Multimodal In Vivo Imaging of Retinal and Choroidal Vascular Occlusion

 , ,
, , 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
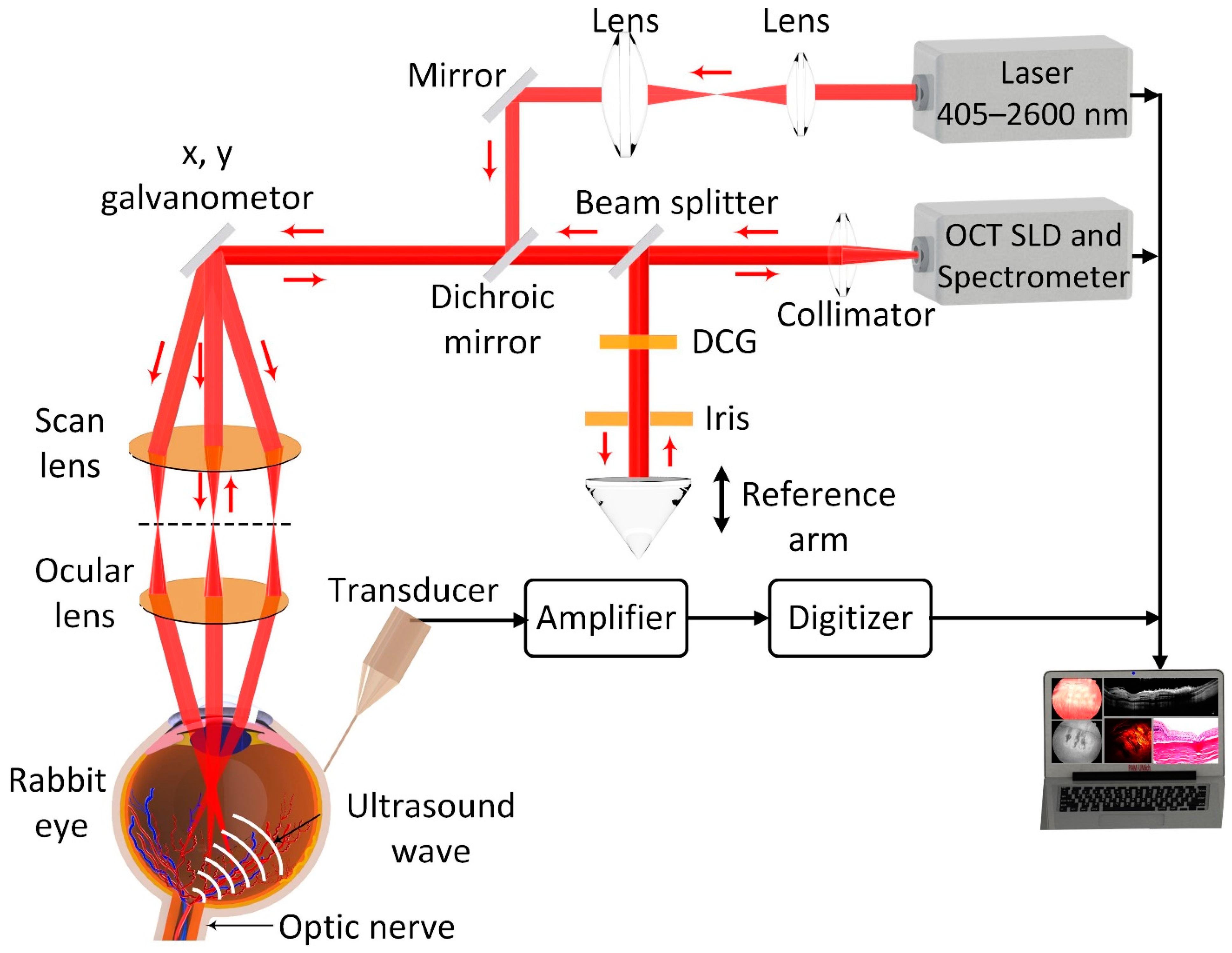
2.1. Multimodal PAM and OCT Imaging
2.2. Animal Preparation
2.2.1. Retinal Vein Occlusion (RVO) Model
2.2.2. Choroidal Vascular Occlusion (CVO) Model
2.3. Imaging of RVO and CVO
2.3.1. Color Fundus Photography, FA, ICGA
2.3.2. In Vivo PAM and OCT of RVO and CVO
2.4. Histological Analysis
3. Results
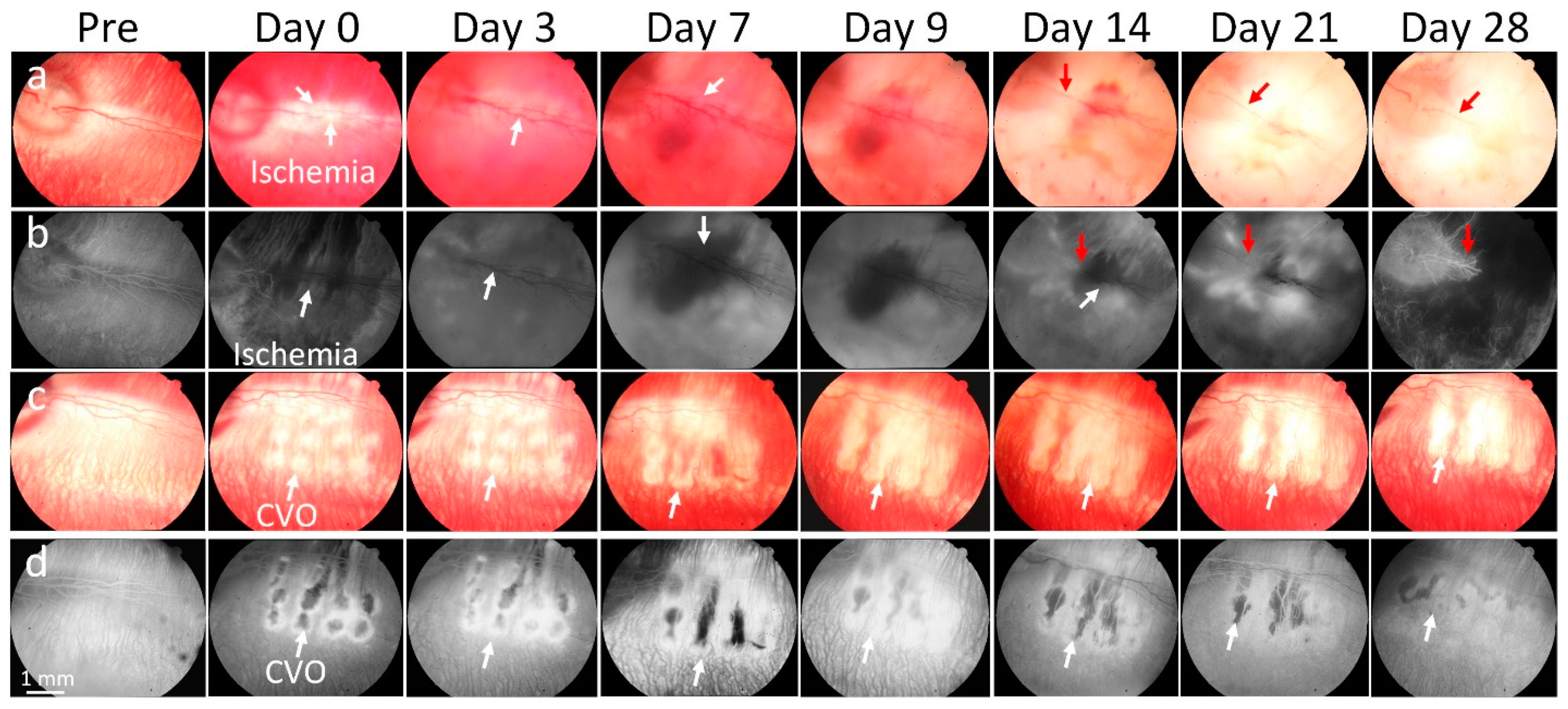
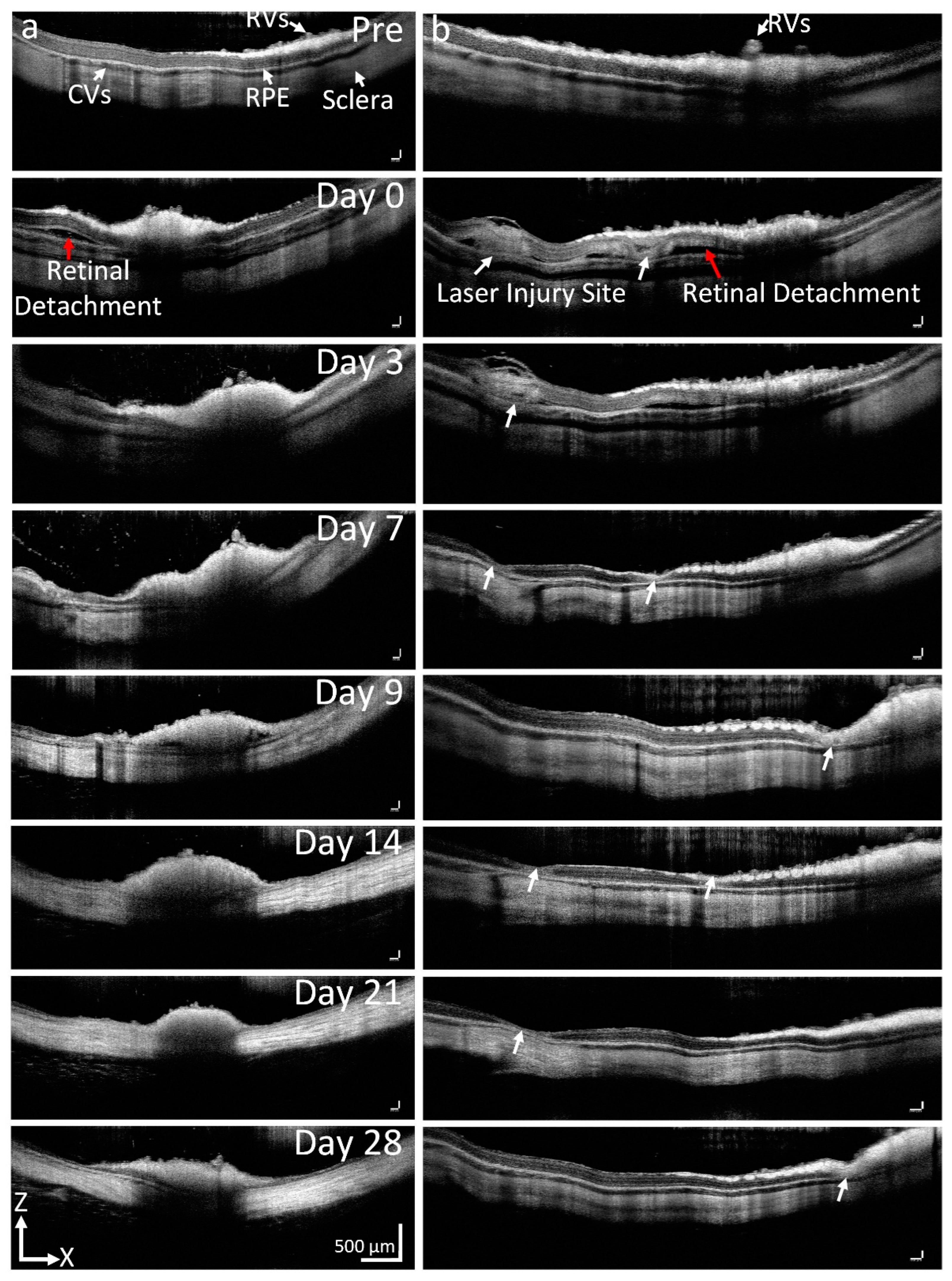
3.1. Retinal Vein Occlusion and Choroidal Vascular Occlusion Cause Severe Retinal Vessel Changes and Increase Vascular Tortuosity
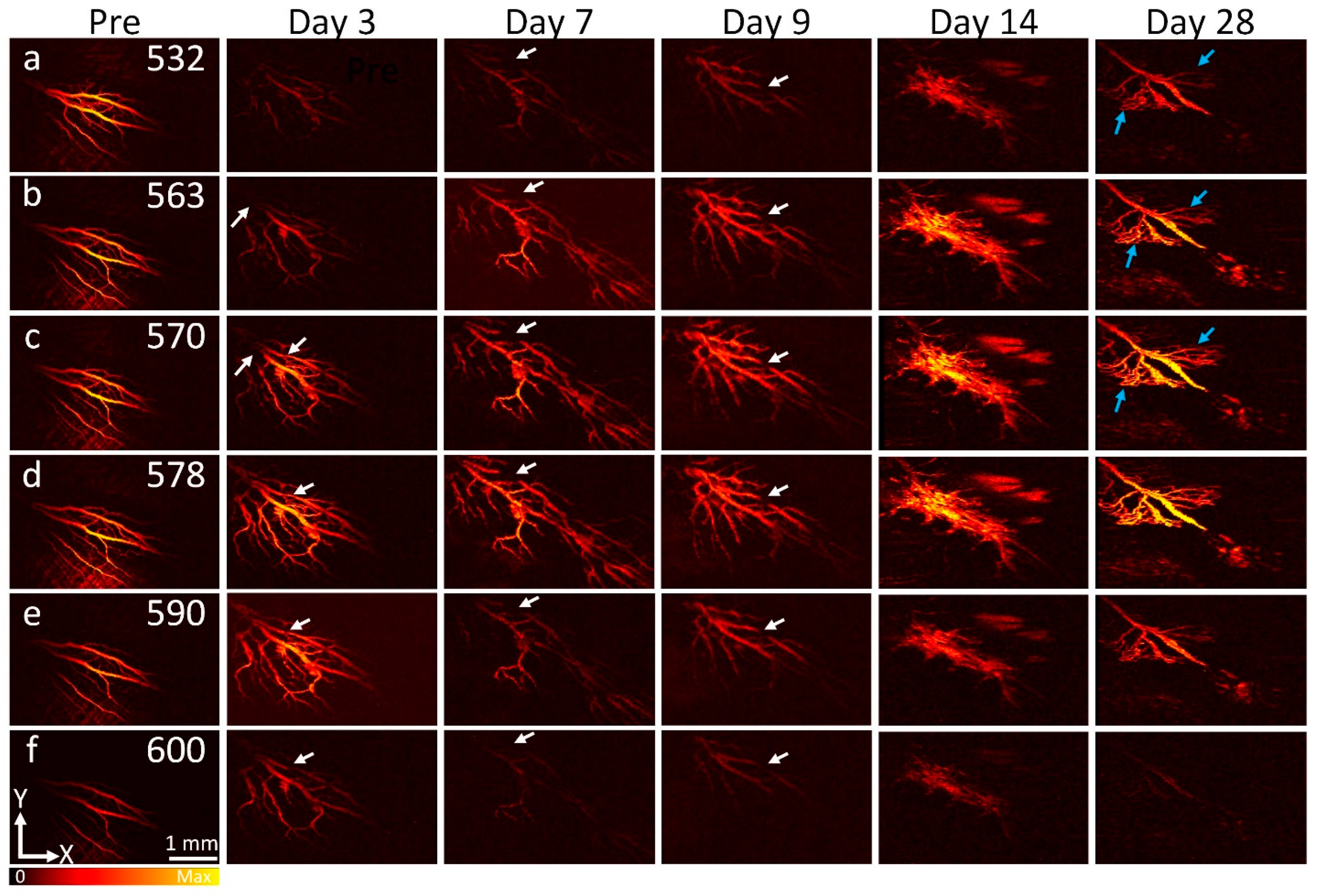
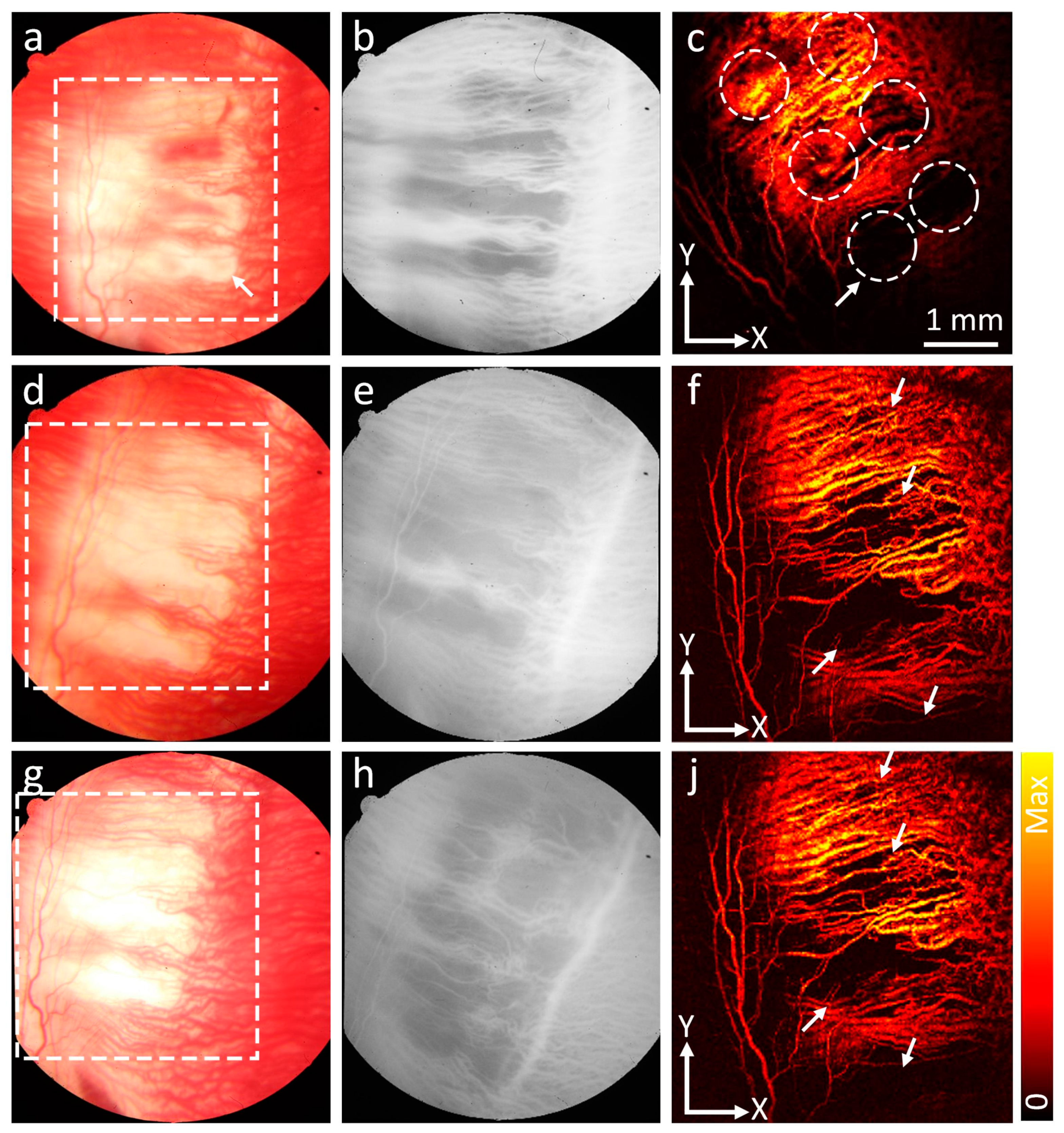
3.2. In Vivo PAM Visualization of Ischemia in RVO and CVO
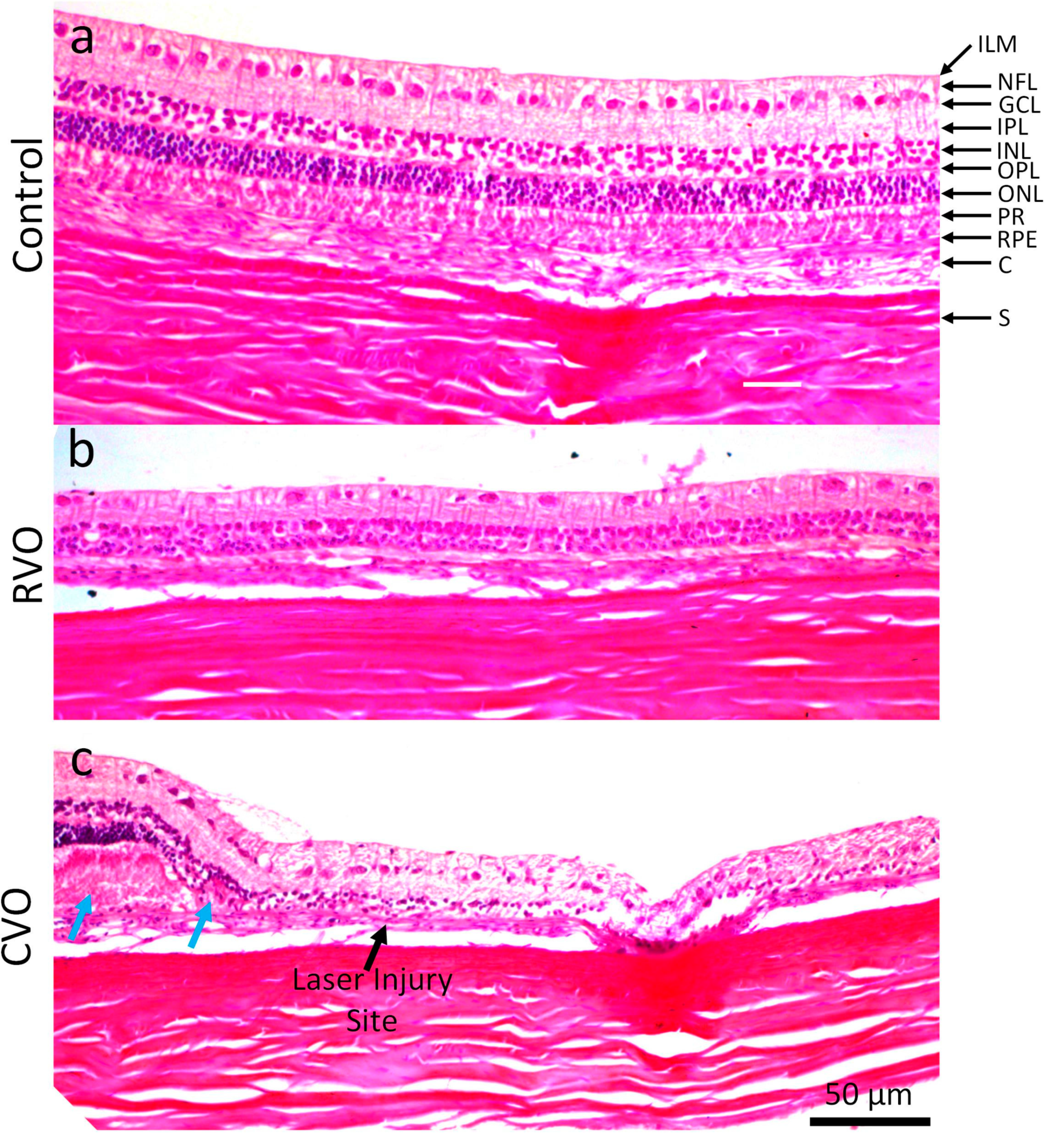
3.3. Histological Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wong, T.Y.; Scott, I.U. Retinal-vein occlusion. N. Engl. J. Med. 2010, 363, 2135–2144. [Google Scholar] [CrossRef] [PubMed]
- Hayreh, S.S. Ocular vascular occlusive disorders: Natural history of visual outcome. Prog. Retin. Eye Res. 2014, 41, 1–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rogers, S.; McIntosh, R.L.; Cheung, N.; Lim, L.; Wang, J.J.; Mitchell, P.; Kowalski, J.W.; Nguyen, H.; Wong, T.Y.; Consortium, I.E.D. The prevalence of retinal vein occlusion: Pooled data from population studies from the United States, Europe, Asia, and Australia. Ophthalmology 2010, 117, 313–319.e311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klein, R.; Klein, B.E.; Moss, S.E.; Meuer, S.M. The epidemiology of retinal vein occlusion: The Beaver Dam Eye Study. Trans. Am. Ophthalmol. Soc. 2000, 98, 133. [Google Scholar]
- Li, J.; Paulus, Y.M.; Shuai, Y.; Fang, W.; Liu, Q.; Yuan, S. New developments in the classification, pathogenesis, risk factors, natural history, and treatment of branch retinal vein occlusion. J. Ophthalmol. 2017, 2017, 4936924. [Google Scholar] [CrossRef] [Green Version]
- Tsuiki, E.; Suzuma, K.; Ueki, R.; Maekawa, Y.; Kitaoka, T. Enhanced depth imaging optical coherence tomography of the choroid in central retinal vein occlusion. Am. J. Ophthalmol. 2013, 156, 543–547.e541. [Google Scholar] [CrossRef] [Green Version]
- Hayreh, S.S. Posterior ciliary artery occlusion and choroidal ischemia. In Ocular Vascular Occlusive Disorders; Springer: Berlin, Germany, 2015; pp. 379–427. [Google Scholar]
- Campochiaro, P.A. Molecular pathogenesis of retinal and choroidal vascular diseases. Prog. Retin. Eye Res. 2015, 49, 67–81. [Google Scholar] [CrossRef] [Green Version]
- Noma, H.; Funatsu, H.; Mimura, T.; Harino, S.; Hori, S. Vitreous levels of interleukin-6 and vascular endothelial growth factor in macular edema with central retinal vein occlusion. Ophthalmology 2009, 116, 87–93. [Google Scholar] [CrossRef]
- Pe’er, J.; Folberg, R.; Itin, A.; Gnessin, H.; Hemo, I.; Keshet, E. Vascular endothelial growth factor upregulation in human central retinal vein occlusion. Ophthalmology 1998, 105, 412–416. [Google Scholar] [CrossRef]
- Aiello, L.P.; Avery, R.L.; Arrigg, P.G.; Keyt, B.A.; Jampel, H.D.; Shah, S.T.; Pasquale, L.R.; Thieme, H.; Iwamoto, M.A.; Park, J.E. Vascular endothelial growth factor in ocular fluid of patients with diabetic retinopathy and other retinal disorders. N. Engl. J. Med. 1994, 331, 1480–1487. [Google Scholar] [CrossRef]
- Standardization of Uveitis Nomenclature (SUN) Working Group. Standardization of uveitis nomenclature for reporting clinical data. Results of the First International Workshop. Am. J. Ophthalmol. 2005, 140, 509–516. [Google Scholar] [CrossRef]
- Fineschi, V.; Monasterolo, G.; Rosi, R.; Turillazzi, E. Fatal anaphylactic shock during a fluorescein angiography. Forensic Sci. Int. 1999, 100, 137–142. [Google Scholar] [CrossRef]
- Hitosugi, M.; Omura, K.; Yokoyama, T.; Kawato, H.; Motozawa, Y.; Nagai, T.; Tokudome, S. 2. An autopsy case of fatal anaphylactic shock following fluorescein angiography. Med. Sci. Law 2004, 44, 264–265. [Google Scholar] [CrossRef] [PubMed]
- Landsman, M.; Kwant, G.; Mook, G.; Zijlstra, W. Light-absorbing properties, stability, and spectral stabilization of indocyanine green. J. Appl. Physiol. 1976, 40, 575–583. [Google Scholar] [CrossRef] [PubMed]
- Anijeet, D.R.; Zheng, Y.; Tey, A.; Hodson, M.; Sueke, H.; Kaye, S.B. Imaging and evaluation of corneal vascularization using fluorescein and indocyanine green angiography. Investig. Ophthalmol. Vis. Sci. 2012, 53, 650–658. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, V.-P.; Li, Y.; Henry, J.; Zhang, W.; Wang, X.; Paulus, Y.M. Gold Nanorod Enhanced Photoacoustic Microscopy and Optical Coherence Tomography of Choroidal Neovascularization. ACS Appl. Mater. Interfaces 2021, 13, 40214–40228. [Google Scholar] [CrossRef]
- Nguyen, V.P.; Fan, W.; Zhu, T.; Qian, W.; Li, Y.; Liu, B.; Zhang, W.; Henry, J.; Yuan, S.; Wang, X. Long-Term, Noninvasive In Vivo Tracking of Progenitor Cells Using Multimodality Photoacoustic, Optical Coherence Tomography, and Fluorescence Imaging. ACS Nano 2021, 15, 13289–13306. [Google Scholar] [CrossRef]
- Nguyen, V.P.; Qian, W.; Li, Y.; Liu, B.; Aaberg, M.; Henry, J.; Zhang, W.; Wang, X.; Paulus, Y.M. Chain-like gold nanoparticle clusters for multimodal photoacoustic microscopy and optical coherence tomography enhanced molecular imaging. Nat. Commun. 2021, 12, 34. [Google Scholar] [CrossRef]
- Yeung, L.; Lima, V.C.; Garcia, P.; Landa, G.; Rosen, R.B. Correlation between spectral domain optical coherence tomography findings and fluorescein angiography patterns in diabetic macular edema. Ophthalmology 2009, 116, 1158–1167. [Google Scholar] [CrossRef]
- Vaz-Pereira, S.; Zarranz-Ventura, J.; Sim, D.A.; Keane, P.A.; Smith, R.; Egan, C.A.; Tufail, A. Optical coherence tomography features of active and inactive retinal neovascularization in proliferative diabetic retinopathy. Retina 2016, 36, 1132–1142. [Google Scholar] [CrossRef]
- Cho, H.; Alwassia, A.A.; Regiatieri, C.V.; Zhang, J.Y.; Baumal, C.; Waheed, N.; Duker, J.S. Retinal neovascularization secondary to proliferative diabetic retinopathy characterized by spectral domain optical coherence tomography. Retina 2013, 33, 542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, V.P.; Li, Y.; Zhang, W.; Wang, X.; Paulus, Y.M. High-resolution multimodal photoacoustic microscopy and optical coherence tomography image-guided laser induced branch retinal vein occlusion in living rabbits. Sci. Rep. 2019, 9, 10560. [Google Scholar] [CrossRef] [Green Version]
- Ishibazawa, A.; Nagaoka, T.; Yokota, H.; Takahashi, A.; Omae, T.; Song, Y.-S.; Takahashi, T.; Yoshida, A. Characteristics of retinal neovascularization in proliferative diabetic retinopathy imaged by optical coherence tomography angiography. Investig. Ophthalmol. Vis. Sci. 2016, 57, 6247–6255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuehlewein, L.; Bansal, M.; Lenis, T.L.; Iafe, N.A.; Sadda, S.R.; Bonini Filho, M.A.; Talisa, E.; Waheed, N.K.; Duker, J.S.; Sarraf, D. Optical coherence tomography angiography of type 1 neovascularization in age-related macular degeneration. Am. J. Ophthalmol. 2015, 160, 739–748.e732. [Google Scholar] [CrossRef] [PubMed]
- Salas, M.; Augustin, M.; Ginner, L.; Kumar, A.; Baumann, B.; Leitgeb, R.; Drexler, W.; Prager, S.; Hafner, J.; Schmidt-Erfurth, U. Visualization of micro-capillaries using optical coherence tomography angiography with and without adaptive optics. Biomed. Opt. Express 2017, 8, 207–222. [Google Scholar] [CrossRef] [Green Version]
- de La Zerda, A.; Paulus, Y.M.; Teed, R.; Bodapati, S.; Dollberg, Y.; Khuri-Yakub, B.T.; Blumenkranz, M.S.; Moshfeghi, D.M.; Gambhir, S.S. Photoacoustic ocular imaging. Opt. Lett. 2010, 35, 270–272. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, V.P.; Paulus, Y.M. Photoacoustic ophthalmoscopy: Principle, application, and future directions. J. Imaging 2018, 4, 149. [Google Scholar] [CrossRef] [Green Version]
- Hennen, S.N.; Xing, W.; Shui, Y.-B.; Zhou, Y.; Kalishman, J.; Andrews-Kaminsky, L.B.; Kass, M.A.; Beebe, D.C.; Maslov, K.I.; Wang, L.V. Photoacoustic tomography imaging and estimation of oxygen saturation of hemoglobin in ocular tissue of rabbits. Exp. Eye Res. 2015, 138, 153–158. [Google Scholar] [CrossRef] [Green Version]
- Tian, C.; Zhang, W.; Mordovanakis, A.; Wang, X.; Paulus, Y.M. Noninvasive chorioretinal imaging in living rabbits using integrated photoacoustic microscopy and optical coherence tomography. Opt. Express 2017, 25, 15947–15955. [Google Scholar] [CrossRef]
- Tian, C.; Zhang, W.; Nguyen, V.P.; Wang, X.; Paulus, Y.M. Novel photoacoustic microscopy and optical coherence tomography dual-modality chorioretinal imaging in living rabbit eyes. JoVE (J. Vis. Exp.) 2018, 132, e57135. [Google Scholar] [CrossRef]
- Nguyen, V.P.; Li, Y.; Qian, W.; Liu, B.; Tian, C.; Zhang, W.; Huang, Z.; Ponduri, A.; Tarnowski, M.; Wang, X. Contrast agent enhanced multimodal photoacoustic microscopy and optical coherence tomography for imaging of rabbit choroidal and retinal vessels in vivo. Sci. Rep. 2019, 9, 5945. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, V.-P.; Li, Y.; Henry, J.; Zhang, W.; Aaberg, M.; Jones, S.; Qian, T.; Wang, X.; Paulus, Y.M. Plasmonic gold nanostar-enhanced multimodal photoacoustic microscopy and optical coherence tomography molecular imaging to evaluate choroidal neovascularization. ACS Sens. 2020, 5, 3070–3081. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, V.P.; Li, Y.; Zhang, W.; Henry, J.; Aaberg, M.; Wang, X.; Paulus, Y.M. Gold nanostar-enhanced multimodal photoacoustic microscopy and optical coherence tomography for the visualization of laser-induced choroidal neovascularization in living rabbits. In Proceedings of the Plasmonics in Biology and Medicine XVII, San Francisco, CA, USA, 3–5 February 2019; International Society for Optics and Photonics: Bellingham, WA, USA, 2020; p. 112570G. [Google Scholar]
- ANSI Z136.1. 2007. Available online: https://www.lia.org/store/product/ansi-z1361-2014-safe-use-lasers-electronic-version (accessed on 11 December 2018).
- Kuo, T.-R.; Hovhannisyan, V.A.; Chao, Y.-C.; Chao, S.-L.; Chiang, S.-J.; Lin, S.-J.; Dong, C.-Y.; Chen, C.-C. Multiple release kinetics of targeted drug from gold nanorod embedded polyelectrolyte conjugates induced by near-infrared laser irradiation. J. Am. Chem. Soc. 2010, 132, 14163–14171. [Google Scholar] [CrossRef] [PubMed]
- Organisciak, D.T.; Vaughan, D.K. Retinal light damage: Mechanisms and protection. Prog. Retin. Eye Res. 2010, 29, 113–134. [Google Scholar] [CrossRef] [Green Version]
- Oncel, M.; Peyman, G.A.; Khoobehi, B. Tissue plasminogen activator in the treatment of experimental retinal vein occlusion. Retina (Philadelphia, Pa) 1989, 9, 1–7. [Google Scholar] [CrossRef]
- Nguyen, V.P.; Li, Y.; Zhang, W.; Wang, X.; Paulus, Y.M. Multi-wavelength, en-face photoacoustic microscopy and optical coherence tomography imaging for early and selective detection of laser induced retinal vein occlusion. Biomed. Opt. Expess 2018, 9, 5915–5938. [Google Scholar] [CrossRef]
- Ho, J.K.; Stanford, M.P.; Shariati, M.A.; Dalal, R.; Liao, Y.J. Optical Coherence Tomography Study of Experimental Anterior Ischemic Optic Neuropathy and Histologic Confirmation. Investig. Ophthalmol. Vis. Sci. 2013, 54, 5981–5988. [Google Scholar] [CrossRef]
- Ameri, H.; Ratanapakorn, T.; Rao, N.A.; Chader, G.J.; Humayun, M.S. Natural course of experimental retinal vein occlusion in rabbit; arterial occlusion following venous photothrombosis. Graefe’s Arch. Clin. Exp. Ophthalmol. 2008, 246, 1429. [Google Scholar] [CrossRef]
- Dominguez, E.; Raoul, W.; Calippe, B.; Sahel, J.-A.; Guillonneau, X.; Paques, M.; Sennlaub, F. Experimental Branch Retinal Vein Occlusion Induces Upstream Pericyte Loss and Vascular Destabilization. PLoS ONE 2015, 10, e0132644. [Google Scholar] [CrossRef] [Green Version]
- Prahl, S.A. A Compendium of Tissue Optical Properties. 2012. Available online: http://omlc.org/spectra/hemoglobin/ (accessed on 11 May 2011).
- Rehak, M.; Hollborn, M.; Iandiev, I.; Pannicke, T.; Karl, A.; Wurm, A.; Kohen, L.; Reichenbach, A.; Wiedemann, P.; Bringmann, A. Retinal Gene Expression and Muller Cell Responses after Branch Retinal Vein Occlusion in the Rat. Investig. Ophthalmol. Vis. Sci. 2009, 50, 2359–2367. [Google Scholar] [CrossRef]
- McAllister, I.L.; Vijayasekaran, S.; Chen, S.D.; Yu, D.-Y. Effect of Triamcinolone Acetonide on Vascular Endothelial Growth Factor and Occludin Levels in Branch Retinal Vein Occlusion. Am. J. Ophthalmol. 2009, 147, 838–846.e832. [Google Scholar] [CrossRef] [PubMed]
- Uddin, M.I.; Jayagopal, A.; McCollum, G.W.; Yang, R.; Penn, J.S. In Vivo Imaging of Retinal Hypoxia Using HYPOX-4-Dependent Fluorescence in a Mouse Model of Laser-Induced Retinal Vein Occlusion (RVO). Investig. Ophthalmol. Vis. Sci. 2017, 58, 3818–3824. [Google Scholar] [CrossRef] [PubMed]







Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nguyen, V.P.; Zhu, T.; Henry, J.; Zhang, W.; Wang, X.; Paulus, Y.M. Multimodal In Vivo Imaging of Retinal and Choroidal Vascular Occlusion. Photonics 2022, 9, 201. https://doi.org/10.3390/photonics9030201
Nguyen VP, Zhu T, Henry J, Zhang W, Wang X, Paulus YM. Multimodal In Vivo Imaging of Retinal and Choroidal Vascular Occlusion. Photonics. 2022; 9(3):201. https://doi.org/10.3390/photonics9030201
Chicago/Turabian StyleNguyen, Van Phuc, Tianye Zhu, Jessica Henry, Wei Zhang, Xueding Wang, and Yannis M. Paulus. 2022. "Multimodal In Vivo Imaging of Retinal and Choroidal Vascular Occlusion" Photonics 9, no. 3: 201. https://doi.org/10.3390/photonics9030201