In cement layer | 3.7 | 2.21 | 6.7 | 3.83 | 0.0151 | 6.9 | 3.48 | 6.5 | 2.37 | 0.8768 |
| Next to tooth | 0.7 | 0.82 | 2.8 | 1.62 | 0.0167 | 0.7 | 0.82 | 1.7 | 1.57 | 0.0165 |
| Next to veneer | 0.3 | 0.95 | 1.6 | 1.84 | 0.0892 | 0.9 | 1.37 | 2.5 | 1.51 | 0.0327 |
| Underfill | 112.9 | 174.79 | 99 | 86.22 | 0.6080 | 210.6 | 159.31 | 150.1 | 175.75 | 0.1610 |
| Wide overfill | 201.9 | 170.55 | 150.7 | 129.29 | 0.0474 | 55.9 | 79.29 | 55.2 | 78.99 | 0.1579 |
| Irrelevant overfill | 373.8 | 110.06 | 299.2 | 103.89 | 0.0469 | 389.4 | 185.06 | 314.3 | 176.15 | 0.0050 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gaile, M.; Papia, E.; Zalite, V.; Locs, J.; Soboleva, U. Resin Cement Residue Removal Techniques: In Vitro Analysis of Marginal Defects and Discoloration Intensity Using Micro-CT and Stereomicroscopy. Dent. J. 2022, 10, 55. https://doi.org/10.3390/dj10040055
Gaile M, Papia E, Zalite V, Locs J, Soboleva U. Resin Cement Residue Removal Techniques: In Vitro Analysis of Marginal Defects and Discoloration Intensity Using Micro-CT and Stereomicroscopy. Dentistry Journal. 2022; 10(4):55. https://doi.org/10.3390/dj10040055
Chicago/Turabian StyleGaile, Mara, Evaggelia Papia, Vita Zalite, Janis Locs, and Una Soboleva. 2022. "Resin Cement Residue Removal Techniques: In Vitro Analysis of Marginal Defects and Discoloration Intensity Using Micro-CT and Stereomicroscopy" Dentistry Journal 10, no. 4: 55. https://doi.org/10.3390/dj10040055