

Increased Oral Dryness and Negative Oral Health-Related Quality of Life in Older People with Overweight or Obesity

Abstract
:
1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Assessment of General Health
2.3. Assessment of Patients’ Data
2.4. Assessment of Oral Health
2.5. Assessment of Oral Health-Related Quality of Life
2.6. Statistical Analysis
3. Results
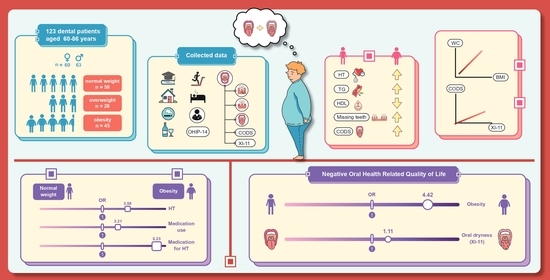
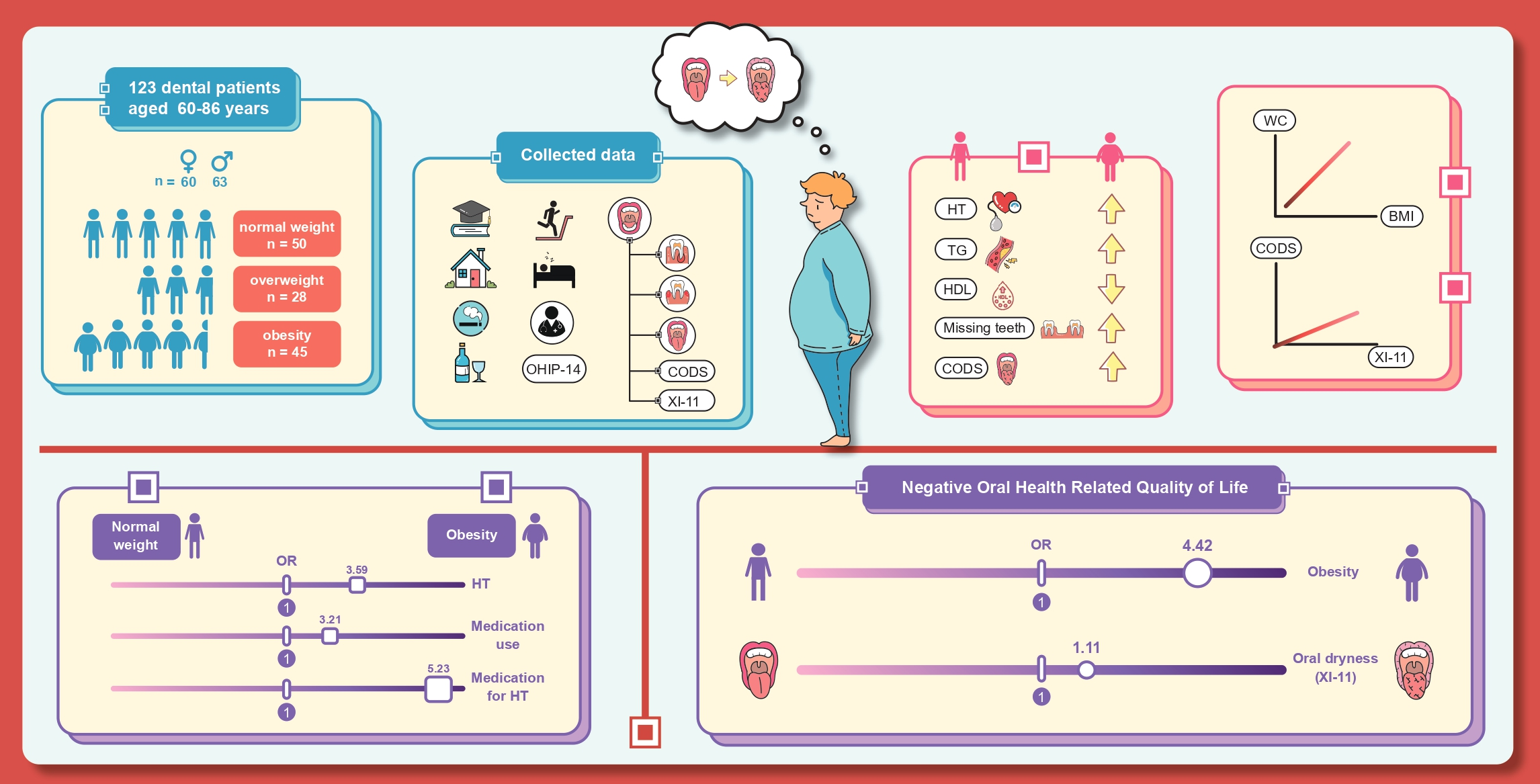
3.1. Characteristics of the Study Population
3.2. Characteristics of Oral Condition
Oral Mucosal Dryness
3.3. Oral Health-Related Quality of Life
3.4. Association of OHIP-14 with Relevant Factors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Demographic, Population and Housing Report on the 2021 Survey of the Older Persons in Thailand. 2022. Available online: http://www.nso.go.th/sites/2014en/Pages/survey/Social/Demographic,%20Population%20and%20Housing/The-Survey-Of-Elderly-In-Thailand.aspx (accessed on 25 August 2022).
- Locker, D.; Clarke, M.; Payne, B. Self-perceived oral health status, psychological well-being, and life satisfaction in an older adult population. J. Dent. Res. 2000, 79, 970–975. [Google Scholar] [CrossRef] [PubMed]
- Clementino, L.C.; de Souza, K.S.C.; Castelo-Branco, M.; Perazzo, M.F.; Ramos-Jorge, M.L.; Mattos, F.F.; Paiva, S.M.; Martins-Júnior, P.A. Top 100 most-cited oral health-related quality of life papers: Bibliometric analysis. Community Dent. Oral Epidemiol. 2022, 50, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Nammontri, O. Validation of the Thai version of the 14- item Oral Health Impact Profile (Thai OHIP-14) amongst the general Thai adult population in a community setting. J. Health Res. 2017, 31, 481–486. [Google Scholar]
- Rosli, T.I.; Chan, Y.M.; Kadir, R.A.; Hamid, T.A.A. Association between oral health-related quality of life and nutritional status among older adults in district of Kuala Pilah, Malaysia. BMC Public Health 2019, 19, 547. [Google Scholar] [CrossRef] [Green Version]
- Tenani, C.F.; De Checchi, M.H.R.; da Cunha, I.P.; Mendes, K.L.C.; Soares, G.H.; Michel-Crosato, E.; Jamieson, L.; Ju, X.; Mialhe, F.L. Factors associated with poor oral health-related quality of life among non-institutionalized Brazilian older adults: Oral health and quality of life in older adults. Spec Care Dentist. 2021, 41, 391–398. [Google Scholar] [CrossRef]
- Zhi, Q.H.; Si, Y.; Wang, X.; Tai, B.J.; Hu, D.Y.; Wang, B.; Zheng, S.G.; Liu, X.N.; Rong, W.S.; Wang, W.J.; et al. Determining the factors associated with oral health-related quality of life in Chinese elders: Findings from the fourth national survey. Community Dent. Oral Epidemiol. 2022, 50, 311–320. [Google Scholar] [CrossRef]
- Vu, H.; Vo, P.T.-D.; Kim, H.-D. Gender modified association of oral health indicators with oral health-related quality of life among Korean elders. BMC Oral Health. 2022, 22, 168. [Google Scholar]
- Bannwart, L.C.; de Moraes Melo Neto, C.L.; Goiato, M.C.; dos Santos, D.M.; da Silva Paiva, C.A.; de Araújo Moreno, N.V.; da Silva, E.V.F.; de Magalhães Bertoz, A.P. Oral health-related quality of life, dry mouth sensation, and level of anxiety in elderly patients rehabilitated with new removable dentures. Eur. J. Dent. 2022, 16, 351–359. [Google Scholar] [CrossRef]
- Dahl, K.E.; Wang, N.J.; Holst, D.; Ohrn, K. Oral health-related quality of life among adults 68-77 years old in Nord-Trøndelag, Norway. Int. J. Dent. Hyg. 2011, 9, 87–92. [Google Scholar] [CrossRef]
- Henni, S.H.; Skudutyte-Rysstad, R.; Ansteinsson, V.; Hellesø, R.; Hovden, E.A.S. Oral health and oral health-related quality of life among older adults receiving home health care services: A scoping review. Gerodontology 2022, 1–11. [Google Scholar] [CrossRef]
- Lindmark, U.; Ernsth Bravell, M.; Johansson, L.; Finkel, D. Oral health is essential for quality of life in older adults: A Swedish National Quality Register Study. Gerodontology 2021, 38, 191–198. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, L.F.S.; Wanderley, R.L.; de AraÚJo, E.C.F.; de Medeiros, M.M.D.; de Figueredo, O.M.C.; Pinheiro, M.A.; Rodrigues Garcia, R.C.M.; Cavalcanti, Y.W. Factors associated with oral health-related quality of life of institutionalized elders. Braz. Oral Res. 2021, 35, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Baniasadi, K.; Armoon, B.; Higgs, P.; Bayat, A.H.; Mohammadi Gharehghani, M.A.; Hemmat, M.; Fakhri, Y.; Mohammadi, R.; Fattah Moghaddam, L.; Schroth, R.J. The association of oral health status and socio-economic determinants with oral health-related quality of life among the elderly: A systematic review and meta-analysis. Int. J. Dent. Hyg. 2021, 19, 153–165. [Google Scholar] [CrossRef] [PubMed]
- Thanakun, S.; Pornprasertsuk-Damrongsri, S.; Izumi, Y. Increased oral inflammation, leukocytes, and leptin, and lower adiponectin in overweight or obesity. Oral Dis. 2017, 23, 956–965. [Google Scholar] [CrossRef]
- Vu, G.T.; Little, B.B.; Esterhay, R.J.; Jennings, J.A.; Creel, L.; Gettleman, L. Oral health-related quality of life in US adults with type 2 diabetes. J. Public Health Dent. 2022, 82, 79–87. [Google Scholar] [CrossRef]
- Ruokonen, H.; Nylund, K.; Meurman, J.H.; Heikkinen, A.M.; Furuholm, J.; Sorsa, T.; Roine, R.; Ortiz, F. Oral symptoms and oral health-related quality of life in patients with chronic kidney disease from predialysis to posttransplantation. Clin. Oral Investig. 2019, 23, 2207–2213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saboya, P.P.; Bodanese, L.C.; Zimmermann, P.R.; Gustavo, A.D.S.; Assumpção, C.M.; Londero, F. Metabolic syndrome and quality of life: A systematic review. Rev. Lat.-Am. De Enferm. 2016, 24, e2848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamashita, J.M.; Moura-Grec, P.G.D.; Freitas, A.R.D.; Sales-Peres, A.; Groppo, F.C.; Ceneviva, R.; Sales-Peres, S.H.D.C. Assessment of oral conditions and quality of life in morbid obese and normal weight individuals: A cross-sectional study. PLoS ONE. 2015, 10, e0129687. [Google Scholar]
- Tengku H, T.N.N.; Peh, W.Y.; Shoaib, L.A.; Baharuddin, N.A.; Vaithilingam, R.D.; Saub, R. Oral diseases and quality of life between obese and normal weight adolescents: A two-year observational study. Children 2021, 8, 435. [Google Scholar] [CrossRef]
- Pina, G.D.M.S.; Mota Carvalho, R.; Silva, B.S.D.F.; Almeida, F.T. Prevalence of hyposalivation in older people: A systematic review and meta-analysis. Gerodontology 2020, 37, 317–331. [Google Scholar] [CrossRef]
- Storbeck, T.; Qian, F.; Marek, C.; Caplan, D.; Marchini, L. Dose-dependent association between xerostomia and number of medications among older adults. Spec Care Dent. 2022, 42, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Botelho, J.; Machado, V.; Proença, L.; Oliveira, M.J.; Cavacas, M.A.; Amaro, L.; Águas, A.; Mendes, J.J. Perceived xerostomia, stress and periodontal status impact on elderly oral health-related quality of life: Findings from a cross-sectional survey. BMC Oral Health. 2020, 20, 199. [Google Scholar] [CrossRef] [PubMed]
- Temcharoen, P.; Kaewboonruang, P.; Pradipasen, M.; Srisorachart, S. The optimal cut-off points of body mass index which reflect the risk factors of cardiovascular disease in the urban Thai male population. J. Med. Assoc. Thai. 2009, 92 (Suppl. 7), S68–S74. [Google Scholar]
- Alberti, K.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.-C.; James, W.P.T.; Loria, C.M.; Smith, S.C., Jr. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [PubMed]
- Landry, R.G.; Jean, M. Periodontal Screening and Recording (PSR) Index: Precursors, utility and limitations in a clinical setting. Int. J. Dent. 2002, 52, 35–40. [Google Scholar] [CrossRef]
- Thomson, W.M.; Chalmers, J.M.; Spencer, A.J.; Williams, S.M. The Xerostomia Inventory: A multi-item approach to measuring dry mouth. Community Dent Health 1999, 16, 12–17. [Google Scholar]
- Osailan, S.M.; Pramanik, R.; Shirlaw, P.; Proctor, G.B.; Challacombe, S.J. Clinical assessment of oral dryness: Development of a scoring system related to salivary flow and mucosal wetness. Oral Surg Oral Med. Oral Pathol. Oral Radiol. 2012, 114, 597–603. [Google Scholar] [CrossRef]
- Slade, G.D. Derivation and validation of a short-form oral health impact profile. Community Dent. Oral Epidemiol. 1997, 25, 284–290. [Google Scholar] [CrossRef]
- Slade, G.D.; Nuttall, N.; Sanders, A.E.; Steele, J.G.; Allen, P.F.; Lahti, S. Impacts of oral disorders in the United Kingdom and Australia. Br. Dent. J. 2005, 198, 489–493. [Google Scholar] [CrossRef]
- Sakboonyarat, B.; Pornpongsawad, C.; Sangkool, T.; Phanmanas, C.; Kesonphaet, N.; Tangthongtawi, N.; Limsakul, A.; Assavapisitkul, R.; Thangthai, T.; Janenopparkarnjana, P.; et al. Trends, prevalence and associated factors of obesity among adults in a rural community in Thailand: Serial cross-sectional surveys, 2012 and 2018. BMC Public Health 2020, 20, 850. [Google Scholar] [CrossRef]
- Jitnarin, N.; Kosulwat, V.; Rojroongwasinkul, N.; Boonpraderm, A.; Haddock, C.K.; Poston, W.S.C. Prevalence of overweight and obesity in Thai population: Results of the National Thai Food Consumption Survey. Eat Weight Disord. 2011, 16, e242–e249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bajgai, G.P.; Okuma, N.; Khovidhunkit, S.-O.P.; Thanakun, S. Comparison of measured blood pressure levels, hypertension history, oral diseases, and associated factors among Thai dental patients. J. Oral Sci. 2022, 64, 236–241. [Google Scholar] [CrossRef] [PubMed]
- Sanguansin, N.; Chinwanitcharoen, P.; Asavarachan, S.; Sasiwilasakorn, C.; Chaikornkij, V.; Thanakun, S.; Vuddhakanok, S. Emerged medically compromised conditions in Thai patients visiting a private dental school. World J. Dent. 2022, 13, 394–399. [Google Scholar] [CrossRef]
- Hall, J.E.; Do Carmo, J.M.; Da Silva, A.A.; Wang, Z.; Hall, M.E. Obesity-induced hypertension. Circ. Res. 2015, 116, 991–1006. [Google Scholar] [CrossRef] [Green Version]
- Sato, M.; Kurokawa, A.; Sugimoto, H.; Yasuhara, Y.; Nakae, H.; Shinohara, Y.; Tanioka, T.; Iga, H.; Hinode, D.; Suzuki, Y.; et al. Relationship among health related quality of life, quality of sleep, and oral health condition. Health 2018, 10, 204–214. [Google Scholar] [CrossRef]
- Grandner, M.A.; Chakravorty, S.; Perlis, M.L.; Oliver, L.; Gurubhagavatula, I. Habitual sleep duration associated with self-reported and objectively determined cardiometabolic risk factors. Sleep Med. 2014, 15, 42–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhi, T.-F.; Sun, X.-M.; Li, S.-J.; Wang, Q.-S.; Cai, J.; Li, L.-Z.; Li, Y.-X.; Xu, M.-J.; Wang, Y.; Chu, X.F.; et al. Associations of sleep duration and sleep quality with life satisfaction in elderly Chinese: The mediating role of depression. Arch. Gerontol. Geriat. 2016, 65, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Herrera, M.; Silvestre-Rangil, J.; Silvestre, F.J. Association between obesity and periodontal disease. A systematic review of epidemiological studies and controlled clinical trials. Med. Oral Patol. Oral Cir. Bucal. 2017, 22, e708–e715. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.-P.; Yu, H.-C.; Lin, T.-H.; Wang, Y.-H.; Chang, Y.-C. Association between obesity and chronic periodontitis: A nationwide population-based cohort study in Taiwan. Medicine 2021, 100, e27506. [Google Scholar] [CrossRef]
- Cortelli, S.C.; Peralta, F.S.; Nogueira, L.M.R.; Costa, F.O.; Aquino, D.R.; Rovai, E.S.; Cortelli, J.R. Periodontal therapy on the oral health-related quality of life of obese and non-obese individuals. Odontology 2021, 109, 956–964. [Google Scholar] [CrossRef]
- Wanichkittikul, N.; Laohapand, P.; Mansa-nguan, C.; Thanakun, S. Periodontal treatment improves serum levels of leptin, adiponectin, and C-reactive protein in Thai patients with overweight or obesity. Int. J. Dent. 2021, 2021, 6660097. [Google Scholar] [CrossRef] [PubMed]
- Somsak, K.; Kaewplung, O. The effects of the number of natural teeth and posterior occluding pairs on the oral health-related quality of life in elderly dental patients. Gerodontology 2016, 33, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Tan, H.; Peres, K.G.; Peres, M.A. Retention of teeth and oral health–related quality of life. J. Dent. Res. 2016, 95, 1350–1357. [Google Scholar] [CrossRef] [PubMed]
- Tôrres, L.H.d.N.; De Marchi, R.J.; Hilgert, J.B.; Hugo, F.N.; Ismail, A.I.; Antunes, J.L.F.; Sousa, M.d.L.R.d. Oral health and obesity in Brazilian elders: A longitudinal study. Community Dent. Oral Epidemiol. 2020, 48, 540–548. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.H.; Kim, M.J.; Kho, H.S. Oral health-related quality of life and associated factors in patients with xerostomia. Int. J. Dent. Hyg. 2021, 19, 313–322. [Google Scholar] [CrossRef]
- Jager, D.H.J.; Bots, C.P.; Forouzanfar, T.; Brand, H.S. Clinical oral dryness score: Evaluation of a new screening method for oral dryness. Odontology 2018, 106, 439–444. [Google Scholar] [CrossRef] [Green Version]
- Ohara, Y.; Kawai, H.; Shirobe, M.; Iwasaki, M.; Motokawa, K.; Edahiro, A.; Kim, H.; Fujiwara, Y.; Ihara, K.; Watanabe, Y.; et al. Association between dry mouth and physical frailty among community-dwelling older adults in Japan: The Otassha Study. Gerodontology 2022, 39, 41–48. [Google Scholar] [CrossRef]
- Saleh, J.; Figueiredo, M.A.Z.; Cherubini, K.; Salum, F.G. Salivary hypofunction: An update on aetiology, diagnosis and therapeutics. Arch. Oral Biol. 2015, 60, 242–255. [Google Scholar] [PubMed]

{kind=link}
| Participants (N = 123) | p-Value | |||
|---|---|---|---|---|
| Normal Weight (n = 50) | Overweight (n = 28) | Obesity (n = 45) | ||
| Age | 65 (63, 68) | 66 (62, 69) | 65 (61, 69) | 0.767 |
| Sex | ||||
| Male | 25 (50.0) | 14 (50.0) | 24 (53.3) | 0.939 |
| Female | 25 (50.0) | 14 (50.0) | 21 (46.7) | |
| BMI (kg/m2) | 21.1 (20.2, 22.0) | 24.2 (23.4, 24.8) | 27.6 (26.2, 29.6) | <0.001 * |
| WC (cm) | ||||
| Male | 80 (78, 82) | 89 (87, 91) | 97 (90, 102) | <0.001 * |
| Female | 75 (68, 78) | 83 (79, 87) | 87 (84, 96) | <0.001 * |
| FPG (mg/dL) | 100 (95, 112) | 100 (92, 117) | 104 (96, 115) | 0.335 |
| HDL (mg/dL) | ||||
| Male | 55 (47, 66) | 57 (52, 70) | 51 (45, 57) | 0.040 |
| Female | 75 (64, 81) | 62 (46, 74) | 52 (47, 61) | <0.001 * |
| TG (mg/dL) | 79 (63, 121) | 97(7, 134) | 116 (86, 178) | <0.001 * |
| Systolic BP (mmHg) | 121 (111, 131) | 132 (119, 138) | 128 (121, 141) | 0.017 * |
| Diastolic BP (mmHg) | 76 (64, 84) | 78 (70, 88) | 79 (74, 87) | 0.228 |
| Hypertension criteria | ||||
| Optimal HT <120 and/or <80 mmHg | 24 (48.0) | 6 (21.4) | 7 (15.6) | 0.002 * |
| Normal 120–129 and/or 80–84 mmHg | 7 (14.0) | 5 (17.9) | 16 (35.5) | |
| High normal 130–139 and/or 85–89 mmHg | 13 (26.0) | 8 (28.6) | 7 (15.6) | |
| Possible hypertension >140/90 mmHg | 6 (12.0) | 9 (32.1) | 15 (33.3) | |
| Number of medication use | ||||
| No | 28 (56.0) | 9 (32.1) | 13 (28.9) | 0.001 * |
| 1 group | 13 (26.0) | 12 (42.9) | 8 (17.8) | |
| ≥2 groups | 9 (18.0) | 7 (25.0) | 24 (53.3) | |
| Medication for diabetes mellitus | ||||
| No | 42 (84.0) | 26 (92.9) | 37 (82.2) | 0.430 |
| Yes | 8 (16.0) | 2 (7.1) | 8 (17.8) | |
| Medication for dyslipidemia | ||||
| No | 31 (62.0) | 16 (57.1) | 18 (40.0) | 0.088 |
| Yes | 19 (38.0) | 12 (42.9) | 27 (60.0) | |
| Medication for hypertension | ||||
| No | 41 (82.0) | 14 (50.0) | 20 (44.4) | <0.001 * |
| Yes | 9 (18.0) | 14 (50.0) | 25 (55.6) | |
| Participants (N = 123) | p-Value | |||
|---|---|---|---|---|
| Normal Weight (n = 50) | Overweight (n = 28) | Obesity (n = 45) | ||
| Number of tooth diseases | 9 (5, 13) | 10 (7, 15) | 11 (5, 16) | 0.366 |
| Number of missing teeth | 3 (1, 5) | 3 (0, 5) | 5 (2, 9) | 0.025 * |
| Periodontal status | ||||
| Gingivitis | 39 (78.0) | 17 (60.7) | 29 (64.4) | 0.198 |
| Periodontitis | 11 (22.0) | 11 (39.3) | 16 (35.6) | |
| Denture wear | ||||
| Upper | 11 (22.0) | 7 (25.0) | 11 (24.4) | 0.421 |
| Lower | 7 (14.0) | 5 (17.9) | 8 (17.8) | 0.171 |
| Total XI-11 score | 17 (12, 21) | 17 (14, 20) | 17 (15, 22) | 0.927 |
| Total CODS | 0 (0, 2) | 0 (0, 2) | 2 (0, 3) | 0.014 * |
| OHIP-14 | Participants (N = 123) | p-Value | ||
|---|---|---|---|---|
| Normal Weight (n = 50) | Overweight (n = 28) | Obesity (n = 45) | ||
| Score 0–3 | 42 (84.0) | 23 (82.1) | 25 (55.6) | 0.004 * |
| Score 4 | 8 (16.0) | 5 (17.9) | 20 (44.4) | |
| OHIP-14: Scoring 4 | ||||||||
|---|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | Model 4 | |||||
| OR (95%CI) | p | OR (95%CI) | p | OR (95%CI) | p | OR (95%CI) | p | |
| Age (years) | 1.03 (0.95, 1.12) | 0.492 | 1.02 (0.94, 1.11) | 0.631 | 0.98 (0.88, 1.09) | 0.672 | 0.96 (0.86, 1.08) | 0.541 |
| Sex (female) | 1.38 (0.62, 3.07) | 0.434 | 1.49 (0.64, 3.48) | 0.352 | 1.64 (0.69, 3.94) | 0.266 | 1.29 (0.51, 3.22) | 0.593 |
| BMI | ||||||||
| Overweight | 1.13 (0.33, 3.88) | 0.846 | 1.24 (0.35, 4.34) | 0.737 | 1.41 (0.39, 5.08) | 0.603 | ||
| Obesity | 4.25 (1.62, 11.15) | 0.003 | 4.06 (1.51, 10.90) | 0.005 | 4.42 (1.57, 12.47) | 0.005 * | ||
| Number of missing teeth | 1.05 (0.95, 1.15) | 0.326 | 1.03 (0.93, 1.15) | 0.570 | ||||
| Number of teeth with pulpal diseases | 1.26 (0.89, 1.79) | 0.194 | 1.24 (0.79, 1.95) | 0.353 | ||||
| Total XI score | 1.11 (1.02, 1.20) | 0.013 * | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khongsirisombat, N.; Kiattavorncharoen, S.; Thanakun, S. Increased Oral Dryness and Negative Oral Health-Related Quality of Life in Older People with Overweight or Obesity. Dent. J. 2022, 10, 231. https://doi.org/10.3390/dj10120231
Khongsirisombat N, Kiattavorncharoen S, Thanakun S. Increased Oral Dryness and Negative Oral Health-Related Quality of Life in Older People with Overweight or Obesity. Dentistry Journal. 2022; 10(12):231. https://doi.org/10.3390/dj10120231
Chicago/Turabian StyleKhongsirisombat, Nattapat, Sirichai Kiattavorncharoen, and Supanee Thanakun. 2022. "Increased Oral Dryness and Negative Oral Health-Related Quality of Life in Older People with Overweight or Obesity" Dentistry Journal 10, no. 12: 231. https://doi.org/10.3390/dj10120231