Success Rate of Direct Pulp Capping with Conventional Procedures Using Ca (OH)2 and Bioactive Tricalcium Silicate Paste vs. Laser-Assisted Procedures (Diode 980 nm, CO2, and Er: YAG)

 ,
,  ,
,  ,
,  ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Different Pulp Capping Protocols
2.2.1. Calcium Hydroxide Ca (OH)2 Paste (n = 376)
2.2.2. Bioactive Tricalcium Silicate (n = 279)
2.2.3. Carbon Dioxide (CO2) Laser (n = 1147)
2.2.4. The 980 nm Diode Laser (n = 124)
2.2.5. Er: YAG Laser (Erbium-Doped Yttrium Aluminum Garnet Laser) (n = 69)
2.3. Inclusion and Exclusion Criteria
2.3.1. Inclusion Criteria
- Permanent teeth with deep caries;
- Vital teeth confirmed by vitality test;
- No spontaneous pain (only provoked pain);
- No periapical radiographic changes (Figure 1);
- No periodontal problems for the tooth in question;
- Acceptance of the research program and guidelines.
2.3.2. Exclusion Criteria
- Symptoms of dental discomfort related to the teeth in question;
- Periapical radiographic changes;
- Bleeding continued for more than 3 min after pulp exposure;
- Pulp exposure larger than 2 mm;
- Spontaneous and prolonged pain, and pain disturbing night sleep;
- Fractured teeth with exposed pulp due to trauma;
- Patients were taking corticosteroids;
- Lack of acceptance of the study’s guidelines;
- Pregnancy.
2.4. Follow-Up and Evaluation of the Success
2.5. Statistical Analysis
3. Results

Cumulative Results Related to Other Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kanodia, S.K.; Iyer, J.V.; Parmar, G.J.; Parmar, A.P.; Asthana, G.; Dhanak, N.R. Comparative Evaluation of Different Direct Pulp Capping Agents in Carious Tooth: An In Vivo Study. J. Conserv. Dent. 2021, 24, 283–287. [Google Scholar] [CrossRef] [PubMed]
- Arandi, N.Z.; Thabet, M. Minimal Intervention in Dentistry: A Literature Review on Biodentine as a Bioactive Pulp Capping Material. BioMed. Res. Int. 2021, 2021, 5569313. [Google Scholar] [CrossRef] [PubMed]
- Duncan, H.F. Present Status and Future Directions—Vital Pulp Treatment and Pulp Preservation Strategies. Int. Endod. J. 2022, 55, 497–511. [Google Scholar] [CrossRef] [PubMed]
- Stratigaki, E.; Tong, H.J.; Seremidi, K.; Kloukos, D.; Duggal, M.; Gizani, S. Contemporary Management of Deep Caries in Primary Teeth: A Systematic Review and Meta-Analysis. Eur. Arch. Paediatr. Dent. 2022, 4, 695–725. [Google Scholar] [CrossRef] [PubMed]
- Komabayashi, T.; Zhu, Q.; Eberhart, R.; Imai, Y. Current Status of Direct Pulp-Capping Materials for Permanent Teeth. Dent. Mater. J. 2016, 35, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Tuna, D.; Ölmez, A. Clinical Long-Term Evaluation of MTA as a Direct Pulp Capping Material in Primary Teeth. Int. Endod. J. 2008, 41, 273–278. [Google Scholar] [CrossRef]
- Peskersoy, C.; Lukarcanin, J.; Turkun, M. Efficacy of Different Calcium Silicate Materials as Pulp-Capping Agents: Randomized Clinical Trial. J. Dent. Sci. 2021, 16, 723–731. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Zheng, L.; Jiang, J.; Gui, J.; Zhang, L.; Huang, Y.; Chen, X.; Ji, J.; Fan, Y. Calcium Hydroxide–Induced Proliferation, Migration, Osteogenic Differentiation, and Mineralization via the Mitogen-Activated Protein Kinase Pathway in Human Dental Pulp Stem Cells. J. Endod. 2016, 42, 1355–1361. [Google Scholar] [CrossRef] [PubMed]
- Phung, S.; Lee, C.; Hong, C.; Song, M.; Yi, J.; Stevenson, R.; Kang, M.; Shin, K.-H.; Park, N.-H.; Kim, R. Effects of Bioactive Compounds on Odontogenic Differentiation and Mineralization. J. Dent. Res. 2017, 96, 107–115. [Google Scholar] [CrossRef]
- Kim, Y.; Lee, D.; Kim, H.-M.; Kye, M.; Kim, S.-Y. Biological Characteristics and Odontogenic Differentiation Effects of Calcium Silicate-Based Pulp Capping Materials. Materials 2021, 14, 4661. [Google Scholar] [CrossRef]
- Sarra, G.; Machado, M.E.d.L.; Caballero-Flores, H.V.; Moreira, M.S.; Pedroni, A.C.F.; Marques, M.M. Effect of Human Dental Pulp Stem Cell Conditioned Medium in the Dentin-Pulp Complex Regeneration: A Pilot In Vivo Study. Tissue Cell 2021, 72, 101536. [Google Scholar] [CrossRef]
- Krechina, E.K.; Volkov, A.V.; Abdurakhmanova, Z.U. Obosnovanie Primeneniya Bioaktivnykh Tsementov Dlya Sokhraneniya Zhiznesposobnosti Pul’py Pri Ee Sluchainom Vskrytii [Rationale for the use of Bioactive Cements by In Vitro Simulation of Accidental Pulp Opening]. Stomatologiia 2021, 100, 11–14. [Google Scholar] [CrossRef] [PubMed]
- Tziafas, D.; Kodonas, K. Differentiation Potential of Dental Papilla, Dental Pulp, and Apical Papilla Progenitor Cells. J. Endod. 2010, 36, 781–789. [Google Scholar] [CrossRef] [PubMed]
- Rathinam, E.; Govindarajan, S.; Rajasekharan, S.; Declercq, H.; Elewaut, D.; De Coster, P.; Martens, L. Transcriptomic Profiling of Human Dental Pulp Cells Treated with Bioactive Tricalcium Silicate Cements by RNA Sequencing. Clin. Oral Investig. 2021, 25, 3181–3195. [Google Scholar] [CrossRef] [PubMed]
- Baldión, P.A.; Velandia-Romero, M.L.; Castellanos, J.E. Odontoblast-Like Cells Differentiated from Dental Pulp Stem Cells Retain Their Phenotype after Subcultivation. Int. J. Cell Biol. 2018, 2018, 6853189. [Google Scholar] [CrossRef] [Green Version]
- Leong, D.J.X.; Yap, A.U. Vital Pulp Therapy in Carious Pulp–Exposed Permanent Teeth: An Umbrella Review. Clin. Oral Investig. 2021, 25, 6743–6756. [Google Scholar] [CrossRef]
- Ali, H.; Raslan, N. Direct Pulp Capping (DPC) in Primary Molars Using (3Mix-MP) and the Characteristics of the Carious Lesion as Predictor Factors for its Success: A Randomized Controlled Trial. Eur. Arch. Paediatr. Dent. 2021, 22, 633–642. [Google Scholar] [CrossRef]
- Lipski, M.; Nowicka, A.; Kot, K.; Postek-Stefańska, L.; Wysoczańska-Jankowicz, I.; Borkowski, L.; Andersz, P.; Jarząbek, A.; Grocholewicz, K.; Sobolewska, E.; et al. Factors Affecting the Outcomes of Direct Pulp Capping using Biodentine. Clin. Oral Investig. 2018, 22, 2021–2029. [Google Scholar] [CrossRef] [Green Version]
- Schwendicke, F.; Brouwer, F.; Schwendicke, A.; Paris, S. Different Materials for Direct Pulp Capping: Systematic Review and Meta-Analysis and Trial Sequential Analysis. Clin. Oral Investig. 2016, 20, 1121–1132. [Google Scholar] [CrossRef]
- Omrani, L.R.; Moradi, Z.; Abbasi, M.; Kharazifard, M.J.; Tabatabaei, S.N. Evaluation of Compressive Strength of Several Pulp Capping Materials. J. Dent. 2021, 22, 41–47. [Google Scholar] [CrossRef]
- Qureshi, A.; Soujanya, E.; Nandakumar, P. Recent Advances in Pulp Capping Materials: An Overview. J. Clin. Diagn. Res. JCDR 2014, 8, 316. [Google Scholar] [CrossRef]
- Zaen El-Din, A.M.; Hamama, H.H.; Abo El-Elaa, M.A.; Grawish, M.E.; Mahmoud, S.H.; Neelakantan, P. The Effect of Four Materials on Direct Pulp Capping: An Animal Study. Aust. Endod. J. 2020, 46, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, M.; Kato, C.; Kawashima, S.; Shinkai, K. Clinical and Histological Study on Direct Pulp Capping with CO2 Laser Irradiation in Human Teeth. Oper. Dent. 2019, 44, 336–347. [Google Scholar] [CrossRef] [PubMed]
- Nammour, S.; Tielemans, M.; Heysselaer, D.; Pilipili, C.; De Moor, R.; Behets, C. Comparative Study on Dogs between CO2 Laser and Conventional Technique in Direct Pulp Capping. Rev. Belg. Med. Dent. 2009, 64, 81–86. [Google Scholar]
- Rajesh, S.; Koshi, E.; Philip, K.; Mohan, A. Antimicrobial Photodynamic Therapy: An Overview. J. Indian Soc. Periodontol. 2011, 15, 323–327. [Google Scholar] [CrossRef]
- Giraud, T.; Jeanneau, C.; Rombouts, C.; Bakhtiar, H.; Laurent, P.; About, I. Pulp Capping Materials Modulate the Balance between Inflammation and Regeneration. Dent. Mater. 2019, 35, 24–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kermanshah, H.; Omrani, L.R.; Ghabraei, S.; Fekrazad, R.; Daneshparvar, N.; Bagheri, P. Direct Pulp Capping with ProRoot MTA Alone and in Combination with Er: YAG Laser Irradiation: A Clinical Trial. J. Lasers Med. Sci. 2020, 11, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Yazdanfar, I.; Barekatain, M.; Jahromi, M.Z. Combination Effects of Diode Laser and Resin-Modified Tricalcium Silicate on Direct Pulp Capping Treatment of Caries Exposures in Permanent Teeth: A Randomized Clinical Trial. Lasers Med. Sci. 2020, 35, 1849–1855. [Google Scholar] [CrossRef]
- Prasad, J.; de Ataide, I.D.; Chalakkal, P.; Likhyani, L.K. Comparison between the Outcomes of Two Platelet-Rich Concentrates on Apexogenesis in Young Permanent Incisors Requiring Endodontic Retreatment. Contemp. Clin. Dent. 2018, 9, 156. [Google Scholar] [CrossRef]
- Hu, C.-C.; Zhang, C.; Qian, Q.; Tatum, N.B. Reparative Dentin Formation in Rat Molars after Direct Pulp Capping with Growth Factors. J. Endod. 1998, 24, 744–751. [Google Scholar] [CrossRef]
- Paranjpe, A.; Zhang, H.; Johnson, J.D. Effects of Mineral Trioxide Aggregate on Human Dental Pulp Cells after Pulp-capping Procedures. J. Endod. 2010, 36, 1042–1047. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Yelick, P.C. Vital Pulp Therapy—Current Progress of Dental Pulp Regeneration and Revascularization. Int. J. Dent. 2010, 2010, 856087. [Google Scholar] [CrossRef] [Green Version]
- Degering, C.I. Physiologic Evaluation of Dental-Pulp Testing Methods. J. Dent. Res. 1962, 41, 695–700. [Google Scholar] [CrossRef] [PubMed]
- Iezzi, I.; Pagella, P.; Mattioli-Belmonte, M.; Mitsiadis, T.A. The Effects of Ageing on Dental Pulp Stem Cells, the Tooth Longevity Elixir. Eur. Cells Mater. 2019, 37, 175–185. [Google Scholar] [CrossRef] [PubMed]
- Hilton, T.J. Keys to Clinical Success with Pulp Capping: A Review of Literature. Oper. Dent. 2009, 34, 615–625. [Google Scholar] [CrossRef] [Green Version]
- Al-Hiyasat, A.S.; Barrieshi-Nusair, K.M.; Al-Omari, M.A. The Radiographic Outcomes of Direct Pulp-Capping Procedures Performed by Dental Students. J. Am. Dent. Assoc. 2006, 137, 1699–1705. [Google Scholar] [CrossRef]
- Thompson, V.T.; Craig, R.G.; Curro, F.A.; Green, W.S.; Ship, J.A. Treatment of Deep Carious Lesions by Complete Excavation or Partial Removal. J. Am. Dent. Assoc. 2008, 139, 705–712. [Google Scholar] [CrossRef]
- Rechenberg, D.-K.; Galicia, J.C.; Peters, O.A. Biological Markers for Pulpal Inflammation: A Systematic Review. PLoS ONE 2016, 11, e0167289. [Google Scholar] [CrossRef] [Green Version]
- Brannstrom, M.; Nordenvall, K.J. Bacterial Penetration, Pulpal Reaction and the Inner Surface of Concise Enamel Bond. Composite Fillings in Etched and Unetched Cavities. J. Dent. Res. 1978, 57, 3–10. [Google Scholar] [CrossRef]
- Watts, A.; Paterson, R.C. Bacterial Contamination as a Factor Influencing the Toxicity of Materials to the Exposed Dental Pulp. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1987, 64, 466–474. [Google Scholar] [CrossRef]
- Murray, P.E.; Windsor, L.J.; Smyth, T.W.; Hafez, A.A.; Cox, C.F. Analysis of Pulpal Reactions to Restorative Procedures, Materials, Pulp Capping, and Future Therapies. Crit. Rev. Oral Biol. Med. 2002, 13, 509–520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yazdanfar, I.; Gutknecht, N.; Franzen, R. Effects of Diode Laser on Direct Pulp Capping Treatment. Lasers Med. Sci. 2015, 30, 1237–1243. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Ma, L.; Li, Q.; Yang, W. Efficacy of Er:YAG laser-Assisted Direct Pulp Capping in Permanent Teeth with Cariously Exposed Pulp: A Pilot Study. Aust. Endod. J. 2020, 46, 351–357. [Google Scholar] [CrossRef]
- Alsofi, L.; Khalil, W.; Binmadi, N.O.; Al-Habib, M.A.; Alharbi, H. Pulpal and Periapical Tissue Response after Direct Pulp Capping with Endosequence Root Repair Material and Low-Level Laser Application. BMC Oral Health 2022, 22, 57. [Google Scholar] [CrossRef] [PubMed]
- El Mobadder, M.; Nammour, S.; Namour, M.; Namour, A.; Grzech-Leśniak, K. Disinfection Potential of 980 nm Diode Laser and Hydrogen Peroxide (3%) in “Critical Probing Depths” Periodontal Pockets: Retrospective Study. Life 2022, 12, 370. [Google Scholar] [CrossRef] [PubMed]
- Namour, M.; El Mobadder, M.; Mulongo, B.; Fagnart, O.; Harb, A.; Peremans, A.; Verspecht, T.; Teughels, W.; Nammour, S.; Rompen, E. Assessment of Disinfection Potential of Q-Switch Nd: YAG Laser on Contaminated Titanium Implant Surfaces. Materials 2021, 14, 6078. [Google Scholar] [CrossRef]
- Namour, M.; El Mobadder, M.; Magnin, D.; Peremans, A.; Verspecht, T.; Teughels, W.; Lamard, L.; Nammour, S.; Rompen, E. Q-Switch Nd:YAG Laser-Assisted Decontamination of Implant Surface. Dent. J. 2019, 7, 99. [Google Scholar] [CrossRef] [Green Version]
- Dawasaz, A.A. In Vivo Efficacy of Diode Laser as a Monotherapy in Root Canal Disinfection: A Systematic Review and Meta-Analysis. Photobiomodul. Photomed. Laser Surg. 2022, 40, 59–70. [Google Scholar] [CrossRef]
- Komabayashi, T.; Ebihara, A.; Aoki, A. The Use of Lasers for Direct Pulp Capping. J. Oral Sci. 2015, 57, 277–286. [Google Scholar] [CrossRef] [Green Version]
- Melcer, J.; Chaumette, M.T.; Melcer, F.; Dejardin, J.; Hassson, R.; Merard, R.; Pinaudeau, Y.; Weill, R. Treatment of Dental Decay by CO2 Laser Beam: Preliminary Results. Lasers Surg. Med. 1984, 4, 311–321. [Google Scholar] [CrossRef]
- Xue, V.; Zhao, I.; Yin, I.; Niu, J.; Lo, E.; Chu, C. Effects of 9,300 nm Carbon Dioxide Laser on Dental Hard Tissue: A Concise Review. Clin. Cosmet. Investig. Dent. 2021, 13, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Ohshiro, T.; Caldenhead, R.G.; Calderhead, R.G. Development of Low Reactive-Level Laser Therapy and Its Present Status. J. Clin. Laser Med. Surg. 1991, 9, 267–275. [Google Scholar] [CrossRef] [PubMed]
- Marques, N.C.T.; Neto, N.L.; Rodini, C.D.O.; Fernandes, A.P.; Sakai, V.T.; Machado, M.A.A.M.; Oliveira, T.M. Low-Level Laser Therapy as an Alternative for Pulpotomy in Human Primary Teeth. Lasers Med. Sci. 2014, 30, 1815–1822. [Google Scholar] [CrossRef]
- Hasheminia, S.M.; Feizi, G.; Razavi, S.M.; Feizianfard, M.; Gutknecht, N.; Mir, M. A Comparative Study of Three Treatment Methods of Direct Pulp Capping in Canine Teeth of Cats: A Histologic Evaluation. Lasers Med. Sci. 2010, 25, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Coluzzi, D.J. Lasers in Dentistry. Compend. Contin. Educ. Dent. 2005, 26, 429–435. [Google Scholar] [CrossRef]
- Gupta, S.; Kumar, S. Lasers in Dentistry—An Overview. Trends Biomater. Artif. Organs 2011, 25, 119–123. [Google Scholar]
- Convissar, R.A. Laser Dentistry 101: An Introduction to Wavelengths and Laser-Tissue Interaction. Semin. Orthod. 2020, 26, 74–79. [Google Scholar] [CrossRef]
- Nammour, S.; Renneboog-Squilbin, C.; Nyssen-Behets, C. Increased Resistance to Artificial Caries-Like Lesions in Dentin Treated with CO2 Laser. Caries Res. 1992, 26, 170–175. [Google Scholar] [CrossRef]
- Nammour, S.; Zeinoun, T.; Bogaerts, I.; Lamy, M.; Geerts, S.O.; Saba, S.B.; Lamard, L.; Peremans, A.; Limme, M. Evaluation of Dental Pulp Temperature Rise During Photo-Activated Decontamination (PAD) of Caries: An In Vitro Study. Lasers Med. Sci. 2010, 25, 651–654. [Google Scholar] [CrossRef]
- Robinson, H.B.; Lefkowitz, W. Operative Dentistry and the Pulp. J. Prosthet. Dent. 1962, 12, 985–1001. [Google Scholar] [CrossRef]
- El Mobadder, M.; Namour, A.; Namour, M.; Dib, W.; El Mobadder, W.; Maalouf, E.; Geerts, S.; Zeinoun, T.; Nammour, S. Dentinal Hypersensitivity Treatment Using Diode Laser 980 nm: In Vivo Study. Dent. J. 2019, 7, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Umana, M.; Heysselaer, D.; Tielemans, M.; Compere, P.; Zeinoun, T.; Nammour, S. Dentinal Tubules Sealing by Means of Diode Lasers (810 and 980 nm): A Preliminary In Vitro Study. Photomed. Laser Surg. 2013, 31, 307–314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ying, L.; Gao, J.; Gao, Y.; Xu, S.; Zhan, X.; Wu, B. In Vitro Study of Dentin Hypersensitivity Treated by 980-nm Diode Laser. J. Lasers Med. Sci. 2013, 4, 111–119. [Google Scholar] [CrossRef]
- Curti, M.; Rocca, J.-P.; Bertrand, M.-F.; Nammour, S.; Parker, S.; El Haddar, Y.S.; Cetik, S.; Bahrami, B.; Atash, R.; Lopes, R.M.; et al. Morpho-structural Aspects of Er:YAG-Prepared Class V Cavities. J. Clin. Laser Med. Surg. 2004, 22, 119–123. [Google Scholar] [CrossRef]
- Huang, P.; Chen, X.; Chen, Z.; Chen, M.; He, J.; Peng, L. Efficacy of Er:YAG Laser Irradiation for Decontamination and its Effect on Biocompatibility of Different Titanium Surfaces. BMC Oral Health 2021, 21, 649. [Google Scholar] [CrossRef]
- Deng, Y.; Zhu, X.; Zheng, D.; Yan, P.; Jiang, H. Laser Use in Direct Pulp Capping: A Meta-Analysis. J. Am. Dent. Assoc. 2016, 147, 935–942. [Google Scholar] [CrossRef]
- Javed, F.; Kellesarian, S.V.; Abduljabbar, T.; Gholamiazizi, E.; Feng, C.; Aldosary, K.; Vohra, F.; Romanos, G.E. Role of Laser Irradiation in Direct Pulp Capping Procedures: A Systematic Review and Meta-Analysis. Lasers Med. Sci. 2017, 32, 439–448. [Google Scholar] [CrossRef]
- Zhang, B.; Yang, B.-B.; Gao, Z.-Y.; Li, L.; An, H. Efficiency of Diode Laser-Assisted Methods in Direct Pulp Capping of Carious Teeth. Shanghai J. Stomatol. 2020, 29, 554. [Google Scholar]
- Zafari, J.; Jouni, F.J.; Nikzad, F.; Esmailnasab, S.; Javan, Z.A.; Karkehabadi, H. Combination of Dental-Capping Agents with Low Level Laser Therapy Promotes Proliferation of Stem Cells from Apical Papilla. Photobiomodul. Photomed. Laser Surg. 2023, 41, 3–9. [Google Scholar] [CrossRef]
- Alharbi, H.; Khalil, W.; Alsofi, L.; Binmadi, N.; Elnahas, A. The Effect of Low-Level Laser on the Quality of Dentin Barrier after Capping with Bioceramic Material: A Histomorphometric Analysis. Aust. Endod. J. 2023, 49, 27–37. [Google Scholar] [CrossRef]
- Cushley, S.; Duncan, H.F.; Lundy, F.T.; Nagendrababu, V.; Clarke, M.; El Karim, I. Outcomes reporting in systematic reviews on vital pulp treatment: A scoping review for the development of a core outcome set. Int. Endod. J. 2022, 55, 891–909. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Number of Treated Teeth | Sex | Age Range (Years) | Patients: Age ≤ 35 Years | Patients: Age ≥ 35 Years | Clinical Size of Exposed Pulp (Range in mm) | Cavity Classification | Tooth Position | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | Avg: 32 Min: 10 Max: 69 | Avg: 16 Min: 10; Max: 35 | Avg: 44 Min: 36; Max: 69 | Size of Exposed Pulp ≤ 1 mm | Size of Exposed Pulp >1 mm and <2 mm | Occlusal | Proximal | Incisor and Canine | Premolar and Molar | |
| 1995 | 1202 (60.25%) | 793 (39.75%) | 1995 | 1044 | 951 | 1163 | 832 | 664 | 1331 | 471 | 1524 |
| Procedure | ||||||
|---|---|---|---|---|---|---|
| Ca (OH)2 Paste | Bioactive Tricalcium Silicate Paste | CO2 | Er: YAG | Diode | Total | |
| Number of teeth | 376 | 279 | 1147 | 69 | 124 | 1995 |
| Teeth | Immediate Permanent Fillings | Delayed Permanent Fillings | Total |
|---|---|---|---|
| Number of teeth | 1249 | 746 | 1995 |
| Test | Normal State of the Pulp Tissue | Pathological State of Pulp Tissue | ||
|---|---|---|---|---|
| Reversible Pulpitis | Irreversible Pulpitis | Necrosis | ||
| Cold test with ethyl chloride | Positive (no change in intensity or duration after stimulation) | Positive (with change in intensity and/or duration less than 5 s after stimulation) | Positive (with change in intensity and/or duration more than 5 s after stimulation) | Negative |
| Horizontal percussion test | Negative | Negative | ---- | positive |
| Vertical percussion test Apical palpation pressure | Negative | Negative | ---- | Positive |
| Negative | Negative | ---- | Positive | |
| Electric vitality test | Positive | Positive | Positive | Negative |
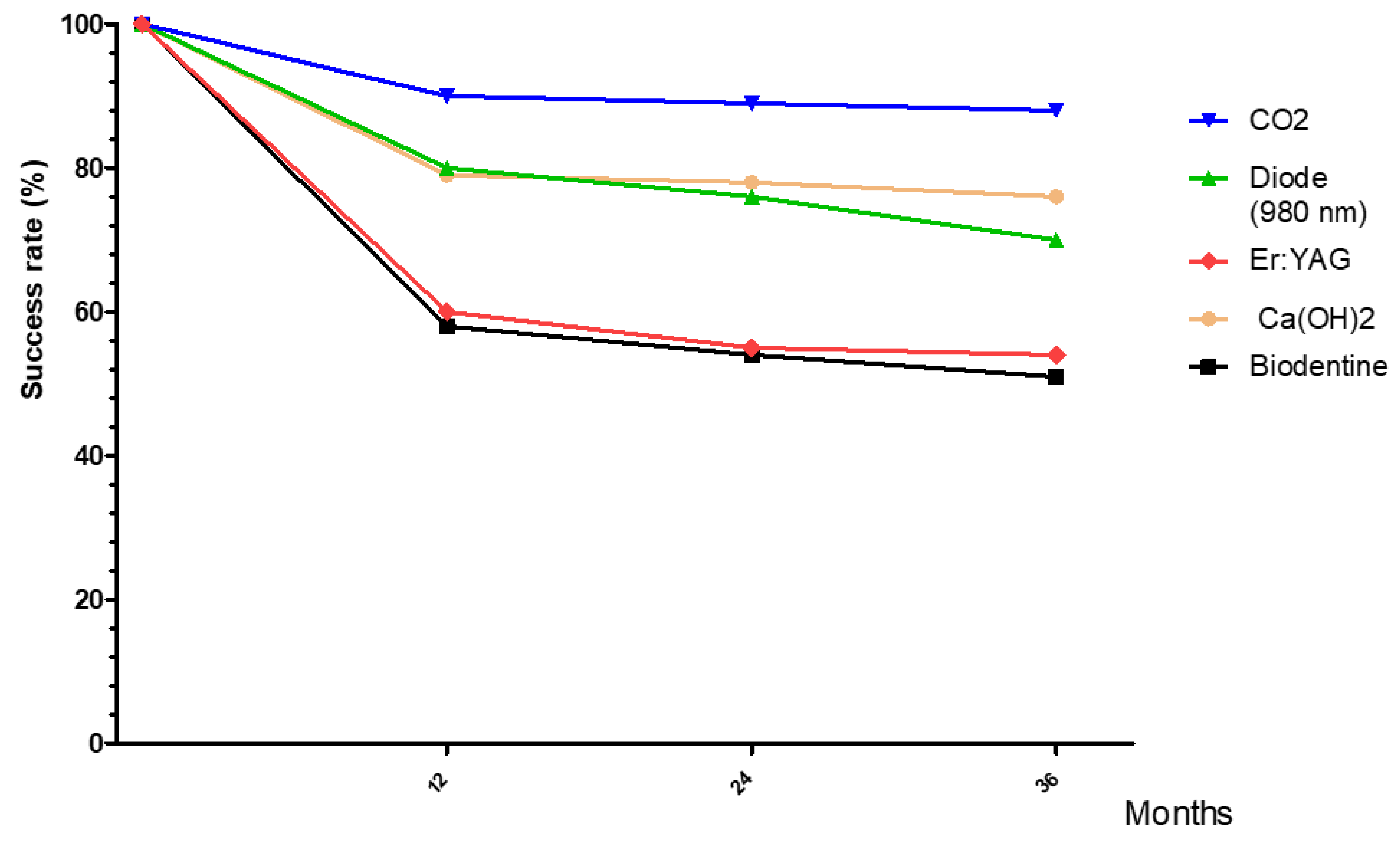
| Period (Months) | Ca (OH)2 (Paste) | Bioactive Tricalcium Silicate | Diode Laser (980 nm) | CO2 Laser | Er: YAG Laser |
|---|---|---|---|---|---|
| Twelve months | 79.81% A | 58.6% C | 80.5% A | 90.10% G | 60.58% C |
| Twenty-four months | 78.09% A | 54.32% D | 76.56% B | 89.86% G | 55.42% D |
| Thirty-six months | 75.72% B | 51.1% E | 70.01% F | 88.01% G | 54.55% D |
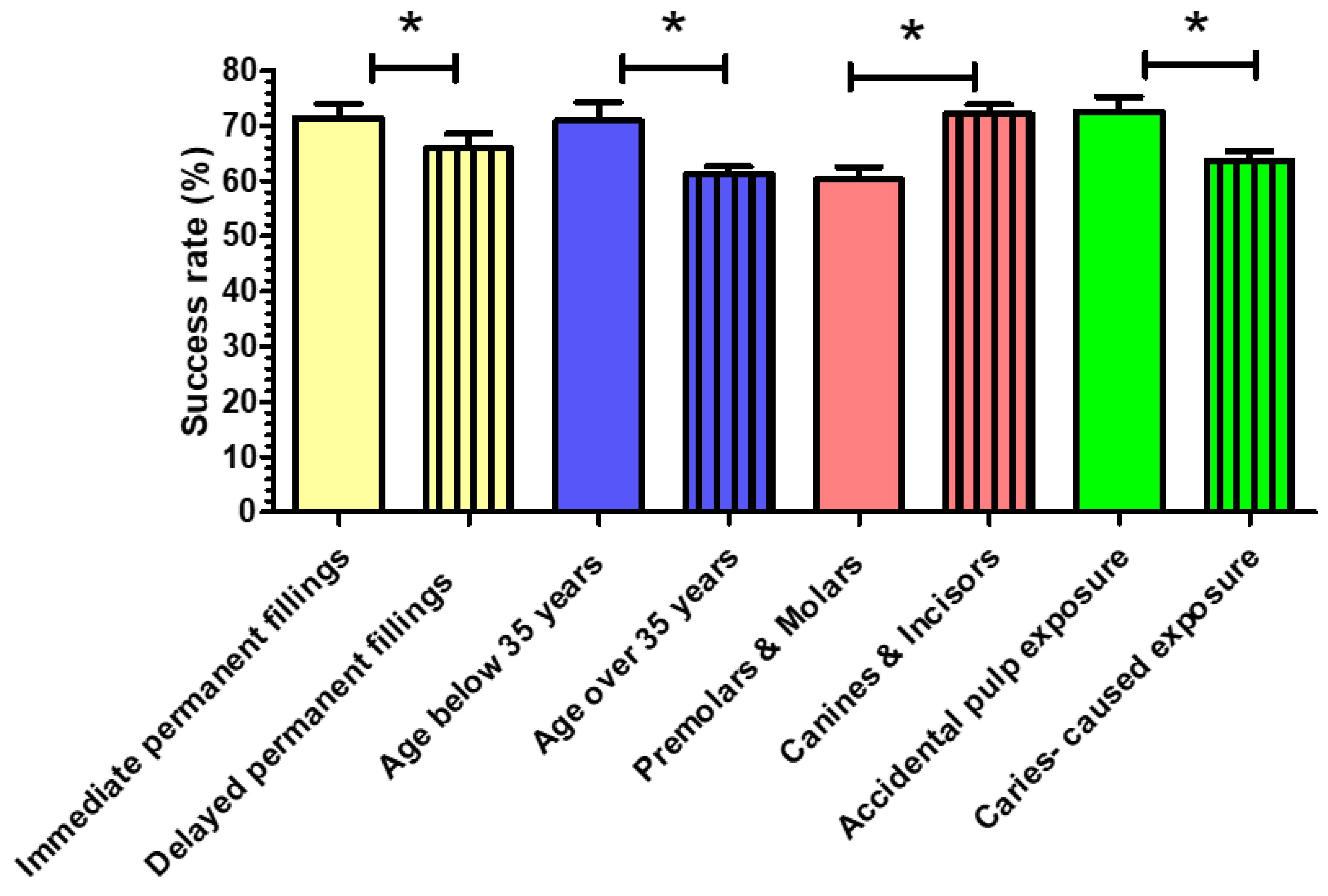
| Immediate Permanent Fillings | Delayed Permanent Fillings (6–8 Weeks) | Patients: Age ≤ 35 Years | Patients: Age > 35 Years | Pulp Exposure on Molars and Premolars | Pulp Exposure on Canines and Incisors | Idiopathic and Accidental Pulp Exposure | Caries-Caused Pulp Exposure |
|---|---|---|---|---|---|---|---|
| 71.41 ± 2.53% A | 65.93 ± 2.7% B | 70.91 ± 3.4% A | 61.2 ± 1.4% C | 60.3 ± 2.2% D | 72.1 ± 1.7% E | 72.58 ± 2.66 E | 63.7 ±1.7% F |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nammour, S.; El Mobadder, M.; Namour, M.; Houeis, S.; Heysselaer, D.; Nahas, P.; Todea, C.D.; Matys, J.; Grzech-Leśniak, K.; Olszewska, A.; et al. Success Rate of Direct Pulp Capping with Conventional Procedures Using Ca (OH)2 and Bioactive Tricalcium Silicate Paste vs. Laser-Assisted Procedures (Diode 980 nm, CO2, and Er: YAG). Photonics 2023, 10, 834. https://doi.org/10.3390/photonics10070834
Nammour S, El Mobadder M, Namour M, Houeis S, Heysselaer D, Nahas P, Todea CD, Matys J, Grzech-Leśniak K, Olszewska A, et al. Success Rate of Direct Pulp Capping with Conventional Procedures Using Ca (OH)2 and Bioactive Tricalcium Silicate Paste vs. Laser-Assisted Procedures (Diode 980 nm, CO2, and Er: YAG). Photonics. 2023; 10(7):834. https://doi.org/10.3390/photonics10070834
Chicago/Turabian StyleNammour, Samir, Marwan El Mobadder, Melanie Namour, Saad Houeis, Daniel Heysselaer, Paul Nahas, Carmen D. Todea, Jacek Matys, Kinga Grzech-Leśniak, Aneta Olszewska, and et al. 2023. "Success Rate of Direct Pulp Capping with Conventional Procedures Using Ca (OH)2 and Bioactive Tricalcium Silicate Paste vs. Laser-Assisted Procedures (Diode 980 nm, CO2, and Er: YAG)" Photonics 10, no. 7: 834. https://doi.org/10.3390/photonics10070834