Numerical Analysis of the Effect of Decentered Refractive Segmented Extended Depth of Focus (EDoF) Intraocular Lenses on Predicted Visual Outcomes

 and
and
Abstract
:1. Introduction
2. Materials and Methods
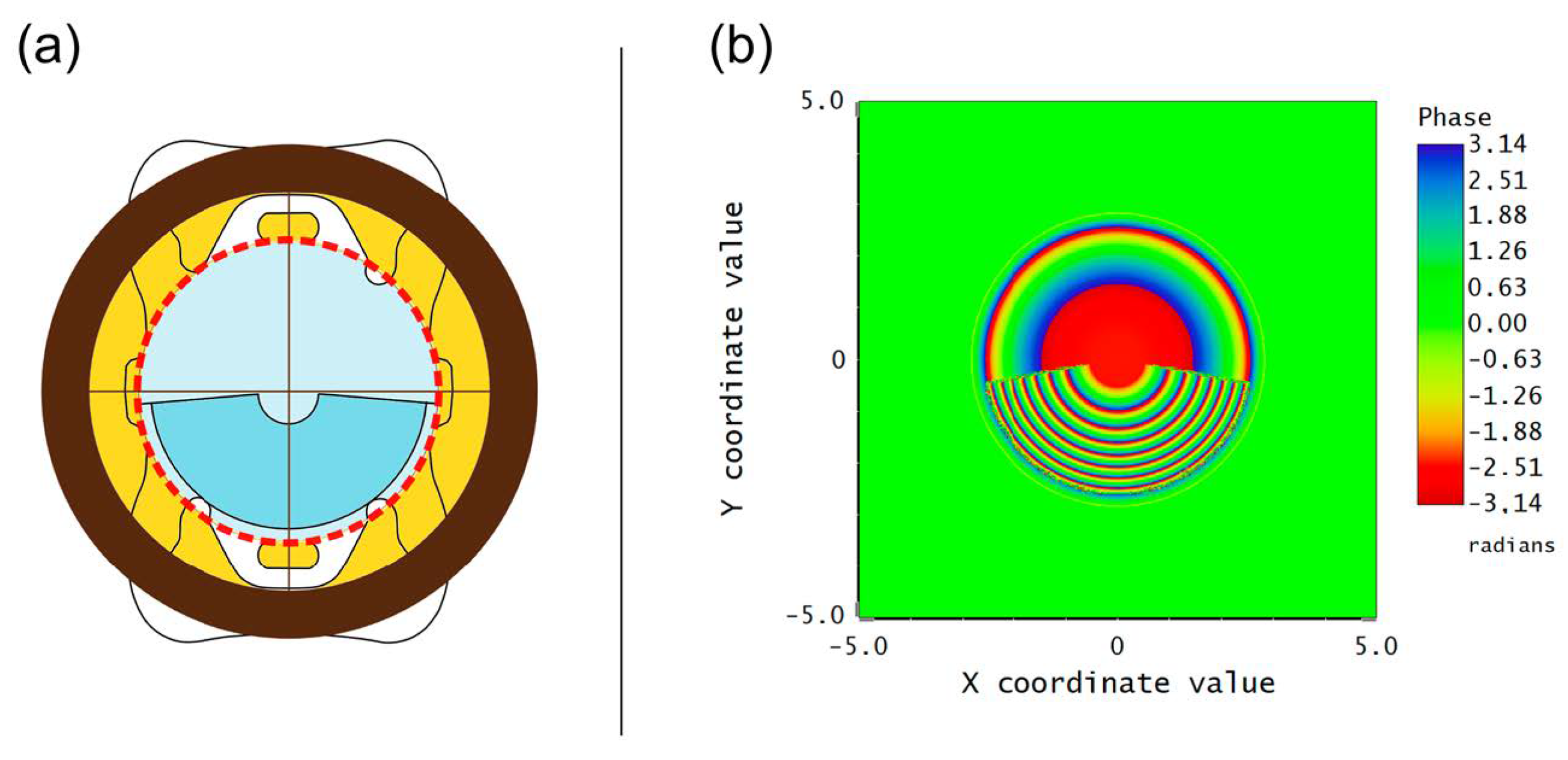
2.1. Multifocal Intraocular Lens
2.2. Numerical Evaluation
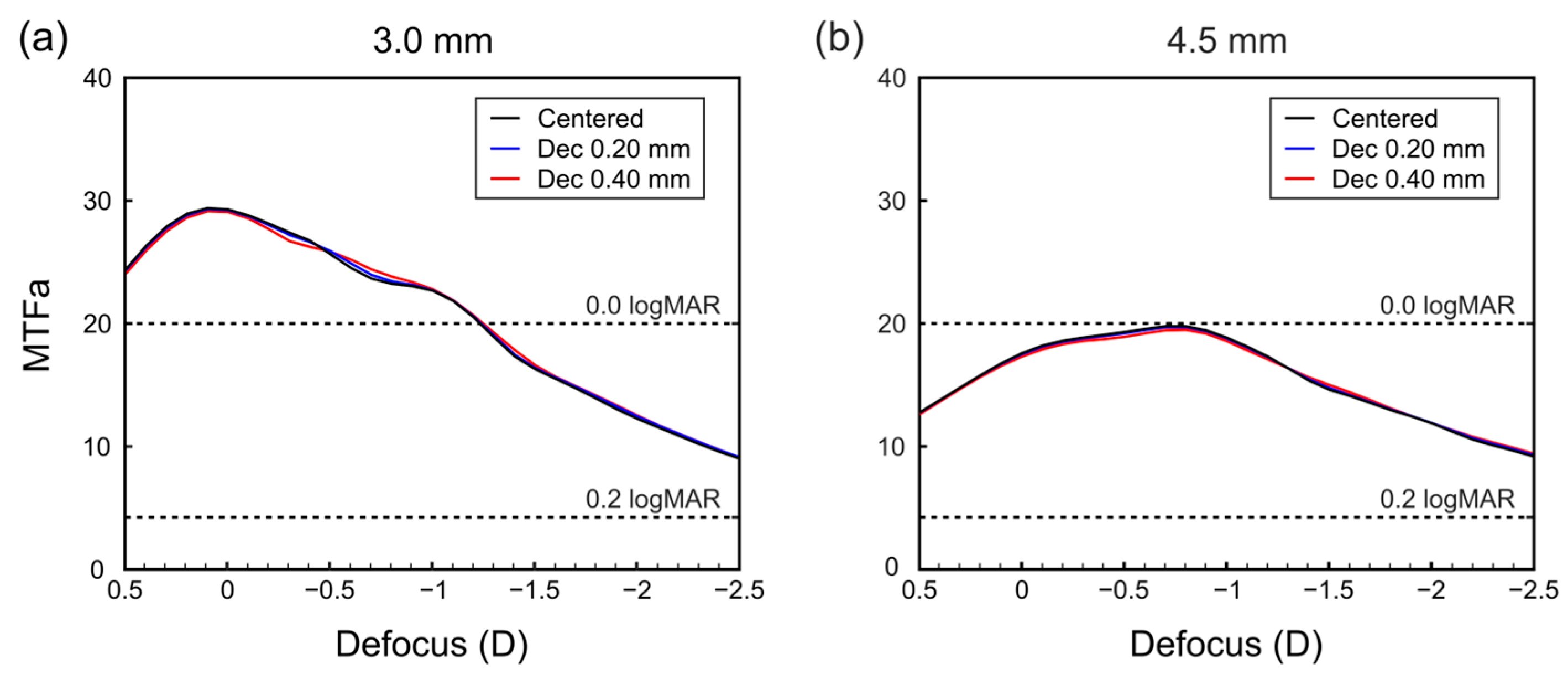
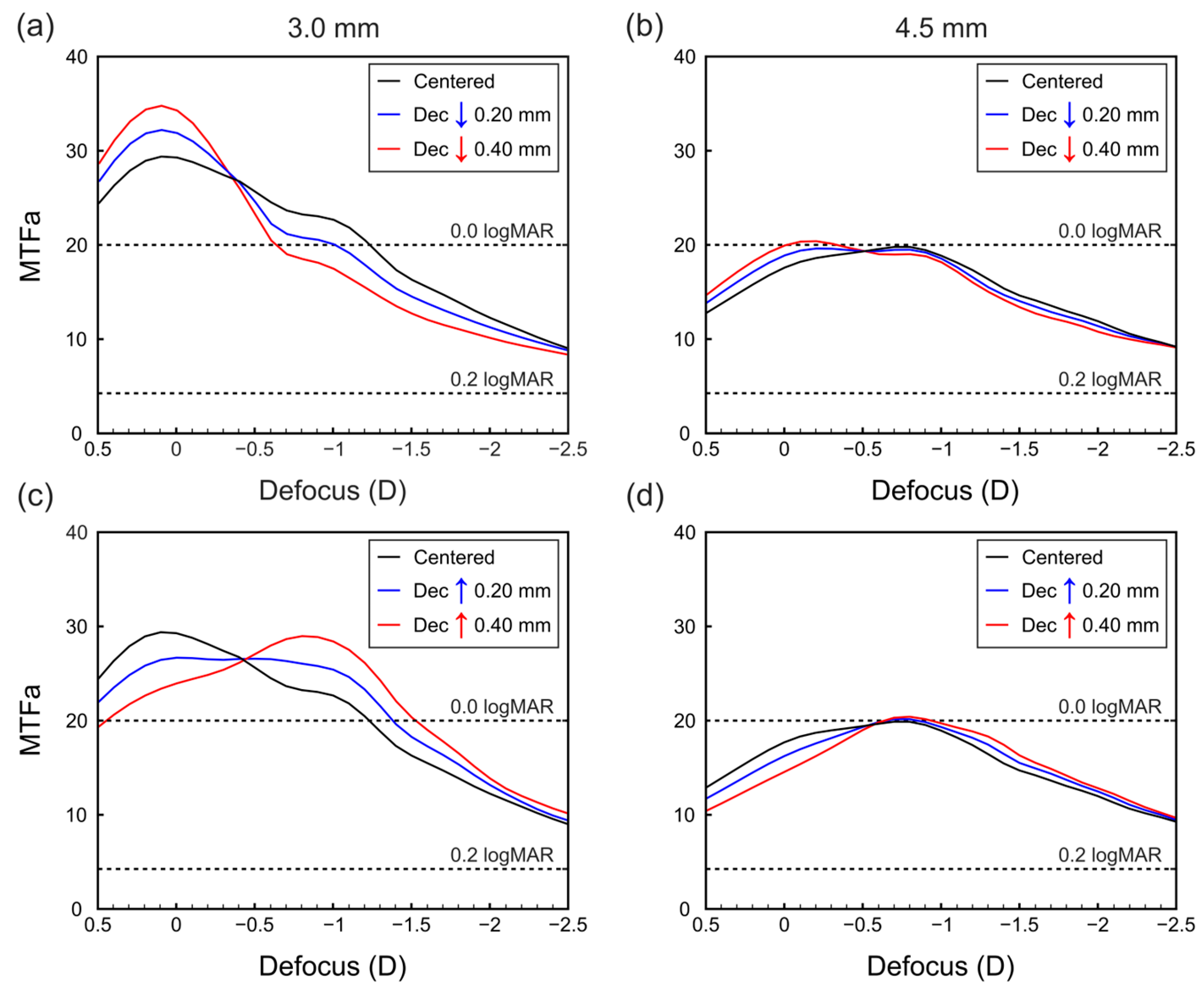
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Charman, W.N. Developments in the Correction of Presbyopia II: Surgical Approaches. Ophthalmic Physiol. Opt. 2014, 34, 397–426. [Google Scholar] [CrossRef] [PubMed]
- Gatinel, D.; Houbrechts, Y. Comparison of Bifocal and Trifocal Diffractive and Refractive Intraocular Lenses Using an Optical Bench. J. Cataract Refract. Surg. 2013, 39, 1093–1099. [Google Scholar] [CrossRef] [PubMed]
- Durrie, D.S.; Moshifar, M. Dysfunctional lens syndrome. In Proceedings of the Annual Meeting of ISRS. Pursuit of Perfection. Section II: Intraocular Refractive Surgery Topics, Chicago, IL, USA; 2016. [Google Scholar]
- Durrie, D.S. Dysfunctional Lens Syndrome, a New Way to Educate Patients—American Academy of Ophthalmology. Available online: https://www.aao.org/eyenet/academy-live/detail/dysfunctional-lens-syndrome-educate-patients (accessed on 9 March 2023).
- Rampat, R.; Gatinel, D. Multifocal and Extended Depth-of-Focus Intraocular Lenses in 2020. Ophthalmology 2021, 128, e164–e185. [Google Scholar] [CrossRef]
- Liu, J.; Dong, Y.; Wang, Y. Efficacy and Safety of Extended Depth of Focus Intraocular Lenses in Cataract Surgery: A Systematic Review and Meta-Analysis. BMC Ophthalmol. 2019, 19, 198. [Google Scholar] [CrossRef] [Green Version]
- MacRae, S.; Holladay, J.T.; Glasser, A.; Calogero, D.; Hilmantel, G.; Masket, S.; Stark, W.; Tarver, M.E.; Nguyen, T.; Eydelman, M. Special Report: American Academy of Ophthalmology Task Force Consensus Statement for Extended Depth of Focus Intraocular Lenses. Ophthalmology 2017, 124, 139–141. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.-Y.; Wang, Y.-C.; Zhao, T.-Y.; Wang, Z.-Z.; Wang, W. Tilt and Decentration with Various Intraocular Lenses: A Narrative Review. World J. Clin. Cases 2022, 10, 3639–3646. [Google Scholar] [CrossRef]
- Pérez-Merino, P.; Marcos, S. Effect of Intraocular Lens Decentration on Image Quality Tested in a Custom Model Eye. J. Cataract Refract. Surg. 2018, 44, 889–896. [Google Scholar] [CrossRef] [PubMed]
- Gu, X.; Chen, X.; Yang, G.; Wang, W.; Xiao, W.; Jin, G.; Wang, L.; Dai, Y.; Ruan, X.; Liu, Z.; et al. Determinants of Intraocular Lens Tilt and Decentration after Cataract Surgery. Ann. Transl. Med. 2020, 8, 921. [Google Scholar] [CrossRef]
- Kimura, S.; Morizane, Y.; Shiode, Y.; Hirano, M.; Doi, S.; Toshima, S.; Fujiwara, A.; Shiraga, F. Assessment of Tilt and Decentration of Crystalline Lens and Intraocular Lens Relative to the Corneal Topographic Axis Using Anterior Segment Optical Coherence Tomography. PLoS ONE 2017, 12, e0184066. [Google Scholar] [CrossRef] [Green Version]
- Poyales, F.; Garzón, N.; Rozema, J.J.; Romero, C.; de Zárate, B.O. Stability of a Novel Intraocular Lens Design: Comparison of Two Trifocal Lenses. J. Refract. Surg. 2016, 32, 394–402. [Google Scholar] [CrossRef] [Green Version]
- Ashena, Z.; Maqsood, S.; Ahmed, S.N.; Nanavaty, M.A. Effect of Intraocular Lens Tilt and Decentration on Visual Acuity, Dysphotopsia and Wavefront Aberrations. Vision 2020, 4, 41. [Google Scholar] [CrossRef] [PubMed]
- Meng, J.; He, W.; Rong, X.; Miao, A.; Lu, Y.; Zhu, X. Decentration and Tilt of Plate-Haptic Multifocal Intraocular Lenses in Myopic Eyes. Eye Vis. 2020, 7, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, X.; Xie, L.; Huang, Y. Effects of Decentration and Tilt at Different Orientations on the Optical Performance of a Rotationally Asymmetric Multifocal Intraocular Lens. J. Cataract Refract. Surg. 2019, 45, 507–514. [Google Scholar] [CrossRef] [PubMed]
- Alió, J.L.; Plaza-Puche, A.B.; Javaloy, J.; Ayala, M.J.; Vega-Estrada, A. Clinical and Optical Intraocular Performance of Rotationally Asymmetric Multifocal IOL Plate-Haptic Design Versus C-Loop Haptic Design. J. Refract. Surg. 2013, 29, 252–259. [Google Scholar] [CrossRef]
- Darian-Smith, E.; Versace, P. Visual Performance and Positional Stability of a Capsulorhexis-Fixated Extended Depth-of-Focus Intraocular Lens. J. Cataract Refract. Surg. 2020, 46, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Shajari, M.; Sonntag, R.; Niermann, T.; Holland, D.; Kohnen, T.; Priglinger, S.; Mayer, W.J. Determining and Comparing the Effective Lens Position and Refractive Outcome of a Novel Rhexis-Fixated Lens to Established Lens Designs. Am. J. Ophthalmol. 2020, 213, 62–68. [Google Scholar] [CrossRef]
- Auffarth, G.U.; Friedmann, E.; Breyer, D.; Kaymak, H.; Holland, D.; Dick, B.; Petzold, A.; Shah, S.; Ladaria, L.S.; Garcia, S.A.; et al. Stability and Visual Outcomes of the Capsulotomy-Fixated FEMTIS-IOL After Automated Femtosecond Laser–Assisted Anterior Capsulotomy. Am. J. Ophthalmol. 2021, 225, 27–37. [Google Scholar] [CrossRef]
- García, S.; Salvá, L.; García-Delpech, S.; Martínez-Espert, A.; Ferrando, V.; Montagud-Martínez, D. Polychromatic Assessment of a Refractive Segmented EDOF Intraocular Lens. J. Clin. Med. 2022, 11, 1480. [Google Scholar] [CrossRef]
- Atchison, D.A. Optical Models for Human Myopic Eyes. Vis. Res. 2006, 46, 2236–2250. [Google Scholar] [CrossRef]
- Atchison, D.A.; Smith, G. Chromatic Dispersions of the Ocular Media of Human Eyes. J. Opt. Soc. Am. A 2005, 22, 29. [Google Scholar] [CrossRef]
- Remón, L.; Cabeza-gil, I. Influence of Material and Haptic Design on the Mechanical Stability of Intraocular Lenses by Means of Finite-Element Modeling. J. Biomed. Opt. 2018, 23, 1. [Google Scholar] [CrossRef] [PubMed]
- Guo, H.; Goncharov, A.; Dainty, C. Intraocular Lens Implantation Position Sensitivity as a Function of Refractive Error. Ophthalmic Physiol. Opt. 2012, 32, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Geniusz, M.; Kazimierska, M.; Zając, M. Impact of Glistenings on Optical Image Quality of Intraocular Lenses—A Preliminary Study. Photonics Lett. Pol. 2015, 7, 109–111. [Google Scholar] [CrossRef] [Green Version]
- Vega, F.; Millán, M.S.; Garzón, N.; Altemir, I.; Poyales, F.; Larrosa, J.M. Visual Acuity of Pseudophakic Patients Predicted from In-Vitro Measurements of Intraocular Lenses with Different Design. Biomed. Opt. Express 2018, 9, 4893. [Google Scholar] [CrossRef] [PubMed]
- Alarcon, A.; Canovas, C.; Rosen, R.; Weeber, H.; Tsai, L.; Hileman, K.; Piers, P. Preclinical Metrics to Predict Through-Focus Visual Acuity for Pseudophakic Patients. Biomed. Opt. Express 2016, 7, 1877. [Google Scholar] [CrossRef]
- Fernández, J.; Rodríguez-Vallejo, M.; Martínez, J.; Burguera, N.; Piñero, D.P. Prediction of Visual Acuity and Contrast Sensitivity From Optical Simulations with Multifocal Intraocular Lenses. J. Refract. Surg. 2019, 35, 789–795. [Google Scholar] [CrossRef]
- Atchison, D.A.; Thibos, L.N. Optical Models of the Human Eye. Clin. Exp. Optom. 2016, 99, 99–106. [Google Scholar] [CrossRef] [Green Version]
- Liou, H.-L.; Brennan, N.A. Anatomically Accurate, Finite Model Eye for Optical Modeling. J. Opt. Soc. Am. A 1997, 14, 1684. [Google Scholar] [CrossRef]
- Patel, S.; Marshall, J.; Fitzke, F.W. Model for Predicting the Optical Performance of the Eye in Refractive Surgery. Refract. Corneal Surg. 1993, 9, 366–375. [Google Scholar] [CrossRef]
- García, C.; Camps, V.J.; Caballero, M.T.; Piñero, D.P.; Tañá, P.; Tello, C.; Miret, J.J. Comparison of the Optical Quality Vision between Real Post-LASIK Myopic Laser Surgery and the Simulated Implantation of a Phakic IOL in Low Myopia. Sci. Rep. 2022, 12, 18942. [Google Scholar] [CrossRef]
- Radhakrishnan, A.; Dorronsoro, C.; Marcos, S. Differences in Visual Quality with Orientation of a Rotationally Asymmetric Bifocal Intraocular Lens Design. J. Cataract Refract. Surg. 2016, 42, 1276–1287. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Surface | Radius (mm) | Asphericity (Q) | Thickness (mm) | Refractive Index | Abbe Number |
|---|---|---|---|---|---|
| Cornea | 7.770 | −0.150 | 0.550 | 1.376 | 55.48 |
| Aqueous | 6.400 | −0.275 | 3.150 | 1.3374 | 50.37 |
| Pupil | - | - | - | 1.3374 | 50.37 |
| Anterior IOL | 21.400 | - | 0.700 | 1.460 | 58.00 |
| Posterior IOL | −8.700 | −1.275 | 18.900 | 1.336 | 51.30 |
| Retina X | −12.720 | 0.250 | - | - | - |
| Retina Y | −12.910 | 0.270 | - | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García, S.; Salvá, L.; García-Delpech, S.; Martínez-Espert, A.; Ferrando, V. Numerical Analysis of the Effect of Decentered Refractive Segmented Extended Depth of Focus (EDoF) Intraocular Lenses on Predicted Visual Outcomes. Photonics 2023, 10, 850. https://doi.org/10.3390/photonics10070850
García S, Salvá L, García-Delpech S, Martínez-Espert A, Ferrando V. Numerical Analysis of the Effect of Decentered Refractive Segmented Extended Depth of Focus (EDoF) Intraocular Lenses on Predicted Visual Outcomes. Photonics. 2023; 10(7):850. https://doi.org/10.3390/photonics10070850
Chicago/Turabian StyleGarcía, Scott, Luis Salvá, Salvador García-Delpech, Anabel Martínez-Espert, and Vicente Ferrando. 2023. "Numerical Analysis of the Effect of Decentered Refractive Segmented Extended Depth of Focus (EDoF) Intraocular Lenses on Predicted Visual Outcomes" Photonics 10, no. 7: 850. https://doi.org/10.3390/photonics10070850